
Abstract
The World Health Organization has identified intimate partner violence (IPV) as a public health issue affecting both men and women, though significantly more information is available regarding female victimization. This study examines IPV through the lens of male victimization, focusing on a comparison of physical and mental health consequences among men who are and are not military veterans. Results from a secondary analysis of data from the Behavior Risk Factor Survey taken by 13,765 males indicated that all males, regardless of veteran status, should be screened for IPV victimization given the prevalence reported in this sample (9.5% to 12.5%). Furthermore, it was found that veteran status did affect prevalence of particular health consequences, such as depression, smoking, and binge drinking. Based on the specific comparisons examined in this study, implications for Veteran’s Administration Health Services are discussed, as is the need for more research on IPV victimization rates for men and the particular health consequences that they suffer.
Background
Intimate partner violence (IPV) is a public health concern that gained national attention in the late 1970s and early 1980s, concurrent with the momentum of the women’s movement, with the proliferation of shelters that provided respite care to female victims and their families (Zorza, 1992). Following this increased public awareness, IPV research and advocacy efforts tended to focus on female victimization due to observed higher incidence. In a national random-digit phone survey conducted with 8,000 women and 8,000 men, lifetime prevalence rates were reported at 25.5% and 7.9%, respectively (Tjaden & Thoennes, 2000a, 2000b, 2000c). However, prevalence rates vary widely depending on the research methodology, questions asked, and populations studied. There is also literature supporting that both men and women are abused at similar rates, roughly 12% over a three-decade research trajectory (Strauss, 1999; Strauss & Gelles, 1989). Another survey, conducted among a sample drawn from private insurance records, revealed that rates of male victimization were three times those reported in national survey rates. Thirty percent of men reported being victimized over their lifetime, and 20% reported physical violence in the past year (Reid et al., 2008). However, these and other studies, demonstrating bilateral and/or significantly higher levels of violence, often did not inquire about motive or self-protection; thus, relatively little is known about men’s experiences with IPV and the mental and physical consequences of their abuse.
Full understanding is further complicated because male victims may experience shame and stigma related to IPV reporting, due to sociocultural expectations of masculinity, and these emotions may create service use barriers. However, the growing availability of help for men may be disrupting these ingrained stereotypes. Over the past decade, agencies have started to consider how to provide services to men, including hotline, counseling, and shelter availability, and advocates have begun to consider how to screen men and provide a continuum of services for their care (Rhodes et al., 2001; Rhodes, Lauderdale, He, Howes, & Levinson, 2002). A recent survey conducted by the Centers for Disease Control and Prevention revealed that the gender gap in regard to reporting is closing: 35.6% of women and 28.5% of men reported that during their lifetime they have been physically assaulted, raped, or stalked (Black et al., 2011). These positive developments have great impact because as the logistical and emotional barriers to reporting and help-seeking decrease, the complexity of men’s IPV experiences can be more fully examined and understood.
Participating in IPV screening is one of the best first steps in demystifying the male experience. Emergency department studies have reported men’s willingness to engage in computer-based risk assessment surveys that include IPV victimization and perpetration (Houry, Kaslow, et al., 2008; Houry, Rhodes, et al., 2008; Rhodes et al., 2009). Men complete the surveys and participate in recruitment efforts, willing to disclose both perpetration and victimization. Once men participate in victimization screening, their assessment data reveal a complicated picture, which will need consideration in creating effective interventions. Even for those men who are emotionally abused in isolation of physical abuse, there are health consequences (Rhodes et al., 2009; Straus et al., 2009). Men who report victimization have worse mental health and health outcomes. Similar to women, men with IPV victimization experiences reveal depression and reduced mental and physical health function compared to national data (Straus et al., 2009).
Given the prevalence of depression, and the physical, emotional, and financial costs associated with this debilitating condition, it is important to begin a dialogue with men about their experiences with IPV and the ways they handle the resultant depression. Kendler and colleagues suggest three pathways to male depression: internalizing symptoms, externalizing symptoms, and adversity and interpersonal difficulties (Kendler, Gardner, & Prescott, 2006). These three pathways are deeply interconnected, and men may exhibit multiple behaviors associated with each that could have serious negative effects. Thus, it is imperative to begin to disentangle the risk factors for increased morbidity and mortality and to begin to understand the unique needs of particular populations of men to inform service providers and improve outcomes.
Military veterans are a unique population with particular health care needs, especially returning veterans with comorbid physical and mental health issues. These men largely receive care through the Veterans Administration (VA), a unique service institution providing integrated health care and social services. It is, therefore, useful to identify the health and service needs of veterans independently from that of the general population. VA medical centers have specialized services to address sexual trauma that occurs during active military service. There is a lack of service attention, however, to IPV that may or may not include sexual violence and may or may not occur during military service. Identifying the prevalence of IPV victimization among male veterans and the associated health risks can inform the development of services through the VA health care system. Despite the emerging interest in male victims’ experiences with IPV, and some research on male veterans and IPV perpetration, we have almost no information about the prevalence of IPV victimization among male veterans and the resultant health consequences.
Purpose
The focus of this article is to examine the intersection between male IPV victimization, veteran status, and health consequences and behaviors. As the national veteran population grows, it is imperative to examine these intersecting issues to create appropriate screening, assessment, and referral strategies both within and beyond veteran health clinic walls. This article provides an alternative lens that examines the vulnerability of male veterans to be victimized and in need of services. We hypothesized that given the availability of health centers and outreach programs specifically catering to the veteran population, veterans would report better health than nonveterans. However, for those reporting both veteran and IPV victimization, we would see compromised health among the veteran population due to the impacts of IPV. There is currently no routine IPV screening in the VA for either men or women.
This article fills a gap in the literature. By using data drawn from the Behavioral Risk Factor Surveillance System (BRFSS) 2006 survey, we examine the intersection of IPV, veteran status, and health outcomes for 13,765 men. The study sought to answer the following questions:
Among male BRFSS participants, what are the sociodemographics of men based on their veteran status?
Is IPV associated with health risks including depression, smoking, binge drinking, and lack of exercise among those who endorse vet status and those who do not?
Method
Sample
Using data from the BRFSS survey, we examined health outcomes for 13,765 men, stratified by veteran status. Our sample was composed of the 2006 Centers for Disease Control and Prevention’s BRFSS survey results from select U.S. states and territories. This nationwide telephone survey was administered on a state level for all adults who were not living in institutions. Survey inclusion criteria required that the respondent was older than 18 years and a U.S. resident. For our analyses, we focused on male participants who provided responses to both the veteran status and IPV questions. The survey includes standardized questions that all states/territories administer, in addition to elective modules. All states/territories inquire about veteran status, the first focus of study aim. However, in 2006 only eight of the U.S. states and territories included the second area of inquiry, IPV status (Arkansas, Hawaii, Louisiana, Montana, Nevada, the U.S. Virgin Islands, Virginia, and West Virginia). Thus, the data for this article were drawn from all male BRFSS respondents in those states/territories that reported IPV status. The final sample size was 13,765 men.
Independent Variables
The BRFSS survey measures veteran status by asking, “Have you ever served on active duty in the United States Armed Forces, either in the regular military or in a National Guard or military reserve unit?” IPV measurement is slightly more complicated. The survey asks participants whether they have ever experienced the following: actual or threatened physical violence or unwanted sex. They define intimate partner as a current or former spouse, boyfriend, or girlfriend, which is a definition commonly employed in state laws regulating protection orders, as well as federal violence prevention legislation.
Covariates
Given earlier studies noted above, covariates included demographic variables selected a priori that could be associated with increased victimization rates. Literature demonstrates that age, poverty, minority status, high school education or less versus more education, and unemployment are all risks for increased victimization. Age was coded as a categorical variable (18-34, 35-55, 45-54, 55+ years). Because of differences in victimization rates by race, we coded race as non-Hispanic White versus non-White or Hispanic, due to sample size. Participants provided financial information, and we coded annual income as less than $25,000, $25,000 to $49,999, and $50,000 or greater. Participant education was reflected as less than a college degree or a college graduate plus postcollegiate training. The survey did not request information on whether those that identified as being a veteran used VA services.
To examine health risks, we were interested in five dependent variables for our logistic regression: depression, smoking status, drinking, exercise, and body weight. The BRFSS used the Patient Health Questionnaire–8 instrument, and our analysis employed a cutoff score of equal to or greater than 10, which has been used as the diagnostic cut point for depression (Kroenke et al., 2009). Due to lingering health risks, current smoking was measured as having smoked at least 100 cigarettes during a lifetime and currently smoking on some or all days. Binge or heavy drinking was identified if the respondent reported consuming five or more alcoholic drinks on one occasion in the past 30 days or having an average of greater than two alcoholic drinks per day within the past 30 days. We were interested in men’s exercise habits and body weight because of the connections between these health risks and IPV status. Exercise was dichotomously coded as “lack of exercise” if the participant reported having no regular exercise within the past month. Weight was calculated by using a body mass index, and we dichotomously (yes/no) coded individuals as overweight or obese for those who reported a body mass index greater than 25. This allows for a reference group for logistic regression purposes. Variables were coded for ease of interpretation with logistic regression. Age was categorized rather than used as a continuous variable for comparison purposes.
Analysis
We first present a chi-square descriptive analysis of the sample’s sociodemographic information, including lifetime IPV victimization, stratified by veteran status. We employed multivariate logistic regression, controlling for sociodemographic characteristics, to obtain the odds of IPV victimization, by veteran status. Finally, to assess for an association between IPV victimization and health risks (depression, smoking, heavy drinking, lack of exercise, high body mass index), we again used bivariate cross-tab analysis to obtain numbers and rates of each type of risk factor, by IPV history and stratified by veteran status. Last, we used multivariate logistic regression to obtain odds of each type of risk factor, by IPV history, controlling for demographic characteristics. We ran these analyses separately for veterans and nonveterans. Cases with missing values were excluded from the analyses. We present the exact p values (rather than merely indicating if significant or not), and all significant p values were <.01. All analyses were adjusted to compensate for sample design and nonresponse and were conducted using SAS version 9.2.
Results
Approximately 30% of the sample reported veteran status. The two groups reported significant differences related to age, race, and income. The veterans were more likely to be older, with 58% of them being older than 55 years (p < .0001). The veterans tended to be largely White, non-Hispanic compared to the nonveteran sample, which had more minorities (p < .001). Fewer veterans reported earning less than $25,000, with the large majority reporting income more than $50,000 (p < .01). There were no significant differences between the two groups regarding education. See Table 1 for more information.
Description of Sociodemographic Factors by Veteran Status Using Chi Square.
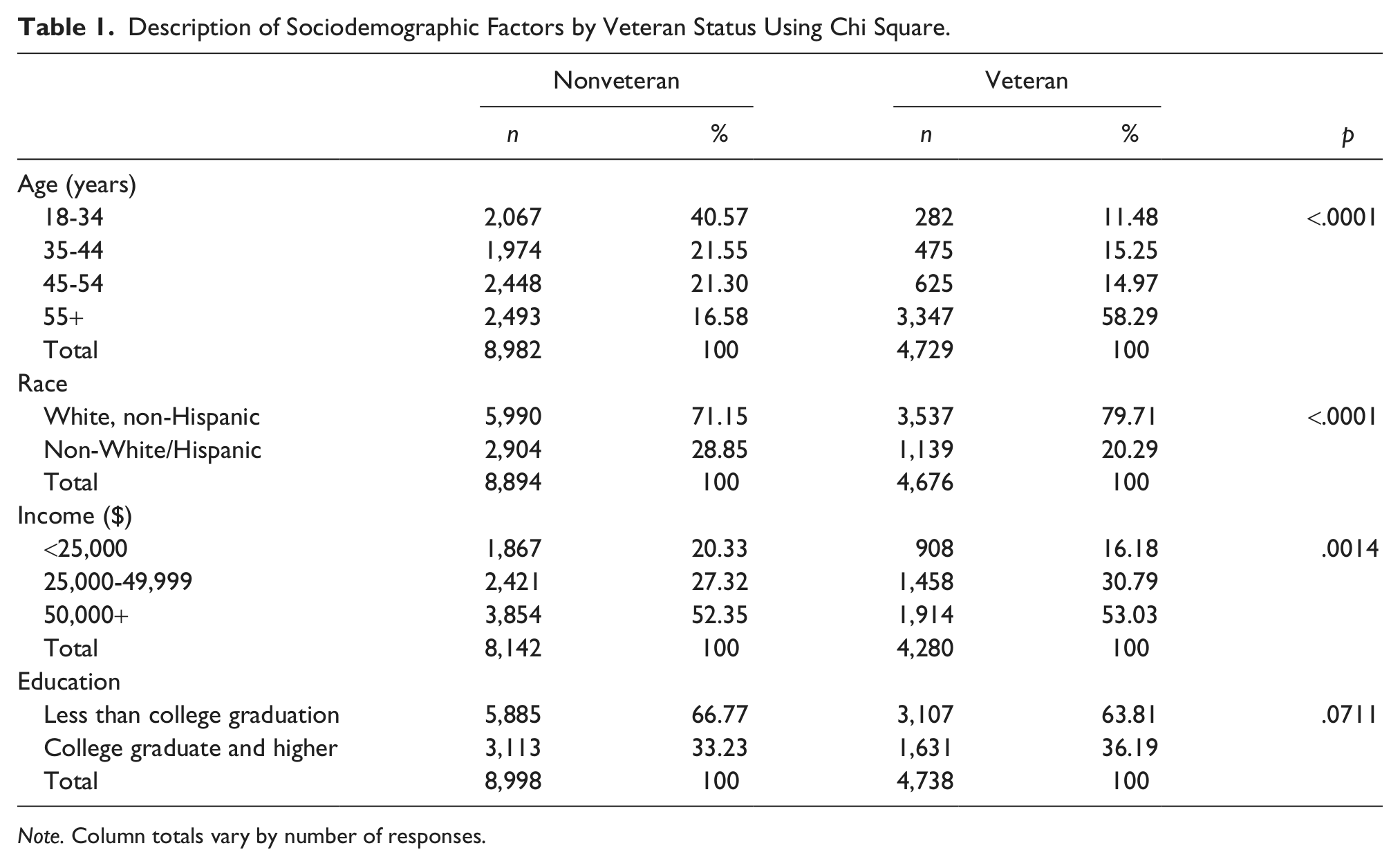
Note. Column totals vary by number of responses.
A smaller percentage of veterans (9.5%) than nonveterans (12.5%) reported lifetime IPV victimization (p < .01). Among nonveterans, those with IPV report statistically more depression, smoking, and binge drinking. IPV-involved nonveterans are more likely to exercise. Among veterans, those same findings hold except that IPV status is not associated with exercise. For both samples, IPV is not associated with being overweight or obese. See Table 2 for more information.
Health Risks by Intimate Partner Violence (IPV), Nonveterans Versus Veterans.

Note. Column totals vary by number of responses.
Mutlivariate analysis, which estimated whether IPV increased these health risk factors, controlling for age, race, income, and education, revealed interesting results (Tables 3 and 4), which replicated the earlier bivariate analysis. IPV increases the odds of depression fourfold for nonveterans, and for veterans IPV more than doubles their odds for depression. Regarding current smoking, nonveterans with IPV have double the odds of smoking. Veterans with IPV have double the risk for smoking. IPV increases both samples’ chances of heavy or binge drinking by almost 1½ times; heavy drinking is reported more often in nonveterans with IPV. IPV status decreased nonveterans’ exercise rates but was unrelated to veterans’ exercise routines. Again, IPV was unrelated to either group’s propensity to be overweight or obese.
Unadjusted Multivariate Logistic Regression Examining Effect of IPV by Veteran Status.

Note. IPV = intimate partner violence; uOR = unadjusted odds ratio; CI = confidence interval. Column totals vary by number of responses.
Adjusted Multivariate Logistic Regression Examining Effect of IPV by Veteran Status.

Note. IPV = intimate partner violence; aOR = adjusted odds ratio; CI = confidence interval. Controlling for age, race, income, and education. Column totals vary by number of responses.
Because data for women reflect higher IPV risk among younger women, and the veterans group was older, we duplicated the analysis for those who were younger than 55 years (not shown). While the sample distributions changed slightly, as did the level of statistical significance, it did not alter statistical associations between age, race, income, and veteran status. However, with the younger sample of veterans, their veteran status was no longer protective regarding IPV prevalence compared to their nonveteran comparison group.
Among the younger sample, IPV was associated with risks for depression and current smoking among both veteran and nonveteran samples. IPV was also associated with heavy drinking and exercise, in the same directions.
Multivariate analyses findings were also similar. IPV increased the odds for nonveteran and veterans alike for depression and current smoking. However, for the nonveteran group only, IPV increased their odds for heavy or binge drinking and a lack of exercise. IPV was unrelated, for both groups, to being overweight or obese.
Discussion
These findings suggest that among all men, regardless of age and veteran status, there are associations between IPV victimization and health risks as indicated by the analysis run on those younger than 55 years (not shown). For all men, both bivariate and robust multivariate logistic regression revealed that IPV victimization increases males’ odds for depressive symptoms and smoking, both health risk factors.
We see that younger veterans had a prevalence rate similar to the nonveterans. However, this is not true among older veterans. While we could speculate that older veterans may be more reluctant to share this information, the finding is consistent in studies involving women. Studies document that among women, there are age effects, albeit with conflicting results. Overall, there are likely age effects—for women, disclosure of lifetime IPV is higher among women younger than 55 more often than not. Among female veterans, younger women report greater IPV (Murdoch & Nichol, 1995).
Among the sample including older males, IPV is also a risk factor among veterans and nonveterans alike for heavy or binge drinking. However, among the younger males, IPV is only associated with binge drinking among nonveterans. Additionally, among men without veteran status, all analyses also report that IPV status increases the odds for a man to not exercise. Clearly, IPV status plays a critical role in men’s physical and mental health status, as found in earlier studies involving women.
There has been long-standing connection between depression, posttraumatic stress disorder, IPV, and suicide among women (Dutton et al., 2006; O’Campo et al., 2006; Seedat, Stein, & Forde, 2005). Researchers have documented that IPV-involved women are at greater risk for depression and suicidal thoughts and attempts (Devries et al., 2011; Rees et al., 2011). This is also true for civilian men who are victims (Coker, Weston, Creson, Justice, & Blakeney, 2005) as well as perpetrators (Taft, Murphy, King, Dedeyn, & Musser, 2005). When one is engaged in a violent or emotionally abusive relationship, it is easy to become hopeless and not understand the available resources. Facing job and housing loss, shrinking economic resources, isolation, and loss of social support, IPV victims face significant hurdles to help seeking. This may be true for male veterans as well, who return from deployments to find altered landscapes at their homes and places of employment.
There is a rise in returning veterans and increasing demands to meet their unique needs. Our returning military men and women are being diagnosed with comorbid depression and posttraumatic stress disorder, often attributed to their deployment. However, it is possible that some of the depression and stress may also be attributable to another battleground—their homes. And IPV victimization can compound social problems such as homelessness, economic strain, and social isolation. The Family Advocacy Program within the Department of Defense actively works to address issues of IPV among military families. The VA, however, does not currently have mandatory screening for IPV victimization among those who have left military service. Individuals returning from deployments and those leaving military service face social isolation and economic strains, as well as tensions associated with reintegration with families and communities, and psychological impacts of military related trauma exposure.
While great attention has been focused on the intersection of IPV and suicide among females, no literature has explored this among males, with the exception of perpetrator suicidal thoughts. Given the increase of reported suicides among men in the middle years, and particularly among veteran men, it seems imperative to begin to screen men, both veterans and nonveterans alike, for both depression and IPV status. While all men are at risk, suicide has become a pressing issue for men in the military and among veterans. When compared with civilians, male veterans were more likely to die by suicide over years 2000 to 2007 (Blow et al., 2012). The intersection of IPV and mental health among men warrants more attention.
Because of limitations in the data, we are unable to assess the nature and frequency of the violence reported in this male-only sample. We are also unable to estimate the timing of the violence relative to the current health conditions reported. The survey did not ask about information such as chronic pain and other common consequences that women experience. Likewise, we are unable to account for childhood experiences. Because this sample is composed of individuals from only those states that implemented the IPV modules, we are lacking representation from Northeast and Midwest regions. We recognize that utilizing one question to assess IPV is an oversimplification of the issue; however, we also recognize that there are little data addressing this important issue among men. We are unable to know whether our findings are generalizable nationally. Despite these limitations, our findings suggest that further inquiry is needed for understanding how male IPV experiences are affecting their physical and mental health.
Conclusion
Recent changes to national health care policies are recommending medical homes for individuals who use a host of medical care for chronic conditions. The Veterans Health Administration is currently implementing and evaluating a medical home model, called Patient Aligned Care Teams, across the country. Focusing on the whole person and coordinating patient care across systems, the medical home is an ideal model for addressing psychosocial health care issues that affect medical and mental health, including IPV victimization. Based on the findings that among veterans and nonveterans alike, IPV is correlated to more depression, smoking, and binge drinking, it is possible that IPV is contributing to chronic health impairment for men who would warrant early screening, assessment, and referral. By increasing early detection, services may be deployed such as safety planning, counseling, and support to hopefully stem the tide of victimization. However, the good news is that the odds for veterans having IPV and lower risk for health consequences suggests that veterans are faring well, including both older and younger veterans. The coordinated health care that some veterans are receiving may play a role in their veteran status being protective of both violence and poor health. This finding merits greater research.
Footnotes
Acknowledgements
The authors thank Neil McLaughlin for feedback on an earlier version of this article and wish to acknowledge Jennifer Thompson-Stone for her assistance with this article regarding editing.
Authors’ Note
The contents of this article do not necessarily represent the views of the Department of Veterans Affairs or the U.S. Government.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.