
Abstract

As the HIV epidemic evolves, health departments are developing and advancing innovative responses. The District of Columbia (hereinafter, the District) is one of a growing number of jurisdictions with a strategy to end the epidemic, called the 90/90/90/50 Plan; its goals are that 90% of District residents with HIV will know their status, 90% who know their status will be in treatment, 90% who are in treatment will be virally suppressed, and new infections will be reduced by 50% by 2020. 1
To work toward these goals and new targets established in a planned update, the DC Department of Health (DC DOH) implemented 2 major changes in the way the city pays for and plans HIV services: (1) a shift toward unit-cost reimbursement for HIV prevention and care services beginning in 2017 and (2) a merger of the prevention and care planning bodies in 2018. These changes—informed by insights from other jurisdictions—allowed DC DOH to refresh and refocus efforts to target the social and structural factors that underlie HIV risk and pose barriers to prevention and care services.
HIV in Washington, DC
Nearly 1 in 50 residents of the District were living with HIV in 2018. The city has made considerable progress in responding to the epidemic: the number of new HIV cases decreased 73%, from 1362 in 2007 to 360 in 2018. The percentage linked to HIV treatment within 90 days of diagnosis increased from 67% in 2014 (294 cases) to 88% in 2018 (316 cases). Meanwhile, the rate of those on HIV treatment achieving viral suppression within 1 year of diagnosis increased from 56% in 2014 (n = 248) to 77% in 2017 (n = 286). 2
The decline in the number of new cases in the District is due, in part, to the same factors contributing to a more modest decline across the nation. 3 The increase in viral suppression rates has led to a reduction in transmission, because persons with undetectable viral loads effectively have no chance of transmitting HIV. 4 -6 The DC DOH officially endorsed the scientific and stigma-reducing evidence of U=U (undetectable equals untransmittable) in 2017, 7 underscoring that persons living with HIV can live long lives without worrying about passing HIV to others or perceiving themselves as carriers of disease. 2 The advent of preexposure prophylaxis (PrEP) for persons without HIV has added a potent prevention opportunity. 6 DC DOH has conducted PrEP social marketing, 8 including sex-positive PrEP television advertisements; social media advertisement campaigns focused on gay and bisexual men (“Explore Your Options”), transgender women (“PrEP Pledge”), and African American women (“PrEP for Her”); and medical provider education. 9 In addition, DC DOH’s PrEP Drug Assistance Program 10 helps address cost-sharing barriers for HIV-negative residents of the DC metropolitan area.
The District’s implementation of needle exchange services, currently offered through 3 community providers at multiple sites and mobile units, has substantially reduced the number of transmissions. 11,12 In 2007, before the District’s needle exchange program launched, 150 newly diagnosed cases of HIV were attributed to injection drug use; in 2017, only 7 newly diagnosed cases of HIV were attributed to injection drug use, a decline of 95%. 2
Despite these positive steps, the District has one of the highest rates of new HIV infections in the nation: in 2016, the rate of new infections per 100 000 population aged ≥13 years was 70.5 in the District compared with 14.3 nationally. 3 The District’s overall HIV prevalence is 1.8%, which is nearly double the World Health Organization’s 1% threshold for a generalized epidemic and substantially higher than the nationwide prevalence of 0.3%. 2,13 A substantial portion of new infections in the District are among adolescents and young adults: in 2018, 38% of new HIV cases were diagnosed among persons aged 13-29 years. 2
The District faces a number of overlapping challenges in addressing HIV. First, many persons who work in the District live in surrounding states and vice versa, creating challenges to ensuring continuous access to prevention and care services. In addition, the District administers Ryan White HIV/AIDS program funding—federal support for HIV care and treatment—for a metropolitan area that includes all areas of the District, 5 counties in suburban Maryland, 11 counties and 6 independent cities in northern Virginia, and 2 counties in West Virginia, all of which must be actively engaged in coordination efforts, including data sharing and funding allocations. 14
The District has high rates of health insurance coverage compared with other states. 15 However, many District residents still face sizeable unmet social service needs and structural challenges, including racism, homophobia, and transphobia, which increase HIV vulnerability and hinder access to prevention and care services. Levels of food insecurity 16 and homelessness 17 are high in the District overall. Among respondents living with HIV who completed a 2017 Ryan White consumer needs survey administered by DC DOH, nearly 1 in 5 had dealt with homelessness in the previous year, and more than 1 in 3 reported lacking enough money for food or other necessities at some point during the year. Respondents were mostly in HIV care; social needs are likely even greater among those who are not in care (unpublished data, 2017 Metropolitan Washington Regional Ryan White Planning Council Unmet Needs Assessment: Consumer Survey and Provider Consultation Results; DC DOH HIV/AIDS, Hepatitis, STD and TB Administration).
Changing How the DC DOH Pays for HIV Services
Unit-Cost Reimbursement
Traditionally, in the Ryan White program and public health programs overall, state and local jurisdictions have used a grants-based model to fund health and social service providers. Grants cover a predetermined portion of salaries and expenses based on proposals and budgets submitted for each grant cycle. In a unit-cost or fee-for-service model, a program pays providers for each unit of service offered. Interested providers demonstrate their capacity to offer services in a given category and then enter an agreement with the program to bill per service.
The literature on using unit cost for Ryan White–funded services is lacking. 18 To better understand the model, DC DOH staff members and consultants conducted telephone interviews with experts from several jurisdictions in 2014 and 2015: Los Angeles County, Orange County, and San Diego, California; Fort Lauderdale/Broward County and Miami-Dade, Florida; St. Louis, Missouri; New York City and New York State; and Washington State. Many interviewees noted that under a unit-cost funding system, funds flow easily toward client needs, offering more flexibility than a fixed annual grant. Some experts also noted that under a traditional grants-based system, providers may have little incentive to serve more people because they receive the same amount of funding regardless of the number of clients served. For medical and dental services, compared with grant-based funding, a unit-cost model better aligns Ryan White funding with reimbursement from other third-party payers. The unit-cost approach also lends itself to performance improvement features, such as bonuses or rate increases for providers who meet quality thresholds. 19
Other jurisdictions noted challenges, such as providers who resist changing from grant-based funding to unit-cost funding, particularly if grants are perceived as a more predictable way of supporting organizational capacity than unit-cost funding. Providers of support services, in particular, may not adapt as easily to a unit-cost model as do clinical providers who already bill other payers. 19 In addition, defining units of service and setting rates can be challenging, particularly in service categories that are difficult to divide into discrete units, such as outreach.
Introduction of Unit-Cost Reimbursement in the District
In 2017, DC DOH adopted a unit-cost approach for a subset of services in the Ryan White program: outpatient ambulatory health services, mental health services, substance abuse outpatient care, oral health services, food bank and home-delivered meals, nonmedical case management, and housing services. These services were selected largely because they were relatively easy to define in discrete units. DC DOH also moved to unit-cost reimbursement for some prevention programs, including HIV testing, linkage to care, PrEP education and enrollment, and health education and outreach. (Ryan White services that remain under the traditional model are medical case management, early intervention services, home and community-based health services, emergency financial assistance, health education/risk reduction, other professional services, linguistic services, medical transportation, and psychosocial support services.)
This transition to a unit-cost approach was not simple. Similar to other jurisdictions, DC DOH heard concerns from providers about this important transition and found rate setting to be challenging. The District faced unique rate-setting challenges because the eligible metropolitan area includes portions of 4 states and a range of urban and suburban settings; it was necessary to identify the varying costs of service delivery across the metropolitan area and set rate levels that would equitably cover the service components for all providers. Certain service delivery issues, such as the need for multiple attempts to navigate some clients into care, required particular consideration. Logistically, unit-cost billing processes required various staffing, billing, and tracking systems both at DC DOH and among providers.
Despite these challenges, the transition to unit-cost reimbursement has helped support the District’s goals for prevention and treatment of HIV. In addition to the benefits noted by other jurisdictions, 19 the District model offers equity for providers across the multistate region and allows funds to flow toward areas of client demand based on service and location.
For example, for HIV prevention, the number of DC DOH–supported PrEP initiations doubled from 1700 in 2017 to 3400 in 2018, among a more racially and economically diverse population than the higher-income, white, gay men who largely benefit from PrEP nationally. 20 We believe this increase is due in part to the change in funding approach. Most community-based organizations that serve diverse populations in the District are small, and in the grants-based model, their reach was limited because of fixed funding for staff members and other costs. Unit-cost reimbursement enables these organizations to grow their outreach and service numbers during the year and be reimbursed accordingly.
The impact of the unit-cost model on use of Ryan White service categories has also been substantial, creating the opportunity to better address structural barriers to HIV care in the region. As seen for prevention services, the previous fixed-funding approach had limited the reach of smaller Ryan White–funded organizations serving diverse populations in the region. Unit-cost reimbursement frees smaller organizations to grow their capacity to provide increased units of service.
From 2017 to 2018, the number of clients and service units increased primarily among a set of supports and services to address unmet social needs (Table). Meanwhile, declines occurred in the number of clients using Ryan White–funded services that are typically covered by health insurance, including outpatient ambulatory health services (33 percentage-point decline), mental health services (68 percentage-point decline), and oral health care (65 percentage-point decline). Because most residents of the District and the DC eligible metropolitan area 14 have health insurance, 15 the unit-cost model provides flexibility to shift funds as appropriate from medical services toward support services, to address social determinants of health. In effect, after the payment model transition, more money flowed to services that address barriers to care and unmet needs beyond the clinical setting, with the potential to contribute to reductions in disparities and structural barriers.
Selected changes in use of Ryan White HIV/AIDS services, DC eligible metropolitan area, a 2017-2018
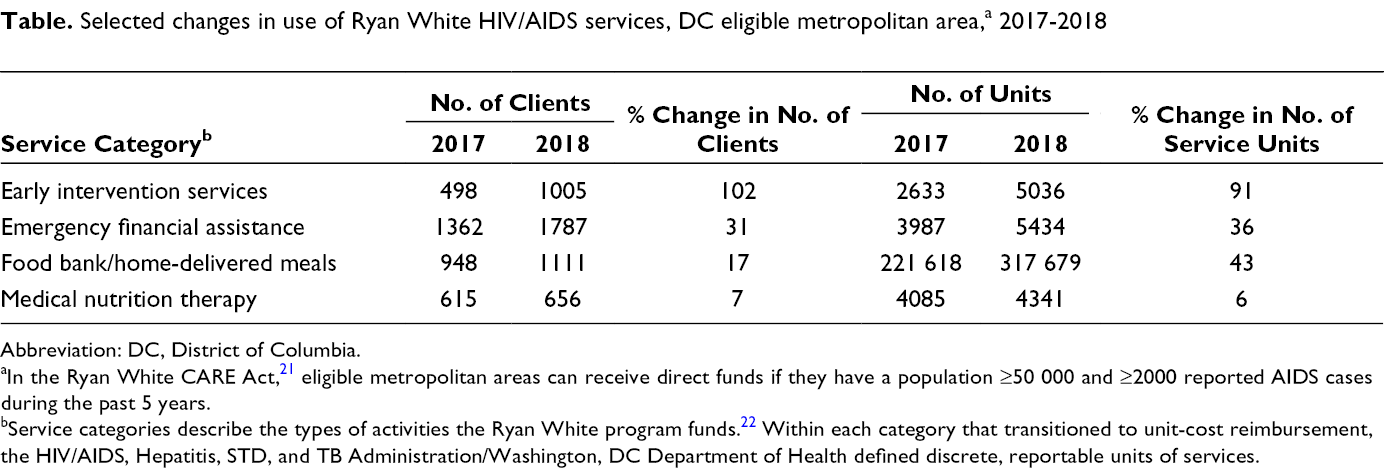
Abbreviation: DC, District of Columbia.
aIn the Ryan White CARE Act, 21 eligible metropolitan areas can receive direct funds if they have a population ≥50 000 and ≥2000 reported AIDS cases during the past 5 years.
bService categories describe the types of activities the Ryan White program funds. 22 Within each category that transitioned to unit-cost reimbursement, the HIV/AIDS, Hepatitis, STD, and TB Administration/Washington, DC Department of Health defined discrete, reportable units of services.
Integrating Prevention and Care Planning
Impetus for Integrated Planning
Under federal law, Ryan White metropolitan programs must have a planning council that conducts prioritization and resource allocation. 23 The Centers for Disease Control and Prevention (CDC) requires health departments that receive prevention funds to have HIV planning groups to inform implementation of the jurisdiction’s prevention plan. 24 Integrated planning guidance issued in 2015 from CDC and the Health Resources and Services Administration to support the submission of Integrated HIV Prevention and Care Plans underscores the national trend toward greater coordination of prevention and treatment, which have often been planned separately. 25
Since the 2015 release of the merged federal guidance, 25 merging the bodies for care and prevention planning began to make sense for DC DOH. HIV programming in the District, as in much of the country, often includes integrated testing, prevention, and care. Both U=U and PrEP blur the boundaries between prevention and treatment. Some providers had been receiving funds for both prevention and care. Most importantly, the social and structural challenges faced by persons living with HIV—including poverty, food insecurity, housing shortages, mental health and substance use disorders, racism, and transphobia—are the same as the challenges experienced by persons at risk for HIV. 26 -29
Although resources are available for best practices for coordinated prevention and care planning, including how to create comprehensive Integrated HIV Prevention and Care Plans, 30 -32 few resources address the integration of prevention and care bodies. In 2017, DC DOH interviewed stakeholders from Chicago, Los Angeles County, San Francisco, and Philadelphia, all of which had merged their prevention and care planning councils. DC DOH then undertook a planning process that included internal meetings, a workgroup with members of the District’s existing prevention and care bodies (the DC HIV Prevention Planning Group and the Metropolitan Washington Regional Ryan White Planning Council), and external community engagement sessions to identify the concerns and priorities of persons living with HIV, persons at risk of HIV, providers, and other stakeholders.
DC’s Merged Planning Commission
In 2018, the 2 former bodies (the DC HIV Prevention Planning Group and Metropolitan Washington Regional Ryan White Planning Council) technically dissolved and a new commission, with a structure and bylaws that synthesized the roles of both previous bodies, was established. 33,34 The new Washington, DC Regional Planning Commission on Health and HIV (hereinafter, the Commission) convened in May 2018, with some members of the previous planning bodies along with new members. The Commission is responsible for setting priorities and allocating resources for Ryan White funding to address HIV care and has an advisory role in HIV prevention. The merger has allowed the Commission to address HIV prevention and care across the metropolitan area as an intersectional approach, assessing needs, programming, and opportunities by capturing the full scope of the HIV continuum, from prevention to viral suppression.
For example, the newly merged Commission helped develop a regional proposal for Ryan White Early Intervention Services (EISs) with a status-neutral framework, referring all persons living with or at risk for HIV to the services they need to improve their health. 35 EISs meet relevant populations with outreach and testing, linking those who test positive to care and treatment services and those who test negative to prevention services such as PrEP. For all clients, EISs include health education, risk-reduction services, and linkage and navigation to meet other health care, housing, and social needs. For DC DOH, the Commission made it easier to develop the EIS proposal than it would have been with 2 separate bodies by offering insights based on a broad view of the epidemic in the region.
The Commission takes an integrated view of other activities that intersect with both prevention and care, such as sexually transmitted infection services; molecular surveillance, which can help health departments better target prevention and care services; and efforts to scale up PrEP and treatment as prevention through the health care system. These and other issues warrant thoughtful consideration by the Commission to view disparities and structural issues across the health care system.
Merging the planning and prevention groups into one Commission was not without friction. Two bodies with distinct operating procedures and bylaws had to be merged. The District has also faced a challenge that other merged jurisdictions described 19 : namely, how to ensure that the new Commission does not focus disproportionately on treatment. The Commission still serves a major, statutorily defined role in priority setting and allocation for Ryan White care and treatment funding, without a corresponding formal role related to CDC prevention funds. Therefore, the DC DOH and the Commission are continuing to explore how to bolster the Commission’s role in prevention.
Next Steps
The District’s policy changes continue to show promise: DC DOH will merge its prevention and care divisions within the department, starting with the appointment of a PrEP coordinator in the Care Division, and is considering integrated data collection strategies. Meanwhile, unit-based funding of Ryan White services has the potential to allocate resources to address HIV in the District more efficiently.
However, challenges remain. DC DOH will be revising its prevention unit-cost services in 2020 in the new context of broader grant funding through its status-neutral EIS initiative. In the context of this revision, DC DOH will also examine how to interweave funding to attribute EIS costs appropriately; for example, Ryan White funds can pay for the person who conducts the HIV test, but prevention funds will pay for the test itself.
DC DOH will also need to change how it monitors programs and implements new evaluation metrics in the context of an anticipated 2020 revision of the 90/90/90/50 plan. For example, DC DOH has set rapid initiation of antiretroviral treatment as a new key strategy; as clinical practices evolve to meet this standard, DC DOH will need to identify an appropriate goal in reducing median time to viral suppression, which was 114 days in 2018. 2 The Commission will have to continue to define its role in HIV prevention and identify priority strategies on ending the epidemic, including establishing new standards of care regionally on rapid antiretroviral therapy, U=U, and PrEP initiation.
The District’s situation is somewhat distinct from other jurisdictions. High rates of health insurance coverage in most of the DC eligible metropolitan area allow a focus on nonclinical services that other grantees, particularly in non-Medicaid expansion states, cannot afford as easily. 22 Meanwhile, the region’s inclusion of portions of 3 additional states requires an even higher level of coordination than in most other jurisdictions. Other jurisdictions could consider whether a change in reimbursement policy is appropriate by assessing the efficacy of their current systems, consulting with providers and consumers about their needs and the feasibility of various approaches, and assessing their own capacity for movement to a different funding model. However, the reasons for addressing prevention and treatment in an integrated fashion—including clinical advances such as PrEP and U=U, as well as the shared set of social determinants affecting both sides—are likely to be relevant across many jurisdictions.
Conclusion
Integrating HIV care and prevention, as well as ensuring that programs continue to use resources to address structural and systemic barriers to health, are important for meeting the goals of the 90/90/90/50 plan. Thanks to community members, providers, planning body members, and other stakeholders, the District continues to address the challenges of ending the HIV epidemic and the many inequities it reflects and perpetuates.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: NS, KH, and GD received contractual funding from the DC Department of Health to conduct policy research to support the department’s activities. Data collection and program activities conducted by the DC Department of Health and described in this article are supported by funding from the Centers for Disease Control and Prevention (Integrated HIV Surveillance and Prevention Programs for Health Departments [PS18-1802], grant no. 5 NU62PS924565-03-00) and the Health Resources and Services Administration (Ryan White HIV/AIDS Program, Part A [HRSA-19-033], grant no. H89HA00012).