
Abstract
Objective:
AIDS Drug Assistance Programs (ADAPs) are state-administered programs that pay for medical care and medication for people living with HIV (PLWH) in the United States. In October 2021, the federal policy requiring that clients recertify for the program every 6 months was repealed, giving states the authority to set their own recertification policies. However, little data exist on the costs and health effects of alternative recertification schedules. We assessed the cost of changing the legacy 6-month recertification to a 12-month schedule in Washington State to inform policy decisions on recertification.
Methods:
We used a Markov model to simulate the population of PLWH in Washington State who are eligible or enrolled in ADAP. We obtained model inputs and validation data from the Washington State Ryan White database. We estimated the cost of 12-month and 6-month criteria over a 5-year time horizon. Model outputs included annual program costs, population sizes, and number of people virally suppressed, by scenario.
Results:
Under a continuation of the legacy 6-month recertification criteria, the annual cost of Washington ADAP would be $37 663 000 (95% CI, $34 570 000-$41 686 000) during the next 5 years, with a per-client cost of $7966 (95% CI, $7478-$8494). Under 12-month criteria, the annual cost would be $40 217 000 (95% CI, $36 243 000-$44 401 000) and the per-client cost would be $7543 (95% CI, $7084-$8042). Under the 12-month scenario, 245 more people will have been virally suppressed by the end of 2025.
Conclusions:
Switching to a less frequent recertification process may improve health outcomes at a modest increase in cost in Washington State.
AIDS Drug Assistance Programs (ADAPs) are state-administered programs that pay for medication and health care for more than 240 000 people living with HIV (PLWH) in the United States. 1 ADAP clients have a high rate of viral suppression compared with other US populations of PLWH, and the program is shown to be cost-effective in increasing viral suppression.2,3 ADAPs are funded by the Ryan White Act, 4 which requires that the programs pay only for services that clients cannot otherwise afford and for which no other payer exists. For clients without health insurance, ADAPs make direct payments to service providers; for clients with health insurance, ADAPs pay for health insurance deductibles, copays, and premiums. ADAP eligibility is based on a client’s income, and historically, programs have been required to verify client eligibility every 6 months. 5 However, completing the 6-month recertification process has been challenging for some clients, particularly for those at high risk of disengaging from care. In Washington State, 1423 (26%) clients were removed from the ADAP during a 2-year period due to failure to complete the recertification, and 12% of these clients lost viral suppression.6,7 Studies in other jurisdictions found the recertification requirement to contribute to the underuse of ADAPs and create a barrier to viral suppression.8,9
In October 2021, the Ryan White HIV/AIDS Program released Policy Clarification Notice 21-02, which substantially reduced the requirements for programs to verify eligibility of clients of the nationwide ADAPs. 10 Programs in each state now have the authority to set the frequency and manner in which PLWH are assessed for ADAP eligibility. This policy change presents an opportunity for improving the recertification process, but the potential impact of this policy change on HIV health outcomes and costs is not known. Before announcing the change, the Health Resources & Services Administration hosted an opportunity for the public to comment on the recertification process in its 2018 Request for Information on Administrative Streamlining and Burden Reduction. 11 One frequently mentioned suggestion was to change the recertification requirement from every 6 months to every 12 months, which could reduce the number of opportunities for clients to miss recertification and lower the administrative costs of verifying eligibility. 11 Such a change has precedent in Medicaid for children and the Children’s Health Insurance Program (CHIP), where 27 states have implemented 12-month continuous eligibility and seen a decrease in disenrollment.12,13 Although a 12-month recertification can reduce disenrollment among people who are eligible, it may increase the length of time that ineligible clients remain in ADAP before they are disenrolled. Therefore, it is important to understand the effect of this commonly proposed policy change on the program’s budget.
To examine the effect of this proposed policy change, we conducted a cost analysis of changing from a 6-month to a 12-month recertification requirement in Washington State. Findings can provide insight to policy makers on the feasibility and effect of implementing a 12-month recertification requirement in Washington State and elsewhere.
Methods
We conducted a cost analysis of a 12-month recertification requirement in Washington State. In conjunction with Ryan White administrators in Washington State, we identified 3 key outcomes: (1) the projected cost of the Washington State ADAP, (2) the number of people virally suppressed in Washington State, and (3) the number of clients who received services while ineligible for the program. In accordance with good practice recommendations and acknowledgment of the uncertainty of the future health care landscape, we chose to model a 5-year time horizon. 14 Our model used a payer perspective (Washington State Department of Health [DOH] ADAP).
Model Structure
We used R software version 4.2.1 (R Foundation for Statistical Computing) to develop a Markov model of PLWH in Washington State who were currently or formerly enrolled in ADAP. The base model contained 3 health states: enrolled in ADAP and eligible, disenrolled from ADAP due to failure to recertify, and removed from ADAP due to ineligibility (Figure 1). The model assumed a constant number of new individuals enrolled in ADAP for the first time every month (eFigure 1 in the Supplement). Clients could transition from being in ADAP to being disenrolled and back to ADAP (eFigure 2 in the Supplement). Clients enrolled in ADAP could also transition to ineligible and back at a fixed rate. We did not include death or emigration in the model, because these events occurred at a negligible rate during the model time horizon. We used a time step of 1 month.
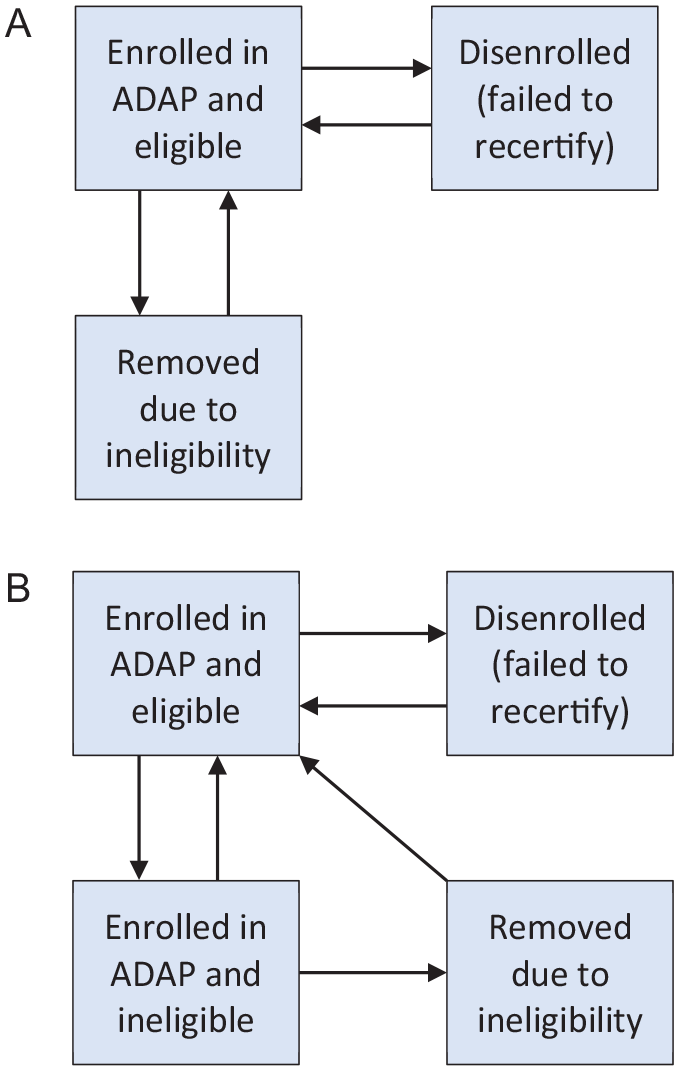
Model structure of the population currently and formerly enrolled in the Washington State ADAP under (A) the legacy 6-month recertification scenario and (B) a proposed 12-month recertification scenario. Under the 12-month recertification scenario, people who become ineligible while in ADAP remain for an average of 6 months before their ineligibility is identified and they are removed. Arrows indicate flow of clients.
The model was stratified by health insurance type (public, private, or no health insurance) and receipt of case management services during the year. Case management is a distinct Ryan White program (with looser annual eligibility requirements). Clients in case management receive help in reenrolling in ADAP, which adds to the cost in staff time.
Clients could change health insurance type at any month and change case management status at the beginning or end of each year. All analyses met the criteria for program evaluation and received exemption from review from the University of Washington Institutional Review Board. Data were collected as surveillance activities as mandated by Washington State law.
Model Parameters
We derived transition probabilities by using enrollment data from the Washington State DOH in its administration of the program from 3 calendar years, 2017 through 2019 (Table 1). A client’s health insurance status was assumed to not change when they were not in the program. Case management status was reassigned annually based on receipt of case management services. Because of the large amount of transition at the beginning of the calendar year, we estimated 2 sets of transition probabilities: a set for the month of January and another set for the months of February through December. We extracted initial population sizes and monthly population sizes from the Washington State DOH Ryan White administrative database.
Parameters for Markov model of population currently and formerly enrolled in the Washington State ADAP, derived from years 2017-2019 a
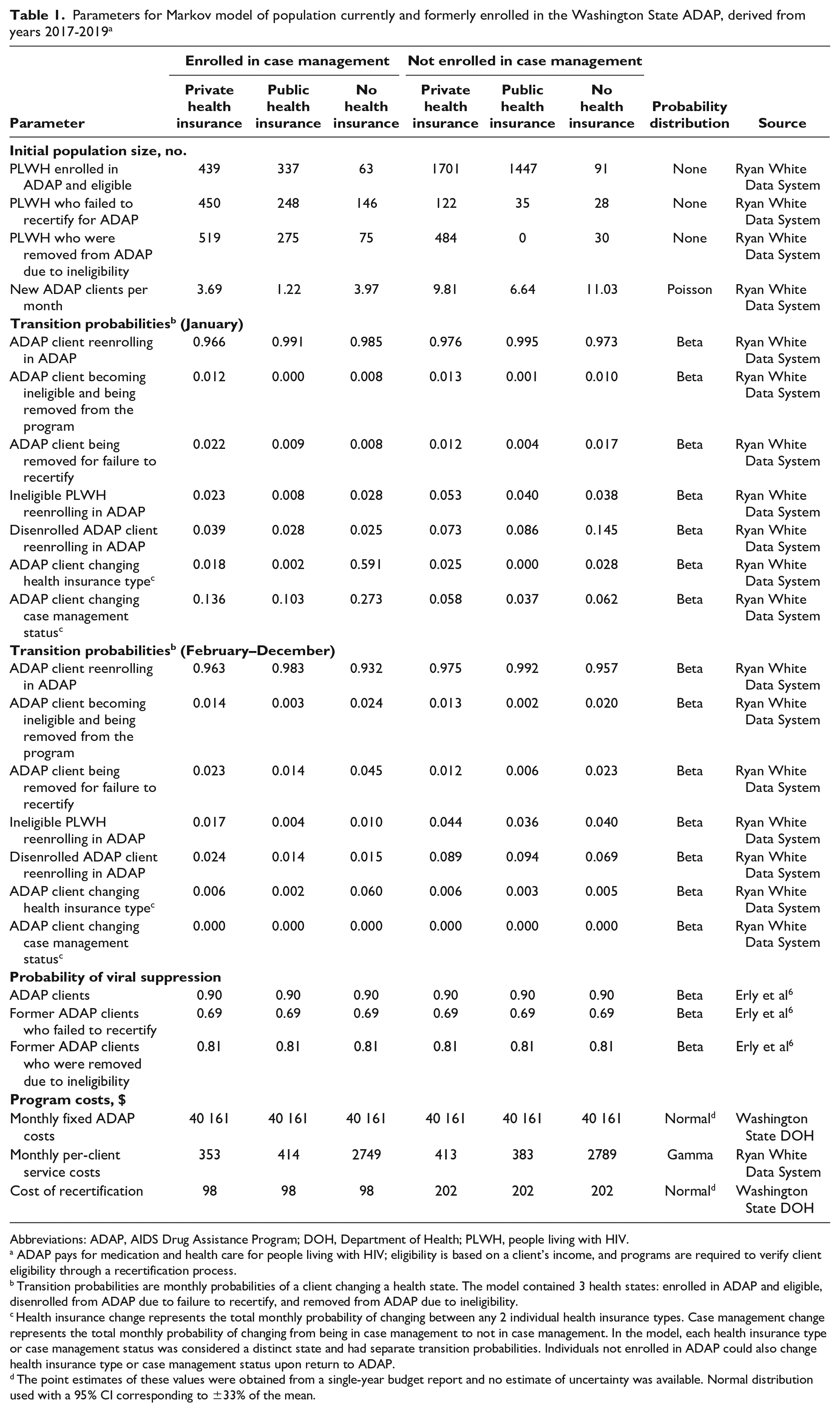
Abbreviations: ADAP, AIDS Drug Assistance Program; DOH, Department of Health; PLWH, people living with HIV.
ADAP pays for medication and health care for people living with HIV; eligibility is based on a client’s income, and programs are required to verify client eligibility through a recertification process.
Transition probabilities are monthly probabilities of a client changing a health state. The model contained 3 health states: enrolled in ADAP and eligible, disenrolled from ADAP due to failure to recertify, and removed from ADAP due to ineligibility.
Health insurance change represents the total monthly probability of changing between any 2 individual health insurance types. Case management change represents the total monthly probability of changing from being in case management to not in case management. In the model, each health insurance type or case management status was considered a distinct state and had separate transition probabilities. Individuals not enrolled in ADAP could also change health insurance type or case management status upon return to ADAP.
The point estimates of these values were obtained from a single-year budget report and no estimate of uncertainty was available. Normal distribution used with a 95% CI corresponding to ±33% of the mean.
Costs
We included costs of ADAP services and recertification (if enrolled in ADAP). Because case managers are also funded via the Ryan White program and are responsible for assisting their clients in recertification, we assigned clients receiving case management an additional cost to represent this service. We also estimated a fixed overhead cost of the ADAP and the cost of health care for PLWH who are not in ADAP. We obtained data on the monthly cost of ADAP services by health insurance type and case management status from the Washington State DOH administrative database. Working with financial staff at the Washington State DOH, we estimated the fixed annual overhead cost of the program, the cost of recertification staff, and the cost of case management staff. Under the assumption that staff time is flexible and can be reallocated, we estimated the cost per recertification as the annual cost of recertification staff divided by the number of recertifications in a year. We estimated the additional cost of case management assistance in recertification as the annual cost of case management staff multiplied by the proportion of time spent by case managers assisting clients in this task (as estimated by program leadership and former case managers). This annual cost was divided by the number of recertifications in a year by clients who use case management services. We derived the probability of viral suppression in each health state from published literature. 7 No discounting was performed.
Model Scenarios
We compared ADAP with a 6-month recertification schedule with a scenario of ADAP with a 12-month recertification schedule. We compared the following outcomes: annual ADAP cost to Washington State DOH and other health care systems, average monthly ADAP enrollment, proportion of population virally suppressed, and proportion of ADAP clients who are enrolled while ineligible.
Model Validation
We validated the model by comparing model output for the years 2017-2019 in the 6-month recertification scenario with empiric data on the average number of enrolled clients, clients disenrolled while eligible per month, clients ruled ineligible per month, program cost, cost per client, and percentage of people virally suppressed at the end of the simulation. We also assessed the monthly number of people in each health state (enrolled in ADAP, disenrolled from ADAP due to failure to recertify, and removed from ADAP due to ineligibility) over time.
Analysis
We simulated the years 2021 through 2025 (5 calendar years) by using the 2017-2019 transition probabilities and the study population as of January 1, 2021. To simulate a 12-month recertification, we made 3 concurrent changes to the model:
We halved the probability of disenrollment to simulate people being removed for failure to recertify half as often.
We added an additional health state that represented ADAP clients who became ineligible and would have been removed under the 6-month recertification (Figure 1). People pass through this health state before being removed from ADAP, which occurs with a monthly probability of 1/6. People in this health state also may regain eligibility, which occurs with the same probability as when they are ineligible and outside of ADAP.
For the initial 6 months, no one is removed from the program as everyone would be granted an additional 6 months of eligibility.
We compared the following model outputs from the 6-month and 12-month recertification scenarios: the average number of clients enrolled in ADAP, the total number of clients dropped from ADAP, the total number of clients ruled ineligible for ADAP, the cost of recertification staff, the cost of case management contribution to recertification, the program cost, the annual program cost per client, the cumulative person-years of viral suppression, and the percentage of the population virally suppressed at the end of the simulation.
Sensitivity Analyses
We assessed uncertainty in our model output by using a Monte Carlo simulation. We sampled 10 000 parameter values from the associated probability distributions (Table 1) and simulated 10 000 iterations of the model. Uncertainty estimates were unavailable for 2 parameters: program overhead cost and cost of recertification. Although it is undesirable to rely on arbitrary ranges, we selected a normal distribution with a 95% CI corresponding to ±33% of the mean to represent these values. We anticipated that this range was wide enough to capture all reasonable possible values for these inputs.
We calculated 95% CIs by taking the 2.5th and 97.5th percentile for each outcome metric. We performed a 1-way best-case/worst-case scenario sensitivity analysis of cost with each transition probability and cost parameter at the upper and lower bound of their 95% CIs. The code for our model is available online at https://github.com/sjerly/EconomicMarkov. Data are protected by Washington State law but can be accessed via a data-sharing agreement with the Washington State DOH.
Results
Model Validation
The model output fit closely to program data from 2017-2019 (0%-5% of the empiric data) (eFigure 3 in the Supplement). The model output fit closely to empiric data for viral suppression at the final year (actual, 88.4%; modeled, 88.7%) and total annual program cost per client (actual, $2233; modeled, $2418) but overestimated the program cost by 5% (actual, $26 235 000; modeled, $27 584 000) and underestimated the size of the ineligible population at year 3 by 16% (actual, 1225 people; modeled, 1057 people) and onward.
Cost Analysis
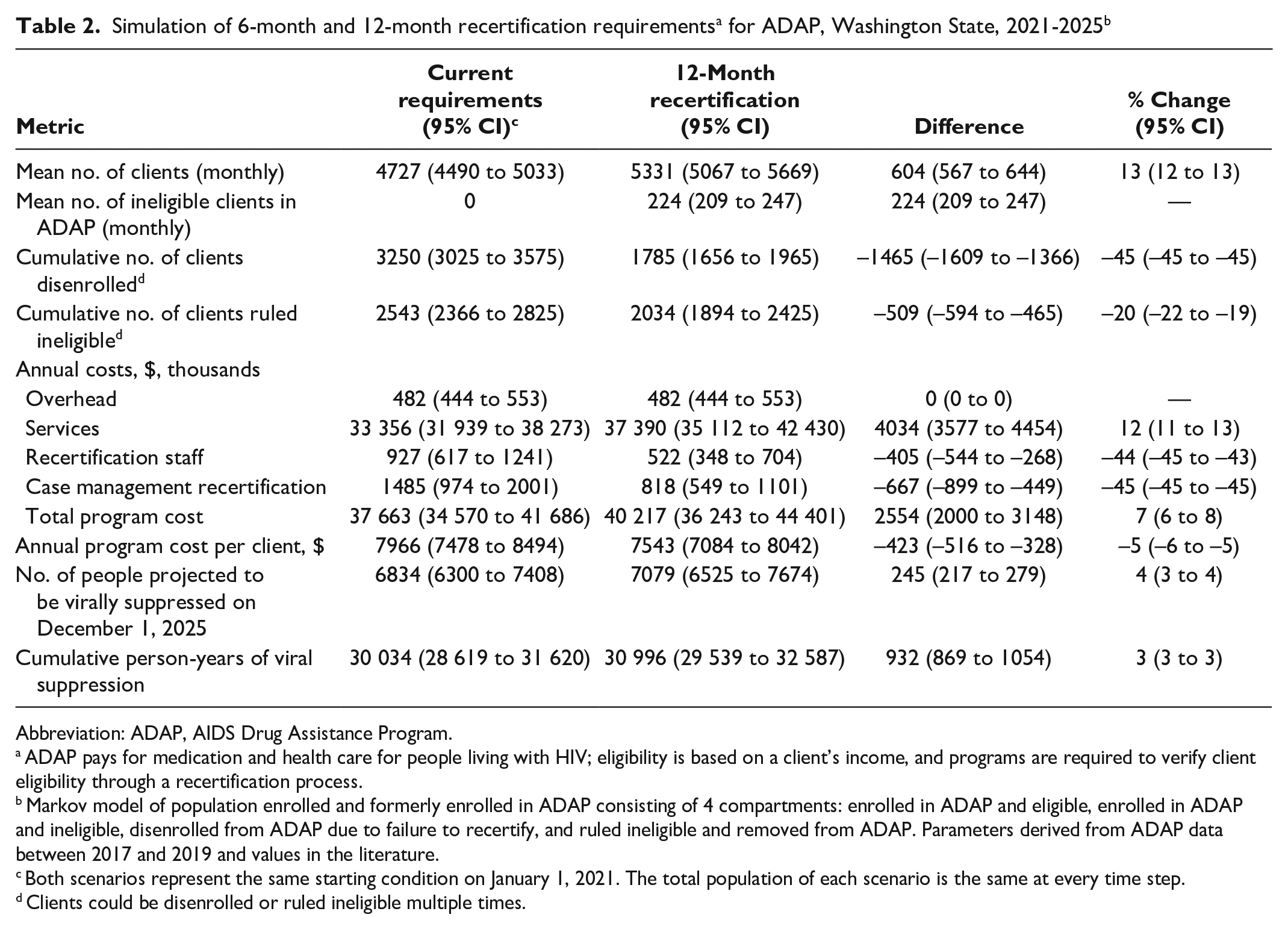
Assuming a continuation of the 6-month recertification criteria, the model estimated that ADAP would enroll 4727 (95% CI, 4490-5033) clients per month at a per-client cost of $7966 (95% CI, $7478-$8494) during the next 5 years (Table 2). At the end of the 5-year period, we estimated that 6834 (95% CI, 6300-7408) ADAP clients would be virally suppressed. The total cost of the program to the Washington State DOH was estimated to be $37 663 000 (95% CI, $34 570 000-$41 686 000). In the 12-month recertification scenario, ADAP was projected to enroll 5331 (95% CI, 5067-5669) clients per month at a per-client cost of $7543 (95% CI, $7084-$8042). At the end of the 5-year period, 7079 (95% CI, 6525-7674) clients were projected to be virally suppressed. The total cost of the program to Washington State DOH would be $40 217 000 (95% CI, $36 243 000-$44 401 000). The disaggregated costs by category and year (Table 3) and a visual comparison are presented (eFigure 4 in the Supplement).
Abbreviation: ADAP, AIDS Drug Assistance Program.
ADAP pays for medication and health care for people living with HIV; eligibility is based on a client’s income, and programs are required to verify client eligibility through a recertification process.
Markov model of population enrolled and formerly enrolled in ADAP consisting of 4 compartments: enrolled in ADAP and eligible, enrolled in ADAP and ineligible, disenrolled from ADAP due to failure to recertify, and ruled ineligible and removed from ADAP. Parameters derived from ADAP data between 2017 and 2019 and values in the literature.
Both scenarios represent the same starting condition on January 1, 2021. The total population of each scenario is the same at every time step.
Clients could be disenrolled or ruled ineligible multiple times.
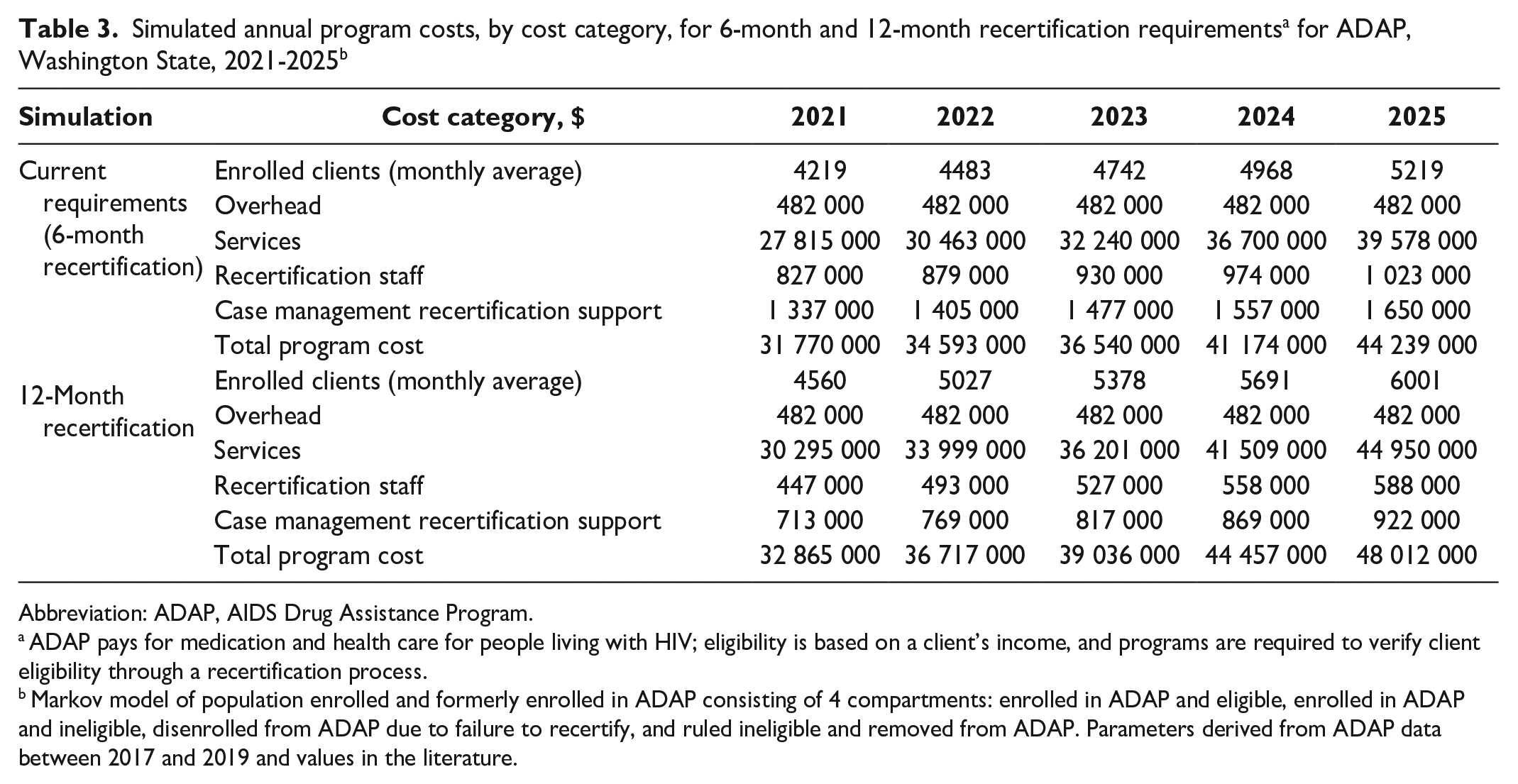
Abbreviation: ADAP, AIDS Drug Assistance Program.
ADAP pays for medication and health care for people living with HIV; eligibility is based on a client’s income, and programs are required to verify client eligibility through a recertification process.
Markov model of population enrolled and formerly enrolled in ADAP consisting of 4 compartments: enrolled in ADAP and eligible, enrolled in ADAP and ineligible, disenrolled from ADAP due to failure to recertify, and ruled ineligible and removed from ADAP. Parameters derived from ADAP data between 2017 and 2019 and values in the literature.
In the 5-year simulation, implementing a 12-month recertification instead of a 6-month recertification resulted in an average monthly increase of 13% (95% CI, 12%-13%) for ADAP enrollment, 7% (95% CI, 6%-8%) for program cost, and 4% (95% CI, 3%-4%) for the projected number of people virally suppressed in the model population (Table 2). The 12-month recertification enabled an average of 224 (95% CI, 209-247) clients to be enrolled in ADAP who were ineligible and would otherwise be excluded (4% of enrolled clients; 95% CI, 4%-5%). Under the 12-month recertification schedule, the cost per client was reduced by $423 (95% CI, $328-$516), or 5%, reflecting a lower administrative cost.
Sensitivity Analysis
Our model comparison was robust to changes in transition probabilities and cost parameters in 1-way sensitivity analyses. Results were most sensitive to changes in the number of new clients added to ADAP each month (cost difference between scenarios: 2.5th percentile, $3 108 000; 97.5th percentile, $2 129 000), the probability of those disenrolled returning to ADAP (cost difference between scenarios: 2.5th percentile, $2 674 000; 97.5th percentile, $2 471 000), and the probability of clients failing to recertify (cost difference between scenarios: 2.5th percentile, $2 876 000; 97.5th percentile, $2 117 000) (Figure 2). The cost difference between the scenarios was greatest when more clients were added each month (creating a larger ADAP), when clients had a greater probability of failing to recertify (increasing the frequency of disenrollment), and when the probability of clients returning to ADAP was low (increasing the impact of disenrollment).
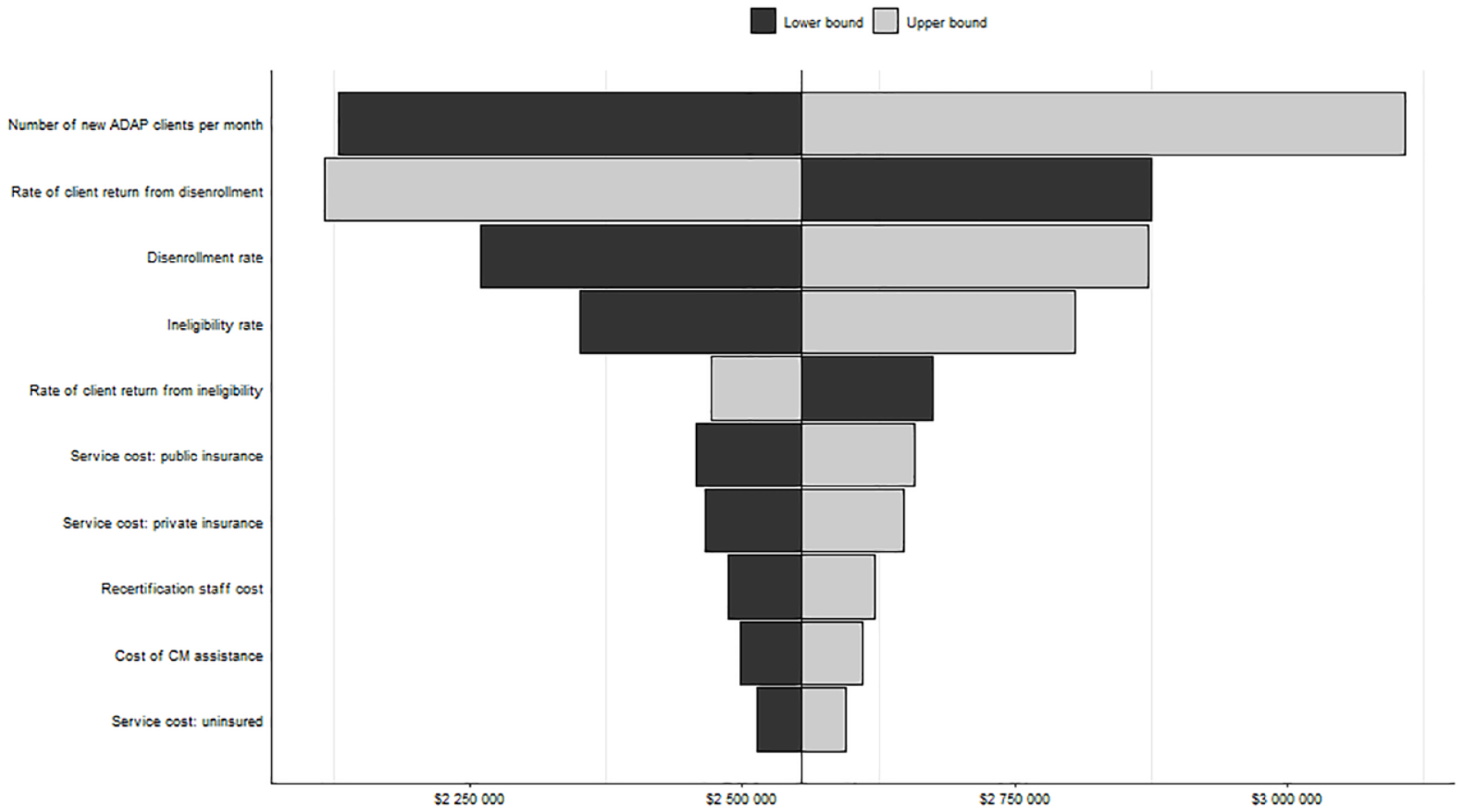
One-way sensitivity analysis of difference in annual ADAP costs, 12-month recertification minus 6-month recertification, Washington State. ADAP pays for medication and health care for people living with HIV; eligibility is based on a client’s income, and programs are required to verify client eligibility through a recertification process. The length of the bars represents the difference in ADAP costs between the 12-month and 6-month scenarios when the individual parameter is varied. The parameters were drawn from associated probability distributions, and the range from the 2.5th and 97.5th percentiles are displayed.
Discussion
Our analysis projected that extending the ADAP recertification requirement from a 6-month to a 12-month schedule can increase the number of people virally suppressed in Washington State at a modest increase in cost. A 12-month recertification program was projected to cost less per client served with only a small increase in ineligible clients who remained in ADAP in Washington State. In the 12-month recertification scenario, the administrative costs associated with the recertification process decreased while the costs of continued coverage for PLWH who were no longer eligible increased.
While our study is, to our knowledge, the first analysis to evaluate a change in ADAP recertification criteria, our results are similar to evaluations of Medicaid, which suggest that 12-month continuous eligibility policies for children’s programs lead to better health outcomes and lower administrative costs compared with more frequent eligibility updates.12,13 For Medicaid programs in general, cyclical disenrollment and reenrollment are associated with high administrative costs and poor health outcomes.12,15 Modeling analyses have estimated that continuous Medicaid eligibility would improve the stability of health care coverage at only a modest increase in cost (1.8% increase in average length of enrollment and 2.2% increase in cost).12,13 ADAPs and Medicaid serve similar roles in providing health care for low-income people who would not otherwise be able to access it; the health and cost impact of changes to Medicaid enrollment would likely be similar to what would be expected in ADAP. Our sensitivity analyses showed that the cost changes associated with a 12-month recertification schedule do not change greatly when modifying any single parameter.
Population viral suppression proportions are a convenient way to measure the effect of a policy change, but they do not capture all the public health benefits of the recertification scenarios; there are additional benefits of a 12-month recertification schedule that were not included in our model. In Washington State, the 6-month ADAP recertification requirement leads to disproportionate disenrollment of PLWH who are Black, young, or lack health insurance. 6 A change to the recertification requirement represents a structural intervention to improve health equity. Our model also does not encompass health conditions other than HIV or the effect of viral suppression on HIV transmission risk. Incorporating these indirect effects would increase the health benefits of 12-month recertification.
Limitations
Our analysis had several limitations. First, our model assumed that people within the same health state were homogenous in their health states, health care costs, and enrollment rates, which is likely an oversimplification of the population who disenroll. People may leave ADAP for different reasons and may have differing access to medical care outside the program. These differences may cause our model to overestimate the number of people who return to ADAP if a subset of people does not want to return to the program. Second, our model did not account for changes to the recertification process beyond the frequency of the process. For example, a 12-month recertification process may give case managers more time to help clients with enrollment activities, which could improve recertification rates (but increase the cost of recertification). Our choice of a 5-year time horizon limited our ability to make claims about the long-term effect of a change in recertification policy but acknowledges the long-term uncertainty in the health care landscape and HIV care in the United States. 16 Third, our validation model underestimated the number of ineligible former ADAP clients by a substantial amount (16%). During the 3-year validation period, this population appeared to grow nonlinearly and outpaced our model. Because the population of ADAP clients is finite and people can transition to ineligibility only through ADAP enrollment, we do not expect this nonlinear increase to continue through 2025. However, if our estimate for the probability of ADAP clients becoming ineligible is too low, our estimates for the size and cost of ADAP in the future may be inflated.
Conclusions
In Washington State, the recertification requirement for ADAP presents a substantial barrier to health care access and contributes to racial and socioeconomic disparities in viral suppression.6,7 Our results suggest that a change in policy from a 6-month to a 12-month recertification requirement would result in a more efficient ADAP with lower administrative costs and a larger population served. This change could improve HIV health outcomes at a modest cost; 245 additional virally suppressed people represent more than 10% of the 13 710 PLWH who were not virally suppressed in Washington State in 2019. 17 Although our simulation was contextualized to Washington State, it is likely to be generalizable to other similar settings; the challenges of the legacy eligibility determination process have been identified in other jurisdictions. 18 With the newfound flexibility granted by the Health Resources & Services Administration in Policy Clarification Notice 21-02, 5 our results support switching to a less frequent recertification process in Washington State.
Supplemental Material
sj-docx-1-phr-10.1177_00333549241227118 – Supplemental material for Cost Analysis of Implementing a 12-Month Recertification Criterion for Ryan White HIV/AIDS Program’s AIDS Drug Assistance Program in Washington State
Supplemental material, sj-docx-1-phr-10.1177_00333549241227118 for Cost Analysis of Implementing a 12-Month Recertification Criterion for Ryan White HIV/AIDS Program’s AIDS Drug Assistance Program in Washington State by Steven Erly, Julia C. Dombrowski, Christine Khosropour, Jennifer R. Reuer, Kandis Boersema and Monisha Sharma in Public Health Reports
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: J.C.D. has conducted research with supplies donated from Hologic, Cepheid, and Mayne Pharmaceuticals. C.M.K. has received donations of research supplies from Hologic, Inc. for activities outside of the submitted work.
Funding
The authors received the following financial support for the research, authorship, and/or publication of this article: J.C.D.’s and C.M.K.’s work was supported by the University of Washington/Fred Hutch Center for AIDS Research, a National Institutes of Health (NIH)–funded program under award no. AI027757, which is supported by the following NIH institutes and centers: National Institute of Allergy and Infectious Diseases, National Cancer Institute, National Institute of Mental Health, National Institute on Drug Abuse, Eunice Kennedy Shriver National Institute of Child Health and Human Development, National Heart, Lung, and Blood Institute, National Institute on Aging, National Institute of General Medical Sciences, and National Institute of Diabetes and Digestive and Kidney Diseases.
Supplemental Material
Supplemental material for this article is available online. The authors have provided these supplemental materials to give readers additional information about their work. These materials have not been edited or formatted by Public Health Reports’s scientific editors and, thus, may not conform to the guidelines of the AMA Manual of Style, 11th Edition.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.