
Abstract
Objectives:
Food insecurity is linked to poor sexual health outcomes, especially among persons engaged in sexual behaviors that are associated with the risk of acquiring sexually transmitted infections (STIs). We examined this link using nationally representative data.
Methods:
We used data on adolescents and adults aged 15-44 who reported sexual activity in the past year from 6 years (September 2011–September 2017) of cross-sectional, weighted public-use data from the National Survey of Family Growth. We compared data on persons who did and did not report food insecurity, accounting for demographic characteristics, markers of poverty, and past-year STI risk indicators (ie, engaged in 1 of 4 high-risk activities or diagnosed with chlamydia or gonorrhea).
Results:
Respondents who reported at least 1 past-year STI risk indicator were significantly more likely to report food insecurity (females: adjusted risk ratio [ARR] = 1.63; 95% confidence interval [CI], 1.35-1.97; P < .001; males: ARR = 1.46; 95% CI, 1.16-1.85) than respondents who did not report food insecurity. This finding was independent of the association between food insecurity and markers of poverty (≤100% federal poverty level [females: ARR = 1.46; 95% CI, 1.23-1.72; P < .001; males: ARR = 1.81; 95% CI, 1.49-2.20; P < .001]; if the respondent or someone in the household had received Special Supplemental Nutrition Program for Women, Infants, and Children or Supplemental Nutrition Assistance Program benefits in the past year [females: ARR = 3.37; 95% CI, 2.81-4.02; P < .001; males: ARR = 3.27; 95% CI, 2.76-3.87; P < .001]). Sex with opposite- and same-sex partners in the past year was significantly associated with food insecurity (females: ARR = 1.44; 95% CI, 1.11-1.85; P = .01; males: ARR = 1.99; 95% CI, 1.15-3.42; P = .02).
Conclusions:
Food insecurity should be considered a social determinant of health independent of poverty, and its effect on persons at highest risk for STIs, including HIV, should be considered when planning interventions designed to decrease engagement in higher-risk sexual behaviors.
Keywords
Social determinants of health, such as exposure to violence in the community, 1 neighborhood prevalence of sexually transmitted infections (STIs), 2,3 economic disadvantage, 4,5 and residential segregation by race/ethnicity, 6 can increase a person’s risk of acquiring STIs, including HIV. One way social determinants increase STI/HIV risk is by placing increased stress on the interaction between individual behaviors (eg, condom use, sexual partner selection) and the biological and behavioral factors that drive disease transmission (ie, the epidemiological context in which a person lives). 7 One such social determinant is food insecurity, defined as “limited or uncertain access to nutritionally adequate and safe foods or limited or uncertain availability to acquire such foods in socially acceptable ways.” 8 Although the number of US households reporting food insecurity has declined since 2011 (when it was 14.9%), 11.1% (14.3 million) of households in 2018 still reported being food insecure at some point during the year. 9
A literature review of developing and developed countries found an association between food insecurity and high-risk sexual behaviors that led to an increased likelihood of HIV transmission, decreased access to health care services, decreased adherence to antiretroviral therapy, and poor HIV immunological outcomes. 10 In North America, research examining the link between food insecurity and HIV has focused on HIV-positive persons. 10 -21 The prevalence of food insecurity among HIV-positive persons ranged from 40% 6 to 71% 18,20 across diverse samples (eg, African American persons recently diagnosed with HIV, 11 homeless and marginally housed HIV-infected persons living in a major US city 12 ). These studies found that food insecurity was associated with outcomes specific to persons living with HIV, such as higher HIV-1 viral load, lower mean CD4+ count, 13 and reduced adherence to antiretroviral therapies, 19 as well as to high-risk sexual behaviors or markers of past high-risk sexual behaviors with broad implications for sexual health. These markers of past high-risk sexual behaviors included past history of STIs, concurrent partnerships, nonmonogamous recent partner(s), 11 and sex without condoms. 12,14
Other research conducted in North America has focused on persons characterized as at high risk for contracting HIV because they or their partners are engaged in high-risk sexual behaviors (eg, young female sex workers, 21 persons recently released from prison 22 ). These groups also reported high levels of food insecurity, ranging from 46% 23 to 72%, 21 with food insecurity linked to high-risk sexual behaviors such as exchanging sex for food or resources to get food, 21 -23 decreasing ability to negotiate with clients for condom use during transactional sex, 21 having sex without condoms, 23 and not knowing a partner’s HIV serostatus. 17
To date, only 1 study has used nationally representative data to examine the link between food insecurity and STIs, including HIV, and indicators of STI risk. One study of National Health and Nutrition Examination Survey data from 1999-2012 found that 22% of men aged 20-29 lived in food-insecure households. 24 Compared with men who did not live in a food-insecure household, men who lived in a food-insecure household were more likely to have HIV or herpes simplex virus-2 and more likely to report an STI diagnosis in their lifetime. Although much of the extant work has focused on HIV, further exploration of the association between food insecurity and STI risk is warranted, because (1) persons at risk for STIs are also at risk for HIV and (2) several STIs are associated with serious health complications, particularly if left untreated. 25,26 We build on research examining the links between food insecurity and STI risk by analyzing results for persons from a nationally representative US survey that includes questions on food insecurity and assessments of sexual behaviors and STI/HIV history.
Methods
Respondents
This analysis used 6 years of public-use data (September 2011–September 2017) collected through the National Survey of Family Growth (NSFG). 27 The NSFG includes a broad range of family life and reproductive and sexual health issues and was designed to be generalizable to the US noninstitutionalized, nonmilitary population of adolescents and adults aged 15-44, with oversamples of adolescents and young adults aged 15-24, non-Hispanic black persons, and Hispanic persons. We included in our analyses only respondents who indicated on the survey that they were sexually active (vaginal, oral, or anal sex with a woman or man) during the past year. The Research Ethics Review Board at the National Center for Health Statistics approved the use of these data.
Overall, 16 191 female and 13 320 male adolescents and adults aged 15-44 participated in NSFG data collection during 2011-2017, few of whom were missing data on food insecurity (n = 181 for female respondents; n = 191 for male respondents). Among participants with information on food insecurity, 13 129 female respondents and 10 438 male respondents had been sexually active in the past year and were included in the analyses. A total of 2160 of 13 129 (16.5%) sexually active female respondents and 1189 of 10 438 (11.4%) sexually active male respondents reported food insecurity in the past year. Fewer than 1% of the sexually active sample (79 female respondents, 84 male respondents) were missing data for food insecurity and thus were excluded from analyses.
Measures
Outcome
Respondents were coded as food insecure if they answered yes to either of the following questions: (1) In the last 12 months, did you receive free or reduced-cost food or meals because you couldn’t afford to buy food? or (2) In the past 12 months, were you or any member of your family ever hungry, but you just couldn’t afford more food?
Covariates
We assessed the following characteristics: age (15-24 y, 25-44 y), race/ethnicity (Hispanic, non-Hispanic white, non-Hispanic black, non-Hispanic other), education (<high school degree, high school degree/general education diploma [GED], >high school degree), marital status (married or cohabiting; widowed, divorced, or separated; never been married), residence in a metropolitan statistical area (MSA; principal city of MSA, other MSA, or non-MSA), federal poverty level (FPL) status (≤100%, >100%), past-year work status (full time, part time, did not work), and number of biological or nonbiological (ie, adopted/stepchild/partner’s child/grandchild/niece/nephew/legal ward/foster) children aged <18 living in the respondent’s household (0, 1, ≥2).
Respondents were asked if they or any member of their family residing in their household had received Supplemental Nutrition Assistance Program (SNAP) benefits or Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) benefits in the past year. If they reported receipt of either or both, they were coded as having received food assistance in the past year (yes, no). Respondents indicated whether their past-year sex partners were all of the opposite sex, all of the same sex, or of both the same and opposite sex. Respondents indicated condom use at last vaginal sex or last anal sex with a partner of the opposite sex (female respondents) or same or opposite sex (male respondents; yes, no). Respondents indicated if they had been told by a physician or other medical care provider that they had been diagnosed with chlamydia or gonorrhea, respectively, in the past year (yes, no).
Dependent Variable
In separate questions, respondents were asked if any of the following were true in the past year: taken money or drugs for sex from opposite sex (female respondents) or same or opposite sex (male respondents), had sex with a male injection drug user, had sex with an HIV-positive partner (opposite sex for female respondents or same or opposite sex for male respondents), had a partner who was nonmonogamous (opposite sex for females respondents or same or opposite sex for male respondents), received a diagnosis of chlamydia, or received a diagnosis of gonorrhea. Responses were yes or no. We used responses to these questions to create a new composite variable indicating whether the respondent reported any STI risk indicator in the past year.
Data Analysis Plan
We performed all analyses by using NSFG cross-sectional data sets spanning 2011-2017. We used 6-year survey weights provided by NSFG to represent the US household population aged 15-44. In bivariate analyses, we used the Pearson χ2 test to determine the association between food insecurity and demographic covariates, receipt of food assistance, and sexual behavior variables. We included in adjusted analyses only variables with P ≤ .20. In adjusted analyses, we used logistic regression to determine adjusted risk ratios (ARRs) and 95% confidence intervals (CIs) to examine the association between indicators of STI risk and food insecurity, accounting for key covariates, with P < .05 considered significant. We conducted additional analyses setting the FPL at >200% compared with ≤200%, >300% compared with ≤300%, and >400% compared with ≤400% to determine whether findings persisted for respondents reporting food insecurity at higher income levels. We conducted analyses by using SAS-callable SUDAAN release 11.0. 28
Results
Demographic and Socioeconomic Characteristics and Food Insecurity
Most food-insecure persons were younger, Hispanic or non-Hispanic black, and had lower levels of educational attainment than food-secure persons (Table 1). In unadjusted analyses, respondents were significantly more likely to report food insecurity than to report food security if they were aged 15-24; non-Hispanic black; had <high school degree or a high school degree/GED; were widowed, divorced, or separated or had never been married; were ≤100% FPL, ≤200% FPL, ≤300% FPL, or ≤400% FPL; worked part time or did not work in the past year; had ≤2 children aged <18 living in the household; or received WIC, SNAP, or WIC and/or SNAP benefits in the past year (Tables 2 and 3).
Food insecurity among sexually active female (n = 13 129) and male (n = 10 438) adolescents and adults aged 15-44, by demographic characteristics, food assistance, and sexual behaviors, National Survey of Family Growth, September 2011–September 2017a
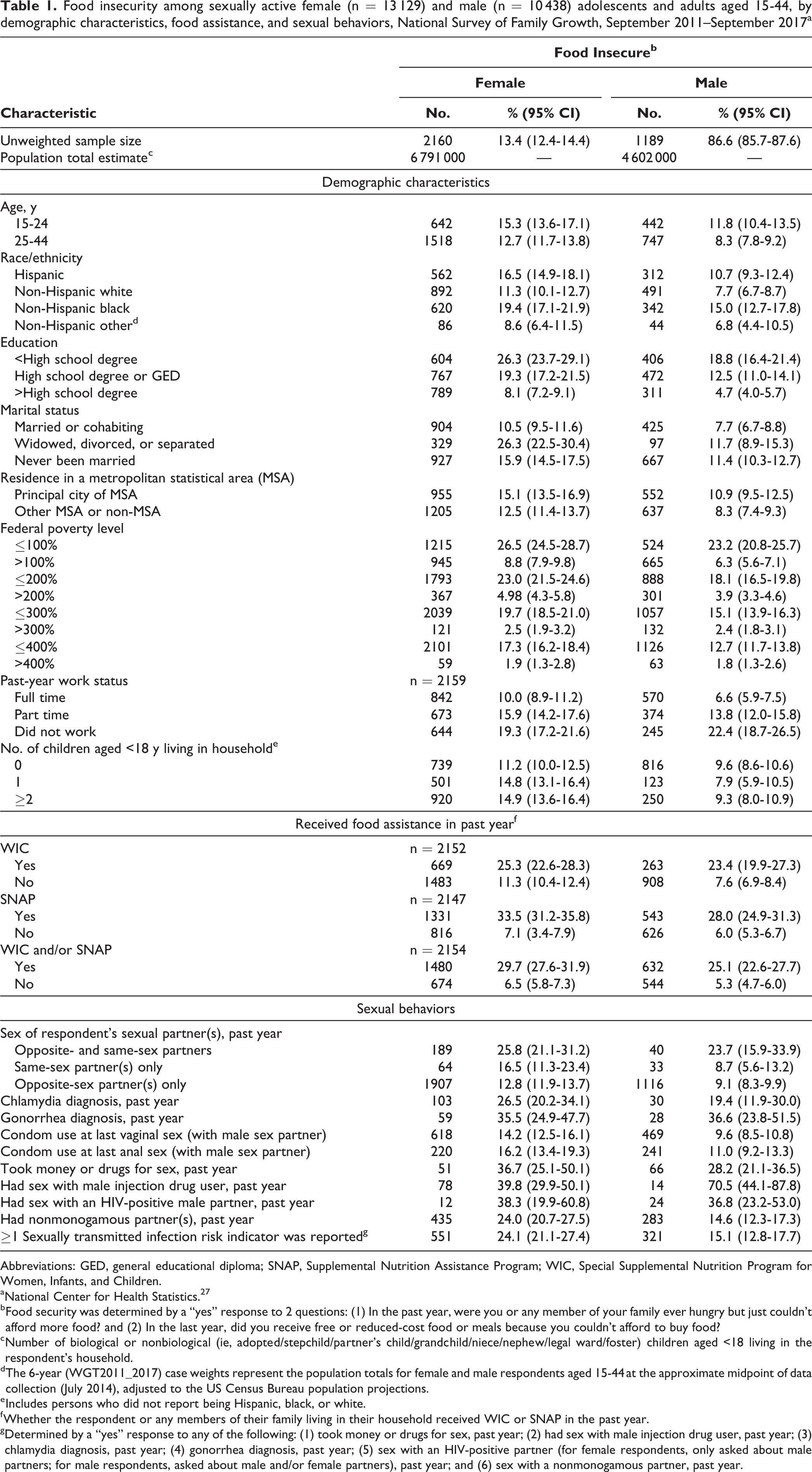
Abbreviations: GED, general educational diploma; SNAP, Supplemental Nutrition Assistance Program; WIC, Special Supplemental Nutrition Program for Women, Infants, and Children.
a National Center for Health Statistics. 27
b Food security was determined by a “yes” response to 2 questions: (1) In the past year, were you or any member of your family ever hungry but just couldn’t afford more food? and (2) In the last year, did you receive free or reduced-cost food or meals because you couldn’t afford to buy food?
c Number of biological or nonbiological (ie, adopted/stepchild/partner’s child/grandchild/niece/nephew/legal ward/foster) children aged <18 living in the respondent’s household.
d The 6-year (WGT2011_2017) case weights represent the population totals for female and male respondents aged 15-44 at the approximate midpoint of data collection (July 2014), adjusted to the US Census Bureau population projections.
e Includes persons who did not report being Hispanic, black, or white.
f Whether the respondent or any members of their family living in their household received WIC or SNAP in the past year.
g Determined by a “yes” response to any of the following: (1) took money or drugs for sex, past year; (2) had sex with male injection drug user, past year; (3) chlamydia diagnosis, past year; (4) gonorrhea diagnosis, past year; (5) sex with an HIV-positive partner (for female respondents, only asked about male partners; for male respondents, asked about male and/or female partners), past year; and (6) sex with a nonmonogamous partner, past year.
Food insecurity among sexually active female adolescents and adults aged 15-44 (n = 13 129), by demographic characteristics, food assistance, and sexual behaviors, National Survey of Family Growth, September 2011–September 2017a
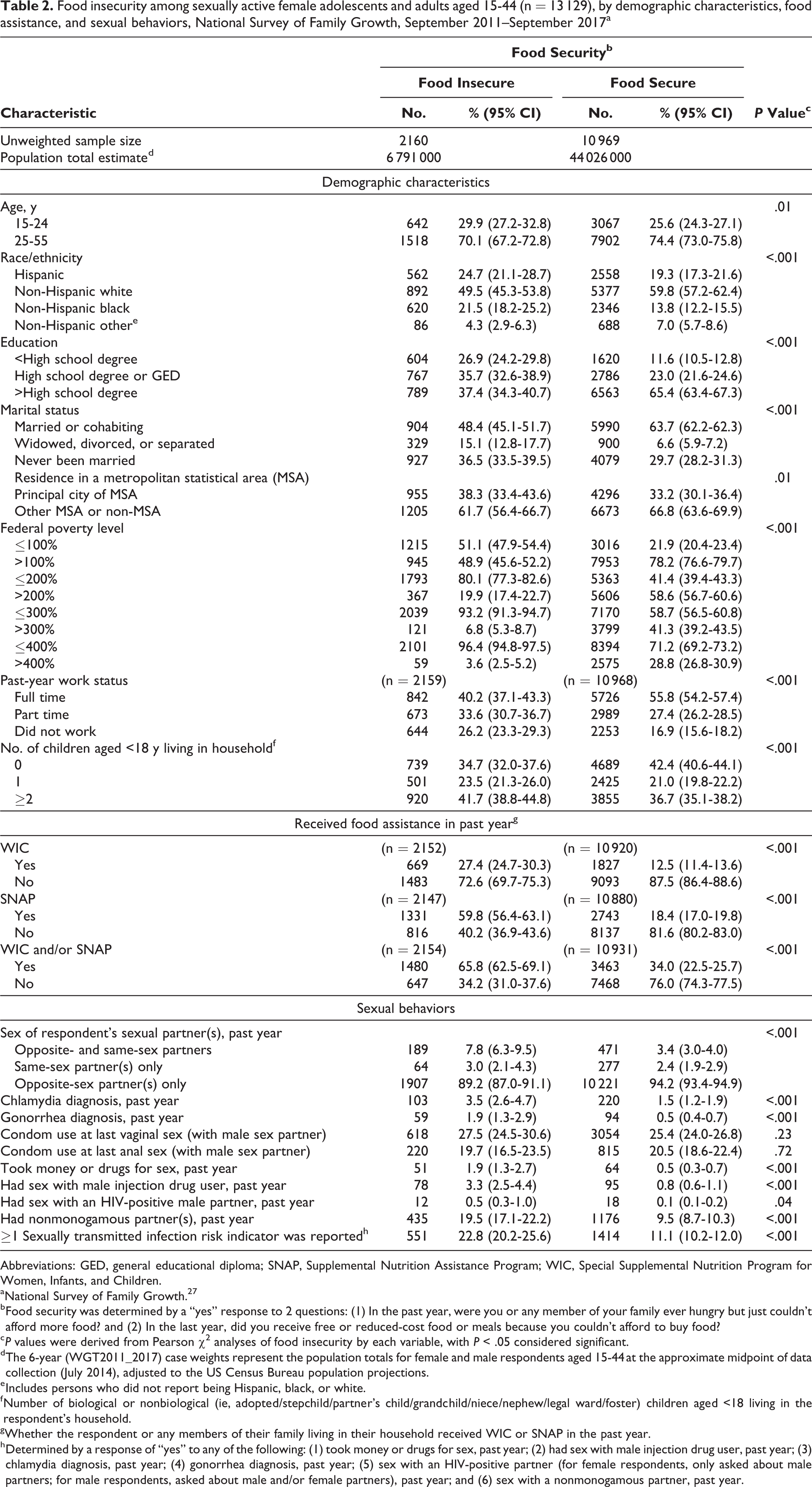
Abbreviations: GED, general educational diploma; SNAP, Supplemental Nutrition Assistance Program; WIC, Special Supplemental Nutrition Program for Women, Infants, and Children.
a National Survey of Family Growth. 27
b Food security was determined by a “yes” response to 2 questions: (1) In the past year, were you or any member of your family ever hungry but just couldn’t afford more food? and (2) In the last year, did you receive free or reduced-cost food or meals because you couldn’t afford to buy food?
c P values were derived from Pearson χ2 analyses of food insecurity by each variable, with P < .05 considered significant.
d The 6-year (WGT2011_2017) case weights represent the population totals for female and male respondents aged 15-44 at the approximate midpoint of data collection (July 2014), adjusted to the US Census Bureau population projections.
e Includes persons who did not report being Hispanic, black, or white.
f Number of biological or nonbiological (ie, adopted/stepchild/partner’s child/grandchild/niece/nephew/legal ward/foster) children aged <18 living in the respondent’s household.
g Whether the respondent or any members of their family living in their household received WIC or SNAP in the past year.
h Determined by a response of “yes” to any of the following: (1) took money or drugs for sex, past year; (2) had sex with male injection drug user, past year; (3) chlamydia diagnosis, past year; (4) gonorrhea diagnosis, past year; (5) sex with an HIV-positive partner (for female respondents, only asked about male partners; for male respondents, asked about male and/or female partners), past year; and (6) sex with a nonmonogamous partner, past year.
Food insecurity among sexually active male adolescents and adults aged 15-44 (N = 10 438), by demographic characteristics, food assistance, and sexual behaviors, National Survey of Family Growth 2011-2017a
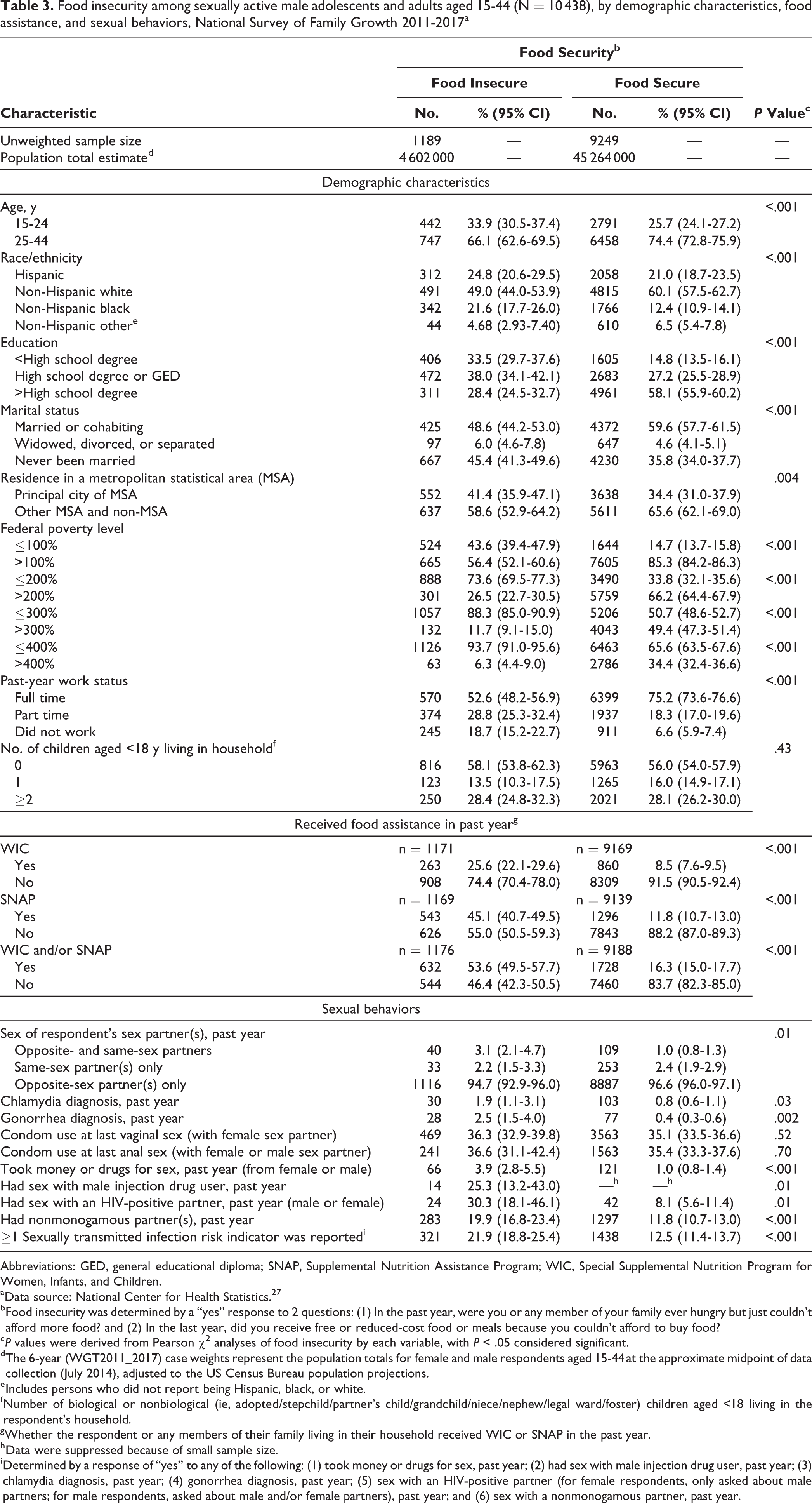
Abbreviations: GED, general educational diploma; SNAP, Supplemental Nutrition Assistance Program; WIC, Special Supplemental Nutrition Program for Women, Infants, and Children.
a Data source: National Center for Health Statistics. 27
b Food insecurity was determined by a “yes” response to 2 questions: (1) In the past year, were you or any member of your family ever hungry but just couldn’t afford more food? and (2) In the last year, did you receive free or reduced-cost food or meals because you couldn’t afford to buy food?
c P values were derived from Pearson χ2 analyses of food insecurity by each variable, with P < .05 considered significant.
d The 6-year (WGT2011_2017) case weights represent the population totals for female and male respondents aged 15-44 at the approximate midpoint of data collection (July 2014), adjusted to the US Census Bureau population projections.
e Includes persons who did not report being Hispanic, black, or white.
f Number of biological or nonbiological (ie, adopted/stepchild/partner’s child/grandchild/niece/nephew/legal ward/foster) children aged <18 living in the respondent’s household.
g Whether the respondent or any members of their family living in their household received WIC or SNAP in the past year.
h Data were suppressed because of small sample size.
i Determined by a response of “yes” to any of the following: (1) took money or drugs for sex, past year; (2) had sex with male injection drug user, past year; (3) chlamydia diagnosis, past year; (4) gonorrhea diagnosis, past year; (5) sex with an HIV-positive partner (for female respondents, only asked about male partners; for male respondents, asked about male and/or female partners), past year; and (6) sex with a nonmonogamous partner, past year.
Bivariate Associations Between STI Risk Indicators and Food Insecurity
Respondents who had been sexually active in the past year were less likely to report food insecurity than respondents who had not been sexually active in the past year (female respondents: χ2 = 7.60, P = .01; male respondents: χ2 = 5.78, P = .02; χ2 = 7.02, P < .001; data not shown).
In unadjusted analyses, respondents were more likely to report food insecurity than to report food security if, in the past year, they had opposite- and same-sex partners, reported a diagnosis of chlamydia or gonorrhea, took money or drugs for sex, had sex with a male injection drug user, had sex with an HIV-positive male partner or had nonmonogamous partner(s), or reported at least 1 STI risk indicator in the past year (Tables 2 and 3).
Multivariable Analyses
In adjusted analyses, female respondents living at ≤100% FPL (vs >100% FPL) were significantly more likely to report food insecurity (ARR = 1.46; 95% CI, 1.23-1.72; P < .001), and female respondents who had worked part time (vs full time) in the past year were significantly more likely to report food insecurity (ARR = 1.39; 95% CI, 1.19-1.63; P < .001; Table 4). If a female respondent or someone in her household had received WIC and/or SNAP benefits in the past year (vs not received these benefits), she was more likely to report food insecurity (ARR = 3.37; 95% CI, 2.81-4.02; P <.001). Female respondents with both opposite-sex and same-sex partners (vs opposite-sex partners only) in the past year were significantly more likely to report food insecurity (ARR = 1.44; 95% CI, 1.11-1.85; P = .01). Female respondents who reported at least 1 STI risk indicator in the past year (vs no risk indicators) were significantly more likely to report food insecurity (ARR = 1.63; 95% CI, 1.35-1.97; P < .001).
Adjusted risk ratio for food insecurity among adolescents and adults aged 15-44, by demographic characteristics, public assistance, and sexual behaviors, National Survey of Family Growth, September 2011–September 2015a
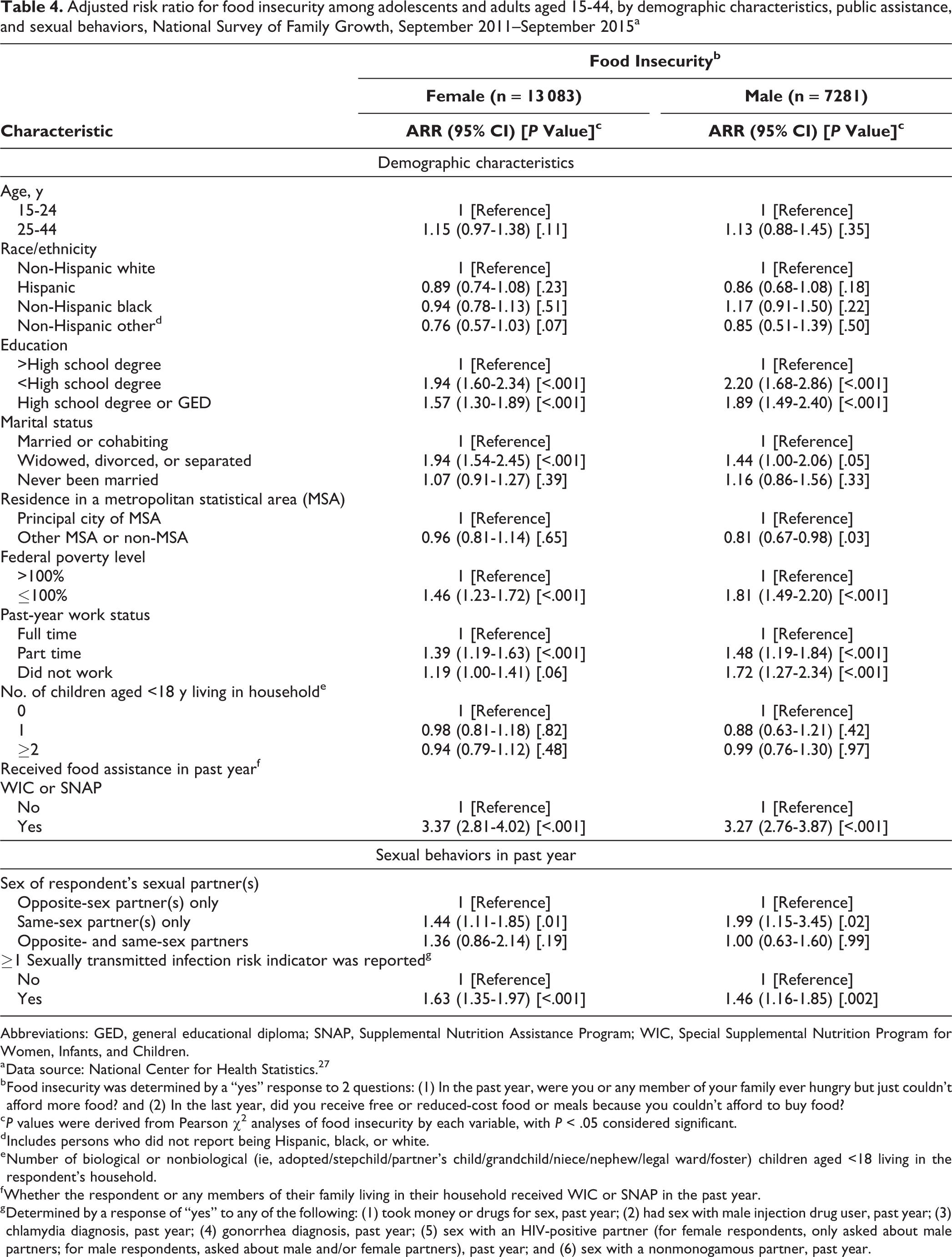
Abbreviations: GED, general educational diploma; SNAP, Supplemental Nutrition Assistance Program; WIC, Special Supplemental Nutrition Program for Women, Infants, and Children.
a Data source: National Center for Health Statistics. 27
b Food insecurity was determined by a “yes” response to 2 questions: (1) In the past year, were you or any member of your family ever hungry but just couldn’t afford more food? and (2) In the last year, did you receive free or reduced-cost food or meals because you couldn’t afford to buy food?
c P values were derived from Pearson χ2 analyses of food insecurity by each variable, with P < .05 considered significant.
d Includes persons who did not report being Hispanic, black, or white.
e Number of biological or nonbiological (ie, adopted/stepchild/partner’s child/grandchild/niece/nephew/legal ward/foster) children aged <18 living in the respondent’s household.
f Whether the respondent or any members of their family living in their household received WIC or SNAP in the past year.
g Determined by a response of “yes” to any of the following: (1) took money or drugs for sex, past year; (2) had sex with male injection drug user, past year; (3) chlamydia diagnosis, past year; (4) gonorrhea diagnosis, past year; (5) sex with an HIV-positive partner (for female respondents, only asked about male partners; for male respondents, asked about male and/or female partners), past year; and (6) sex with a nonmonogamous partner, past year.
In adjusted analyses, male respondents at ≤100% FPL (vs <100% FPL) were significantly more likely to report food insecurity (ARR = 1.81; 95% CI, 1.49-2.20; P < .001; Table 4). Male respondents who had worked part time (ARR = 1.48; 95% CI, 1.19-1.84; P < .001) or not worked (ARR = 1.72; 95% CI, 1.27-2.34; P < .001) in the past year (vs worked full time) were significantly more likely to report food insecurity. If a male respondent or someone in his household had received WIC and/or SNAP benefits (vs not received these benefits) in the past year, he was significantly more likely to report food insecurity (ARR = 3.27; 95% CI, 2.76-3.87; P < .001). Male respondents who reported both opposite-sex and same-sex partners in the past year (vs opposite-sex partners only) were significantly more likely to report food insecurity (ARR = 1.99; 95% CI, 1.15-3.42; P = .02). Male respondents who reported at least 1 STI risk indicator in the past year (vs no risk indicators) were significantly more likely to report food insecurity (ARR = 1.46; 95% CI, 1.16-1.85; P = .002).
Models run with the covariate indicating FPL changed to thresholds of ≤200%, ≤300%, and ≤400% did not significantly affect the direction or magnitude of effects (data not shown).
Discussion
Male and female respondents to NSFG shared many of the same risk factors for food insecurity. Similar to other studies, this analysis also found an association between self-reported food insecurity and STI risk indicators in the United States. 24 This association was extended to both sexes, existed even after accounting for the association between markers of poverty (eg, living at ≤100% FPL, receiving WIC or SNAP benefits), and expanded on findings from research using convenience samples or samples of predominantly high-risk persons by using a nationally representative sample that did not purposively select persons at risk for STIs.
Given the extent to which food insecurity is associated with other indicators of adversity, our analyses were unable to fully explore the pathways between food insecurity and STI risk. However, other research may shed light on this connection. It is possible that the need to procure food may result in transactional sexual encounters expressly or partially enacted to acquire food or the resources needed to procure food. In qualitative work in San Francisco with persons living with HIV/AIDS who were also food insecure, researchers found that food insecurity was linked with risky sex in 2 ways: (1) transactional sex as a way to procure food and (2) having sex without condoms expressly linked to food insecurity. 29 Both women and men described having sex with men so that they could get food or get money to buy food when their food insecurity was severe. In fact, it was generally when they were at their most food insecure (ie, when they did not have access to any food) that they engaged in transactional sex for food procurement purposes. Some participants, though not all, could not always negotiate condom use during transactional sex when their food insecurity was at its most severe, either because they had been offered more money or because hunger made food more of a priority than practicing safer sex. For these participants, the socioeconomic imbalance between partners facilitated risky sex. Echoing this finding of socioeconomic imbalance, among young female sex workers (aged 14-29) in Vancouver, Canada, limited financial ability to afford food was associated with reports of client refusal to use condoms during sexual encounters. 21
Food insecurity has also been linked to depression or depressive symptoms and other affective disorders, 15,16,18,30,31 which have, in turn, been linked to engagement in high-risk sexual behaviors. It may be that increased levels of depression or depressive symptoms in food-insecure persons may result in higher levels of some types of high-risk sexual behavior. For example, even though depression does not seem to be linked to condom use, 32,33 a longitudinal analysis observed that African American men and women who reported high levels of depressive symptoms were more likely to have had ≥6 partners in the past year than men and women who did not report high levels of depressive symptoms. 33 Likewise, among men and women seeking care at a sexually transmitted disease clinic, persons who met cutoff scores for major depressive disorder were more likely to have traded sex for drugs or money in the past 30 days or to report a partner who used injection drugs than persons who did not meet cutoff scores for major depressive disorder. 34 In another longitudinal study of women at risk of HIV acquisition, a consistent pattern of high-risk sexual behavior over time was associated with both food insecurity and depressive symptoms, independently. 23 Although we were not able to examine the influence of depression or its interplay with food insecurity in these analyses, it may be that increased levels of depression or depressive symptoms as a result of food insecurity may be an important pathway through which engagement in high-risk sexual behaviors operates.
Other research has found that men who have sex with men and women may be more likely than men who have sex with men only to engage in high-risk sexual behaviors, such as giving or receiving drugs or money in exchange for sex 35 -37 or having higher rates of condomless sex. 36,37 Men who have sex with men and women are also more likely than men who have sex with men only to report depression 37 and substance use. 37,38 Data on women who have sex with women and men are limited. It may be that psychosocial outcomes associated with a nonheterosexual orientation, such as depression and substance use associated with experiencing stigma, are part of an enmeshed web wherein they interact with social determinants of health such as food insecurity to amplify STI risk for men who have sex with men and women and women who have sex with men.
Limitations
This study had several limitations. First, whereas other analyses used standardized scales to assess food insecurity, such as the US Department of Agriculture’s Household Food Security Survey 39 or Household Food Insecurity Access Scale, 40 only 2 items were used to measure food insecurity in the NSFG. This shortened measure likely underestimated the number of persons classified as food insecure and may reflect a more severe level of food insecurity than might be detected by use of a more nuanced instrument. Although a full scale was not used, a meta-analysis of the association between food insecurity and HIV viral load suppression found that outcomes were consistent even when an attenuated measure of food insecurity was used. 41
Second, our results are generalizable only to adolescents and adults aged 15-44 in US households and, as such, may not appropriately represent some groups at high risk for food insecurity, notably persons who are homeless. Third, because the NSFG is a population-based survey and did not specifically sample for persons at high risk for STI acquisition, the number of persons reporting a diagnosis of chlamydia or gonorrhea in the past year was low, in line with population prevalence, as were rates of engagement in some of the highest-risk sexual behaviors. Low endorsement rates for these items might have reduced the statistical power to detect associations between food insecurity and STI risk, especially as compared with data collections targeting persons at higher risk of STI acquisition.
Fourth, because data were cross-sectional, we could not draw inferences about the direction in which the relationship between food insecurity and STI risk operated, and findings could not be considered causal. Finally, because our composite measure of food insecurity included a question that asked about food assistance but did not specify a source of that assistance (ie, “In the last 12 months, did you receive free or reduced-cost food or meals because you couldn’t afford to buy food?”) alongside variables measuring receipt of SNAP or WIC, an unmeasured correlation could have influenced the results. To address concerns that findings may have been affected by an unmeasured correlation between this item and receipt of food assistance through SNAP or WIC, we also ran models that used only the single item of “In the past 12 months, were you or any member of your family ever hungry, but you just couldn’t afford more food?” to measure food insecurity. However, results did not differ, so we used the composite measure in our analyses.
Conclusion
Our analysis provides additional support for the link between STI risk indicators and reports of food insecurity in the United States. This net association persisted after accounting for markers of poverty and in a nationally representative survey that did not target persons among groups known to be at highest risk for STI and HIV acquisition or currently diagnosed with an STI or HIV infection. Because a substantial proportion of food-insecure respondents lived in households where they or a family member received WIC and/or SNAP benefits, it may behoove local STI prevention partners to work with agencies that offer governmental or nongovernmental food assistance to provide services or linkage to services for STI/HIV care. Furthermore, food insecurity should be considered a social determinant of health independent of poverty, and its effect on persons at highest risk for STIs, including HIV, should be considered when planning interventions designed to decrease engagement in high-risk sexual behaviors.
Footnotes
Authors’ Note
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.