
Abstract
The dramatic racial disparities in the rates of HIV/STIs(sexually transmitted infections) among African Americans make understanding broader structural factors that increase the risk for HIV/STIs crucial. The current study of young 564 African American men attending STI clinics investigated whether those who had ever been incarcerated reported recent sexual behaviors relatively more risky than their counterparts who had never been incarcerated. Participants were recruited from clinics treating STIs in three southern U.S. cities. Males 15 to 23 years of age who identified as Black/African American and reported recent (past 2 months) sexual activity were eligible. Linear mixed-effects models and generalized estimating equation models were used to assess associations between baseline incarceration history and sexual risk behavior over a 6-month follow-up period. Mean age was 19.6 years (SD = 1.87). At baseline, 240 (42.6%) men reported history of incarceration. Incarceration history predicted several risk behaviors over a 6-month follow-up period. Compared with those with no incarceration history, men previously incarcerated reported a desire to conceive a pregnancy (β = .40, p = .02), were less likely to have used a condom at last sex act (odds ratio = .91, p = .02) and were more likely to have used drugs and alcohol before sex in the past 2 months (β = .69, p < .001; β = .41, p < .001). A history of incarceration may influence the sexual risk behavior of young African American males. Prevention programs and interventions should intensify support for postincarceration African American males to help mitigate this behavior.
Keywords
Introduction
In the United States, African Americans continue to be disproportionately affected by the HIV/AIDS epidemic. In the southern United States this remains a major concern (Centers for Disease Control and Prevention [CDC], 2012). Although African Americans represent approximately 12% of the population, they acquire more than 40% of all new HIV infections and account for nearly half of all AIDS diagnoses. Recent data indicate that African American HIV incidence is almost 8 times that of Whites. In 2010, 62% of persons diagnosed with AIDS in the South were African American (CDC, 2012). Individual-level risk factors do not adequately account for racial differences in HIV/AIDS disparity. Instead structural and contextual factors such as poverty and homelessness have been reported to contribute to observed differences in disease status (Adimora & Schoenbach, 2002; Sumartojo, 2000).
Incarceration is one such structural factor that has been associated with sexually transmitted infections (STIs)/HIV transmission (National AIDS Minority Council, 2013; Widman, Noar, Golin, Willoughby, & Crosby, 2013). A study of a national sample of young previously and never-incarcerated men reported that prior to incarceration, no significant differences in sexual behavior existed between the two groups (Knittel, Snow, Griffith, & Morenoff, 2013). Compared with men with no history of incarceration, previously incarcerated men are 3 to 6 times more likely to become HIV-infected (Adimora et al., 2006; Maruschak, 2009).
Incarceration in the United States is highly racialized. One in three African American men born today can expect to go to prison. One in every 15 African American men are already behind bars (Sentencing Project, 2013), making them approximately 2.5 times more likely to be arrested and 5 to 7 times more likely to be incarcerated compared with White counterparts (Carson & Golinelli, 2013). These men are often socially marginalized and represent lower socioeconomic strata. Upon release, coinciding factors such as substance abuse, loss of income, poor health, and interruption of intimate relationships compound preexisting social disadvantage limiting their ability to secure basic needs such as gaining or maintaining housing (Aidala & Sumartojo, 2007), which further increases HIV vulnerability (Aidala, Lee, Abramson, Messeri, & Siegler, 2007; Alabama Department of Public Health, 2012; Shubert, Botein, Wagner, Poulin, & Culhane, 2004; Widman et al., 2013).
The intersection of HIV risk and mass incarceration among African American men is characterized by social and sexual network disruption in their communities. Incarceration results in low male-to-female ratios which in turn increase sexual risk behaviors such as concurrent partnerships, more sexual partners, casual sex, exchange sex, and unprotected sex in community sexual networks (Adimora, Schoenbach, & Doherty, 2007; CDC, 2014; Khan et al., 2011). After leaving incarceration, evidence denotes a hypermasculine focus on desires such as fatherhood and sexual pleasure among recently incarcerated African American men, which may influence noncondom use (Patrick, 2013). These men return to their community and reestablish previous relationships without causing disruption to those established while they were absent. This increases the size of sexual networks with more members who are engaging in HIV/STIs risk behaviors with more people, eventually leading to an increase in the spread of HIV/STIs throughout a community (Potterat, Rothenberg, & Muth, 1999; Potterat, Zimmerman-Rogers, et al., 1999; Rothenberg, Potterat, et al., 1998; Rothenberg, Sterk, et al., 1998).
Few (Widman et al., 2013) studies have examined the influence of incarceration history on sexual risk behavior of young, male African American STI clinic patients despite epidemic levels of incarceration among these men. Furthermore, HIV risk variables may function differently in clinic-attending samples. Evidence has demonstrated an association between STI and HIV transmission (CDC, 2004; Quinn, 1996). High reinfection rates have been identified among male STI clinic patients (Crosby, DiClemente, Charnigo, Snow, & Troutman, 2009). Additionally, STI clinic patients represent a core group that substantially contributes to STI epidemics yet may be accessed readily for interventions. Studies conducted in STI clinic settings, however, disproportionally focus on women. In comparison with women, who may have more sites of care to choose from if they are in need of STI assessment, men have fewer options (Grimley, Hook, DiClemente, & Lee, 2004). Accordingly, the purpose of this study was to determine whether young clinic-attending African American men residing in the southern United States who had ever been incarcerated, reported recent sexual behaviors that were relatively more risky than young African American men who had never been incarcerated.
Method
A purposive sample of young African American men was recruited for participation in an NIH-funded randomized controlled trial of a safer sex intervention program designed for brief delivery in clinics. Recruitment occurred in clinics that diagnose and treat STIs. Inclusion criteria were (a) self-identification as Black/African American, (b) aged 15 to 23 years, (c) engaged in penile–vaginal sex at least once in the past 2 months, (d) not knowingly HIV-positive. After providing assent, research assistants asked young men less than 18 years of age for their permission to contact one parent or guardian to obtain consent for study participation. All other young men provided written informed consent. Young men were then randomly assigned to the control or intervention conditions using a computer-generated allocation procedure. (R Core Team, 2008) Men in the control condition received a 60-minute one-to-one informational session about several aspects of male sexual health. The content and objectives are related only to knowledge acquisition. In addition to this program, those randomized to the control condition received standard-of-care services from the clinic (i.e., provision of free condoms and a brief nurse-delivered counseling message to practice safer sex). Young men randomized to the intervention arm received a 60-minute Focus on the Future program (see Crosby et al., 2009). This theory-based program was explicitly designed to increase the quality and frequency of teen’s condom use within the context of making safer choices regarding partners and sexual behaviors. The study protocol was approved by the institutional review boards at all participating sites.
Recruitment occurred from approximately 2010 through 2012, in a primary site (New Orleans, Louisiana) and two secondary sites (Baton Rouge, Louisiana and Charlotte, North Carolina). Of 896 young men screening eligible in New Orleans, 550 enrolled (61.3%). Of 121 young men screening eligible in Baton Rouge, 57 enrolled (52.7%). Unfortunately, records of study refusals for the Charlotte site were not available; however, 95 young men were enrolled. Of the enrolled 702 eligible young men, 564 responded to the self-report baseline question assessing incarceration history.
Measures
Assessment of participants occurred at baseline and at 2-month and 6-month follow-up. At each assessment, participants completed an audio–computer-assisted self-interview assessing sociodemographic characteristics and behavioral and psychosocial factors. The behavioral outcome measures included unprotected penile–vaginal/penile–anal sex, number of sex partners, sex with male partners, drug and alcohol use preceding sex, and sex in exchange of drugs or money. The psychosocial constructs included desire to conceive a pregnancy. To ascertain STI status, participants provided first-catch urine specimens that were assayed for Chlamydia trachomatis and Neisseria gonorrhoeae. Incarceration history was assessed using the question, “have you ever been incarcerated.”
Data Analysis
Bivariate analysis used t tests for continuous sexual risk behaviors and contingency table analysis for dichotomous sexual risk behaviors. Subsequently, a series of linear regression models were used to create age-adjusted associations for continuous sexual risk behaviors. Similarly, a series of logistic regression models were used to create age-adjusted associations for dichotomous sexual risk behaviors. Significance was defined by an alpha of .05. Linear mixed-effects models and binary generalized estimating equations models were conducted to control for repeated within-subject measurements and allow for a number of observations on participants longitudinally. These models examined the independent contribution of incarceration history at baseline—with age, education, marital status, income level, housing, age at first sex, and intervention group as covariates—on each outcome over a 6-month follow-up period. Intervention group was included as a covariate to control for any effects the prevention program may have had on participants’ behaviors
Results
Participant Characteristics
The mean age of the sample was 19.6 years (SD = 1.87; range = 15-23 years). Of those 18 years and older, more than half (78.9%, N = 405) reported earning $1,000 or less per month and 88.2% (N = 45) of those younger than 18 years reported that they qualified for a free or reduced lunch at school. The mean number of lifetime sex partners was 18.4 (SD = 19.1) and the mean number of sex partners in the past 2 months was 3.0 (SD = 6.2). Sixty-seven percent (N = 376) of the sample reported ever being diagnosed with an STI.
Multivariate Regression Analyses
In cross-sectional analysis, age-adjusted multivariate linear regression analyses revealed that compared with men who had never been incarcerated, men with a previous history of incarceration had a higher frequency of unprotected sex acts (β = .10, p = .02), were more likely to have had sex while under the influence of drugs and alcohol (β = .18, p < .001; β = .13, p < .001), and were more likely to report a desire to conceive a pregnancy (β = .11, p < .001; Table 1). Results of age-adjusted multivariate logistic regression analyses indicated that men previously incarcerated were more likely to have had sex in exchange for drugs and money (odds ratio [OR] = 1.32, p < .001; OR = 2.23, p = .01). Incarceration history was less likely to be associated with having sex with a male in the past 2 months (OR = .51, p = .03; Table 1). There were no significant associations for biologically confirmed STIs or number of sex partners in the past 2 months.
Results for Adjusted Linear and Logistic Multivariate Regression Analyses: Previously Incarcerated Versus Never Incarcerated African American Men Participating in Multicity Safer Sex Intervention, 2010-2012.

Past 2 months.
Either penile–vaginal or penile–anal in the past 2 months.
Generalized Estimating Equation and Linear Mixed-Effects Models
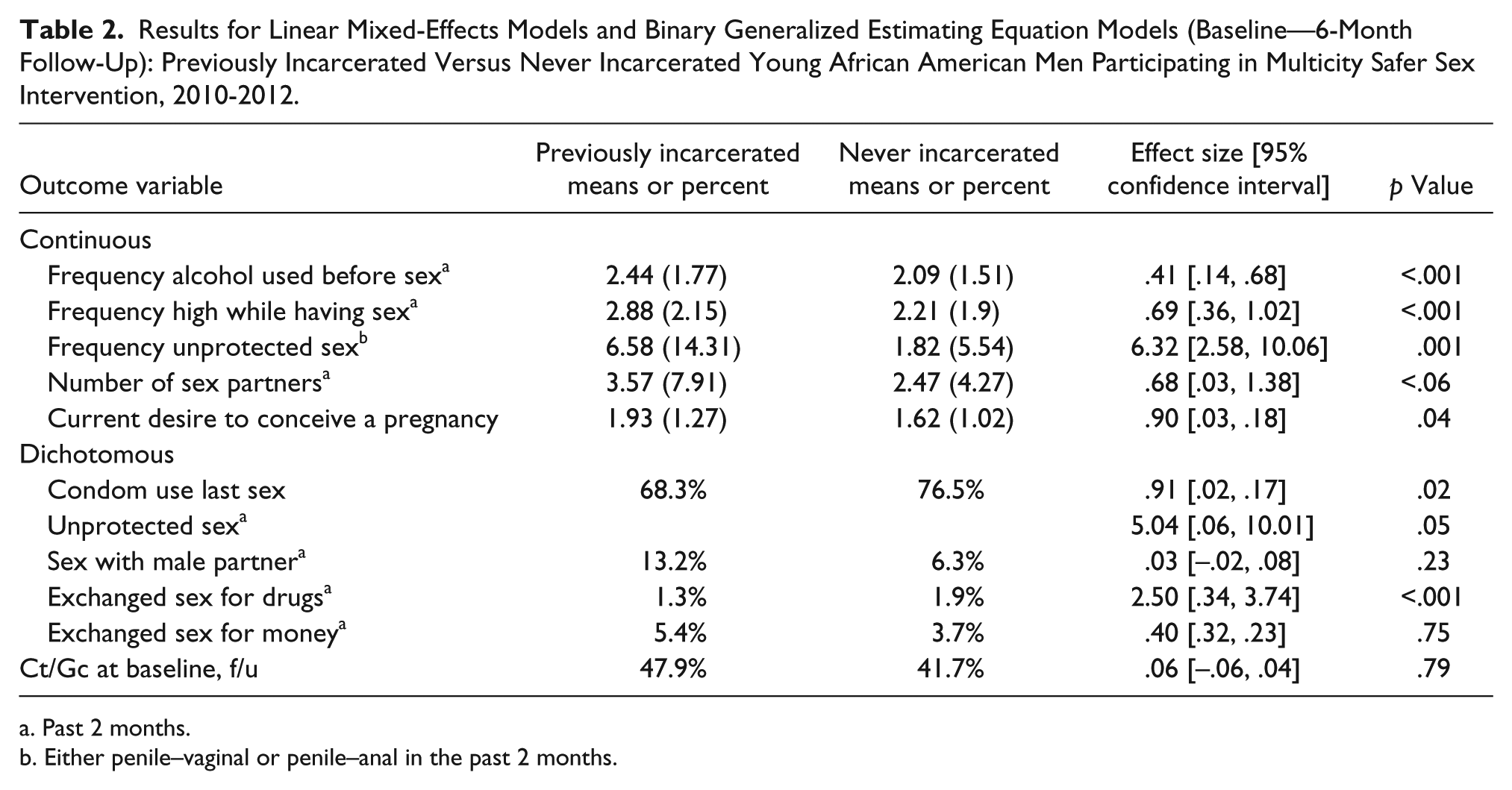
Table 2 displays the results of the generalized estimating equation models. After controlling for age, education, marital status, income level, housing, age at first sex, and intervention group, men who reported a previous history of incarceration at baseline, relative to those who did not, were less likely to have used a condom at last sex act (OR = 0.91, p = .02) and more likely to have exchanged sex for drugs (OR = 2.50, p < .001). Results of linear mixed-effects models indicated that drug and alcohol use prior to sex was predicted by incarceration history (β = .69, p < .001; β = .41, p < .001) as well as, a desire to conceive a pregnancy (β = .90, p = .04). Unprotected sex (penile–vaginal or penile–anal) was significantly more likely among those who had been incarcerated (β = 5.04, p = .05; Table 2). There were no significant associations for STI outcomes, sex with a male partner, number of sex partners, or having sex in exchange for money.
Results for Linear Mixed-Effects Models and Binary Generalized Estimating Equation Models (Baseline—6-Month Follow-Up): Previously Incarcerated Versus Never Incarcerated Young African American Men Participating in Multicity Safer Sex Intervention, 2010-2012.
Past 2 months.
Either penile–vaginal or penile–anal in the past 2 months.
Discussion
This is one of few studies to specifically examine incarceration history as a correlate and predictor of HIV/STI risk behavior among young African American men attending STI clinics. Previous research has primarily examined populations recruited in prison (Arriola et al., 2001; Chen, Bovee, & Kerndt, 2003; Macgowan et al., 2003; Sosman et al., 2011) and community (Khan et al., 2009; Khan, Wohl, et al., 2008) settings. A history of incarceration was common (42.6%). Prior incarceration was correlated with and predicted risky sexual behaviors, even after accounting for the individual factors of age, education, marital status, income level, housing, and age at first sex. These findings contribute to understanding the ways in which structural risk factors contribute to the STI and HIV epidemics among African Americans. For African American men in particular, incarceration has reached epidemic levels (Carson & Golinelli, 2013; Hartney & Vuong, 2009). Therefore, this structural factor in particular deserves significant attention as it presents the potential attribute to the continuation of the disturbing trend of HIV among African Americans.
Overall, participants with a history of incarceration were less likely to consistently use condoms and more likely to use drugs and/or alcohol before sex and to exchange sex for drugs. These results aligned with those of previous research which has demonstrated a link between incarceration and risky behavior (Khan et al., 2009; Khan, Wohl, et al., 2008; Knittel et al., 2013; Macgowan et al., 2003; Sosman et al., 2011). It is noteworthy that even after controlling for intervention group, incarceration history emerged as a significant predictor for risky sexual behavior among this sample of young African American men.
Of interest, incarceration history was linked with current desire to conceive a child. Few existing studies have examined this relationship (Patrick, 2013; Seal, Margolis, Sosman, Kacanek, & Binson, 2003). A study of postrelease providers by Seal and colleagues highlighted perceptions of health care providers who indicated a desire to father children as a determinant of sexual risk behaviors (i.e., concurrent partnerships, lack of condom use) among recently incarcerated men. In a series of interviews with recently incarcerated men, Patrick noted that this desire was an emergent theme that related to masculine self-conceptualization. Future research to further investigate this phenomenon as the critical influence of desire for fatherhood as a contextual factor can influence health behaviors of these men.
Many men in this study reported engaging in high rates of sexual behavior that could put them at significant risk for an STI or HIV. However, multivariate analysis demonstrated that incarceration history was not associated with biologically confirmed STIs. Increased risk for reinfection has been highlighted among clinic-attending populations (Crosby et al., 2009). Although postincarcerated men in this study were not at greater risk for testing positive for STIs, based on STI clinic attendance, these men did perceive themselves at high risk for STIs, but may forgo primary prevention (condom use) for secondary prevention (seeking treatment). McDonald, Thomas, and Eng (2001) noted that the social and cultural contextual experiences of low-income ethnic communities more often frame STI prevention as a calculation of “their risk and take actions based on what they have learned through their own observations and experiences” (p. 624). Moreover, STI outcomes of this study may have been moderated by the average duration of prior incarceration of these men. Previous research noted that short-term incarceration increased risk of infection (Khan, Miller, et al., 2008; Wohl et al., 2000). An important direction for subsequent research is to examine the impact of different durations of incarceration on infection among these young men.
Limitations
Although this study contributes to the mounting evidence that structural factors can increase vulnerability to HIV/STDs, it is not without limitations. As is true for most sexuality research, findings are limited by the validity of self-report. The use of a convenience sample limits the generalizability of the findings to other populations of STI clinic attendees. Also, although this study investigated structural risk factors, only individual-level data were included in analyses. To examine contributions to HIV/STI risk at various levels within an ecological framework, future research should also collect additional data from external sources on contextual factors such as incarceration rates, poverty, and homelessness for use in multilevel modeling. Unfortunately, this study did not measure the duration of incarceration, the number of times incarcerated or the reason for incarceration nor effects of involvement in the criminal justice system without incarceration factored for. These factors have all been reported to influence observed risk behavior.
Conclusion
Findings of the current study suggest several critical HIV/STI prevention needs for African Americans. First, periods of incarceration offer a unique opportunity to provide HIV/STI testing and to deliver postrelease planning prevention messages that focus on high-risk behaviors outside the incarcerated setting. Additionally, HIV interventions should be expanded in community settings to address the prevention needs of women partnered with incarcerated or recently released men. It is also critical to promote primary prevention to young African American men who are STI clinic patients. Without resources and efforts allocated for primary prevention among these men, a continued focus on early detection will perpetuate the current cycle of reinfection. Finally, social policies and population-level interventions that address racial and income disparities in arrests and incarceration and that offer men equal access to resources and opportunities should be encouraged as mechanisms to address factors driving STI racial disparities in the United States.
Footnotes
Acknowledgements
We gratefully acknowledge the assistance of the clinic directors and the clinic staff members.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support for this project was provided by a grant from the National Institute of Mental Health (5R01 MH083621). JaNelle M. Ricks was supported by K12 GM000680 from the National Institute of General Medical Sciences.