
Abstract
Background:
With recent increases in syphilis, there is growing interest in expanding screening; however, treatment rates have historically been low.
Objectives:
This study examines demographic and clinical factors that may contribute to non-completion of syphilis treatment.
Design:
This is a retrospective comparative cohort study of all patients with syphilis from January through November 2018 at an urban, tertiary care hospital.
Methods:
Demographics and clinical information were extracted from the electronic medical record. Descriptive statistics and odds ratios (ORs) were calculated.
Results:
Of 171 patients with syphilis, 89 (52.0%) completed treatment. Patients ages 40–49 were least likely to complete treatment (OR 0.14; 95% CI 0.03–0.72, p = 0.02) compared to those ages 18–24. Non-heterosexual patients were significantly more likely to complete treatment (OR 3.60; 95% CI 1.13–11.49, p = 0.03) compared to heterosexual patients. Patients diagnosed in the emergency department completed treatment at the lowest rate.
Conclusion:
A major gap in syphilis treatment still exists, which must be addressed to achieve optimal impact from syphilis screening programs.
Plain language summary
Rates of syphilis, a common sexually transmitted infection, have been steadily increasing in the United States, now at their highest in decades. Left untreated, syphilis can lead to major health complications, and in pregnant women can cause abnormalities in newborn babies or stillbirth. To address this epidemic, screening programs are being developed to diagnose syphilis in vulnerable populations. However, screening without treatment is not an effective strategy, and historically syphilis treatment rates have been low. This is most likely because the treatment can require a lengthy antibiotic course and often several office visits. In this study, we looked back at the patients diagnosed with syphilis at our hospital for 11 months in 2018 to understand factors that might be associated with a risk of not completing treatment. In this sample, only slightly more than half of patients with syphilis completed treatment. We found that younger patients, patients who didn’t identify as heterosexual, and patients with private insurance were all more likely to complete syphilis treatment. We also found that patients diagnosed in the emergency department completed treatment at the lowest rates. These findings suggest some areas where new strategies can be developed to help support patients with syphilis to get treated. Only with sufficient treatment of patients with syphilis can we make progress on the growing syphilis epidemic.
Keywords
Introduction
The syphilis epidemic is a growing public health crisis in the United States, with more than 207,000 cases reported in 2022, the highest number of cases since 1950, and an increase of 17.3% since 2021. 1 Syphilis disproportionately affects racial and ethnic minority groups. 1 There has been increasing interest in increasing the reach of syphilis screening to improve early diagnosis and address disparities in access to care, but these programs are only effective if patients diagnosed with syphilis also complete treatment. Syphilis can be treated with readily available and affordable antibiotics, either a single dose or three weekly injections of intramuscular penicillin, or an alternative regimen of oral doxycycline. 2 Earlier studies have shown that treatment completion rates among patients diagnosed with syphilis are alarmingly low, 3 with one recent study finding only a 42.9% treatment completion rate among patients with late latent syphilis and syphilis of unknown duration. 4 Barriers to care such as test processing time and distance from residence to clinic have also been associated with failure to complete treatment for gonorrhea and chlamydia. 5 These infections are treated during a single visit, however, and they often are treated empirically during the same visit in which the testing is performed. Treatment of syphilis, in many cases, requires return visits for multiple injections, which may lead to additional or different barriers to treatment completion. Little existing literature addresses this knowledge gap about barriers to treatment specifically in the case of syphilis, which is critical to controlling rising syphilis rates. This study aims to examine demographic and clinical factors that may contribute to non-completion of syphilis treatment in order to better focus future syphilis treatment efforts.
Methods
A retrospective comparative cohort study was performed examining all adult patients with a positive syphilis screen from January through November 2018 at a large, urban, tertiary care hospital. Patients were tested at clinician’s discretion following the standard of care, as no formal screening program was in place. All patients ages 18 and older who were tested for syphilis anywhere in the hospital system were eligible for inclusion, however, only patients with confirmed untreated syphilis defined by a combination of test results and clinical history determined from chart review were included. While some patients were tested using only the rapid plasma reagin (RPR), most patients were screened using a reverse sequence algorithm, in which initial testing was via qualitative multiplex flow immunoassay for syphilis IgG, which, if positive, reflexed to RPR testing. If there was a discrepancy between IgG and RPR results, a second treponemal test, the Treponema pallidum particle agglutination assay was performed. Patients with positive IgG but negative reflex testing were excluded, as this was considered a negative test. Patients with known prior treated infection were excluded unless there was a four-fold rise in RPR titer or the clinical notes indicated the treating physician believed the patient had a new infection.
Patient demographics (age, race/ethnicity, gender identity, sexual orientation, pregnancy status), insurance status, location of testing (e.g. emergency department (ED), inpatient ward, Labor and Delivery, and outpatient clinic), information about concurrent testing and diagnosis of other sexually transmitted infections (STIs), and completion of syphilis treatment were extracted from the electronic medical record (EMR). Treatment completion was defined as a record of administration of all medication doses deemed necessary by the treating clinician, documented patient report of receiving all doses of medication, or an appropriate prescription provided in cases of treatment with oral medications. Any patients not meeting these criteria were considered not to have completed treatment.
Statistical analyses/data analysis
For all subjects with confirmed or presumed new syphilis infection, descriptive statistics were calculated, including demographic information, HIV and STI testing, and syphilis treatment completion status. Univariate and multivariate analyses were performed to compare those who completed treatment to those who did not by demographics, clinical factors, and location of testing. In the multivariate models, odds ratios (ORs) were calculated to compare syphilis treatment groups (unadjusted), while controlling for both demographic (age, race, sex at birth, and sexual identity) and clinical attributes (insurance, pregnancy status, and testing location) in the adjusted models. p Values that were less than or equal to 0.05 were considered statistically significant. All analysis was performed in SAS Version 9.4 (SAS Institute, Cary, NC, USA). The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement (see Supplemental Material). 6
Results
During the 11-month study period, 321 patients had positive syphilis IgG or RPR, of which 171 patients were considered to have syphilis (Table 1). Of these, 107 (61.9%) were cis-male and 157 (91.8%) were non-Hispanic Black. Sexual orientation was only documented in the medical record for 65 (38.0%) patients, but of these, 39 (60.0%) identified as heterosexual. People aged 50 or older comprised about half (50.3%) of syphilis diagnoses, followed by those ages 30–39 (20.5%). There were nine pregnant women with confirmed syphilis. The largest proportion of patients (47.4%) had Medicaid, a government-funded insurance program for low-income individuals, followed by Medicare (29.2%), federal health insurance for people 65 or older and some younger people with disabilities, then private insurance (13.5%). Uninsured patients represented 9.9% of the sample. The majority (63.2%) of diagnoses originated in the ED, followed by the primary care clinic (19.3%). Most (76.0%) patients had late latent syphilis or syphilis of unknown duration, with the remainder of those for whom a stage could be determined approximately equally spread among primary, secondary, tertiary, and early latent.
Comparison of patients completing and not completing syphilis treatment by demographics, HIV and STI testing, location of testing, and other clinical factors from January through November 2018.
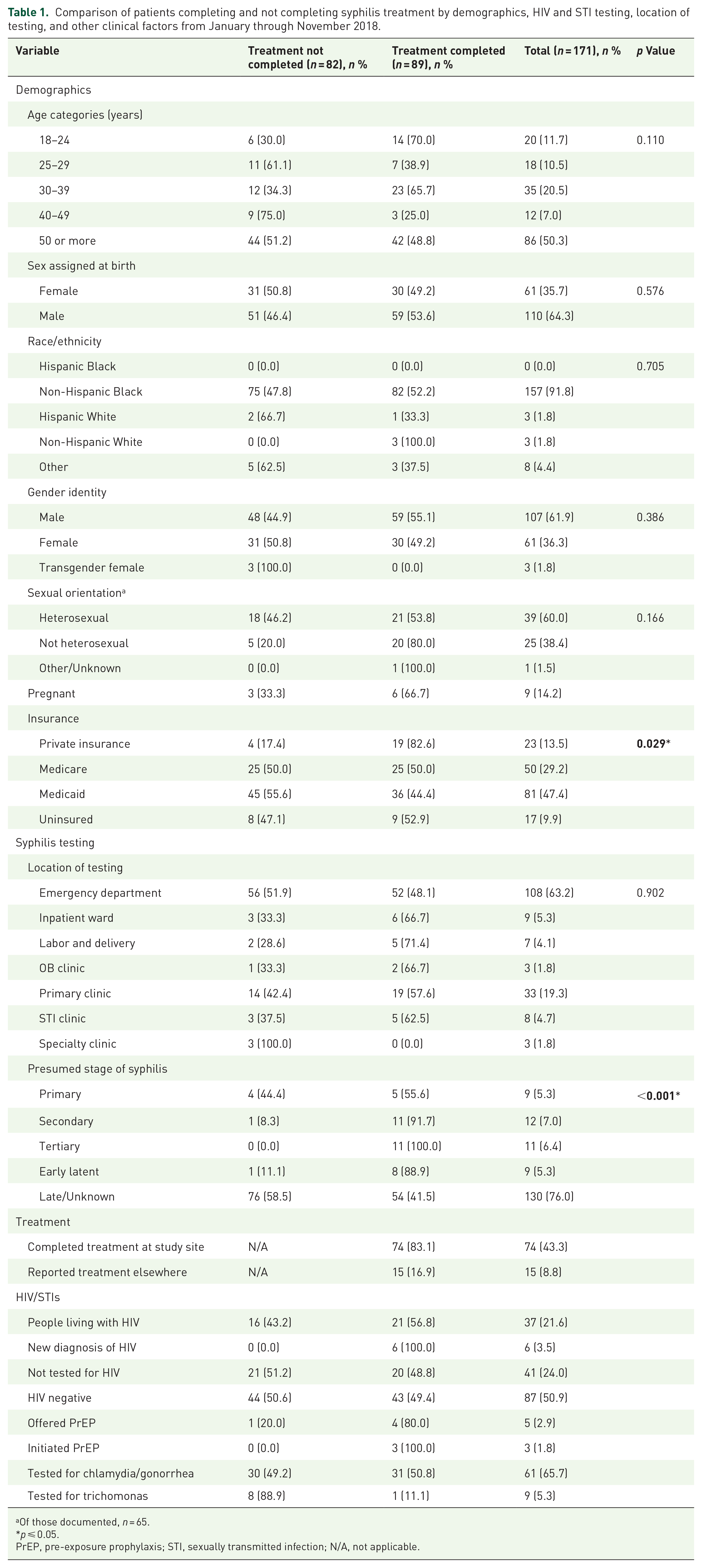
Of those documented, n = 65.
p ⩽ 0.05.
PrEP, pre-exposure prophylaxis; STI, sexually transmitted infection; N/A, not applicable.
People living with HIV comprised 37 (21.6%) of patients with syphilis. Of 134 people who did not have a known HIV diagnosis, 93 (69.4%) were tested for HIV, and 6 (4.5%) were concurrently diagnosed with HIV and syphilis. Notably, only 5 (3.7%) patients without HIV were offered HIV pre-exposure prophylaxis (PrEP), of whom three started PrEP. Patients were tested for gonorrhea/chlamydia at slightly lower rates (65.7%) and trichomonas at a much lower rate (5.3%), resulting in four diagnoses of chlamydia, seven of gonorrhea, and one case of trichomonas. Among female patients, testing for other STIs was much less common. Of 57 women without HIV found to have syphilis, only 39 (68.4%) were tested for HIV, of whom none were diagnosed with HIV. Only 19 (31.2%) women were tested for chlamydia and gonorrhea and 4 (6.6%) for trichomonas. Only one woman without HIV was offered PrEP, and she declined.
Overall, 89 patients (52.0%) either completed syphilis treatment within the same hospital system or reported treatment elsewhere. Of these, 54 were treated with penicillin, 19 with doxycycline, and 18 with unknown regimens. Women and men completed treatment at about equal rates. Patients ages 40–49 were the least likely to complete treatment (OR 0.14; 95% CI 0.03–0.72, p = 0.02) compared to the youngest age group 18–24, which was the most likely to complete treatment (Table 2). Patients who did not identify as heterosexual were significantly more likely to complete treatment (OR 3.60; 95% CI 1.13–11.49, p = 0.03) than those who identified as heterosexual. Patients with private insurance were most likely to complete treatment (OR 4.22; 95% CI 1.00–17.8, p < 0.05), while those with Medicaid were least likely, even less so than uninsured patients. Patients diagnosed in the ED had the lowest proportion of treatment completion (48.1%), followed by primary care (57.6%), and the ED was the only testing location with fewer patients completing treatment than not. However, the association between location of testing and treatment completion was not statistically significant. There was no significant association between likelihood of treatment completion and race, sex, or pregnancy status. In the adjusted multivariate analysis, the associations between likelihood of treatment and age, sexual orientation, and insurance remained, and the association of patients aged 25–29 with low likelihood of treatment completion became statistically significant (adjusted OR 0.10; 95% CI 0.02–0.56, p < 0.01), compared to patients ages 18–24, after controlling for demographic and clinical factors.
Multivariate analysis of sociodemographic factors and testing location associated with syphilis treatment completion among patients with confirmed syphilis from January through November 2018.

OR, odds ratio; STI, sexually transmitted infection; N/A, not applicable.
p ≤ 0.05.
Labor and delivery/Obstetrics and Gynecology.
While reasons for lack of treatment completion were frequently not documented, 7 (4.1%) patients were referred to an affiliated clinic or back to their own primary care physician and it is unknown if they completed treatment, 4 (2.3%) were documented as unable to be reached at all, and 7 (4.1%) did not show up for follow-up appointments, six of whom received a first dose of penicillin in the ED or during an inpatient stay but never returned to finish their treatment course.
Discussion
As syphilis continues to increase in the United States, efforts are being made to implement and expand screening programs.7,8 However, screening must be accompanied by treatment for a program to be effective. Infections left untreated may lead to further transmission to others, as well as significant morbidity and mortality over time. This study found that only just over half of patients diagnosed with syphilis at a large, urban, academic medical center were confirmed or self-reported to have completed treatment. Younger patients, those reporting sexual orientations other than heterosexual, and patients with private insurance were most likely to complete treatment. Previous studies have not found any demographic factors significantly associated with likelihood of STI treatment completion.5,9 While a retrospective review is unable to determine the reasons for loss to follow-up (LTFU), these findings may reflect greater awareness and less stigma around STIs among younger 10 or non-heterosexual 11 patients, and private insurance may represent a proxy for patients who have the financial means to return for treatment or maintain a telephone for result notification.
Most syphilis diagnoses in this study originated in the ED, but patients diagnosed in the ED least often completed treatment, with several even receiving a first dose of penicillin but not returning to complete the course of treatment. While there is limited published data about treatment completion rates for syphilis, studies of gonorrhea and chlamydia screening in ED populations have shown fairly high LTFU, ranging from 15.9% to 66.7% of ED patients with positive gonorrhea or chlamydia testing not returning for treatment. 12 ED patients can be very difficult to reach after discharge for result notification, 13 may be affected by social determinants of health limiting their ability to access outpatient follow-up, 14 or may be reluctant to engage with hospital staff after their visit if they do not have an established relationship such as with a primary care clinic. This is reflected in the fact that only 51.8% of ED patients with syphilis completed treatment, by far the lowest treatment completion proportion of any site.
Importantly, 63.2% of syphilis diagnoses originated in the ED, emphasizing the urgency of developing and improving infrastructure to increase linkage to care for ED patients. This is consistent with published data demonstrating a large proportion of urogenital STI diagnoses originate in the ED. 15 Expansion of rapid point-of-care testing 16 might also afford the opportunity to provide a diagnosis, counseling, and linkage to care while patients are still in the ED. Additional strategies that have since improved treatment rates in the study ED include the institution of a partner clinic within the hospital to provide outreach and linkage to care support 17 and the implementation of an EMR alert for patients unable to be reached who then re-present to the ED, allowing results to be addressed at the next ED visit.
Similar studies in the inpatient or outpatient primary or specialty care setting are rare, and the LTFU rate is unknown. Because these are settings in which the patient may have an established relationship or made an appointment for testing, it might be presumed that the LTFU rate would be quite low. However, this study suggests that treatment rates in non-ED settings are also much lower than expected. This may in part reflect the burden of weekly in-person visits for 3 weeks required for syphilis treatment. While intramuscular penicillin is the gold standard for treatment, if patients are unable to complete this treatment, alternative treatment strategies such as doxycycline, which does not require return clinic visits, should be investigated. Given concerns about adherence to lengthy antibiotic regimens, more research is needed to understand ideal treatment regimens to support optimal patient adherence. Additional resources, staff, and infrastructure are needed to help both hospitals and health departments engage patients in treatment.
An incidental finding of this study was the low rate of co-testing for HIV and other STIs alongside syphilis testing. While syphilis is a well-known risk factor for HIV, only 79.1% of syphilis patients without HIV were tested for HIV. Of these, a staggeringly high proportion of 5.7% were newly diagnosed with HIV at the time of their syphilis diagnosis. Of those without HIV, only 3.7% were offered PrEP, which would have been indicated as a result of their syphilis diagnosis. 18 Among women, these numbers were even lower, with only 68.4% of HIV-negative women with syphilis tested for HIV, and only one woman offered PrEP. While the limitations of a chart review make it difficult to know if lack of HIV testing was attributable to patient preference or clinician discretion, this finding suggests a need for improved patient and clinician education around HIV screening and prevention, targeted outreach surrounding the importance of HIV screening and prevention in women, and perhaps a role for automated EMR reminders for HIV testing19,20 triggered by syphilis or other STI testing. Similar trends were found in rates of testing for urogenital STIs, with again much lower rates of testing among women. However, 12 urogenital STIs were diagnosed among 61 patients tested, again suggesting the need for education and technological support to encourage comprehensive STI testing in any patient suspected to have or diagnosed with an STI.
Limitations
This is a single-site study at an academic medical center, and it is unknown if the results are generalizable to other settings. Retrospective reviews are inherently limited by what was documented in the clinical record. If no reason for LTFU was documented, there was no way to infer or investigate the individual patient outcomes or the factors that may have affected treatment completion, including severity of illness or other behavioral factors. For this same reason, data on sexual orientation was also missing for many patients in the study. Lastly, it is possible that some of the patients did complete treatment at another hospital or clinic. Due to the lack of an accessible centralized treatment data repository, it is impossible to ascertain treatment data not recorded in the EMR, and there is limited availability of post-treatment laboratory testing to confirm successful treatment.
Conclusion
In this study of all patients with syphilis at a large, urban, academic medical center, slightly more than half reported or were confirmed to have completed treatment. A large proportion of syphilis cases were diagnosed in the ED, and these were also the least likely to complete treatment. These findings suggest the need for more robust infrastructure to support rapid diagnosis and linkage to care, collaboration with local health departments to provide a central data repository for syphilis treatment information, more resources devoted to contacting patients and arranging treatment, and novel strategies to leverage existing technology to reach patients diagnosed with syphilis. These changes are urgently needed to improve syphilis treatment rates in tandem with expansion of syphilis screening programs, which will maximize the effectiveness of testing to impact the ongoing syphilis epidemic.
Supplemental Material
sj-docx-1-tai-10.1177_20499361241265941 – Supplemental material for Risk factors for treatment non-completion among patients with syphilis
Supplemental material, sj-docx-1-tai-10.1177_20499361241265941 for Risk factors for treatment non-completion among patients with syphilis by Abigail Clarkson-During, Ellen Almirol, Dylan Eller, Aniruddha Hazra and Kimberly A. Stanford in Therapeutic Advances in Infectious Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.