
Abstract
Objectives:
Despite a push for increased local public health capacity, no clear baseline for performance of local health departments (LHDs) exists. The objectives of this study were to quantify the self-reported performance of LHDs on the 10 Essential Public Health Services (EPHSs) and describe the relationships between performance and characteristics of LHDs.
Methods:
We used data on 2000 LHDs from the 2013 National Profile of Local Health Departments survey to develop principal components analysis–based scores to evaluate each LHD on the performance of EPHSs. Scores ranged from 0 to 100. LHDs that performed no activities within an EPHS had a score of 0, and LHDs that performed all activities within an EPHS had a score of 100. We explored the relationships between EPHS scores and LHD characteristics by using multivariate linear regression and cluster analysis.
Results:
Performance scores varied greatly by LHDs and EPHSs; however, LHDs typically scored <50, indicating that they performed fewer than half of the activities evaluated. LHDs that served larger populations (vs smaller populations) and LHDs that had higher per-capita funding (vs lower per-capita funding) had higher EPHS scores. We identified 6 EPHS performance score–based LHD clusters, which suggests similarities in which EPHSs LHDs focused on.
Conclusions:
Our results suggest weaknesses in many LHDs’ fulfillment of the EPHSs, particularly in low-population and low-funding settings. LHDs should be given the resources to increase capacity and ensure the EPHSs are met in communities.
Keywords
The public health infrastructure in the United States comprises a network of federal, state, and local health agencies intended to work in concert. 1,2 The effectiveness of this system relies on agencies at each level having the capacity to complete the required tasks. 3 In 1994, the Public Health Functions Working Group defined the 10 Essential Public Health Services (EPHSs) that serve as a benchmark for public health practice (Table 1). 4 Fulfillment of the EPHSs by local health departments (LHDs) is vital, because LHDs are the most proximal health agencies to the communities they serve. 1,2 However, the current literature suggests that the capacity of LHDs varies greatly and may be weak overall. 1,7 -17
Activities, in order of importance, that best capture performance of the Essential Public Health Servicesa and the combined variance in the activities used that is explained by the principal component, 2013 National Profile of Local Health Departments Surveyb
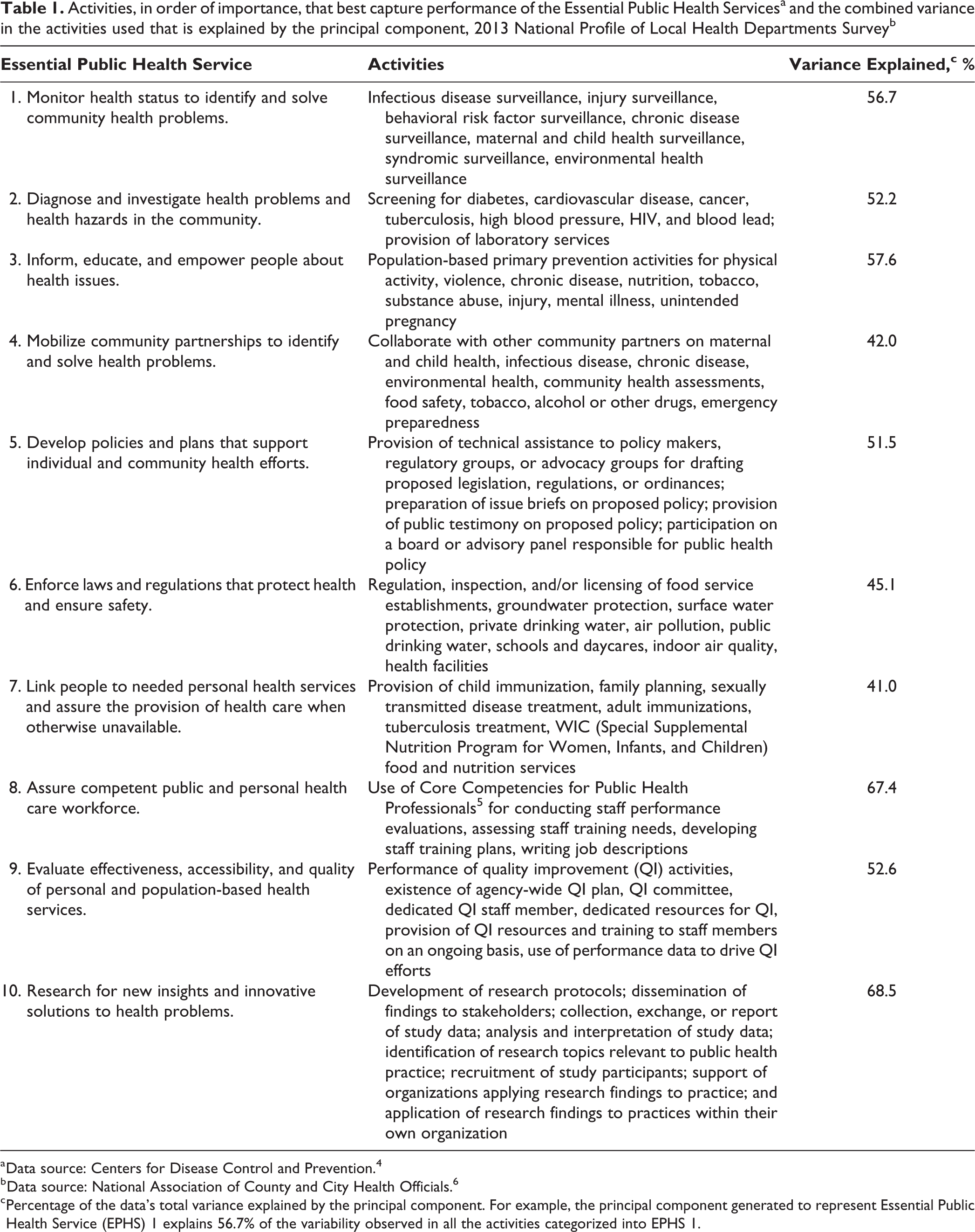
a Data source: Centers for Disease Control and Prevention. 4
b Data source: National Association of County and City Health Officials. 6
c Percentage of the data’s total variance explained by the principal component. For example, the principal component generated to represent Essential Public Health Service (EPHS) 1 explains 56.7% of the variability observed in all the activities categorized into EPHS 1.
Concerns about lack of capacity have led to a push for public health infrastructure improvements through programs such as Healthy People 2020 and health department accreditation. 18,19 However, many Healthy People goals are unmet, and only 209 LHDs had achieved accreditation as of November 20, 2018, with many indicating that the time and effort are too high for the benefit. 20 -24 In addition, no clear baseline for performance of LHDs exists. Studies investigating the performance of LHDs tend to focus on the most populous cities or health departments that opted into programs such as the National Public Health Performance Standards Program and, hence, may overestimate nationwide capacity. 10,12,25,26
In this study, we evaluated the self-reported capacity of LHDs by using scores derived from principal components analysis (PCA). We quantified the performance of 2000 LHDs on each of the 10 EPHSs to objectively measure performance across a heterogeneous group of LHDs. We further explored the relationships between the performance and characteristics of LHDs.
Methods
Study Data
We used data from the National Association of County and City Health Officials (NACCHO) 2013 National Profile of Local Health Departments Survey, which is the largest, most comprehensive source of data on LHD infrastructure and activities in the United States. 6 The NACCHO profile enumerated 2532 LHDs, 2000 (79.0%) of which responded to the NACCHO profile survey. Researchers selected health departments by population-based stratified random sampling to receive only the core questionnaire or the core plus 1 of 2 supplemental modules. The Johns Hopkins Bloomberg School of Public Health Institutional Review Board (IRB) Office determined this study was not human subjects research and did not require IRB oversight.
Measures of EPHS Performance
We categorized reported health department activities into EPHSs based on metrics used in previous health department evaluations. 2,27,28 The number of activities included in each EPHS category varied based on the number of relevant activities for each EPHS available in the data set. Some of the activities used to describe EPHS 4, EPHS 8, EPHS 9, and EPHS 10 came from module 1 of the questionnaire; therefore, the sample size for analysis of these EPHSs was reduced (n = 490). For EPHS 8, assurance of a competent workforce, we focused on the use of the Core Competencies for Public Health Professionals for workforce development. 5 For the purpose of this analysis, we included only activities that were directly performed by the LHDs. We excluded from further analysis LHDs with missing values for that EPHS. For the remainder of the analysis, these combinations of activities served as proxy measures for an LHD’s capacity to provide the EPHSs.
Data Analysis
For each EPHS, we used PCA to derive a score (the principal component) from the activities categorized into each EPHS. We derived these scores from a linear combination of responses that captured most of the variability in the data on that EPHS. Because many variables of interest were discrete, we used polychoric correlation matrices to estimate correlations between the variables of interest. 29 Our analysis focused only on the principal components of each EPHS, which explained an average of 53.5% of the combined variances in the variables used. Activity contributions to the EPHS scores were weighted by factor loadings, which represent the correlations between the activities and the principal component. We highlighted those activities with the largest contribution to the score (ie, those with a correlation >25%) (Table 1). We normalized each EPHS score to range from 0 to 100, such that LHDs performing all activities in a given EPHS would have a score of 100 and LHDs performing none of the activities in a given EPHS would have a score of 0.
We used multivariate linear regression analysis to examine the association between EPHS scores and LHD characteristics shown to be associated with performance in previous studies. 9,11,12,15,30,31 We examined the following characteristics: population size of jurisdiction, per-capita LHD expenditures, presence of a local board of health, and region as defined by the US Census Bureau (Midwest, Northeast, South, West). 32 We also examined health department governance, classifying decentralized structures as “local,” centralized structures as “state,” and combined structures as “shared governance.” We modeled population size and per-capita expenditures on the log scale to maintain a linear relationship with the dependent variables. We accounted for correlations between health departments in the same state by using clustered standard errors.
To determine whether there were natural groupings of LHDs that shared similar strengths and weaknesses, we created clusters based on health department EPHS scores by using Gaussian finite mixture modeling, as implemented in the mclust R package. 33,34 To maximize the number of LHDs considered, we ran the cluster analysis by using only those EPHSs with activities included on the core questionnaire. We identified 6 performance-based LHD clusters. We compared the characteristics of EPHS-based clusters and assessed associations by using the Pearson χ2 and analysis of variance tests of significance. We considered P < .05 to be significant. We analyzed data by using R version 3.3.2. 35
Results
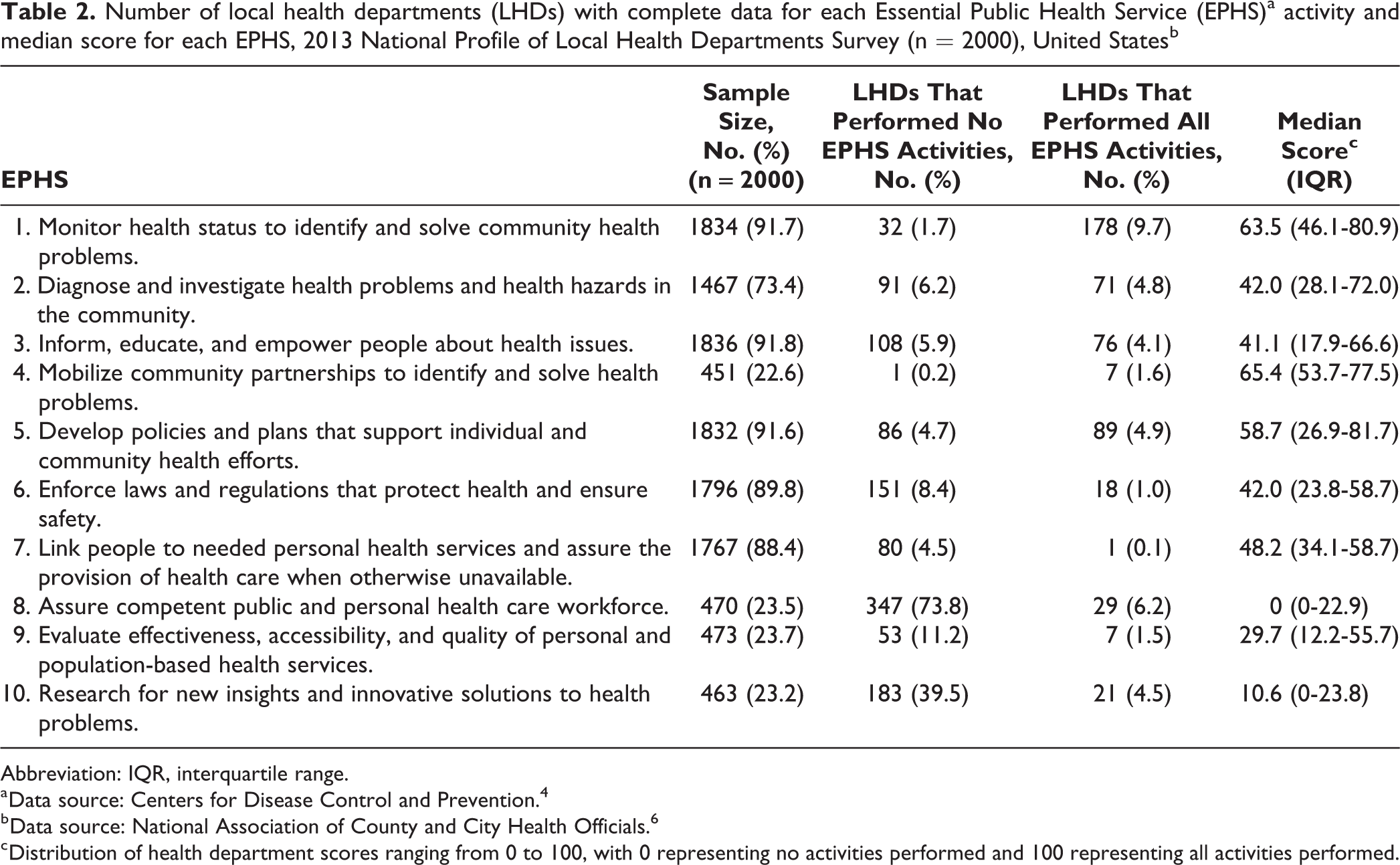
LHDs performed well on EPHS 1; most LHDs scored >50 (Table 2). A typical (ie, scoring closest to the median) LHD performed 4 of 7 surveillance activities and had completed a community health assessment within the previous 5 years. Infectious disease surveillance was the most frequently reported activity (91.2%; 1802 of 1975), and injury surveillance was the least frequently reported activity (27.3%; 522 of 1910).
Number of local health departments (LHDs) with complete data for each Essential Public Health Service (EPHS)a activity and median score for each EPHS, 2013 National Profile of Local Health Departments Survey (n = 2000), United Statesb
Abbreviation: IQR, interquartile range.
a Data source: Centers for Disease Control and Prevention. 4
b Data source: National Association of County and City Health Officials. 6
c Distribution of health department scores ranging from 0 to 100, with 0 representing no activities performed and 100 representing all activities performed.
For EPHS 2, a typical LHD performed 4 of 8 disease screening activities and provided no laboratory services. Tuberculosis screening was the most frequently reported activity (83.7%; 1650 of 1971), and cardiovascular disease screening was the least frequently reported activity (27.3%; 523 of 1915).
For EPHS 3, a typical LHD performed 3 of 9 population-based primary prevention activities and provided food safety education. Food safety education was the most frequently reported activity (73.1%; 1428 of 1954), and mental illness programs were the least frequently reported activity (12.4%; 240 of 1933).
EPHS 4 had the highest median score overall, indicating that most LHDs were working with their community partners (Table 2). A typical LHD coordinated efforts with partners on most topics but rarely reported full collaboration on activities. Emergency preparedness was the most frequently reported collaboration activity (70.1%; 338 of 482), and land use collaboration was the least frequently reported collaboration activity (5.6%; 26 of 468).
For EPHS 5, a typical LHD had strategic and community health improvement plans, but these plans had not been updated in the previous 5 years. They also participated in some policymaking activities but had not passed a new public health ordinance in the past 2 years. Communicating with legislators was the most frequently reported activity (69.4%; 1350 of 1945), and adopting a new public health ordinance or legislation was the least frequently reported activity (36.8%; 719 of 1954).
For EPHS 6, a typical LHD performed 5 of 13 regulatory activities. Regulation, inspection, and/or licensing of food services establishments was the most frequently reported activity (78.5%; 1540 of 1962), and regulation, inspection, and/or licensing of cosmetology businesses was the least frequently reported activity (12.3%; 235 of 1913).
For EPHS 7, a typical LHD performed 8 of 20 health services. Adult immunization was the most frequently reported activity (90.6%; 1789 of 1975), and substance abuse services were the least frequently reported activity (7.4%; 143 of 1940).
EPHS 8 had the lowest scores overall, with a median score of 0 (Table 2). A typical LHD did not use the Core Competencies for Public Health Professionals for any employee hiring or training activities. Use of core competencies for evaluating training needs was the most frequently reported activity (directly performed by 18.9%; 89 of 470), and use of core competencies in job descriptions was the least frequently reported activity (13.4%; 63 of 470).
For EPHS 9, a typical LHD reported informal or ad hoc quality improvement activities, with no consistent resources dedicated to quality improvement. Formal or informal quality improvement activities were reported by most health departments (performed by 88.9%; 424 of 477); however, fewer than half of LHDs reporting quality improvement activities had dedicated resources to quality improvement activities (43.6%; 185 of 424).
LHDs scored poorly on EPHS 10; 39.5% of LHDs performed none of the research activities evaluated (Table 2). A typical LHD performed 1 of 8 research activities. Collecting, exchanging, or reporting data for a study was the most frequently reported activity (performed by 40.4%; 187 of 463), and developing or refining research plans and/or protocols was the least frequently reported activity (12.5%; 58 of 463).
LHDs included in the multivariate analysis had an average population of 155 200 and average per-capita expenditures of $55.54, although both distributions were right skewed (Table 3). Most of the 1511 LHDs included in the multivariate analysis were locally governed (77.0%; n = 1163) and had a local board of health (73.9%; n = 1116).
Characteristics of local health departments that responded to the 2013 National Profile of Local Health Departments Surveya with complete data for Essential Public Health Serviceb score calculation (n = 1511), United Statesa
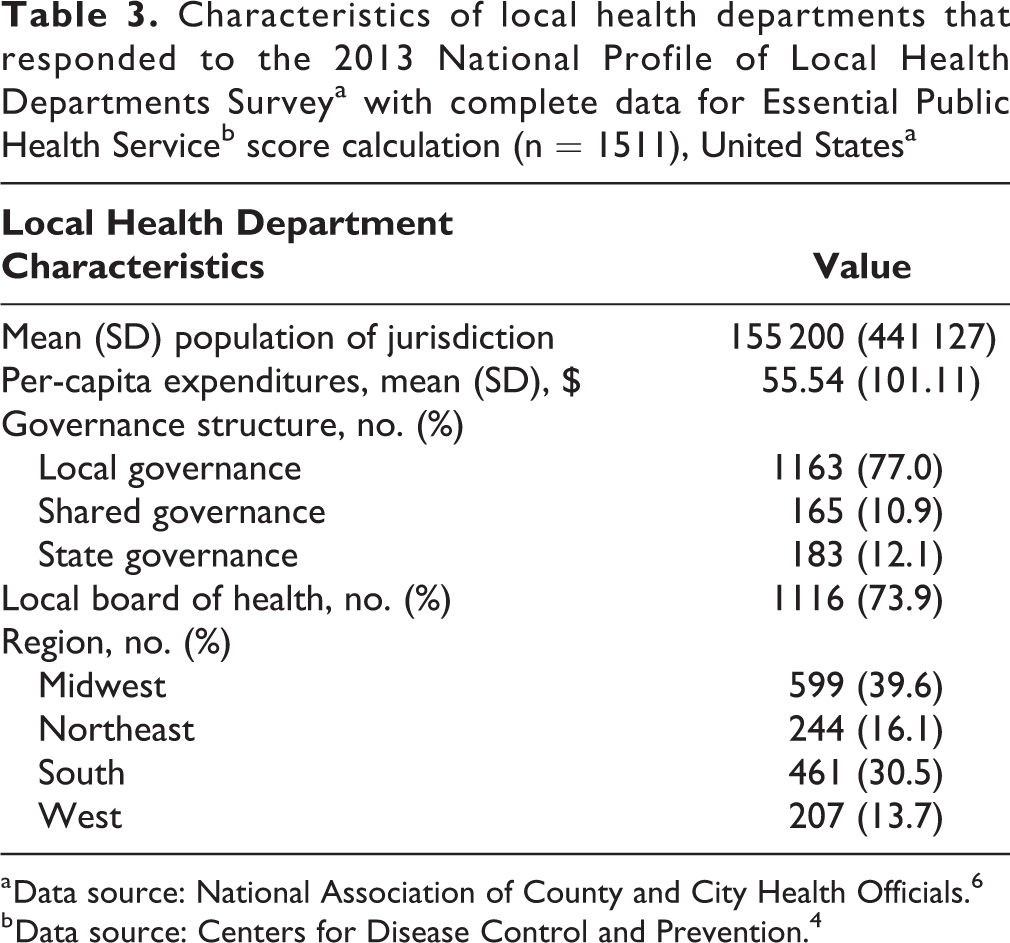
a Data source: National Association of County and City Health Officials. 6
b Data source: Centers for Disease Control and Prevention. 4
LHDs that served larger populations and had more funding tended to have higher EPHS scores than LHDs that served smaller populations and had less funding (Table 4). However, expenditures were unrelated to performance for EPHS 6 or EPHS 8. LHDs with a local board of health scored 3.0 points higher, on average, on EPHS 1 (95% confidence interval [CI], 0.5-6.0), 7.9 points higher on EPHS 3 (95% CI, 3.5-12.3), and 7.5 points higher on EPHS 9 (95% CI, 0.1-14.9) than LHDs with no local board of health.
Associations between Essential Public Health Service (EPHS)a scores and local health department (LHD) characteristics among LHDs that completed the 2013 National Profile of Local Health Departments Survey, United Statesb
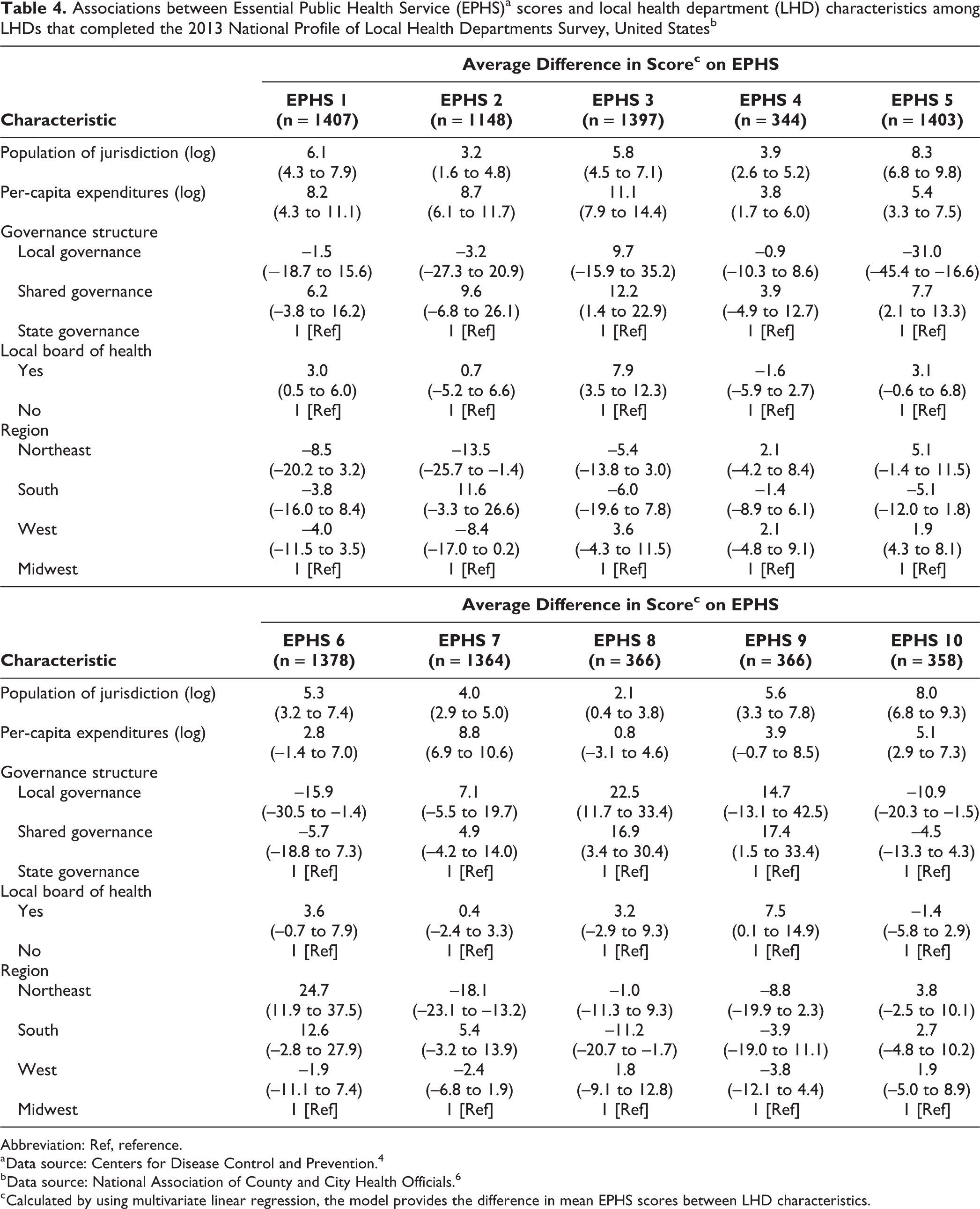
Abbreviation: Ref, reference.
a Data source: Centers for Disease Control and Prevention. 4
b Data source: National Association of County and City Health Officials. 6
c Calculated by using multivariate linear regression, the model provides the difference in mean EPHS scores between LHD characteristics.
State-governed LHDs scored an average of 31.0 points lower on EPHS 5 (95% CI, –45.4 to –16.6), 15.9 points lower on EPHS 6 (95% CI, –30.5 to –1.4), and 10.9 points lower on EPHS 10 (95% CI, –20.3 to –1.5) than locally governed health departments but 22.5 points higher on EPHS 8 (95% CI, 11.7-33.4) (Table 4). Health departments with shared governance scored higher than their locally governed counterparts: 12.2 points higher on EPHS 3 (95% CI, 1.4-22.9), 7.7 points higher on EPHS 5 (95% CI, 2.1-13.3), 16.9 points higher on EPHS 8 (95% CI, 3.4-30.4), and 17.4 points higher on EPHS 9 (95% CI, 1.5-33.4).
LHDs in the Northeast scored an average of 13.5 points lower on EPHS 2 (95% CI, –25.7 to –1.4) and 18.1 points lower on EPHS 7 (95% CI, –23.1 to –13.2) than LHDs in the Midwest (Table 4). However, compared with LHDs in the Midwest, LHDs in the Northeast scored 24.7 points higher on EPHS 6 (95% CI, 11.9-37.5) and LHDs in the South scored 11.2 points lower, on average, on EPHS 8 (95% CI, –20.7 to –1.7).
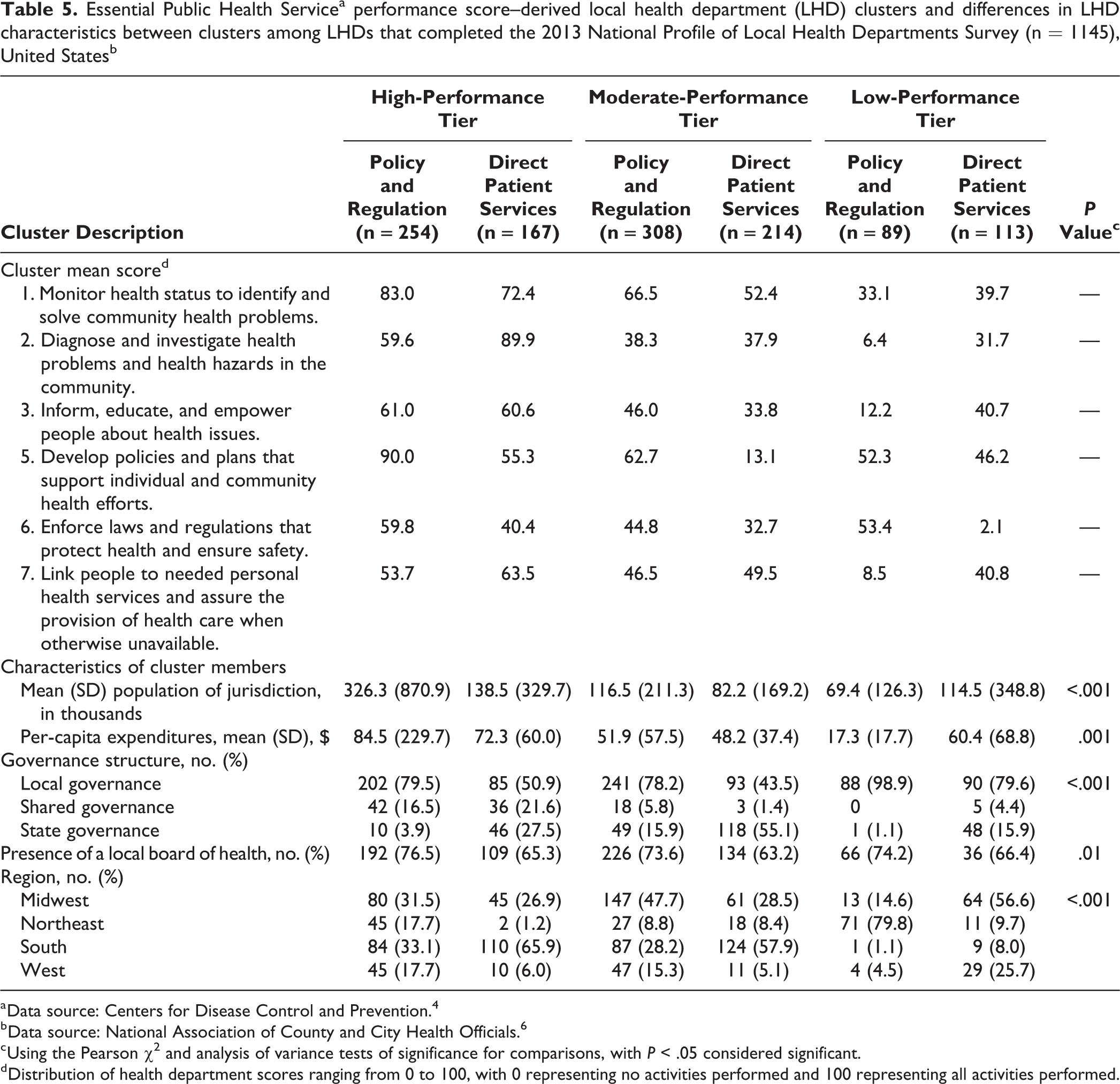
Of 6 performance-based LHD clusters, 2 had high mean EPHS scores, 2 had moderate EPHS scores, and 2 had low mean EPHS scores (Table 5). With few exceptions, high-scoring clusters had higher mean scores across all EPHSs. However, within scoring tiers, health departments could be divided between those that emphasized policy and regulation (eg, EPHS 5 and EPHS 6) and those that emphasized direct patient services (eg, EPHS 2 and EPHS 7).
Essential Public Health Servicea performance score–derived local health department (LHD) clusters and differences in LHD characteristics between clusters among LHDs that completed the 2013 National Profile of Local Health Departments Survey (n = 1145), United Statesb
a Data source: Centers for Disease Control and Prevention. 4
b Data source: National Association of County and City Health Officials. 6
c Using the Pearson χ2 and analysis of variance tests of significance for comparisons, with P < .05 considered significant.
d Distribution of health department scores ranging from 0 to 100, with 0 representing no activities performed and 100 representing all activities performed.
The LHD clusters differed significantly by size of the population served; LHDs in the high-performance tier had the largest mean populations, and LHDs in the low-performance tier had the smallest mean populations (P < .001) (Table 4). Clusters also differed significantly by per-capita expenditures; LHDs in the high-performance tier spent the most overall (P < .001). The clusters differed significantly in their governance classifications; policy and regulation clusters tended to be more frequently locally governed than those that emphasized direct patient services (P < .001). In addition, the policy and regulation clusters were more likely to have a local board of health than were the direct patient services clusters (P = .01). The clusters also differed by their regional makeup; LHDs in the low-performance tier policy and regulation cluster were mostly in the Northeast, LHDs in the high- and moderate-performance tier direct patient services clusters were mostly in the South, and LHDs in the low-performance tier direct patient services cluster were mostly in the Midwest (P < .001).
Discussion
Our analysis indicates that LHDs have room for improvement on EPHS performance. Most health departments performed fewer than half of the activities that are key to the EPHSs. However, performance varied widely, with high performers and low performers in each EPHS category. On average, LHDs reported the highest performance in monitoring population health, mobilizing community partnerships, and developing public health policies. Health departments had the lowest scores overall for assuring a competent workforce, evaluating population-based health services, and performing research. Most health departments (73.8%) scored zero on EPHS 8, indicating that they do not use the Core Competencies for Public Health Professionals in any workforce recruitment or development activities. 5
Findings from the multivariate model support previous studies that show health department performance increases with the size of the population served and per-capita health department spending. 9,11,12,15,30,31,36 The governance structure of LHDs had an interesting relationship with EPHS performance scores. State-governed health departments had significantly lower scores in local policymaking, enforcement of laws and regulations, and research than did locally governed health departments. However, state-governed health departments had significantly higher scores than locally governed health departments in assurance of a competent workforce. Health departments with shared governance often scored better than their locally governed counterparts. These patterns in EPHS performance by governance structure are likely driven in part by differences in health department responsibilities, with state-governed and locally governed LHDs serving different purposes within a state’s public health infrastructure. We also found significant relationships between EPHS scores and region. These regional differences may indicate that regional populations share similar needs, which the health departments are responding to, or may be a product of the differing roles of LHDs in the public health systems in various regions.
EPHS score–based cluster analysis indicated that LHDs may specialize in particular EPHS areas, consistent with findings of previous studies. 36 -38 This finding suggests that given resource limitations or political limitations, LHDs may be focusing on some areas and not on others. The associative analysis between structural characteristics and health department clusters also highlights important potential drivers of health department priorities. As expected, the high-performing LHD clusters had larger mean population sizes and higher mean per-capita expenditures than health departments with smaller mean populations and lower mean per-capita expenditures. Health department governance and presence of a local board of health also appear to be related to the types of services a health department provides. In addition, health departments within a given cluster tended to be from the same region. This finding again supports the notion of regional similarities in health departments.
Limitations
This study had several limitations. First, although this study drew from a sampling frame that included all LHDs, responses differed by population size, and LHDs serving smaller populations were less likely to respond than LHDs serving larger populations. Based on the associations between population size and LHD performance in our model, the differential response rate by population size may indicate that we overestimated nationwide EPHS performance.
Second, although activities included in the PCAs were informed by metrics used in previous evaluations, we were limited to the questions asked by the NACCHO survey and did not cover all activities necessary for fulfillment of each EPHS. Furthermore, many surveillance activities categorized to EPHS 1 are often included in EPHS 2. However, we felt these activities fit well within the “monitor health” description of EPHS 1. EPHS 7, which represents linkage to and provision of care, has typically been interpreted as a health department assuring access to care. In this analysis, we included activities that represented health departments not just linking to care but also providing clinical care. We believe the inclusion of these activities provides a more robust picture of the services being offered by LHDs to ensure access to care in their communities. In addition, scores were derived from statistical relationships identified in PCA and not on any indication that an activity was more or less important. That is, highly loaded variables should be considered indicators of performance rather than drivers of performance.
Third, there was likely unmeasured variability in both LHD performance and the LHD characteristics that we did not account for in our analysis. We based our analysis on self-reported performance of activities, not on how well those activities were performed. Therefore, we would expect additional variability in performance within each activity. Similarly, we lacked detailed information on the characteristics of LHDS evaluated. For example, although we could account for the presence of a local board of health, we had no information on the board of health’s tasks, which may be meaningful for health department success.
Fourth, we focused on those activities being performed by LHDs directly. However, LHDs exist within a larger local health system in which other entities may be responsible for providing essential services to their communities. State or other local government agencies may be mandated to carry out 1 or more of the EPHSs rather than all EPHSs falling under the purview of the LHD. Therefore, low EPHS scores may indicate a sharing of responsibilities rather than a lack of EPHS provision. In addition, these data were collected from LHDs in 2013, and capacities may have changed since then.
Future research exploring temporal trends in LHD performance and the relationships between structural characteristics and performance is vital to further improve the understanding of LHD capacity needs. In addition to the NACCHO profile data, other data sets, such as the National Longitudinal Survey of Public Health Systems, offer opportunities to further investigate these relationships. 39
Conclusions
Our analysis suggests that LHD performance on the EPHSs varies widely and is weak overall. Performance was positively associated with per-capita expenditures and size of the population served, which supports previous findings. Performance also differed by governance structure, suggesting that the governance structure affects the LHD’s role in states’ public health infrastructure. The clustering of LHDs by performance scores indicates that LHDs may be specializing in services.
Understanding the level of EPHS performance by LHDs, and the variations in that performance, is fundamental in evaluating population access to critical public health services. These findings allow us to identify underserved populations and evaluate correlates to health department performance, which serve to guide performance improvement efforts. Further research on LHD capacity and the changes in that capacity over time is necessary for identifying gaps in the provision of public health services. Finally, LHDs are an essential part of the public health infrastructure in the United States and require continued resources and support to provide EPHSs to their communities.
Footnotes
Acknowledgments
The authors acknowledge the National Association of County and City Health Officials (NACCHO) for its data contributions to this project and Tom Burke and Carla Zelaya for their contributions to the conceptualization of this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The 2013 NACCHO Profile of Local Health Departments Survey was funded by the Centers for Disease Control and Prevention and the Robert Wood Johnson Foundation. The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.