
Abstract
Objectives:
The Council of State and Territorial Epidemiologists (CSTE) has periodically assessed the epidemiological capacity of states since 2001, but the data do not reflect the total US epidemiology capacity. CSTE partnered with the Big Cities Health Coalition (BCHC) in 2017 to assess epidemiology capacity in large urban health departments. We described the epidemiology workforce capacity of large urban health departments in the United States and determined gaps in capacity among BCHC health departments.
Methods:
BCHC, in partnership with CSTE, modified the 2017 State Epidemiology Capacity Assessment for its 30 member departments. Topics in the assessment included epidemiology leadership, staffing, funding, capacity to perform 4 epidemiology-related Essential Public Health Services, salary ranges, hiring requirements, use of competencies, training needs, and job vacancies.
Results:
The 27 (90%) BCHC-member health departments that completed the assessment employed 1091 full-time equivalent epidemiologists. All or nearly all health departments provided epidemiology services for programs in infectious disease (n = 27), maternal and child health (n = 27), preparedness (n = 27), chronic diseases (n = 25), vital statistics (n = 25), and environmental health (n = 23). On average, funding for epidemiology activities came from local (47%), state (24%), and federal (27%) sources. Health departments reported needing a 40% increase from the current number of epidemiologists to achieve ideal epidemiology capacity. Twenty-five health departments reported substantial-to-full capacity to monitor health problems, 21 to diagnose health problems, 11 to conduct evaluations, and 9 to perform applied research.
Conclusions:
Strategies to meet 21st century challenges and increase substantial-to-full epidemiological capacity include seeking funds from nongovernmental sources, partnering with schools and programs of public health, and identifying creative solutions to hiring and retaining epidemiologists.
Keywords
The Council of State and Territorial Epidemiologists (CSTE) began conducting periodic assessments of workforce capacity as it relates to functional applied public health epidemiology in the United States and its territories in 2001 and has subsequently conducted 6 such assessments. 1 -6 The most recent of these assessments, known as Epidemiology Capacity Assessments (ECAs), was conducted early in 2017 and included all 50 states, the District of Columbia, and 3 territories (American Samoa, Northern Mariana Islands, and the US Virgin Islands). 6
The ECAs are an important source of information for policy makers about epidemiology workforce strength and capacity. However, a limitation of the ECAs is that they have focused only on state health departments and have not measured the numeric and functional epidemiology capacity of local health departments (LHDs). In some cases, LHDs may have more staff members and capacity than state health departments. In 2014, CSTE and the National Association of County and City Health Officials (NACCHO) conducted a preliminary assessment of epidemiology capacity within LHDs. 7 However, the analysis did not differentiate between large urban health departments and other LHDs, thereby limiting the ability to draw meaningful conclusions from the results.
To address this limitation, CSTE partnered with the Big Cities Health Coalition (BCHC) in late 2017 to conduct an assessment of epidemiology workforce capacity in its 30 member departments, which together serve nearly 20% of the US population. 8 The 2017 state-level ECA was modified for use among BCHC members with 4 goals: (1) enumerate and describe the applied epidemiology workforce, (2) describe the skills of the applied epidemiology workforce, (3) describe the sources of funding support for the applied epidemiology workforce, and (4) describe epidemiology capacity in these large LHDs. Herein, we provide a summary and interpretation of key findings from the assessment.
Methods
Study Population
The BCHC is a forum for the leaders of the largest metropolitan health departments in the United States. To be eligible for membership, health departments must (1) represent a city in one of the 30 most urban areas in the United States, as defined by the 2010 US Census, 9 and have a minimum city population of 400 000 persons or (2) have a minimum city population of at least 800 000 persons. BCHC also requires that member health departments be locally controlled and not be state agencies. 10 We asked all 30 BCHC-member departments to participate in this study. Of these, the health commissioner or similar official for 28 member departments initially agreed to participate and designated a single person to coordinate a response to the assessment.
Assessment Instrument
We used a modified version of the 2017 state-level ECA as the assessment for this study. CSTE and BCHC solicited input from epidemiologists in BCHC-member departments to tailor the 2017 state-level ECA 6 so that the version would be relevant to LHDs. Topics covered in the modified questionnaire included epidemiology leadership in health departments, epidemiology staffing and funding sources, capacity to perform 4 of the 10 Essential Public Health Services 11 most closely linked to epidemiology, civil service salary ranges for epidemiologists, minimum hiring requirements for epidemiologists, use of the Applied Epidemiology Competencies (ie, competencies essential for applied epidemiologists), 12 epidemiology training needs, and epidemiology job vacancies and intended hires. Most questions in the assessment were short answer, multiple choice, scales, or matrix tables. The modified questionnaire also included an open-ended question that asked about the most important epidemiology staffing and capacity issues facing LHDs. Additional materials about the assessment are available on CSTE’s website.
For this study, we defined an epidemiologist as “an investigator who studies the occurrence of disease or other health-related conditions or events in defined populations. The control of disease in populations is often also considered to be a task for the epidemiologist.” 13 For enumerating epidemiologists, we instructed respondents to consider job functions rather than titles, and we provided the Applied Epidemiology Competencies as examples of those functions. 14
We defined epidemiology capacity as “the ability of your health department to lead epidemiologic activities, provide subject matter expertise, and apply for, receive, and manage resources to conduct key epidemiologic activities.” Respondents were asked to use this definition to estimate their capacity to conduct each of 4 Essential Public Health Services most closely related to epidemiology in each of their public health program areas. The 4 Essential Public Health Services were: (1) monitoring health status, (2) investigating community health problems and hazards, (3) evaluating the effectiveness of public health interventions, and (4) conducting applied research. Their choices for capacity were none (0%), minimal (1%-24%), partial (25%-49%), substantial (50%-74%), almost full (75%-99%), or full (100%). For our analysis, we narrowed these responses to 3 categories of capacity: none to minimal (0%-24%), partial (25%-49%), and substantial to full (50%-100%).
In addition, respondents were asked to assess the need for improvement (yes or no) and the priority level of that need (high, medium, low, or not a priority) for each program area. Respondents were also asked to estimate the minimum and maximum annual salaries for civil service epidemiology employees in their departments, stratified by academic degrees and career levels (entry level, midlevel, senior level).
Assessment Administration and Analysis
We collected data from October through December 2017. BCHC staff members emailed the modified ECA to the designated person, who responded to it directly or collected information and coordinated a single response on behalf of the health department. This person coordinated with programmatic and human resources staff members in the health department as necessary to complete the assessment.
We coded and thematically grouped the qualitative data from an open-ended question about epidemiologic staffing: “With respect to epidemiologic staffing and capacity, what are the most critical issues your department faces?” We determined some codes a priori based on our research aims, and other codes emerged through an iterative process. We used Epi Info 7 15 and Microsoft Excel 2016 to analyze the quantitative data.
Results
Structure and Leadership of the Epidemiology Workforce
Of the 27 BCHC respondents, 13 (48%) reported a decentralized epidemiology workforce across the health department, 10 (37%) reported a centralized structure within an epidemiology division or office, and 4 (15%) reported a combination of decentralized and centralized structures. Eleven (41%) BCHC departments had a single lead epidemiologist who oversaw all epidemiology activities in the department, 11 (41%) had multiple epidemiologists leading across various program areas, and 5 (18%) had no identified lead epidemiologists.
All BCHC departments provided epidemiology services for programs in infectious disease, maternal and child health, and preparedness; most provided epidemiology services for programs in chronic disease (n = 25, 93%), vital statistics (n = 25, 92%), and environmental health (n = 23, 85%); and few provided epidemiology services for programs in mental health (n = 9, 33%), occupational health (n = 5, 19%), and genomics (n = 0) (Figure 1).
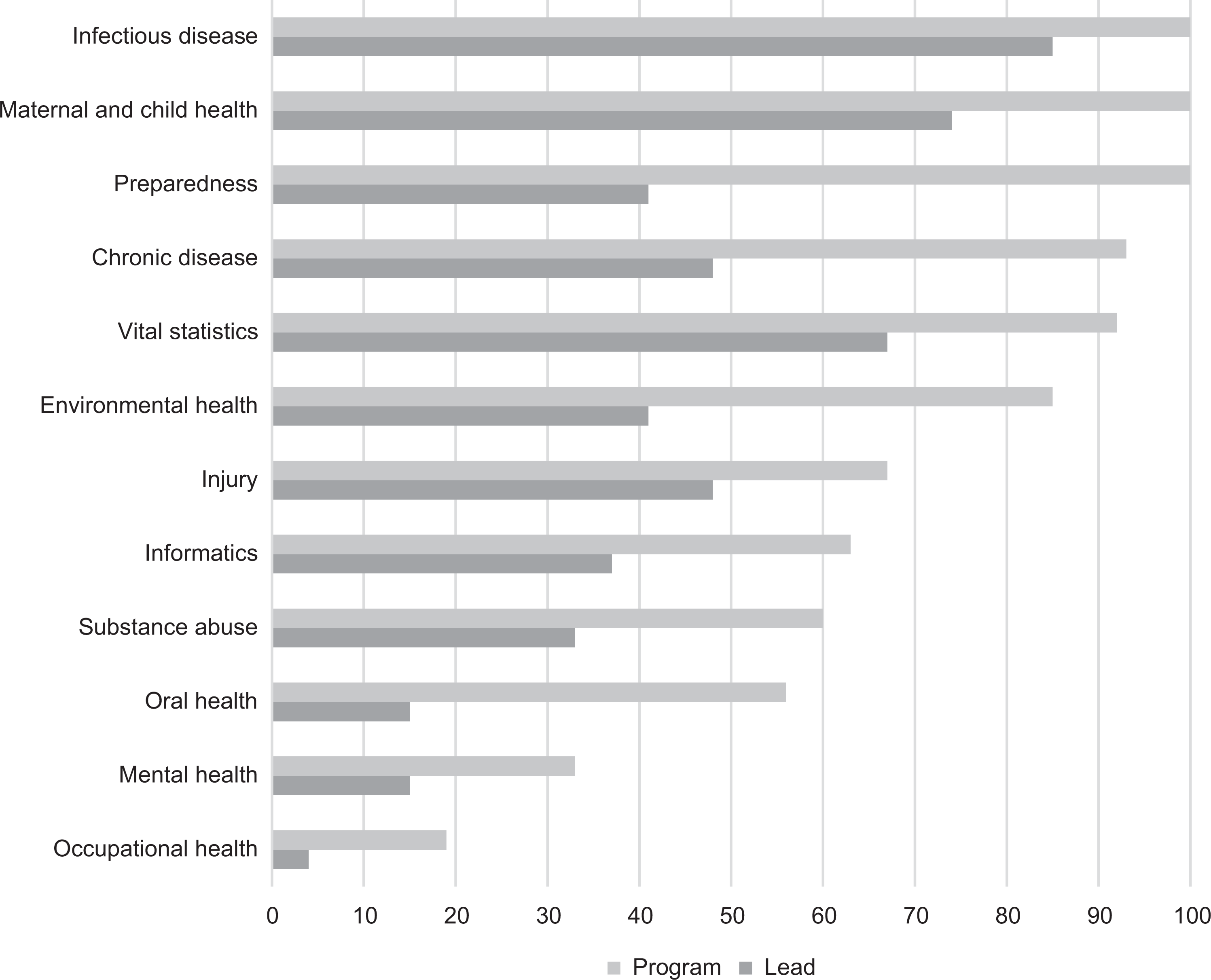
Proportions of 27 Big Cities Health Coalition (BCHC)–member health departments providing epidemiology services to and having formal lead epidemiologists for program areas, based on BCHC-modified Epidemiology Capacity Assessment, United States, 2017. Data source: National Association of County and City Health Officials. 16
Most BCHC departments had lead epidemiologists for programs in infectious disease (n = 23, 85%), maternal and child health (n = 20, 74%), and vital statistics (n = 18, 67%), but only a few health departments had lead epidemiologists in other program areas (Figure 1). However, 21 (78%) health departments reported having generalist epidemiologists who supported some or all of their program areas.
Funding for Epidemiology Activities and Personnel
The 27 BCHC departments received a mean of 47% (range, 0%-100%) of their epidemiology activity funding from local sources, 27% (range, 0%-90%) from federal sources, and 24% (range, 0%-79%) from state sources (Figure 2). Similarly, they received a mean of 44% (range, 0%-100%) of their funding for epidemiology personnel from local sources, 29% (range, 0%-80%) from federal sources, and 24% (range, 0%-71%) from state sources. The BCHC departments received a mean of only 1% for personnel and 3% for activities from other nongovernment sources.
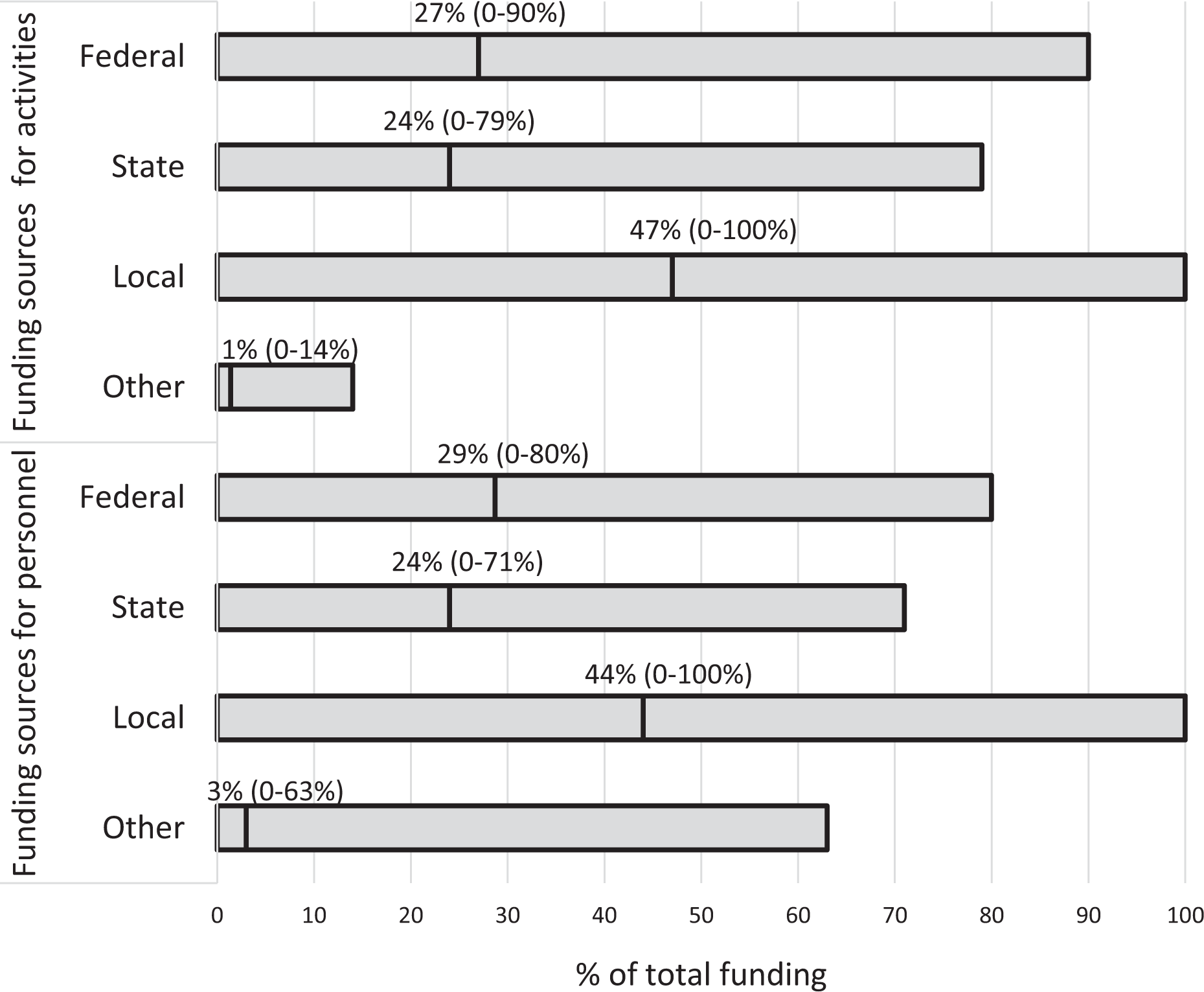
Mean percentage and range of funding sources for epidemiologic activities and epidemiologic personnel at 27 Big Cities Health Coalition (BCHC)–member health departments, based on BCHC-modified Epidemiology Capacity Assessment, United States, 2017. Data source: National Association of County and City Health Officials. 16 Vertical lines in bars represent means.
Epidemiology Staffing: Current and Ideal
The 27 BCHC departments employed 1091 full-time equivalent (FTE) epidemiologists (Table 1). The median number of epidemiologists per BCHC department was 18 (range, 3-385). The median number of epidemiologists per 100 000 population was 1.4 (range, 0.4-7.5). Of all FTE epidemiologists, 474 (43%) worked in infectious disease programs and 201 (18%) were generalists who supported multiple or all program areas.
Current and ideal numbers of full-time equivalent epidemiologistsa at 27 Big Cities Health Coalition (BCHC)–member health departments, by program area, based on BCHC-modified Epidemiology Capacity Assessment (ECA),b United States, 2017c
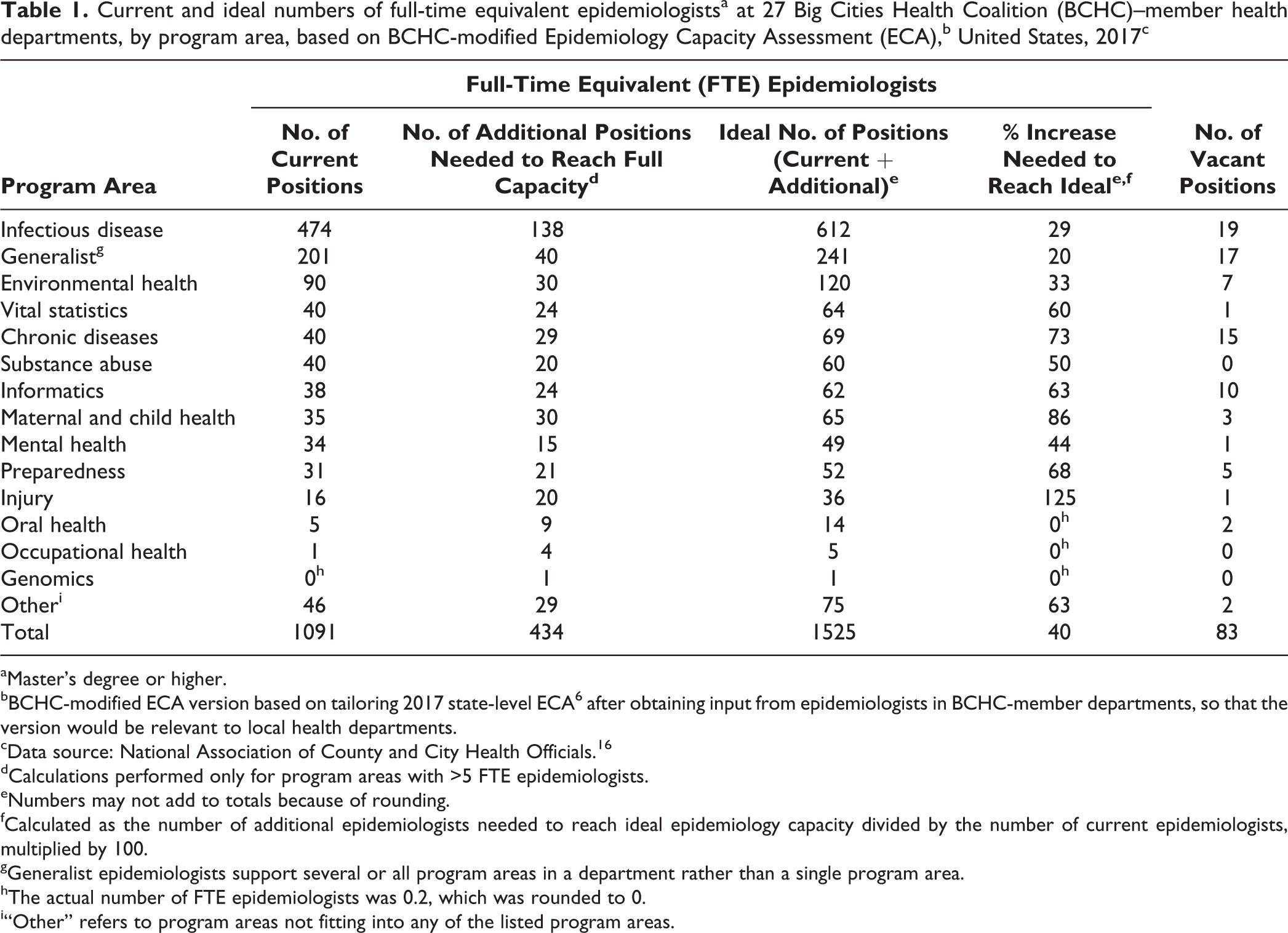
aMaster’s degree or higher.
bBCHC-modified ECA version based on tailoring 2017 state-level ECA 6 after obtaining input from epidemiologists in BCHC-member departments, so that the version would be relevant to local health departments.
cData source: National Association of County and City Health Officials. 16
dCalculations performed only for program areas with >5 FTE epidemiologists.
eNumbers may not add to totals because of rounding.
fCalculated as the number of additional epidemiologists needed to reach ideal epidemiology capacity divided by the number of current epidemiologists, multiplied by 100.
gGeneralist epidemiologists support several or all program areas in a department rather than a single program area.
hThe actual number of FTE epidemiologists was 0.2, which was rounded to 0.
i“Other” refers to program areas not fitting into any of the listed program areas.
Respondents reported a need for an additional 434 FTE epidemiologists across all program areas and departments to reach what they considered ideal or full capacity (1526 FTE epidemiologists), a 40% increase from the current number of FTE epidemiologists (Table 1). The largest number of epidemiologists (n = 138) needed in a single program was for infectious disease. Among program areas with an overall total of more than 5 FTE epidemiologists, the greatest proportional increases in FTE epidemiologists needed to reach full capacity were for injury (125%) and maternal and child health (86%) programs.
Current Epidemiology Vacancies
Respondents reported 83 vacancies for all BCHC departments in positions requiring a master’s degree or higher, including 75 (90%) civil service positions and 8 (10%) contract positions (Table 1). The largest numbers of vacant epidemiology positions were in infectious disease (n = 19), generalist (n = 17), and chronic diseases (n = 15). The 83 vacant positions represented only 19% of the 434 positions that BCHC departments had reported needing to reach what they considered full capacity. More than half (n = 15, 56%) of BCHC departments reported using contractors to fill vacancies for epidemiology and surveillance positions.
Epidemiology Capacity
Twenty-five (93%) BCHC departments reported having substantial-to-full capacity to monitor health status to identify and solve community health problems; 21 (78%) to diagnose and investigate health problems and health hazards in the community; 11 (41%) to evaluate effectiveness, accessibility, and quality of personal and population-based health services; and 9 (33%) to research new insights and innovative solutions to health problems.
Most BCHC departments reported having adequate capacity to conduct all 4 epidemiology-related Essential Public Health Services in program areas, including infectious disease (n = 27, 100%), maternal and child health (n = 25, 93%), chronic diseases (n = 24, 89%), injury (n = 24, 89%), and preparedness (n = 22, 81%) (Figure 3). In contrast, fewer than half of the BCHC departments reported having adequate epidemiology capacity in other program areas, including mental health (n = 13, 48%), oral health (n = 10, 37%), and occupational health (n = 4, 15%); none reported adequate epidemiology capacity in genomics.
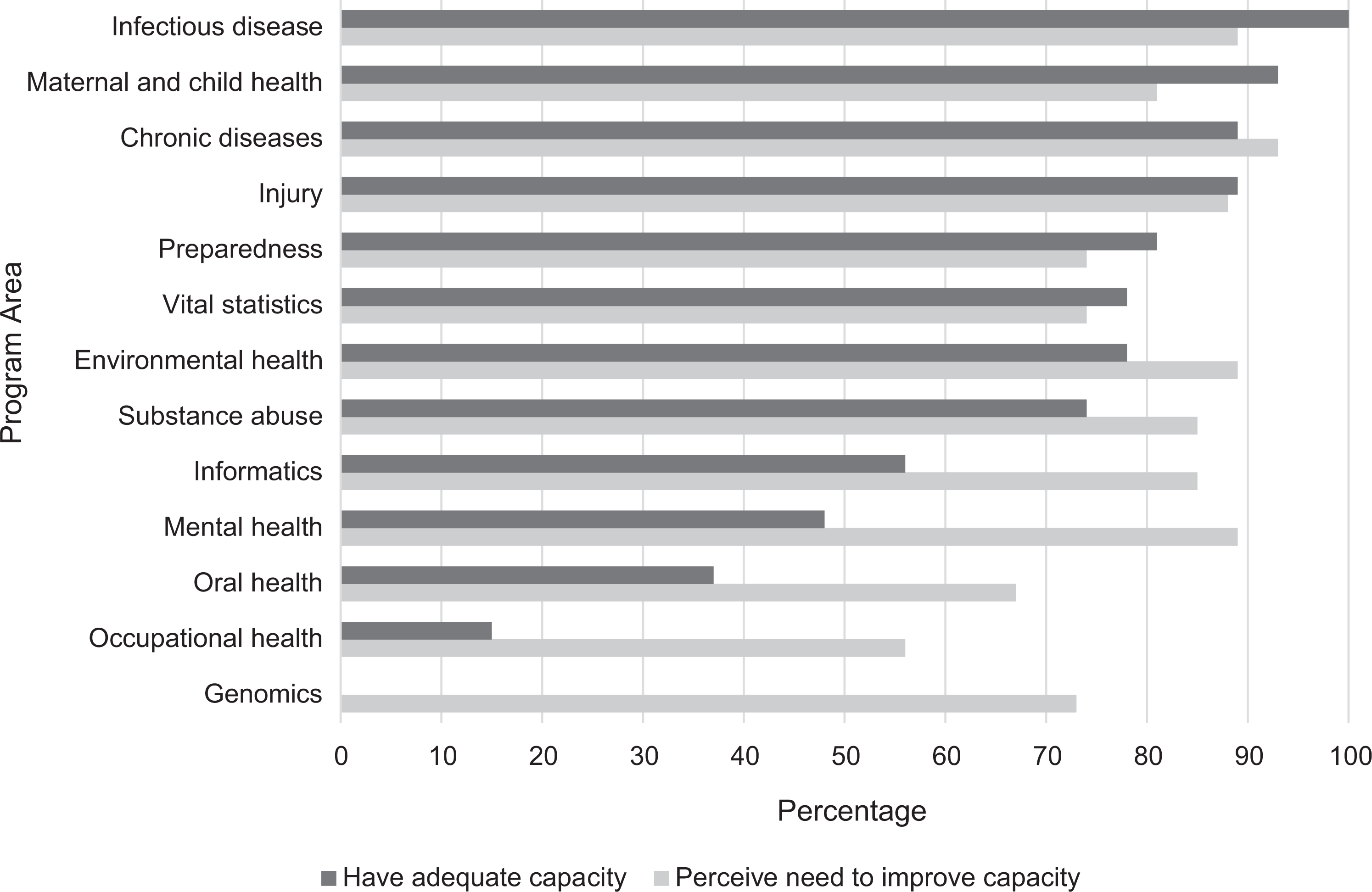
Proportions of 27 Big Cities Health Coalition (BCHC)-member health departments with adequate epidemiology workforce capacity and needing improvement in epidemiology workforce capacity to conduct all 4 Essential Public Health Services, by program area, based on BCHC-modified Epidemiology Capacity Assessment (ECA), United States, 2017. BCHC-modified ECA version based on tailoring 2017 state-level ECA 6 after obtaining input from epidemiologists in BCHC-member departments, so that the version would be relevant to local health departments. The 4 Essential Public Health Services are to monitor health status to identify and solve community health problems; to diagnose and investigate health problems and health hazards in the community; to evaluate effectiveness, accessibility, and quality of personal and population-based health services; and to research new insights and innovative solutions to health problems. 10 Respondents were asked to estimate their percent capacity to conduct the 4 Essential Public Health Services in each of their public health program areas. The responses were narrowed down to 3 categories: none-to-minimal (0%-24%), partial (25%-49%), or substantial-to-full (50%-100%) capacity. In addition, respondents were asked to assess the need for improvement in capacity for each of their program areas, with their response options being yes or no.
Even in program areas that had adequate capacity, however, many BCHC departments still perceived a need in most of their programs to improve their capacity to conduct the 4 Essential Public Health Services. For all program areas except occupational health and oral health, at least 74% of BCHC departments reported such a need (Figure 3). The program areas BCHC departments reported as being high priority for needing capacity improvements were chronic disease (n = 13, 48%), substance use (n = 12, 44%), infectious disease (n = 11, 41%), and informatics (n = 10, 37%).
Academic Degree and Experience Requirements
For entry-level epidemiologists, a master’s degree or higher was required by 16 (60%) BCHC departments, a bachelor’s degree by 9 (33%) departments, and an associate’s degree or less by 2 (7%) departments. Nearly half (n = 13, 48%) of BCHC departments required ≥2 years of experience, 5 (19%) required ≥1 year of experience, and 9 (33%) required <1 year of experience for entry-level epidemiologists. The most frequent responses about what qualified as experience were paid work (n = 25, 93%), full-time work (n = 24, 89%), internships (n = 22, 81%), and volunteer work (n = 14, 52%).
Epidemiologist Salaries
Median minimum and maximum salaries for epidemiologists with bachelor’s degrees were $51 493 and $72 506, for epidemiologists with doctor of philosophy degrees were $71 462 and $117 537, and for epidemiologists with doctor of medicine degrees were $100 000 and $150 000, respectively (Table 2). Median minimum and maximum salaries for epidemiologists with doctor of medicine degrees were approximately $20 000 to $30 000 higher than for epidemiologists with other doctoral degrees, despite completing comparable years of graduate school. Median minimum and maximum salaries were $55 900 and $76 999 for entry-level employees, $69 958 and $94 477 for midlevel employees, and $80 283 and $120 000 for senior-level employees, respectively.
Median minimum and maximum salaries and salary ranges of epidemiologists, by degree and career level, at 27 Big Cities Health Coalition (BCHC)–member health departments, based on BCHC-modified Epidemiology Capacity Assessment (ECA),a United States, 2017b
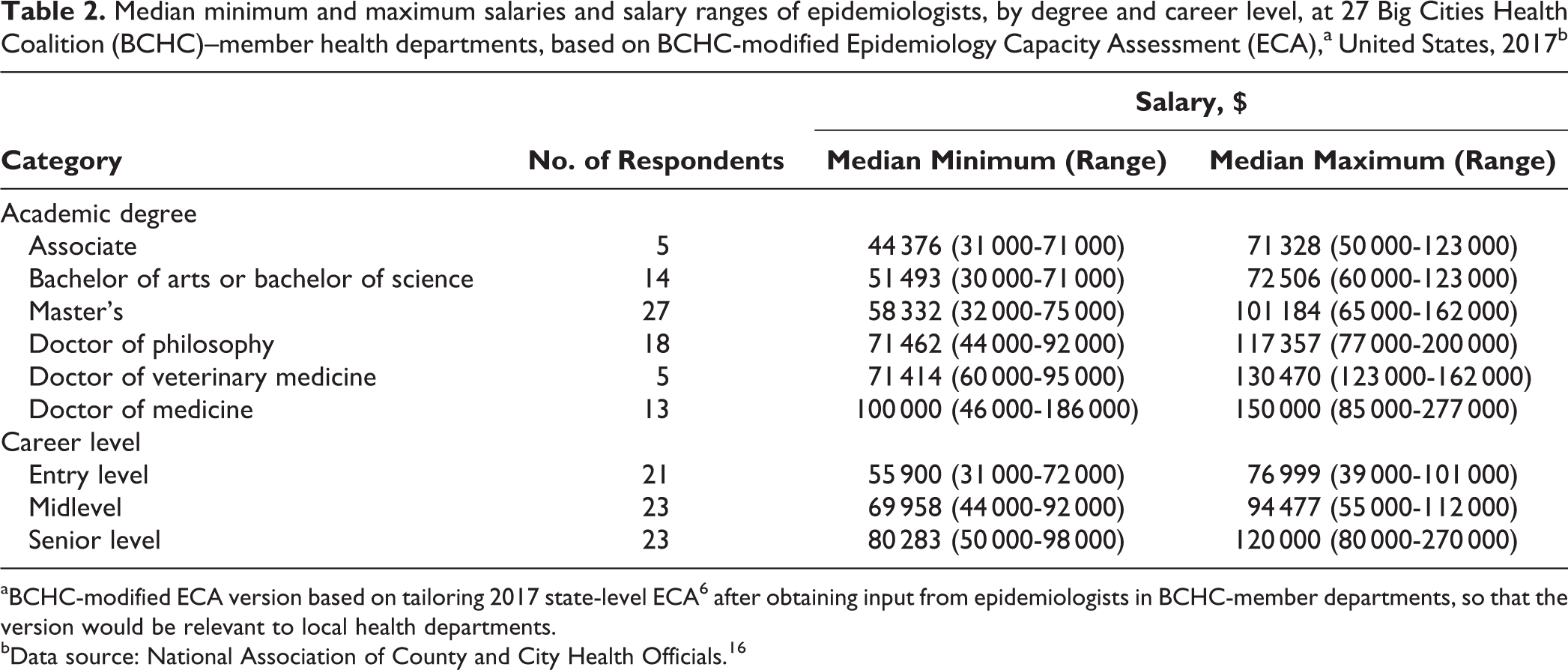
aBCHC-modified ECA version based on tailoring 2017 state-level ECA 6 after obtaining input from epidemiologists in BCHC-member departments, so that the version would be relevant to local health departments.
bData source: National Association of County and City Health Officials. 16
Training Priorities
Thirteen (48%) BCHC departments identified data analytics, which includes informatics and translating and applying public health data, as the highest training priority. Other training priorities identified were systems thinking (n = 9, 33%), persuasive communication (n = 7, 26%), software skills (n = 6, 22%), and general continuing education (n = 6, 22%). No departments reported fiscal management training (including planning, budgeting, or resource monitoring) as a training need.
Critical Issues and Themes
For the open-ended question, respondents reported inadequate epidemiology staffing and capacity as the most critical issue facing their health departments. Based on the responses, we identified several common themes about the sources and implications of this problem.
Lack of predictable, sustainable funding hindered the ability to build epidemiology workforce capacity
BCHC departments had fiscal challenges because of their need to rely on time-limited grant funding for core functions, the unpredictability of their funding from year to year, and the provision of short-term funding for disease outbreaks and emergency responses rather than sufficient resources to sustain ongoing programmatic readiness. Some respondents suggested that the lack of reliable epidemiology funding may have been due to the fact that the roles of epidemiologists and health departments were not well understood by funders making it difficult for departments to successfully advocate for additional epidemiology resources.
Recruiting and retaining epidemiologists was challenging
Health departments had difficulty finding candidates with appropriate skill sets in epidemiology and biostatistics, coupled with adequate field experience. Additional barriers to successful recruitment included inadequate resources for hiring, hiring freezes and delays, and a lack of continuity in the recruiting and hiring processes. Challenges in retaining quality staff members resulted from limited opportunities for promotion, restricted career ladders, and the lack of competitive compensation.
Current staffing levels and models made it difficult to meet increasing demands for epidemiological services and to respond to emergencies
Health departments noted that needing to respond to new and shifting demands for epidemiology information and needing to prioritize urgent and emerging problems often distracted epidemiology staff members from performing their routine epidemiologic functions and, ultimately, often led to burnout. Furthermore, because program-specific funding sometimes led to an approach that focused on individual programs, epidemiology capacity was inconsistent across programs, and epidemiology services for programs without direct funding were often limited. This model of funding and, by extension, staffing leads to an inherent lack of flexibility, thereby limiting both internal and external collaboration, leading to inefficiencies, confusion, and lost opportunities.
A workforce of epidemiologists, with new or different knowledge and skill sets, who are able to adapt to new technologies and respond to emerging public health challenges, is needed to fill gaps in capacity
BCHC departments reported that important noninfectious disease program areas remained underdeveloped, especially areas dealing with social determinants of health, health equity, and behavioral health. Respondents noted that additional training and mentoring were needed to ensure programmatic continuity and to maintain high levels of expertise, particularly in program areas that required staff members to have unique and advanced skill sets, as well as familiarity with new technologies. Yet respondents reported that departmental resources for training and mentoring activities as well as opportunities to share experiences were often limited.
Discussion
The 27 BCHC departments employed 1091 epidemiologists, compared with 3369 epidemiologists employed by the 50 US states and the District of Columbia, according to results of the 2017 ECA. 6 The median number of BCHC-member epidemiologists was 1.4 per 100 000 population, which was higher than the nationally recommended number of epidemiologists of 1.0 per 100 000 population for states. 16,17 It is instructive, if only for discussion purposes, to consider the adequacy of staffing of both LHDs and state health departments together. For example, areas without a strong state health department presence may also have low levels of staffing in their LHDs, such that the overall capacity to respond to public health emergencies or disasters, or even to conduct routine activities, may be inadequate. On the other hand, a strong local presence may be able to compensate for lower capacity at the state level. Ensuring the public’s health demands a coordinated system among local, state, and federal partners. Investments and other resources should take this into account and be distributed accordingly.
We observed that the capacity of BCHC departments to monitor health status and diagnose and investigate health problems and health hazards was high, but it was considerably lower for evaluating effectiveness, accessibility, and quality of health services, and for researching new insights and innovative solutions to health problems. A similar pattern was observed in the 2017 ECA results for the 50 states and the District of Columbia. 6 When we examined this finding further by program area, we noted that capacity was high in some program areas (eg, infectious disease) but lower in other program areas (eg, mental health). This suggests the need for additional strategies for both hiring and training to build workforce capacity. This is particularly true not only in evaluation and research but also in such program areas as mental health, substance use, social determinants of health, health equity, and violence, in which capacity is low. Health departments can partner with schools and programs of public health to ensure the workforce is trained in these low-capacity programs.
Our results demonstrate a substantial unmet need for epidemiologists in BCHC departments—an estimated 40% increase in the number of epidemiologists to achieve ideal or full capacity for the 27 BCHC departments. However, the numbers alone do not provide a comprehensive picture of the complexity of this issue. Our qualitative findings point to both the importance and the difficulty of finding staff members with the appropriate skills to complement the existing staff and to respond to constantly changing public health priorities. Hiring and retaining epidemiologists was a major challenge for many BCHC departments. One contributing factor cited was the lack of competitive salaries in BCHC departments, despite the fact that these LHDs, on average, had higher salaries at most levels of education and experience than their state health department counterparts. 6 Other contributing factors, such as hiring freezes and delays and limited career mobility, were also cited as playing a role in hiring and retaining quality staff members. These issues should be addressed and will demand creative solutions from health department leaders. Developing an epidemiology workforce that is able to meet current challenges will also require working with schools and programs of public health to ensure that their graduates have the needed skills, as well as developing training and mentoring programs for existing staff members to adapt to the evolving public health priorities.
Limitations
The BCHC ECA and its results had several limitations. First, although the ECA provided respondents with a functional definition of epidemiologist, this definition had a subjective component to it and did not necessarily align directly with job titles in some BCHC departments. Likewise, assessing capacity is inherently subjective, although we attempted to mitigate this concern and limit the potential for broad interpretation by providing respondents with a definition of epidemiology capacity. To the degree that subjectivity affected results, it may have influenced comparisons among BCHC departments and between findings from the BCHC assessment and state-level ECA findings. Second, questions in the BCHC ECA about ideal staffing were focused on epidemiologists at the master’s degree level or higher. This focus may have resulted in underestimating the overall epidemiology needs in some departments. Third, the qualitative data that we used came from a single open-ended question, which required some subjective interpretation. However, we reported only a small number of themes for which multiple departments had described an issue or discussed a challenge. In addition, based on our experience working with these health departments, we believe these issues and challenges are common and exist in multiple BCHC departments. Finally, the results presented here reflect the responses of participating BCHC-member departments and may not be generalizable to other LHDs that are not BCHC members. However, as the first-of-its-kind assessment of epidemiology capacity among large urban LHDs, we believe these results will nonetheless prove useful in identifying and addressing epidemiology workforce development challenges throughout the United States.
Conclusion
Although many BCHC-member departments reported substantial-to-full capacity to conduct core epidemiology functions related to the monitoring and diagnosing of health problems in traditional program areas, they noted numerous challenges in obtaining funding, hiring and retaining epidemiologists with the skills needed to conduct evaluations and applied research for program improvement, and expanding capacity in important emerging program areas. Strategies that might be considered to address these challenges include seeking additional funds from nongovernmental sources, partnering with schools and programs of public health to ensure a workforce that is trained to meet new challenges, and identifying creative administrative solutions to hiring and retention.
Footnotes
Acknowledgments
The authors acknowledge and thank our colleagues for their support and guidance on the project: Beth Daly, Rich Danila, Jeff Engel, Aaron Fleischauer, Bob Harrison, Sara Huston, Becky Lampkins, Jennifer Lemmings, Meredith Lichtenstein Cone, Amanda Masters, Joe McLaughlin, Patty Quinlisk, Dhara Shah, Kathy Turner, Sharon Watkins, epidemiologists in BCHC health departments, and the National Association of County and City Health Officials local epidemiology workgroup. BCHC also thanks its Foundation funders and members for enabling and supporting our participation in this work. The contents of this article are solely the responsibility of the authors and do not necessarily represent the official views of the Centers for Disease Control and Prevention.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors declared the following funding with respect to the research, authorship, and/or publication of this article: This publication was supported in part by the Centers for Disease Control and Prevention cooperative agreement numbers 5U38OT000143-04 and 5U38OT000143-05.