
Abstract
Objectives:
Given the known high morbidity and mortality of hepatitis C virus (HCV) infection in Oregon, we sought to develop a practical method of estimating the severe sequelae of HCV infection among Medicaid beneficiaries in Oregon.
Methods:
We assembled a retrospective cohort that identified all Oregon Medicaid beneficiaries with HCV infection enrolled for at least 1 year during 2009-2013. We linked this cohort to 3 data sets to identify HCV-related deaths, cases of hepatocellular carcinoma (HCC), and first hospitalizations for advanced liver disease (ALD). We calculated incidence density rates and used multivariable Cox regression modeling to calculate adjusted hazard ratios (aHRs) to evaluate the association between demographic characteristics (birth year, sex, race, ethnicity) and these 3 outcomes.
Results:
Of 11 790 Oregon Medicaid beneficiaries with HCV infection, 474 (4.0%) had an HCV-related death, 156 (1.3%) had HCC, and 596 (5.1%) had a first hospitalization for ALD. Adjusted hazard ratios for deaths were 2.2 (95% confidence interval [CI], 1.6-2.8) among persons born in 1945 through 1965 (vs persons born after 1965), 2.1 (95% CI, 1.7-2.5) among males (vs females), and 1.9 (95% CI, 1.2-2.9) among Asian/Pacific Islanders and 2.2 (95% CI, 1.5-3.2) among American Indian/Alaska Natives (vs white persons). The same risk groups had significant aHRs for first hospitalizations for ALD. Persons born before 1945 (aHR = 17.0; 95% CI, 5.2-55.8) and in 1945 through 1965 (aHR = 12.8; 95% CI, 4.1-40.3) vs born after 1965, males (aHR = 3.3; 95% CI, 2.3-4.8) vs females, and Asian/Pacific Islanders (aHR = 3.9; 95% CI, 2.3-6.7) vs white persons had higher risks for HCC.
Conclusions:
Continued assessments using the methods piloted in this study will allow Oregon to monitor trends in severe sequelae of HCV infection over time.
Hepatitis C virus (HCV) infection is the most common chronic blood-borne infection in the United States. 1 The World Health Organization estimated the number of persons living with chronic HCV infection to be 71 million worldwide in 2015, 2 and the Centers for Disease Control and Prevention estimated the number of persons living with chronic HCV infection in the United States to be 2.7 million during 2003-2010. 3 A 1999-2008 study estimated that 75% of HCV-infected persons in the United States were born in 1945 through 1965, leading to a growing concern for HCV-associated morbidity and mortality in this population and a recommendation by the US Preventive Services Task Force (USPSTF) to offer a 1-time screening to persons in this cohort regardless of other risk factors. 4 –6
After Oklahoma and the District of Columbia, Oregon has the third highest prevalence of HCV infection in the nation. 7 In a viral hepatitis profile covering the period 2009-2013, the Public Health Division of the Oregon Health Authority (OHA) estimated that HCV infection across Oregon was linked to 2207 deaths, 3917 hospitalizations, and 611 cases of hepatocellular carcinoma (HCC). The report also documented that age-adjusted HCV-related mortality in Oregon (8.7 deaths per 100 000 persons) was nearly twice the national average in 2011 (4.8 deaths per 100 000 persons) and that the number of cases of HCC rose 64%, from 95 cases in 2008 to 156 cases in 2012. 8
New direct-acting antiviral agents are highly effective. 9 Despite their effectiveness and tolerability, however, the use of direct-acting antiviral agents in the Medicaid population varies widely because of cost and budgetary constraints. 10,11 To better inform evidence-based decisions about expanding direct-acting antiviral treatment to Medicaid beneficiaries, we sought to establish a method to accurately estimate the incidence of severe outcomes of HCV infection that could be used by local health authorities and yield data that are useful to policy makers.
Methods
Data Sources, Participants, and Data Source Matching
We assembled a retrospective cohort that consisted of Oregon Medicaid beneficiaries with at least 1 year of Medicaid enrollment from January 1, 2009, through December 31, 2013 (hereinafter referred to as the HCV Medicaid cohort). We used administrative claims data from the Division of Medical Assistance Programs, which coordinates the operation of the Medicaid portion of the Oregon Health Plan, to identify beneficiaries with an HCV infection, as defined by a medical claim with a diagnosis of HCV infection (recorded using the International Classification of Diseases, Ninth Revision, Clinical Modification [ICD-9-CM] and Current Procedural Terminology codes; available from the authors upon request) 12,13 or a pharmacy claim for a relevant drug therapy, including interferon alfa, peginterferon alfa-2a, peginterferon alfa-2b, ribavirin, boceprevir, telaprevir, simeprevir, or sofosbuvir, which were available on the market during the study period. For each beneficiary, we abstracted first and last name, date of birth, sex, race/ethnicity, and ZIP code. We then matched data on persons in this HCV Medicaid cohort with outcomes data from 3 databases: death certificate data obtained from the Oregon Center for Health Statistics, the Oregon State Cancer Registry (OSCaR), and the state inpatient hospital discharge data set. 14 –16 We used death certificate data to identify HCV-related deaths, OSCaR to identify cases of HCC, and the state inpatient hospital discharge data set to identify first hospitalizations for advanced liver disease (ALD). By using these data sets, which include all Oregonians, not just those on Medicaid, we were able to identify deaths, patients with HCC, or first hospitalizations from ALD even if a patient was no longer enrolled in Medicaid at the time the event occurred. The Oregon Center for Health Statistics registers only vital events that occur in Oregon, but it also collects data on deaths among Oregon residents that occur out of state through an interstate exchange agreement. By statute, all cases of cancer diagnosed in Oregon must be reported to OSCaR. The hospital discharge data set includes every inpatient hospitalization from every nonfederal general acute-care hospital in the state (excluding Veterans Health Administration hospitals, rehabilitation facilities, long-term care facilities, and psychiatric hospitals). Participating hospitals submit records based on set ICD-9-CM coding requirements directly from their electronic record systems.
We used LinkPlus 2.0, a probabilistic record linkage program, to identify persons who appeared in both the Medicaid cohort and at least 1 of the outcome databases. 17 We used guidelines for determining matches that were developed by staff members at the Northwest Portland Area Indian Health Board. 18 For matching purposes, we created a data set from our full HCV Medicaid cohort data set that contained only the Medicaid identification number and limited data on beneficiaries’ demographic characteristics: we used patient’s last name, first name, date of birth, and sex to identify matches between the HCV Medicaid cohort and each of the 3 databases. After each round of matching with 1 of the 3 data sets, 2 authors (K.J. and A.R.T.) manually reviewed the results to verify the matches. After completing a match with another data set (eg, OSCaR), we extracted data from the OSCaR database only on persons who matched to the HCV Medicaid cohort and retained only the data confirming the diagnosis of HCC, which we then merged into our main HCV Medicaid cohort data set. Similarly, for deaths and hospitalizations for ALD that matched persons in the HCV Medicaid cohort, we retained only the matched pairs and their diagnoses, and we deleted the data sets provided to us for matching purposes. This project was considered exempt from human subjects review by the OHA.
Measures
The primary outcomes of interest were HCV-related deaths, cases of HCC as identified in OSCaR, and first hospitalizations for ALD. We used the underlying cause of death to classify HCV-related deaths, and we included a hospitalization if 1 of the first 3 discharge diagnoses was related to ALD. Given the USPSTF recommendation to offer 1-time screening for HCV infection to adults born in 1945 through 1965, 6 we categorized birth year into 3 groups: born before 1945, born in 1945 through 1965, and born after 1965. We dichotomized sex as female or male; we categorized race as white, black, American Indian/Alaska Native (AI/AN), Asian/Pacific Islander (API), and other/unknown race; and we dichotomized ethnicity as Hispanic or non-Hispanic/unknown. We categorized patients as having initiated treatment if they had filled an appropriate prescription at least twice, and we considered treatment completed if patients had filled an appropriate prescription for 24 weeks, which was the minimum length of treatment with peginterferon and ribavirin commonly used during the study period. We classified residence as rural or urban by using patient ZIP code, according to the definition of rural as ≥10 miles from the centroid of a population center of ≥40 000 persons. 18 We additionally abstracted data on the status of co-infection with HIV or hepatitis B virus (HBV) by using ICD-9-CM codes 042, 079.53, and V08 for HIV and 070.20, 070.21, 070.22, 070.23, 070.31, 070.32, 070.33, and V02.61 for HBV. We did not exclude any patients for missing data.
Statistical Analysis
We calculated the frequencies of demographic characteristics of the Medicaid cohort and compared them with characteristics of persons with chronic HCV infection reported to OHA to understand the differences between Medicaid patients with HCV and the general population of Oregonians with HCV. The at-risk period began on the first date in the study period that the patient was covered by Medicaid (index date) and ended on the date of occurrence of the outcome(s) or at the end of the study period, whichever came first. To calculate the incidence density stratified by demographic characteristics, we used the outcome cases as numerators, and we tabulated denominators for each patient by using the time between each patient’s index date and occurrence of the outcome or the end of the study period, whichever came first. We excluded from the denominator patients who died of non–HCV-related causes. We used 2-sided mid-P exact tests to determine significance. We considered P < .05 to be significant.
Lastly, we used multivariable Cox proportional hazard models to calculate the adjusted hazard ratios (aHRs) to estimate the effect of demographic characteristics on each outcome. We examined the following variables: birth year, sex, race/ethnicity, treatment status, and residence. We used the purposeful selection process for multivariable model building: we evaluated each deleted variable’s impact on model fit and on the HRs of the remaining covariates in the model before making a decision to remove variables from the model. 19 We also assessed statistical interaction and violations of the proportional hazards assumption in Cox regression. We examined residual plots by using the Cox-Snell residuals to assess the appropriateness of the model. We conducted a sensitivity analysis to evaluate whether our estimates varied with duration of Medicaid enrollment by calculating aHRs for all 3 outcomes among the subset of HCV Medicaid patients who were enrolled for fewer than 4 years.
We merged all data sets into a final data set and maintained the HCV Medicaid cohort data set by using SAS version 9.4. 20 We performed descriptive analysis and proportional hazards modeling by using Stata version 13.1. 21
Results
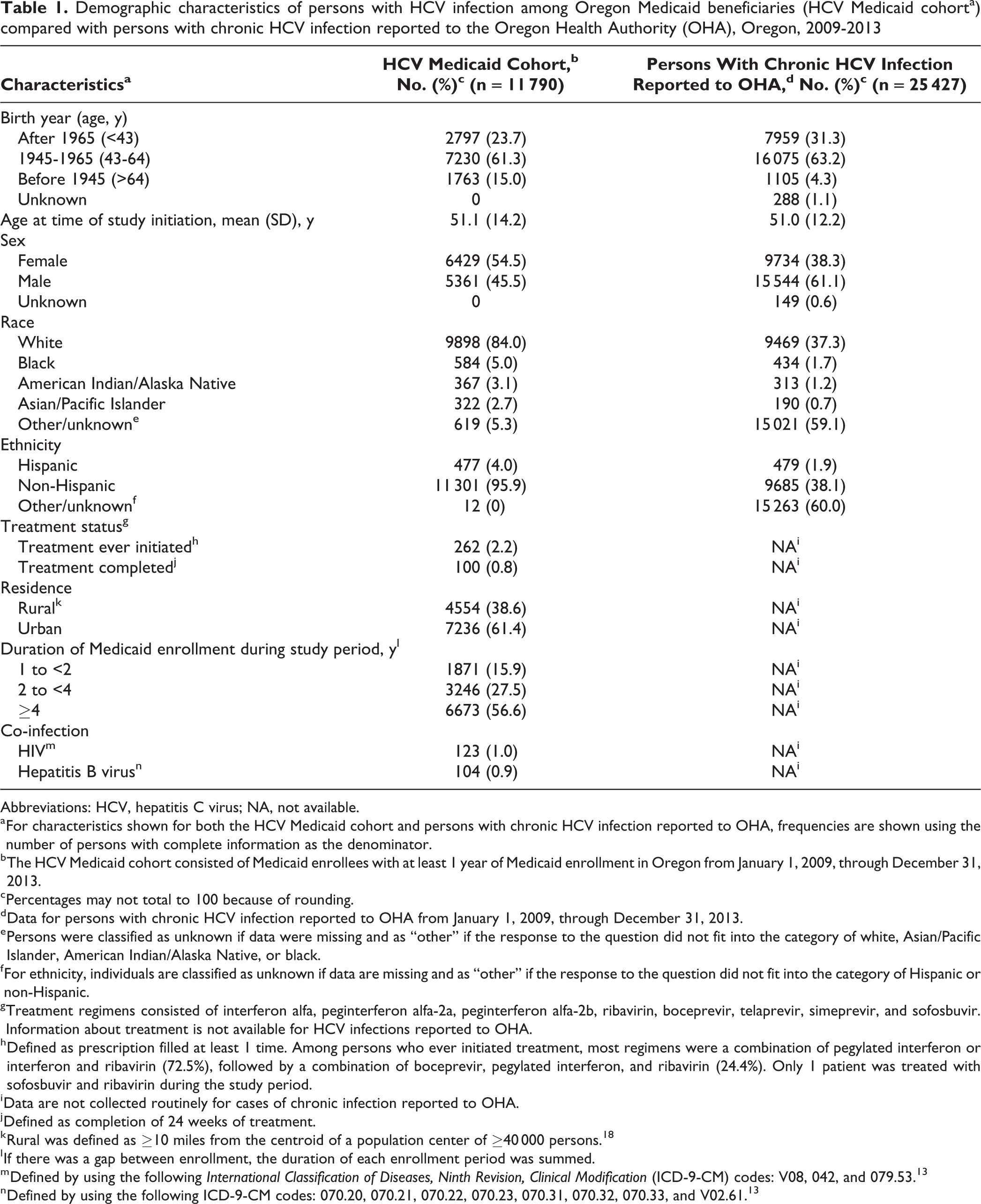
We identified 11 790 Oregon residents with HCV infection enrolled in Medicaid for at least 1 year from January 1, 2009, through December 31, 2013 (Table 1), with 47 728 person-years of follow-up. Of the 11 790 persons in the cohort, most were born in 1945 through 1965 (n = 7230, 61.3%), female (n = 6429, 54.5%), and white (n = 9898, 84.0%). Age distribution varied by race: the mean ages (year [SD]) of white, black, AI/AN, and API were 50.8 (13.9), 51.5 (12.8), 49.7 (11.3), and 63.1 (16.8) years, respectively. A greater percentage of the HCV Medicaid cohort than the general Oregon population with HCV infection was female (54.5% vs 38.3%) and born before 1945 (15.0% vs 4.3%).
Demographic characteristics of persons with HCV infection among Oregon Medicaid beneficiaries (HCV Medicaid cohorta) compared with persons with chronic HCV infection reported to the Oregon Health Authority (OHA), Oregon, 2009-2013
Abbreviations: HCV, hepatitis C virus; NA, not available.
a For characteristics shown for both the HCV Medicaid cohort and persons with chronic HCV infection reported to OHA, frequencies are shown using the number of persons with complete information as the denominator.
b The HCV Medicaid cohort consisted of Medicaid enrollees with at least 1 year of Medicaid enrollment in Oregon from January 1, 2009, through December 31, 2013.
c Percentages may not total to 100 because of rounding.
d Data for persons with chronic HCV infection reported to OHA from January 1, 2009, through December 31, 2013.
e Persons were classified as unknown if data were missing and as “other” if the response to the question did not fit into the category of white, Asian/Pacific Islander, American Indian/Alaska Native, or black.
f For ethnicity, individuals are classified as unknown if data are missing and as “other” if the response to the question did not fit into the category of Hispanic or non-Hispanic.
g Treatment regimens consisted of interferon alfa, peginterferon alfa-2a, peginterferon alfa-2b, ribavirin, boceprevir, telaprevir, simeprevir, and sofosbuvir. Information about treatment is not available for HCV infections reported to OHA.
h Defined as prescription filled at least 1 time. Among persons who ever initiated treatment, most regimens were a combination of pegylated interferon or interferon and ribavirin (72.5%), followed by a combination of boceprevir, pegylated interferon, and ribavirin (24.4%). Only 1 patient was treated with sofosbuvir and ribavirin during the study period.
i Data are not collected routinely for cases of chronic infection reported to OHA.
j Defined as completion of 24 weeks of treatment.
k Rural was defined as ≥10 miles from the centroid of a population center of ≥40 000 persons. 18
l If there was a gap between enrollment, the duration of each enrollment period was summed.
m Defined by using the following International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes: V08, 042, and 079.53. 13
n Defined by using the following ICD-9-CM codes: 070.20, 070.21, 070.22, 070.23, 070.31, 070.32, 070.33, and V02.61. 13
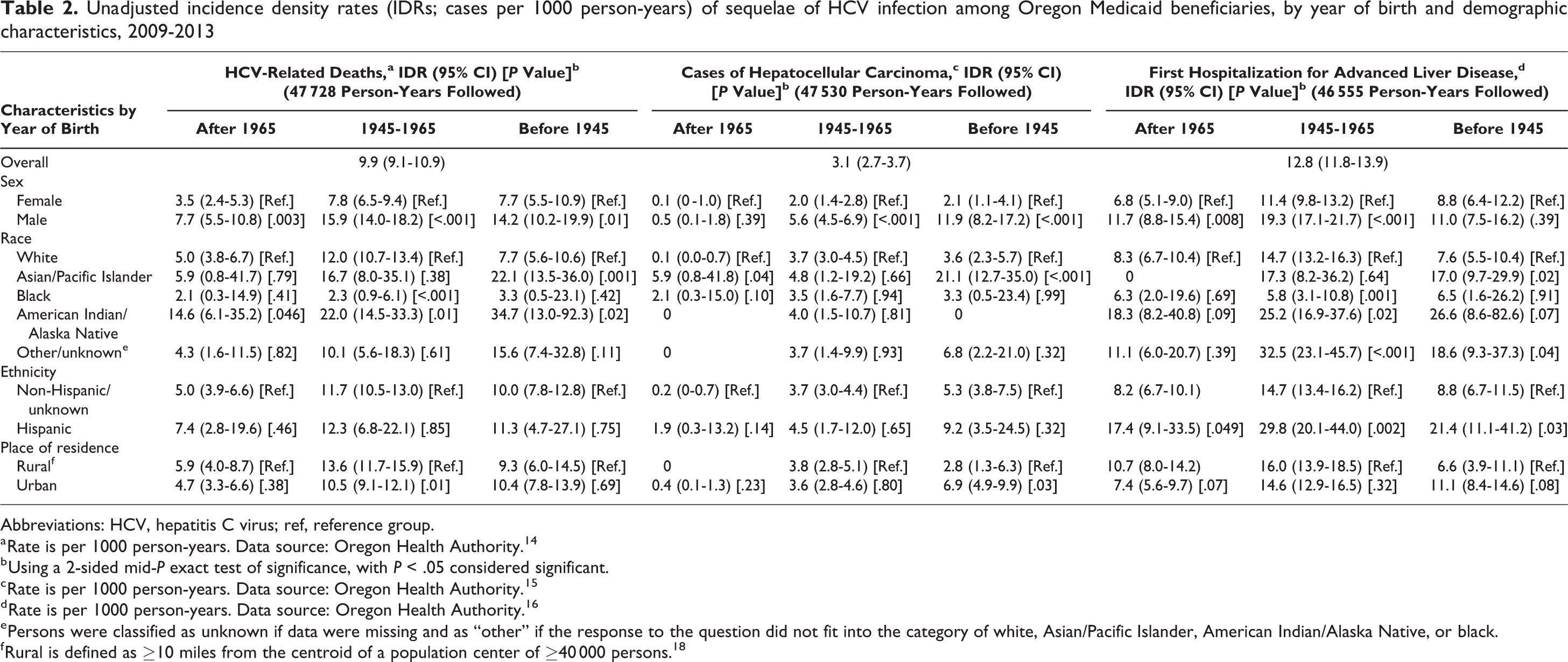
A total of 2457 all-cause deaths occurred during the study period, of which 474 deaths were related to HCV infection, for an HCV-related incidence density rate (IDR) of 9.9 (95% confidence interval [CI], 9.1-10.9) deaths per 1000 person-years. Rates of HCV infection were highest among males (vs females) in all 3 birth-year groups, among APIs (vs white persons) born before 1945, and among AI/ANs (vs white persons) born before 1965 (Table 2). During the study period, we identified 156 cases of HCC, including 3 (1.9%) patients who were co-infected with HIV and 5 (3.2%) patients who were co-infected with HBV. The overall IDR of HCC was 3.1 (95% CI, 2.7-3.7) cases per 1000 person-years, with the highest rates of HCC among males (vs females) of all birth-year groups and among APIs (vs white persons), particularly APIs born before 1945 (Table 2). A total of 1040 hospitalizations were for ALD among 631 patients during the study period. Limiting the estimates to the first hospitalization for ALD yielded 596 hospitalizations, corresponding to an IDR of 12.8 (95% CI, 11.8-13.9) hospitalizations per 1000 person-years. Significantly elevated rates of hospitalization for ALD occurred among males born after 1945 (born 1945-1965: IDR = 19.3 [95% CI, 17.1-21.7]; born after 1965: IDR = 11.7 [95% CI, 8.8-15.4]), APIs born before 1945 (IDR = 17.0; 95% CI, 9.7-29.9), AI/ANs born in 1945 through 1965 (IDR = 25.2; 95% CI, 16.9-37.6), and Hispanic persons of all birth years (born after 1965: IDR = 17.4 [95% CI, 9.1-33.5]; born in 1945 through 1965: IDR = 29.8 [95% CI, 20.1-44.0]; born after 1965: IDR = 21.4 [95% CI, 11.1-41.2]) (Table 2). We also noted differences by location. Rural residents born in 1945 through 1965 had the highest rates of HCV deaths (IDR = 13.6; 95% CI, 11.7-15.9) and urban residents born before 1945 had the highest rates of HCC (IDR = 6.9; 95% CI, 4.9-9.9).
Unadjusted incidence density rates (IDRs; cases per 1000 person-years) of sequelae of HCV infection among Oregon Medicaid beneficiaries, by year of birth and demographic characteristics, 2009-2013
Abbreviations: HCV, hepatitis C virus; ref, reference group.
a Rate is per 1000 person-years. Data source: Oregon Health Authority. 14
b Using a 2-sided mid-P exact test of significance, with P < .05 considered significant.
c Rate is per 1000 person-years. Data source: Oregon Health Authority. 15
d Rate is per 1000 person-years. Data source: Oregon Health Authority. 16
e Persons were classified as unknown if data were missing and as “other” if the response to the question did not fit into the category of white, Asian/Pacific Islander, American Indian/Alaska Native, or black.
f Rural is defined as ≥10 miles from the centroid of a population center of ≥40 000 persons. 18
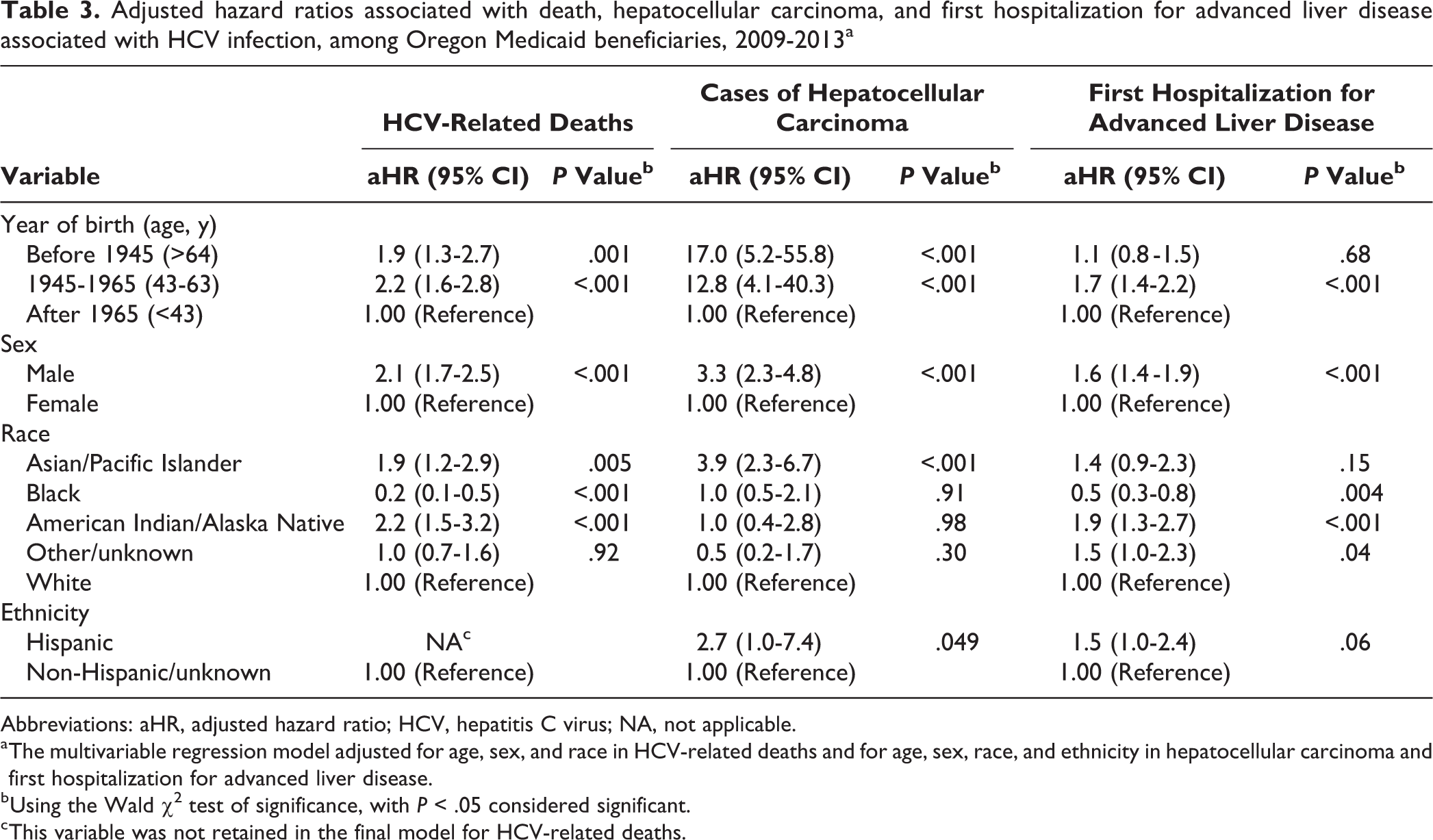
One multivariable regression model retained birth-year group, sex, and race for HCV-related mortality, and a second multivariable regression model retained birth-year group, sex, race, and ethnicity for both HCC and first hospitalization for ALD (Table 3). For HCV-related mortality, the aHR was 2.1 (95% CI, 1.7-2.5) for males compared with females. The aHRs for persons born before 1945 (1.9; 95% CI, 1.3-2.7) and in 1945 through 1965 (2.2; 95% CI, 1.6-2.8) were higher than among persons born after 1965. Both APIs (aHR = 1.9; 95% CI, 1.2-2.9) and AI/ANs (aHR = 2.2; 95% CI, 1.5-3.2) had an elevated risk for HCV-related death compared with white persons. Similarly, the 2 older birth-year groups (birth before 1945: aHR = 17.0 [95% CI, 5.2-55.8]; born in 1945 through 1965: aHR = 12.8 [95% CI, 4.1-40.3), male sex (aHR = 3.3; 95% CI, 2.3-4.8), and API race (aHR = 3.9; 95% CI, 2.3-6.7) were significant risk factors for HCC. We observed a similar trend for first hospitalization for ALD. We found a higher risk for being hospitalized for ALD among persons born in 1945 through 1965 versus after 1965 (aHR = 1.7; 95% CI, 1.4-2.2), males vs females (aHR = 1.6; 95% CI, 1.4-1.9), and AI/ANs vs white persons (aHR = 1.9; 95% CI, 1.3-2.7). Compared with white persons, black persons had the lowest risk for both HCV-related death (aHR = 0.2; 95% CI, 0.1-0.5) and first hospitalization for ALD (aHR = 0.5; 95% CI, 0.3-0.8). In the sensitivity analysis, the magnitude and direction of the aHRs in the subset of HCV Medicaid patients with fewer than 4 years of Medicaid enrollment were similar to those of the entire cohort.
Adjusted hazard ratios associated with death, hepatocellular carcinoma, and first hospitalization for advanced liver disease associated with HCV infection, among Oregon Medicaid beneficiaries, 2009-2013a
Abbreviations: aHR, adjusted hazard ratio; HCV, hepatitis C virus; NA, not applicable.
a The multivariable regression model adjusted for age, sex, and race in HCV-related deaths and for age, sex, race, and ethnicity in hepatocellular carcinoma and first hospitalization for advanced liver disease.
b Using the Wald χ2 test of significance, with P < .05 considered significant.
c This variable was not retained in the final model for HCV-related deaths.
Discussion
We piloted a novel method for estimating the short-term incidence of severe sequelae of HCV infection among Oregon Medicaid beneficiaries. This approach allowed for more complete ascertainment of outcomes despite possible changes in patients’ Medicaid enrollment status (either from loss of Medicaid coverage or a change in coverage) by matching multiple secondary data sources. Simultaneously, it provided baseline estimates of outcomes from a period when direct-acting antiviral agents were not used frequently in the Medicaid population. Although the findings were limited to Oregon, our study provides methods that could be validated and used by other local and state jurisdictions to measure the burden of the complications of HCV infection by using readily available administrative data sets.
In Oregon, public health statutes that give the Public Health Division of OHA broad authority to conduct special studies of public health importance allowed us to proceed without human subjects review, 22 although we did need to develop data-use agreements with the Health Services Division of the OHA to use Medicaid and inpatient hospital discharge data. In addition, within the Public Health Division, we created data-use agreements with the Oregon Cancer Program for OSCaR data and the Center for Health Statistics for access to death certificate data. Although it was daunting to negotiate multiple data-use agreements, given the sensitivity of the diagnosis of HCV infection and the need to use protected health data to conduct the matches, we felt that we benefited from working with these partners to develop a transparent standard operating procedure for creating and implementing rigorous security procedures for conducting the matches and maintaining our data.
In the multivariable model, we found an elevated risk for HCV-related mortality and HCC among API Medicaid patients, which contrasted with earlier findings seen in the Oregon viral hepatitis profile from the same period (2009-2013). 8 In the Oregon viral hepatitis profile, the highest average annual incidence per 100 000 population of HCV-related HCC was found in black persons (5.1 cases) and AI/ANs (4.1 cases) followed by white persons (3.1 cases) and APIs (2.7 cases). 8 Similarly, for HCV mortality, the highest death rates per 100 000 population in the general population occurred among AI/ANs (17.4) and black persons (16.1)—almost twice the rate among white persons (8.9) and more than twice the rate among APIs (5.9). The finding in the Medicaid analysis was driven by the high rates of HCV-related mortality among API Medicaid beneficiaries born before 1945; the HCV Medicaid cohort had a higher proportion of patients born before 1945 than the general population of persons with HCV infection reported to the OHA, and APIs in this cohort were older on average than persons in the other racial groups. A systematic review of HCV infection among Asians found that HCV infection tends to be diagnosed at older ages among Asian immigrants to the United States compared with the general US population, and they are more likely to present with HCC and liver fibrosis. 23 Late presentation among Asian patients might be secondary to possible underuse of health care services among Asians 24 and a lack of awareness on the part of both patients and providers, suggesting that more efforts are needed to promote screening among APIs, even those born before 1945, who would not normally be considered at high risk for HCV infection.
We also found that black race had a lower HR for HCV-related death and first hospitalization for ALD in the Cox proportional hazard models. Other published data suggest that liver fibrosis may progress more slowly in black persons with HCV infection than in persons of other races. 25 However, we found elevated rates of chronic HCC and HCV-related deaths among black persons in the general Oregon population with HCV infection compared with white persons, 8 suggesting the possibility of differences in the incidence of complications of HCV between black Medicaid beneficiaries and black persons who do not receive Medicaid benefits. Given that Medicaid had not yet expanded during the study period, some of the differences could potentially be explained by worse outcomes in uninsured black patients. This issue warrants further study.
Limitations
This study had several limitations. First, estimates of each outcome likely were underestimates, because we did not collect data on events that occurred outside Oregon, with the exception of deaths. Hospitalizations may have been underestimated if patients were admitted to a Veterans Health Administration hospital or other facility that does not report to the state hospital discharge data set. Second, complications such as cirrhosis and HCC take decades to develop 26 ; our study’s 5-year project period therefore did not allow for comparisons with other studies of the natural history of HCV infection, because use of administrative data did not allow us to determine the onset date of the HCV infection. Third, published reports using claims data vary in their methods of classifying HCV infection; the decision to use a single medical claim for HCV infection could have resulted in an overly sensitive analysis compared with analyses that use stricter case definitions. 27,28 Fourth, unmeasured detailed clinical factors that putatively accelerate the progression of liver fibrosis, such as alcohol use 29 or metabolic syndrome, 30,31 could modify the estimates. Data on these factors are not readily available in the Medicaid administrative database; as such, they were not included. Finally, because studies have found that racial misclassification of racial/ethnic minority groups, especially among AI/ANs, can lead to underestimation of mortality and cancer incidence, 32,33 the risk for HCV infection sequelae in nonwhite racial groups also could have been underestimated.
Conclusions
This study may assist policy makers in Oregon in making evidence-based decisions about prioritizing resources for funding treatment of HCV infection in Oregon. As direct-acting antiviral agents become more widely used in Medicaid patients, repeated assessments using these methods will allow evaluation of efforts to alter the trajectory of the HCV epidemic in Oregon. The study also identified a risk group for severe outcomes related to HCV infection that was not previously recognized in Oregon, namely, APIs enrolled in Medicaid. Hence, it will be increasingly important for clinical practice and health care policies to respond to such Oregon-specific estimates by encouraging system-wide efforts to implement hepatitis C testing and linkage to care for APIs born before 1965.
Footnotes
Acknowledgments
The authors thank Atif Zaman, MD, MPH (Division of Gastroenterology and Hepatology, Oregon Health and Science University), and Dan Hartung, PharmD, MPH (College of Pharmacy, Oregon State University), for helpful feedback in the study design. We also thank Jeff Capizzi, BA (HIV/STD/TB Prevention, Oregon Health Authority Public Health Division), for technical assistance with LinkPlus. Part of this study was presented at IDWEEK 2016 (October 26-30) in New Orleans, Louisiana. The research represented in this article is that of the authors and does not reflect the official policy of the Oregon Health Authority.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded through the Centers for Disease Control and Prevention’s Emerging Infections cooperative agreement (grant no. 3U5OCK000197).