
Abstract
Human immunodeficiency virus (HIV) and hepatitis C virus (HCV) infections affect millions of persons around the globe and cause profound morbidity and mortality. A major intersection exists between these two epidemics, with HCV infection being more common in persons with HIV than in the general population, largely due to shared routes of transmission. HCV co-infection increases risk for liver- and non-liver-related morbidity and mortality, making HCV treatment a priority in HIV co-infected persons, but the treatment of HCV in co-infected patients has been daunting for multiple reasons. Until recently, HCV treatment has frequently been deferred due to the low rates of cure, significant adverse effects, burdensome duration of therapy and drug–drug interactions with HIV antiretroviral medications. Untreated HCV has resulted in significant health consequences for the millions of those infected and has led to multiple downstream impacts on our healthcare systems around the world. The development of a remarkable number of new HCV direct-acting agents (DAAs) that are significantly more efficacious and tolerable than the previous interferon-based regimens has transformed this important field of medicine, with the potential to dramatically reduce the burden of infection and improve health outcomes in this population. This review will summarize the epidemiology and clinical impact of HIV/HCV co-infection and current approaches to the treatment of HCV in HIV/HCV co-infected patients.
Epidemiology of HIV/hepatitis C co-infection
Of the approximately 35 million people living with human immunodeficiency virus (HIV) worldwide, an estimated 4–7 million are co-infected with chronic hepatitis C virus (HCV), based on the most recent reports [Soriano et al. 2010; Alter, 2006]. The actual number of co-infected patients is likely significantly higher, given that half of patients with chronic HCV in the United States and in Europe are unaware that they are infected [Denniston et al. 2012; Wiessing et al. 2014], and approximately 14% of HIV-infected individuals living in the United States and 47–85% in Europe are undiagnosed [Centers for Disease Control and Prevention, 2014; Ferrer et al. 2015]. Identification of those with infection is urgently needed in order to improve health outcomes and prevent further transmission of both viruses. In Europe and the United States, it is estimated that 20–30% of HIV-infected persons are co-infected with HCV, yet the prevalence varies widely among subpopulations as the efficiency of viral transmission depends upon the route [Sulkowski et al. 2000; Strader, 2005]. Rates of co-infection are highest in individuals with a history of injection drug use (IDU); an estimated 75–90% of HIV-infected patients with a reported history of IDU are co-infected with HCV. Although the majority of HCV is transmitted via percutaneous exposure, sexual transmission of HCV also occurs in individuals without reported histories of IDU, primarily among HIV-positive men who have sex with men [Hagan et al. 2015].
Outcomes with HIV/HCV co-infection
HIV and HCV co-infection is associated with an increased risk of adverse health outcomes, largely due to the effects of HIV infection on the natural history of HCV. HIV infection is associated with higher rates of HCV replication and therefore higher levels of HCV viremia, although the clinical implications of the increased HCV viremia are unclear [Thomas et al. 1996]. Moreover, HIV-infected persons who become infected with HCV are less likely to spontaneously clear HCV after acute infection, likely as a result of impaired cellular immune response, and are therefore at a higher risk for developing chronic HCV infection [Danta et al. 2008].
While remarkable advances in combination antiretroviral therapy (ART) have transformed HIV infection from an inexorably progressive disease in most individuals to a manageable chronic disease, and enabled HIV mono-infected individuals on therapy to have a life expectancy near that of the general population [Samji et al. 2013], individuals with concomitant chronic HCV infection have significantly worse health outcomes, even when HIV is virologically suppressed on ART [Weber et al. 2006]. Compared with HCV mono-infected patients, HIV/HCV co-infected patients typically experience accelerated rates of liver fibrosis and are consequently at higher risk of developing cirrhosis and hepatic decompensation; the underlying causes are possibly related to HIV-associated immune activation and dysregulation as well as ART-related toxicity, such as the association recently described between the use of an abacavir-lamivudine backbone and higher rates of liver fibrosis progression [Lo Re et al. 2014; Rockstroh et al. 2013; Brunet et al. 2016; Graham et al. 2001]. Hepatocellular carcinoma (HCC) is a well-established complication of HCV and has been shown to occur at a younger age and higher rate in co-infected patients [Puoti et al. 2004; Kramer et al. 2015]. The prevalence of end-stage liver disease complications (cirrhosis, liver failure, and HCC) has been rising dramatically over the past 15 years in persons living with HIV, especially among those co-infected with HCV [Ioannou et al. 2013]. Since the development of effective ART, liver disease has become a leading cause of morbidity and mortality in HIV-infected individuals [Kitahata et al. 2009; Monga et al. 2001; Smith et al. 2014]. Furthermore, some studies show that HIV/HCV co-infected patients may also be at higher risk for extra-hepatic end-organ disease, such as bone and kidney disease, compared to those with HIV mono-infection, and have an increase in all-cause, and not just liver-specific mortality [Dong et al. 2014; Lucas et al. 2013; Chen et al. 2009]. Whether and how HCV affects the progression of HIV disease remains unclear.
Optimal management of HCV-associated liver disease in HIV co-infected patients includes treatment of HIV with the goal of sustained HIV virologic suppression. The achievement of HIV virologic suppression with ART reduces, but does not eliminate, the adverse effects of HIV co-infection on the course of HCV disease and the risk of the associated complications described above [Lo Re et al. 2014].
Benefits of treating HCV in HIV/HCV co-infected patients
Because co-infected patients with well-controlled HIV infection remain at higher risk of worse clinical outcomes than HIV mono-infected patients, it is imperative that HCV infection also be effectively treated. The goal of HCV treatment is to achieve a sustained virologic response (SVR), which is considered to be cure. The eradication of HCV in co-infected patients is associated with a significantly lower risk of liver-related complications and improved overall survival [Limketkai et al. 2012; Berenguer et al. 2009]. Non-liver-related mortality may also be reduced with HCV clearance [Berenguer et al. 2012].
Evolution of HCV treatment for HIV/HCV co-infected patients
Data on treatment of HCV infection in HIV/HCV co-infected patients were lacking until 2004, when three randomized controlled clinical trials including co-infected populations were published. These trials, APRICOT, AIDS Clinical Trials Group A5071, and RIBAVIC, compared 48 weeks of standard interferon (IFN) to the same duration of peginterferon in combination with ribavirin. Overall SVR rates were 27–40%, with only 14–29% SVR in genotype 1 patients [Torriani et al. 2004; Chung et al. 2004; Carrat et al. 2004]. Importantly, the rates of SVR in these as well as other trials throughout the remainder of the 2000s were significantly lower in HIV/HCV co-infected patients compared to HCV mono-infected patients, especially among those with genotype 1 HCV infection [Manns et al. 2001]. Anemia and neutropenia were common adverse effects requiring dose reduction, use of hematopoietic growth factors, or drug discontinuation for management. In RIBAVIC but not the other trials, serious adverse events were more frequent than what had been reported among HIV-seronegative patients (35% versus 10–15%), resulting in higher rates of premature treatment discontinuation, in part related to mitochondrial toxicity with co-administration of older HIV nucleoside reverse transcriptase inhibitors (NRTIs; namely didanosine) and ribavirin. In summary, combination peginterferon and ribavirin treatment in co-infected patients led to disappointingly low rates of SVR, required long durations of therapy, and were poorly tolerated. Together with concern for psychiatric adverse effects with IFN-based therapy and poor adherence in a population with significant comorbid psychiatric disease and substance use, rates of HCV treatment initiation in this population were especially low [Fleming et al. 2005].
The first HCV direct-acting antivirals
Hepatitis C direct-acting antiviral agents (DAAs), which target HCV non-structural (NS) proteins essential to viral replication, fall into the following classes: NS3/4A protease inhibitors (PIs), NS5B nucleot(s)ide inhibitors, NS5B non-nucleoside inhibitors, and NS5A inhibitors. In 2011, the first DAAs, the first-generation HCV NS3/4A PIs telaprevir and boceprevir, were approved for genotype 1 HCV mono-infected patients. The addition of telaprevir or boceprevir to peginterferon and ribavirin improved SVR rates in phase II trials to 74% and 63%, respectively, among predominantly non-cirrhotic patients co-infected with HIV and previously untreated genotype 1 HCV, similar to responses seen in HCV mono-infected patients [Sulkowski et al. 2013b; Sulkowski et al. 2013a; Jacobson et al. 2011; Poordad et al. 2011]. Despite the improved SVR rates, the regimens still required 24–48 weeks of treatment and were accompanied by an even higher frequency of toxicities than with peginterferon and ribavirin alone, such as severe anemia, neutropenia, and rash. The safety profile was particularly poor in cirrhotic patients, with a high incidence of serious adverse events, including deaths, observed in a real-world compassionate use cohort of HCV mono-infected patients [Hezode et al. 2014]. In addition, as telaprevir and boceprevir are inhibitors of the cytochrome P450 (CYP)3A4 enzyme, there were significant drug–drug interactions (DDIs) with antiretroviral (ARV) agents, as well as other commonly used medications, that limited their use in HIV co-infected patients [Hulskotte et al. 2013; Kiser et al. 2012]. Given the limited safety and efficacy data in co-infected patients, the US Food and Drug Administration (FDA) also did not approve a specific indication for the use of telaprevir and boceprevir in this population. These drugs should not be used today, given the further advancements in HCV treatment.
Current HCV therapy for HIV/HCV co-infected patients
Further advancements made in the development of highly efficacious, safe, well-tolerated, all oral, direct-acting HCV regimens without the need for IFN have revolutionized HCV treatment. Modern HCV DAAs have been especially transformative for co-infected patients, as they have closed the gap in treatment responses previously seen between mono- and co-infected patients. Figure 1 illustrates the narrowed gap in treatment response rates over the years of HCV treatment advances. Here, we will summarize information regarding the current agents available for the treatment of HIV/HCV co-infected patients, and describe the relevant clinical trials. The rapid pace of HCV drug development results in published recommendations that quickly become outdated. Up-to-date guidance on HCV treatment recommendations are available through the European Association for the Study of the Liver (EASL) guidelines at http://www.easl.eu/research/our-contributions/clinical-practice-guidelines and the American Association for the Study of Liver Diseases/Infectious Diseases Society of America (AASLD/IDSA) guidance at http://www.hcvguidelines.org. With the current regimens proving equally efficacious for both HCV mono-infected and HIV/HCV co-infected patients, the recommended regimens for the treatment of co-infected patients are the same as for HCV mono-infected patients, with the additional consideration of potential DDIs with HIV ARVs. We suggest the frequent use of a drug interactions software program to review potential drug interactions, not just with HIV ARVs, but with other medications for comorbid conditions, as well. One resource that is frequently updated is the University of Liverpool drug interactions website, http://www.hep-druginteractions.org. Given the accelerated disease seen with HIV co-infection, HIV co-infected patients are considered a high priority group for treatment, regardless of stage of fibrosis.
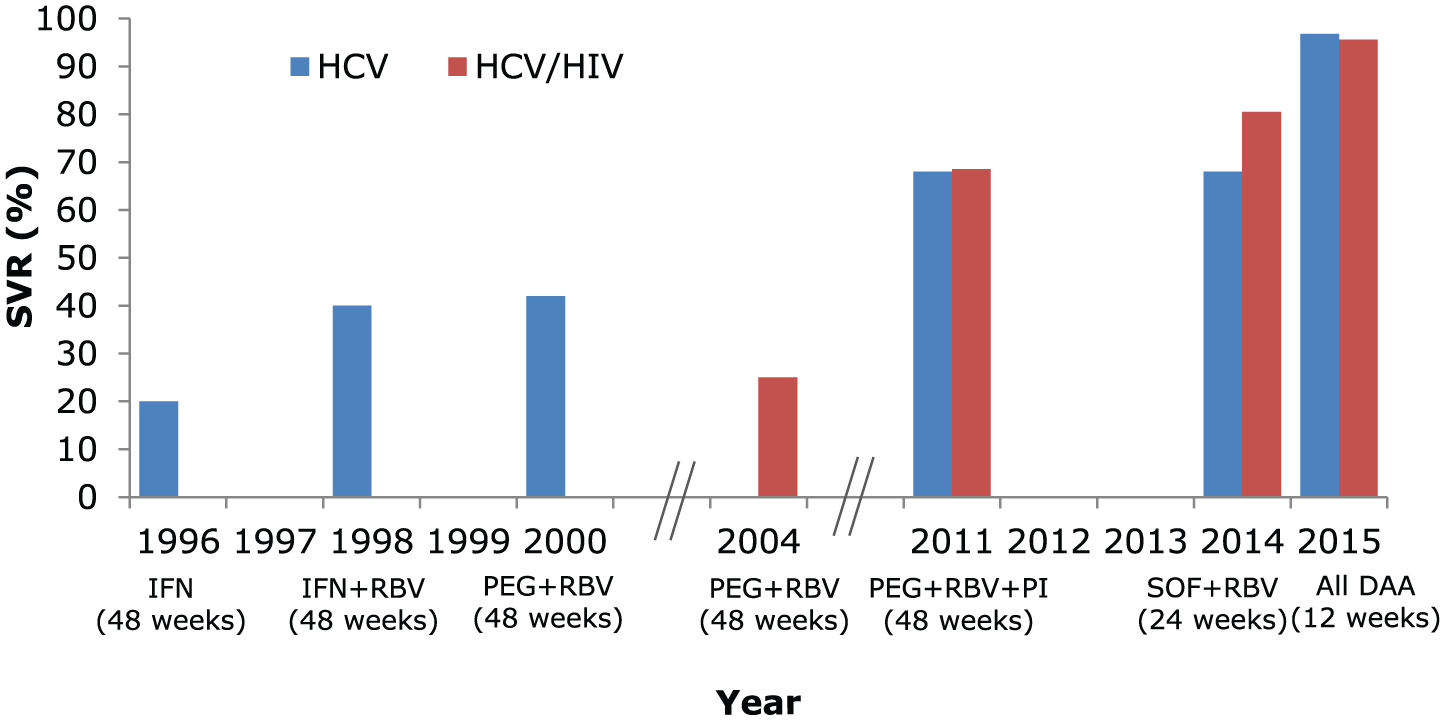
Improvements in hepatitis C virus (HCV) treatment and narrowed gap in SVR between HIV/HCV co-infected and HCV mono-infected persons (genotype 1, treatment-naïve).
Review of newer HCV antiviral agents
Since the introduction of boceprevir and telaprevir, multiple new agents have become available, including NS5B nucleotide and non-nucleoside inhibitors, NS5A inhibitors, and ‘second-wave’ PIs. All of the currently available agents have activity against genotype 1 HCV, with fewer having broader genotypic activity. Perhaps the most groundbreaking advancement in HCV therapy was the development of the potent pan-genotypic agent, sofosbuvir, the first and only approved nucleotide analogue inhibitor of the HCV NS5B polymerase. Comprehensive pharmacokinetic studies of sofosbuvir and its renally excreted metabolite, GS-331007, have shown minimal or no DDIs with a wide variety of ARV drugs; it is neither induced nor inhibited by CYP enzymes, although some interactions exist related to intestinal efflux transporters, such that it should not be co-administered with potent inducers of intestinal efflux transporters, such as rifampin, which may be more commonly used in HIV co-infected persons due to other co-infections [Kirby et al. 2015]. Furthermore, it has a high barrier to resistance, in comparison to the currently available agents in the other DAA classes, where resistance commonly develops in the setting of virologic failure. The combination of sofosbuvir and ribavirin was the first IFN-free HCV regimen approved for co-infected patients.
Table 1 summarizes the currently available all-oral regimens for the treatment of HCV, by HCV genotype. Specifics of therapy including durations of therapy and when to include ribavirin are not provided as they may depend on genotype 1 subtype, baseline NS3 or NS5A resistance polymorphisms, treatment history, and cirrhosis status, and reference should be made to the available guidelines for the current recommendations [AASLD-IDSA, n.d., EASL, 2016]. In the next section, we will review the clinical trials data for these regimens, with the exception of the regimen of sofosbuvir plus simeprevir, for which no clinical trial was conducted in co-infected patients. Simeprevir is a second-wave first-generation PI that was approved in 2013 for the treatment of genotypes 1 and 4 infection. Simeprevir plus sofosbuvir with or without ribavirin was studied in a small phase II study of HCV mono-infected patients and has been used in clinical practice since, and can be considered in HIV/HCV co-infected patients [Lawitz et al. 2014]. Simeprevir co-administered with peginterferon and ribavirin has been studied in HIV/HCV co-infected patients, but there is little role for this regimen today [Dieterich et al. 2014]. Because of the potential for significant DDIs, simeprevir should not be used with a number of ARV agents, including efavirenz, etravirine, nevirapine, cobicistat, and HIV-1 PIs [Kiser et al. 2013]. Subsequently, two additional HCV PIs have been introduced: paritaprevir (approved in combination with ritonavir, ombitasvir, an NS5A inhibitor, and dasabuvir an NS5B non-nucleoside polymerase inhibitor, in the United States and Europe, in 2014 and 2015, respectively, and referred to as PrOD), and grazoprevir (co-formulated with elbasvir, an NS5A inhibitor), recently approved in 2016 in the United States and Europe. Additional NS5A inhibitors have also been approved, including ledipasvir, co-formulated with sofosbuvir (approved in 2014 in Europe and the United States), daclatasvir (approved in 2014 and 2015 in Europe and the United States, respectively), and velpatasvir, co-formulated with sofosbuvir (approved in 2016 in Europe and the United States). A review of the clinical data on the use of these agents in the treatment of HIV/HCV co-infection will be discussed in further detail below.
Currently available all-oral regimens for the treatment of hepatitis C, by genotype.

HCV, hepatitis C virus.
Inclusion of ribavirin varies by regimen and may depend on HCV subtype (genotype 1a or 1b), prior treatment experience, cirrhosis status (present or absent and compensated or decompensated), and presence of HCV resistance mutations.
Review of clinical trials of IFN-free HCV treatment in HIV/HCV co-infected patients
We focus here on the HCV treatment trials of IFN-free therapy published to date involving HIV/HCV co-infected patients, summarized in Table 2. Although there are substantially more data on the use of DAAs in HCV mono-infected patients, these trials show the efficacy rates between the two groups to be strikingly similar. All of the trials were open-label studies that evaluated the efficacy and safety of an orally administered, IFN-free regimen, and all trials used SVR at 12 weeks (SVR12) as their primary end point. A majority of the patients studied in these trials had well-controlled HIV and were adherent to various ARV regimens. Participants were HCV treatment-naïve or previously treated with an IFN-based regimen or a single DAA plus ribavirin. Recommended dosing is summarized in available guidelines [AASLD-IDSA, n.d., EASL, 2016]. We will not discuss re-treatment of all-DAA failures given the more limited data and lack of published clinical trial data at this time.
Summary of sustained virologic response rates in published HCV treatment trials in HIV/HCV co-infected patients.
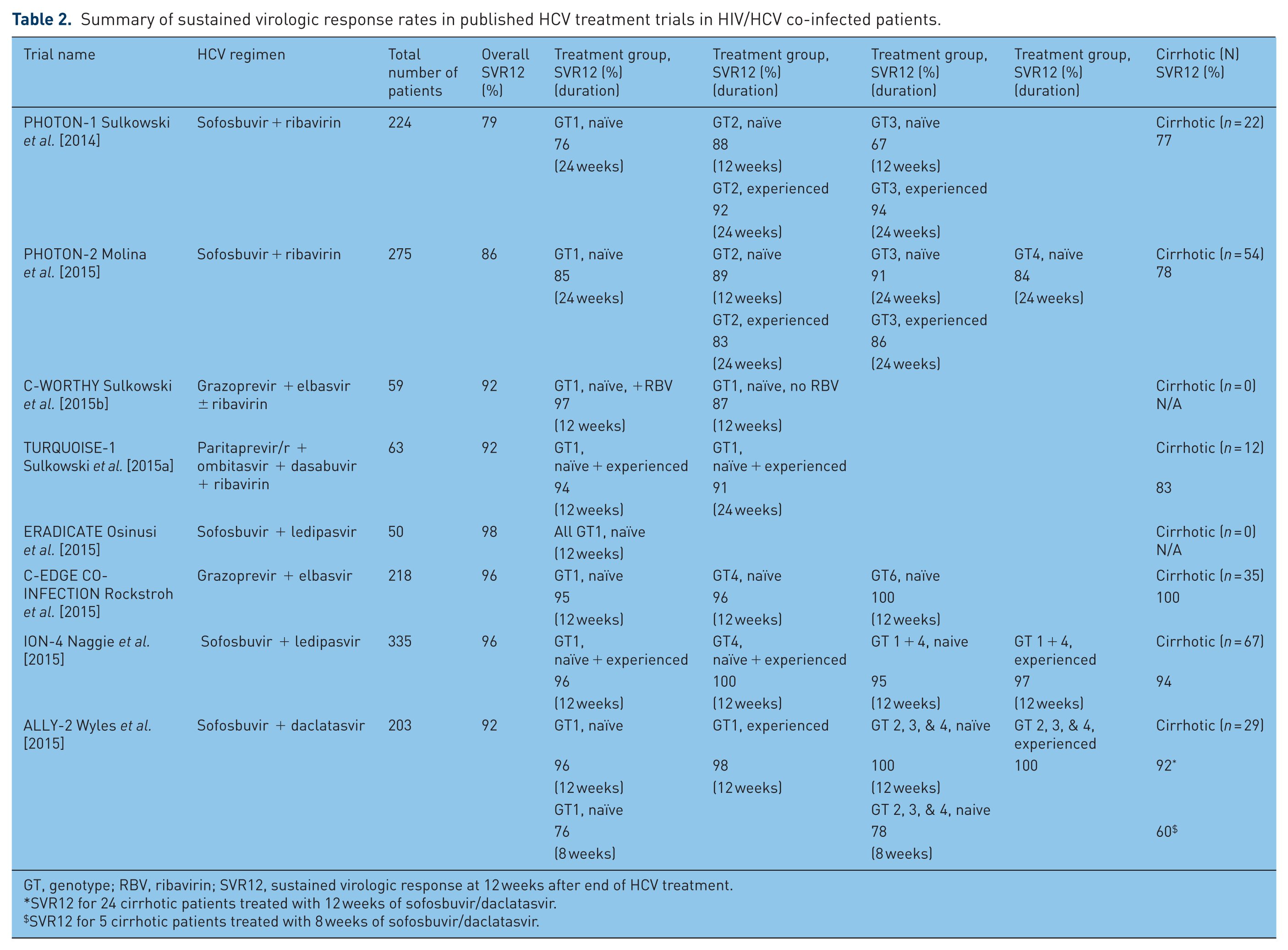
GT, genotype; RBV, ribavirin; SVR12, sustained virologic response at 12 weeks after end of HCV treatment.
SVR12 for 24 cirrhotic patients treated with 12 weeks of sofosbuvir/daclatasvir.
SVR12 for 5 cirrhotic patients treated with 8 weeks of sofosbuvir/daclatasvir.
Sofosbuvir and ribavirin
There have been two phase III trials of sofosbuvir plus ribavirin in HIV/HCV co-infected patients, the PHOTON-1 and PHOTON-2 trials. The PHOTON-1 trial examined sofosbuvir in combination with weight-based ribavirin for 12 or 24 weeks in treatment-naïve patients infected with HCV genotypes 1, 2, and 3, and in treatment-experienced patients with genotypes 2 and 3, all of whom were co-infected with HIV [Sulkowski et al. 2014]. PHOTON-1 was a multi-center, open-label, nonrandomized phase III trial conducted between August 2012 and March 2013 at 34 sites in the United States and Puerto Rico. ARV regimens included ritonavir-boosted atazanavir, ritonavir-boosted darunavir, efavirenz, raltegravir, or rilpivirine in combination with tenofovir/emtricitabine. A total of 223 patients were included in the primary analysis, of whom 114 patients (51%) had genotype 1 infection and 52 patients (23%) identified as black – a notable proportion given that black patients with genotype 1 HCV have historically had lower rates of response to IFN-based therapy and to the first-generation DAAs, boceprevir and telaprevir, and their inclusion in treatment studies is critical to optimizing their treatment outcomes [McHutchison et al. 2000; Wilder et al. 2016]. A minority of participants (22 [10%]) had evidence of cirrhosis (all compensated) prior to enrollment. Rates of SVR12 differed among genotypes and by treatment history (naïve or experienced). Among treatment-naïve patients SVR12 was achieved in 76% of patients with genotype 1, 88% with genotype 2, and 67% with genotype 3. Of treatment-experienced patients with genotypes 2 and 3, 92% and 94% achieved SVR, respectively. Sofosbuvir plus ribavirin was well tolerated, with only 3% discontinuing the study treatment due to adverse events. Moderately severe anemia and hyperbilirubinemia were attributable to the effects of ribavirin, with atazanavir-associated UGT1A1 inhibition likely also contributing to ribavirin-associated hemolysis, which resolved with switch off of atazanavir. Two patients experienced transient breakthrough of HIV viremia, although one of these patients had documented ART nonadherence and neither patient required change of ARV agents. Limitations of the PHOTON-1 study include the absence of HCV treatment-experienced patients infected with genotype 1, an underrepresentation of cirrhotic patients, and the lack of a control group. The study highlighted that genotype 3 patients are more difficult to treat. Response rates in genotype 1–infected persons were also not significantly improved from those seen with boceprevir or telaprevir plus peginterferon and ribavirin. Still, this study heralded a transformative shift towards effective and well-tolerated IFN-free HCV therapy for co-infected patients. In addition, this trial was also one of the first to show overall rates of SVR12 in co-infected patients that were similar to response rates in phase III clinical trials of mono-infected patients treated with sofosbuvir and ribavirin [Jacobson et al. 2013; Lawitz et al. 2013].
The PHOTON-2 trial allowed the same HIV regimens as PHOTON-1 [Molina et al. 2015]. It involved 275 treatment-naïve and experienced patients at 45 sites in 7 European countries and Australia. The study included more patients with compensated cirrhosis (54, or 20%) and in addition to genotypes 1, 2, and 3, included 31 patients with genotype 4 infection. Only 3 (1%) black patients were enrolled in the study. All patients in PHOTON-2 were treated for 24 weeks except for treatment-naïve genotype 2 patients, who received 12 weeks of treatment. Ninety-five (85%) treatment-naïve patients with genotype 1 infection achieved SVR12, compared to 76% in PHOTON-1, and compared to 68% in the SPARE trial, which studied sofosbuvir and ribavirin for 24 weeks in genotype 1 HCV mono-infected patients [Osinusi et al. 2013]. SVR12 rates in treatment-naive genotype 2 and 3 participants were 89% and 91%, respectively. Again, few patients (6, or 2%) discontinued study treatment due to adverse events. Until recently, sofosbuvir plus ribavirin had been the primary regimen recommended for genotype 2 infection, but there is no longer a role for this regimen with the availability of two newer agents (fixed-dose combination sofosbuvir/velpatasvir and daclatasvir given with sofosbuvir). For genotypes 1, 3, and 4, further advancements have also been made, as described in the trials below.
Paritaprevir/ritonavir/ombitasvir plus dasabuvir
TURQUOISE-1 was a small phase II trial conducted at 17 sites in the United States and Puerto Rico. It evaluated 63 HCV genotype 1 co-infected patients treated with an all-oral regimen of weight-based ribavirin and 3 DAAs, paritaprevir (a NS3/4A PI, co-dosed/boosted with ritonavir), ombitasvir (a NS5A inhibitor), plus dasabuvir (a non-nucleoside NS5B inhibitor) (PrOD) [Sulkowski et al. 2015a]. The majority (65%) of patients were treatment-naïve and the remainder previously failed peginterferon plus ribavirin. Patients were randomized to 12 or 24 weeks of therapy. Fifty-six patients (89%) were infected with genotype 1a, 7 (11%) with genotype 1b, 15 (24%) identified as black, and 12 patients (19%) had compensated cirrhosis prior to enrollment. All were on ART with either raltegravir or ritonavir-boosted atazanavir (ritonavir given through the HCV regimen while on treatment) plus two HIV-1 NRTIs. SVR12 was achieved in 29 (94%) of those treated for 12 weeks and 29 (91%) who completed 24 weeks of therapy. Adverse events were common (most often fatigue, insomnia, nausea, and headache), but none were serious and no patients discontinued treatment due to an adverse event. Seven patients (11%) experienced grade 2 declines in hemoglobin (<10 g/dl), likely related to ribavirin toxicity. Treatment-emergent NS3, NS5A, and NS5B resistance-associated variants (RAVs) were detected in patients with virologic failure. The high rates of SVR and excellent safety profile were consistent with phase III studies of this regimen in HCV mono-infected patients [Feld et al. 2014]. Of note, the PrOD regimen should not be used for HIV/HCV co-infected patients who are not HIV virologically suppressed on ART, and expected to remain HIV suppressed during PrOD treatment, since ritonavir has anti-HIV activity and could potentially select for HIV PI resistance. Due to drug interactions related to CYP3A4 and transporters, compatible ARV regimens are also limited, and this regimen should not be used with efavirenz, etravirine, nevirapine, rilpivirine, HIV PIs other than atazanavir or possibly darunavir, or co-formulated elvitegravir/cobicistat, atazanavir/cobicistat, or darunavir/cobicistat, given the inclusion of ritonavir in PrOD and additional boosting. PrOD is a recommended regimen for HCV genotype 1 treatment. Paritaprevir/ritonavir/ombitasvir with weight-based ribavirin and without dasabuvir is recommended for HCV genotype 4 treatment. Several limitations to their current use include a higher pill burden compared with other available regimens, need for ribavirin in genotype 1a and 4 patients, and post-marketing experience concerning for serious liver injury with hepatic decompensation and liver failure noted in patients with underlying advanced cirrhosis [FDA, 2015a].
Sofosbuvir plus ledipasvir
The fixed-dose combination regimen of sofosbuvir plus ledipasvir (an NS5A inhibitor) has been studied in two HIV/HCV co-infection trials, ERADICATE and ION-4. The ERADICATE trial was a single-center, phase IIb pilot study that was conducted at the National Institute of Allergy and Infectious Diseases (NIAID) [Osinusi et al. 2015]. This study evaluated 50 previously untreated HCV genotype 1 patients with HIV co-infection (both on and off ART) who were given 12 weeks of sofosbuvir/ledipasvir. A majority (84%) of the patients identified as black. Patients with cirrhosis were excluded, although 13 (26%) had stage 3 liver disease. Seventy-eight percent had subtype 1a infection. Of the 37 on ART, all received tenofovir disoproxil fumarate (TDF)-emtricitabine in addition to efavirenz, raltegravir, or rilpivirine (or a combination of the latter). Median CD4 cell count was 576 and 687 cells/mm3 for the groups on ART and not on ART, respectively. The overall SVR12 rate was a remarkable 98% (49 out of 50 patients). One patient experienced HCV relapse and by deep sequencing had a detectable NS5A RAV, Y93H, which was present at baseline and enriched during the study. The regimen was very well tolerated without any discontinuations, and without any serious adverse events attributable to the study drugs. Co-administration of ledipasvir with TDF can lead to increases in tenofovir levels and potential renal toxicity; no significant changes in renal function were observed. This study was small, and it excluded patients with cirrhosis, but it was the first study to show SVR rates greater than 90% in HIV/HCV co-infected patients treated with an IFN- and ribavirin-free regimen.
ION-4 is the largest of the HCV treatment studies involving HIV/HCV co-infected patients [Naggie et al. 2015a]. This study included 335 patients at 60 different sites in the United States, Puerto Rico, Canada, and New Zealand. Like the ERADICATE study, ION-4 evaluated the efficacy and safety of 12 weeks of fixed-dose once daily combination sofosbuvir and ledipasvir. In contrast to the ERADICATE study, however, ION-4 also included genotype 4 and treatment-experienced patients. The allowed HIV regimens were the same as for ERADICATE. The study included 327 genotype 1 (75% genotype 1a and 23% 1b) and 8 (2%) genotype 4 patients. One hundred eighty-five (55%) were treatment-experienced and 67 (20%) had cirrhosis. All but 13 out of 335 patients (96%) achieved SVR12: 314 out of 327 with genotype 1 (96%); all 8 with genotype 4 (100%); 63 out of 67 patients with cirrhosis (94%), 259 out of 268 without cirrhosis (96.6%); 103 out of 115 black patients (89.6%), 216 out of 217 non-black patients (99.5%); 143 out of 150 treatment-naïve (95%); and 179 out of 185 treatment-experienced patients (97%). Of the 13 who did not achieve SVR, 10 had a virologic relapse. All 10 with relapse were black, and 7 of these patients had the TT allele in the IL28B gene. While the TT allele had previously been associated with increased risk of treatment failure with IFN-containing regimens, the IL28B genotype has not appeared to influence treatment response with IFN-free DAA regimens to date. Eight of the 10 patients with relapse were receiving efavirenz. A multivariate analysis identified black race as the only factor significantly associated with virological relapse. Neither race nor ART regimen was observed to affect pharmacokinetic parameters in the study. The role of race and ART regimen or their interaction in the mechanism of these treatment failures remains unclear, but the findings are provoking. This association was not observed in the phase III HCV mono-infection studies, which included 308 HCV mono-infected black patients treated with sofosbuvir/ledipasvir [Afdhal et al. 2014a, 2014b; Kowdley et al. 2014]. The regimen was very well tolerated overall and the safety profile similar to that observed in HCV mono-infected patients. Of note, however, 4 patients developed treatment-emergent worsening of renal function (increases ⩾0.4 mg/dl in serum creatinine), which were possibly related to higher tenofovir exposures. Phase I studies showed that sofosbuvir/ledipasvir and TDF co-administration resulted in 40–60% increases in exposure to tenofovir, compared to TDF-containing ART alone [Gilead Sciences, 2015]. Because of the potential for ledipasvir to increase tenofovir levels, it is recommended that baseline and ongoing renal function be closely monitored, and that consideration be made for changing the ART regimen (particularly if on a ritonavir-boosted HIV PI and TDF, where tenofovir levels are further increased) or selecting a different HCV treatment regimen in those at high risk for renal toxicity, including pre-existing renal disease with creatinine clearance <60 ml/min. Elvitegravir/cobicistat is also expected to potentiate this tenofovir effect (and cobicistat levels are markedly increased with coadministration with sofosbuvir/ledipasvir), and coadministration is not recommended. Tenofovir alafenamide (TAF) may be an alternative to TDF, but safety data are not yet available for the coadministration of TAF with other ARVs plus sofosbuvir/ledipasvir in co-infected patients. In addition to these drug interactions, other potential interactions exist related to transporter (primarily P-glycoprotein) effects and reduced absorption of ledipasvir with medications that increase gastric pH [EASL, 2016].
The ION-4 study demonstrated that sofosbuvir/ledipasvir achieves high rates of SVR similar among treatment-naïve cirrhotic and non-cirrhotic patients, as well as in patients who previously failed DAA/peginterferon/ribavirin or sofosbuvir/ribavirin, with an excellent safety profile. With the caveat of potential renal toxicity with tenofovir when co-administered with select ARVs, this regimen improved access to HCV treatment for HIV co-infected patients as nearly all available ARVs, including HIV PIs, can be administered with it. It also offered the simplicity of a single tablet daily regimen. Sofosbuvir/ledipasvir is currently a recommended regimen for genotypes 1, 4, 5, and 6 infection. While ribavirin was not included in ION-4, it is recommended in addition to sofosbuvir/ledipasvir in select settings for harder-to-treat genotype 1 patients (see EASL and AASLD/IDSA guidelines) [EASL, 2016; AASLD-IDSA, n.d.].
Sofosbuvir plus daclatasvir
ALLY-2 was a phase III trial that studied the regimen of sofosbuvir and daclatasvir (a NS5A inhibitor) in 203 HIV/HCV co-infected patients [Wyles et al. 2015]. The trial was conducted at 37 sites in the US and it included patients with HCV genotypes 1 (83% of patients), 2 (9%), 3 (6%), and 4 (2%). Both HCV treatment-naïve (n = 151) as well as treatment-experienced (n = 52, prior IFN-based treatment or sofosbuvir plus ribavirin) patients were enrolled, and 29 patients (14%) with cirrhosis were included; 34% were black. Treatment-naïve patients were randomly assigned in a 2:1 ratio to receive either 12 or 8 weeks of therapy. All treatment-experienced patients received 12 weeks of treatment. Since daclatasvir is a CYP3A4 substrate, it is susceptible to important drug interactions with medications that induce or inhibit the CYP3A4 enzyme. Based on pharmacokinetic data with ARV CYPA3A4 inducers and inhibitors, the dose of daclatasvir was decreased (from the standard 60 mg dose to 30 mg) in patients receiving ritonavir-boosted PIs and increased to 90 mg in patients receiving efavirenz or nevirapine [Bifano et al. 2013]. ALLY-2 allowed the broadest range of ARV agents among the trials discussed: darunavir-ritonavir, atazanavir-ritonavir, lopinavir-ritonavir, efavirenz, nevirapine, rilpivirine, dolutegravir, raltegravir, enfuvirtide, maraviroc, tenofovir, emtricitabine, abacavir, lamivudine, and zidovudine. Among those who received 12 weeks of daclatasvir and sofosbuvir, the overall rate of SVR12 was 97% across all four HCV genotype groups. SVR12 rates among treatment-naïve and treatment-experienced patients were 97% and 98%, respectively. The SVR12 rate among cirrhotic patients treated for 12 weeks was 92% (22 out of 24 patients). Although on-treatment HCV RNA responses were similar between the 8- and 12-week treatment groups, the 8-week regimen was shown to be significantly inferior to the 12-week regimen, with an overall SVR12 rate of 76% compared to 97%. The regimen was safe and well tolerated among all subgroups. HCV relapse was observed in 12 patients. Relapse rates were higher among patients who had a high baseline HCV RNA level (>2 million IU/ml) and were given 8 weeks of therapy. Nine out of the 12 patients who experienced HCV relapse were patients who were administered the lower (30 mg) dose of daclatasvir while on concomitant ritonavir-boosted darunavir. Subsequent data indicated that the dose of daclatasvir should not be reduced with ritonavir-boosted darunavir or lopinavir. Regarding resistance, several of those who relapsed had detectable treatment-emergent NS5A resistance variants (Q30R/E).
ALLY-2 demonstrated that 12 weeks of HCV treatment with sofosbuvir plus daclatasvir was highly efficacious and well tolerated among HIV/HCV co-infected patients across HCV genotypes 1–4 (predominantly genotype 1), regardless of prior treatment experience and race. A wide range of ARVs can be co-administered with sofosbuvir plus daclatasvir, but with dose adjustment for select agents, including ritonavir-boosted atazanavir and efavirenz. Additional drug interactions to consider include effects via the P-gp and OATP1B1 transporters. There were few cirrhotic patients in ALLY-2 and data in HCV mono-infected patients has suggested that 12 weeks of sofosbuvir plus daclatasvir does not provide adequate efficacy for cirrhotic patients [Poordad et al. 2015]. The optimal duration of treatment for cirrhotic patients is unknown; at this time, the recommendations include extension of therapy to 24 weeks, with or without ribavirin [EASL, 2016; AASLD-IDSA, n.d.]. Also still to be clarified is the impact of baseline NS5A resistance polymorphisms on treatment outcome. The presence of baseline NS5A resistance polymorphisms, namely the RAV Y93H, appears to have an adverse impact on SVR rates in genotype 3 infected patients, and particularly those with cirrhosis; in this setting, baseline NS5A RAV testing is recommended, with the addition of ribavirin to the treatment regimen if Y93H is present. Sofosbuvir plus daclatasvir is currently a recommended regimen for HCV genotypes 1, 2, and 3 infection.
Grazoprevir plus elbasvir
Two published trials of the once daily two-drug combination of grazoprevir (a second-generation NS3/4A PI) plus elbasvir (a NS5A inhibitor) have included HIV/HCV co-infected patients: the C-WORTHY and C-EDGE CO-INFECTION trials. The C-WORTHY trial was an international, randomized, open-label phase II trial that studied 159 HCV mono- and 59 HIV/HCV co-infected patients [Sulkowski et al. 2015b]. All patients were previously untreated and had HCV genotype 1 (78% 1a and 22% 1b). Cirrhotic patients were excluded. Co-infected patients received 12 weeks of therapy and were randomized to the inclusion or not of weight-based ribavirin. The majority of participants had early-stage liver disease (92% F0–F2). Only raltegravir plus 2 NRTIs was allowed for ART. Overall rates of SVR12 were achieved in 54 of 59 co-infected patients (92%), compared to 122 of 129 mono-infected patients (95%), and the safety profile of the regimens was similar in mono- and co-infected patients. None of the patients discontinued the study therapy due to adverse events. There was no statistically significant difference in SVR12 between mono- and co-infected patients, but the HIV group was small and the two groups were not matched demographically to allow for adequate comparison. Rates of SVR12 in co-infected patients were slightly higher in the ribavirin group (28 out of 29, or 97%) than in those not treated with ribavirin (26 out of 30, or 87%). Overall, however, the addition of ribavirin was not associated with higher rates of SVR12, yet it was associated with anemia and increased adverse effects. Although patients with cirrhosis were excluded from this particular study, a parallel arm of the C-WORTHY trial, using the same regimens, did include HCV genotype 1 mono-infected patients with cirrhosis, and rates of SVR12 in these patients were surprisingly high (81 out of 86, or 94%, in the ribavirin group and 80 out of 84, or 95%, in those not treated with ribavirin) [Lawitz et al. 2015].
The C-EDGE CO-INFECTION trial was a nonrandomized, open-label, single-arm phase III trial that followed the C-WORTHY phase II trial and studied the use of grazoprevir and elbasvir in a fixed-dose combination once-daily tablet given for 12 weeks in co-infected patients with HCV genotype 1, 4, or 6 [Rockstroh et al. 2015]. The trial studied 218 HIV/HCV co-infected patients at 37 sites in 9 countries across Europe, the United States, and Australia, including 144 patients infected with HCV genotype 1a (66%), 44 with genotype 1b (20%), 28 with genotype 4 (13%), and 2 with genotype 6 (1%). Thirty-five patients (16%) had cirrhosis. Nearly all were on stable ART, which included tenofovir or abacavir with either emtricitabine or lamivudine plus raltegravir, rilpivirine, or dolutegravir. The overall SVR12 rate was 96% (210 out of 218 patients), similar to the 95% SVR12 rate seen in the C-EDGE Treatment-Naïve trial in HCV mono-infected patients [Zeuzem et al. 2015]. Rates of SVR12 were greater than 94% across all subgroups. An SVR12 was achieved in 136 of 144 patients with HCV genotype 1a (94.4%), 42 of 44 with 1b (95.5%), 27 of 28 with genotype 4 (96.4%), both patients with genotype 6 (100%), and all 35 patients with cirrhosis (100%). Five patients experienced HCV relapse, four with genotype 1a and one with genotype 4, possibly related in genotype 1a patients to baseline or treatment-emergent NS5A RAVs. Treatment-emergent NS3 resistance mutations were also identified in 2 of the genotype 1a patients. Most of the adverse events reported were considered mild and the six serious adverse events were not attributed to the study drugs; as with the other trials, there were no discontinuations of therapy due to adverse events.
Grazoprevir/elbasvir was recently approved by the FDA in the United States and the European Commission for the treatment of genotype 1 and 4 HCV infection. In a pooled analysis, the presence of baseline NS5A polymorphisms at amino acid positions 28, 30, 31, or 93 was associated with SVR12 of 70% (39 of 56) compared with 98% SVR12 if baseline polymorphisms were absent with grazoprevir/elbasvir given for 12 weeks. For genotype 1a patients, testing for NS5A resistance-associated polymorphisms is recommended with extension of treatment from 12 to 16 weeks and the addition of ribavirin, if baseline NS5A polymorphisms are present. ARV options are more limited than with sofosbuvir plus ledipasvir or daclatasvir; due to OATP1B1/3 inhibition and CYP3A induction, efavirenz and HIV PIs may not be used, potentially limiting use of grazoprevir/elbasvir in HIV-infected patients with limited ART options. One benefit of grazoprevir/elbasvir is that it can be administered without dose adjustment in patients with severe renal impairment, including those on hemodialysis; PrOD may also be considered in this setting. Grazoprevir/elbasvir is contraindicated in moderate to severe hepatic impairment (Child-Pugh Class B or C).
Sofosbuvir plus velpatasvir
The fixed-dose combination of sofosbuvir plus velpatasvir (a second-generation NS5A inhibitor), given once daily for 12 weeks with or without ribavirin, is the first pan-genotypic oral regimen to be approved in the United States and Europe for the treatment of all six major HCV genotypes. It has primarily been studied in HCV mono-infected patients, in the published phase III ASTRAL trials. These trials demonstrated the broad and potent activity of sofosbuvir/velpatasvir in HCV treatment-naïve and –experienced patients with HCV genotypes 1 through 6.
ASTRAL-1, ASTRAL-2, and ASTRAL-3 included a total of 1,035 HCV mono-infected patients with or without compensated cirrhosis treated with sofosbuvir/velpatasvir [Feld et al. 2015; Foster et al. 2015]. The combined overall SVR12 rate for patients in these trials was 98%. Treatment outcomes were similar across genotypes, including by genotype 1 subtype (1a versus 1b), and by cirrhosis status (with cirrhosis rates of 14–29% across the studies), with the exception that there did appear to be an adverse impact of cirrhosis status and baseline NS5A RAVs among genotype 3 patients, similar to the experience with daclatasvir, although SVR rates still remained high. In ASTRAL-3, the trial that included patients with HCV genotype 3 infection, the SVR12 rate for sofosbuvir/velpatasvir recipients was 95% (versus 98–100% for genotypes 1, 2, and 4). Sustained virologic response rates were 91% among 80 cirrhotic patients versus 97% among 197 non-cirrhotic patients. Of 43 patients with detectable NS5A RAVs (A30K, L31M, and Y93H) at baseline, 38 (88%) achieved SVR12. Of 25 with Y93H at baseline, 21 (84%) achieved SVR12, compared with 97% SVR12 among the 231 patients without NS5A RAVs at baseline [Foster et al. 2015]. We refer you to the US and European HCV guidelines for the recommendations for the addition of weight-based ribavirin based on pre-treatment NS5A RAV testing. In general, patients with prior HCV treatment experience and/or cirrhosis should have NS5A RAV testing if possible and if Y93H is present, ribavirin should be added to sofosbuvir/velpatasvir. If reliable NS5A RAV testing is not available, ribavirin should be included in the treatment regimen. Per the US guidelines, ribavirin should be added for all treatment-experienced patients with cirrhosis, without regard to NS5A RAV testing. [AASLD-IDSA, n.d., EASL, 2016].
Across the ASTRAL trials in non-cirrhotic and compensated cirrhotic patients, adverse events were minimal and not significantly different from placebo, and fewer than compared to sofosbuvir plus ribavirin. ASTRAL-4 studied sofosbuvir/velpatasvir treatment in 267 HCV mono-infected patients with Child-Pugh class B cirrhosis and HCV genotypes 1, 3, 4, and 6 infection, comparing sofosbuvir/velpatasvir with ribavirin for 12 weeks to sofosbuvir/velpatasvir without ribavirin for 12 or 24 weeks. Patients treated with 12 weeks of sofosbuvir/velpatasvir plus ribavirin had higher rates of SVR12 (94%) compared to those treated for 12 or 24 weeks without ribavirin (83% and 86%, respectively) [Curry et al. 2015].
HIV/HCV co-infected patients were included in the ASTRAL-5 trial. This was a single-arm, open-label phase III trial examining the safety and efficacy of sofosbuvir/velpatasvir for 12 weeks in 106 co-infected patients, with interim results presented at an international meeting [Wyles et al. 2016]. Participants had genotypes 1–4 infection (62% genotype 1a), 19 (18%) had compensated cirrhosis, 31 (29%) were treatment experienced, and 48 (45%) of black race. All patients had virologically suppressed HIV infection, with a mean CD4 cell count of 598 cells/µl (range 183–1513). ARV regimens included darunavir, lopinavir, atazanavir (boosted with ritonavir or cobicistat), rilpivirine, raltegravir, or elvitegravir in combination with either TDF/emtricitabine or abacavir/lamivudine. The SVR12 rate for 104 participants with available SVR12 data was 95% (99 of 104) with similar response rates by cirrhosis status and treatment history and across genotypes, noting the sample size was small (4–11 participants in each group) for genotypes 1b-4. Sofosbuvir/velpatasvir was well tolerated with a similar side effect profile to other DAA regimens (fatigue and headache being the most common adverse events), with indirect bilirubin elevation being the most common laboratory abnormality in participants receiving atazanavir/ritonavir.
There are some important considerations related to ART and other concomitant medications with the use of sofosbuvir/velpatasvir in HIV/HCV co-infected patients. As with sofosbuvir/ledipasvir, sofosbuvir/velpatasvir can increase tenofovir levels, particularly when co-administered with ritonavir- or cobicistat-containing ARV regimens and when tenofovir is given as TDF, and of particular concern in patients with creatinine clearance less than 60 ml/min. In this setting, use of TAF instead of TDF can be considered, although safety data for TAF in this setting are not available at this time; if the combination of TDF with ritonavir or cobicistat is necessary, renal function should be monitored [AASLD-IDSA, n.d.]. Sofosbuvir/velpatasvir should not be co-administered with efavirenz due to observed reductions in velpatasvir concentrations; co-administration with etravirine, nevirapine, and tipranavir/ritonavir is also not recommended due to expected reductions in velpatasvir concentrations [AASLD-IDSA, n.d., EASL, 2016]. Additionally, similar to ledipasvir, velpatasvir solubility is pH dependent and recommendations for co-administration of sofosbuvir/velpatasvir with acid reducing agents should be followed as treatment efficacy may be impacted [Gilead Sciences, 2016]. Additional considerations for DDIs relate largely to P-gp and other transporter and CYP enzyme effects; coadministration with significant P-gp and CYP inducers is contraindicated.
The availability of fixed-dose combination sofosbuvir/velpatasvir is a significant advancement for the treatment of genotypes 2 and 3 HCV infection in patients with and without cirrhosis, eliminating the need for ribavirin and its associated pill burden and toxicities for many patients and allowing a single tablet regimen. Across all genotypes, sofosbuvir/velpatasvir also has the added benefit of an improved resistance profile, although its efficacy has not been established in persons who previously failed treatment with other regimens that included a NS5A inhibitor. The pan-genotypic activity of sofosbuvir/velpatasvir is also attractive, particularly for resource-limited settings where treatment uptake may be limited by access to HCV genotype testing, although considerations in this setting must be made for the available ART and drug interactions.
The clinical trials data reviewed above are limited to treatment-naïve and predominantly IFN-experienced patients, with an underrepresentation of cirrhotic and genotype 3 patients, who remain two of the hardest groups to treat. They highlight that resistance polymorphisms involving all HCV drug targets (NS3, NS5A, NS5B) frequently emerge with treatment failures. The optimal approach to re-treating DAA failures remains to be seen. They also highlight that we have not yet reached a ‘one size fits all’ treatment, particularly for HIV co-infected patients where drug interactions with ARVs continue to impact HCV treatment options, although improving.
Post-marketing experience and US FDA warning on serious bradycardia
In March 2015, the US FDA issued a drug safety communication on serious symptomatic bradycardia that had been observed with coadministration of amiodarone with sofosbuvir given in combination with another DAA (such as ledipasvir, daclatasvir, and simeprevir) [FDA, 2015b], whereby a fatal cardiac arrest had been reported. Bradycardia was observed to occur within hours to up to 2 weeks, and concomitant use of beta blockers, underlying cardiac disease and/or advanced liver disease may increase the risk of this adverse event. Co-administration of amiodarone with sofosbuvir plus any other DAA is not recommended.
Shortening treatment courses for chronic HCV infection in HIV/HCV co-infected patients
The ION-3 trial compared 12 weeks of sofosbuvir/ledipasvir versus 8 weeks of sofosbuvir/ledipasvir with or without ribavirin in HCV mono-infected, treatment-naïve, genotype 1 patients without cirrhosis [Kowdley et al. 2014]. In the primary intention-to-treat analysis, relapse rates were higher with 8 weeks compared to 12 weeks of sofosbuvir/ledipasvir. In post-hoc analyses, relapse rates were similar (2%) between the 12 and 8 week treatment groups when restricting to participants with baseline HCV RNA levels less than 6 million IU/ml, leading to the real-world treatment of some patients with only 8 weeks of sofosbuvir/ledipasvir. The experience with 8 weeks of therapy in co-infected patients is much more limited than in HCV mono-infected patients, and limited in the published literature to 35 HIV/HCV co-infected patients included in the real-world GECCO cohort, a prospective multi-center cohort of 9 treatment centers in Germany [Ingiliz et al. 2016]. Of the 35 co-infected patients treated with 8 weeks of sofosbuvir/ledipasvir, all of whom were ART-treated with median CD4 cell count of 601/mm3, mostly male and Caucasian, only 29 fulfilled the criteria for shortened therapy and were included in the effectiveness analysis. On-treatment response was presented for 28 of the 29 patients, with SVR12 achieved in 27 or 28 patients (96.4%). While shortening therapy may be feasible and cost-saving for select patients, the very limited experience in co-infected patients is not sufficient to recommend shorter than 12 week courses of treatment for HIV/HCV co-infected patients at this time [AASLD-IDSA, n.d.].
Treatment of acute HCV in HIV/HCV co-infected patients
Acute HCV, typically defined as the initial period of infection within 6 months of exposure, more often leads to chronic infection in HIV-infected as compared to HIV-uninfected persons [Thomas et al. 2000]. In the past, treatment during acute HCV infection with IFN-based regimens led to higher response rates with shortened courses of therapy [Jaeckel et al. 2001; Kamal et al. 2006]. However, with the high efficacy of currently available DAA regimens when given during chronic infection, the role of treatment during acute infection in both mono- and co-infected patients is unclear. Preliminary data have been presented from two small studies of 12 weeks of sofosbuvir plus ribavirin treatment during acute HCV infection in HIV co-infected persons, the majority on ART, with discrepant results. In a small multi-center clinical trial of 17 participants, 15 with genotype 1 infection, all had undetectable HCV RNA at end of treatment, but only 10 (59%) achieved SVR12 [Naggie et al. 2015b]. A separate single-center study enrolled 13 men, with 1 spontaneously clearing HCV prior to initiating treatment [Fierer et al. 2015]. Of the remaining 12, all with genotype 1 infection, SVR12 was achieved in 11 (92%). One notable difference between the study participants in these two studies was that a greater proportion of participants in the latter cohort bore IL28B CC alleles (58% versus 24%), and it is unclear how many may have had spontaneous clearance instead of treatment response, although median time to treatment was similar (22 versus 20 weeks) [Vispo et al. 2014]. Shortened durations of therapy with all-DAA regimens for acute HCV in co-infected persons are also being examined. Preliminary data have been presented of 6 weeks of sofosbuvir/ledipasvir in 26 co-infected patients with genotype 1 or 4 infection in Europe, where 12 (46%) had the IL28B CC genotype. The SVR12 rate was 77% (20/26, where 3 were documented to have relapsed, 1 was re-infected, and 2 were lost to follow-up), and it appeared that higher baseline viral load was associated with treatment failure. Current European and US guidelines differ in their recommendations for treatment during acute HCV infection. Whereas the EASL guidelines recommend antiviral therapy during acute infection with a shortened duration of 8 weeks (with consideration of extension to 12 weeks if HIV co-infected or with HCV viral load of >1 million IU/ml) of sofosbuvir/ledipasvir, sofosbuvir/velpatasvir, or sofosbuvir/daclatasvir, US AASLD/IDSA guidance recommends monitoring for spontaneous clearance for a minimum of 6 months prior to initiating treatment pending further efficacy and safety data for treatment of acute HCV with IFN-free regimens, unless there are other identified benefits to early treatment, such as prevention of HCV transmission or pre-existing liver disease [AASLD-IDSA, n.d., EASL, 2016]. Per AASLD/IDSA guidance, if treatment is pursued, the same durations of therapy as for chronic HCV infection are recommended. Some studies have suggested rapid progression of liver fibrosis during acute HCV in HIV-infected persons at rates exceeding that observed during chronic infection [Vogel et al. 2012; Fierer et al. 2008]. Whether or not treatment during acute infection would have a significant impact on long-term outcomes is unknown.
Treatment of HCV in HIV/HCV co-infected liver transplant recipients
HIV/HCV co-infected patients who undergo orthotopic liver transplantation (OLT) have lower reported rates of graft and overall survival (approximately 50% at 5 years post-transplant) compared with HIV-infected patients who undergo OLT for non-HCV indications, as well as compared with HCV mono-infected patients [Stock and Terrault, 2015]. Access to liver transplantation for HIV/HCV co-infected patients is thus limited to fewer centers. Data are also limited to guide HCV therapy in OLT recipients. IFN-based regimens used for HCV-infected OLT recipients had low efficacy and high rates of treatment-limiting clinical challenges. A prospective study of 8 co-infected OLT recipients recently conducted at Northwestern University showed that sofosbuvir-based DAA therapy achieved SVR12 in 7 patients (87.5%) and there were no treatment-limiting adverse effects observed [Grant et al. 2016]. Given the complex clinical variables to be considered in transplant recipients, including drug interactions with various immunosuppressive agents and HIV ART, further clinical trials are needed to elucidate the optimal therapeutic approach for OLT recipients, and to optimize OLT outcomes in HIV co-infected patients. Limited access to OLT also suggests that HCV treatment prior to the need for liver transplantation is especially imperative in HIV-infected patients.
Conclusion
Treatment of HCV is considered a high priority for patients co-infected with HIV, given the significantly worse health outcomes associated with co-infection. Historically, treatment uptake in this population has been limited due to a host of factors, such as longer durations of therapy, the myriad and often debilitating toxicities, drug interactions, and suboptimal efficacy. Extraordinary advancements made within just the last few years have introduced a range of excellent treatment options for HIV/HCV co-infected patients. The most recent HCV regimens have closed the gap between HCV mono-infected and co-infected patients with regard to the disparities in efficacy, safety, and drug interactions. The transformative shift in therapeutic options has enormous potential for curing HCV in a great number of individuals, and for dramatically changing the epidemiological landscape of HCV across the globe.
At this time, various barriers to care continue to limit the potential impact of these great new advancements in HCV treatment. In order to take advantage of the strides made toward HCV eradication, it is imperative to overcome barriers at the system, provider, and patient levels. Improvements need to continue in HCV education, testing, and utilization of HCV treatment. Active drug and alcohol abuse, neuropsychiatric disease, and unstable housing among HCV-infected persons continue to be ongoing barriers to access to care; however, several studies have presented convincing evidence that these particular barriers are not contraindications to treatment and that patients with these disadvantages do not necessarily have reduced responses to therapy [Cachay et al. 2015; Robaeys et al. 2013; Barua et al. 2015]. Based on these conclusions, both the EASL and the AASLD/IDSA guidelines favor the treatment of patients with recent or ongoing illicit drug use, in part to prevent the risk of ongoing HCV transmission. It is important, of course, to provide these patients access to harm reduction programs and alcohol and substance use counseling, and that treatment teams consider DDIs with both prescribed and non-prescribed drugs.
Lastly, despite modest increases in access to DAAs, the exorbitant pricing of these agents remains an enormous – and controversial – impediment to treatment. Various healthcare payers frequently deny HCV treatment that has been prescribed for patients, often because of the high costs of these drugs [Trooskin et al. 2015]. Globally, marked variations in drug pricing have been reported [Phelan and Cook, 2014]. The reasons for the high costs of these agents, and the proposals put forth to contain them, are complex and beyond the scope of this review, but until the costs of these agents are made more affordable for patients and healthcare systems, this barrier stands as a significant challenge to disseminating HCV treatment, improving the health outcomes of the millions affected, and eradicating HCV.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: J.A.S. has no conflicts of interest to disclose. K.W.C. has been granted research support to the institution from Gilead Sciences, Inc. and Merck Sharp and Dohme Corp.