
Abstract
Introduction:
Mental health and substance use are growing public health concerns, but established surveillance methods do not measure the burden of these conditions among women of reproductive age. We developed a standardized indicator from administrative data to identify inpatient hospitalizations related to mental health or substance use (MHSU) among women of reproductive age, as well as co-occurrence of mental health and substance use conditions among those hospitalizations.
Materials and Methods:
We used inpatient hospital discharge data from 2012-2014 for women aged 15-44 residing in Illinois and Wisconsin. We identified MHSU-related hospitalizations through the principal International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) diagnosis and first-listed ICD-9-CM external cause of injury code (E code). We classified hospitalizations as related to 1 of 3 mutually exclusive categories: a mental disorder, a substance use disorder, or an acute MHSU-related event. We defined co-occurrence as the presence of both mental health and substance use codes in any available diagnosis or E-code field.
Results:
Of 1 173 758 hospitalizations of women of reproductive age, 150 318 (12.8%) were related to a mental disorder, a substance use disorder, or an acute MHSU-related event, for a rate of 135.6 hospitalizations per 10 000 women. Of MHSU-related hospitalizations, 115 163 (76.6%) were for a principal mental disorder, 22 466 (14.9%) were for a principal substance use disorder, and 12 709 (8.5%) were for an acute MHSU-related event; 42.4% had co-occurring mental health codes and substance use codes on the discharge record.
Practice Implications:
MHSU-related disorders and events are common causes of hospitalization for women of reproductive age, and nearly half of these hospitalizations involved co-occurring mental health and substance use diagnoses or events. This new indicator may improve public health surveillance by establishing a systematic and comprehensive method to measure the burden of MHSU-related hospitalizations among women of reproductive age.
Mental disorders and substance use disorders are leading causes of disability and death in the United States. 1 In 2014, nearly 1 in 5 adults had a mental disorder and nearly 1 in 10 had a substance use disorder. 2 Both mental disorders and substance use disorders are associated with subsequent chronic physical conditions, 3 premature death, 4,5 and deaths due to suicide 5 or accidental overdose. 6 These disorders are also costly; nearly $80 billion was spent on hospitalizations for mental disorders in 2012 in the United States. 7 In addition, mental disorders and substance use disorders often co-occur, and co-occurrence increases the risk of homelessness, incarceration, relapses, chronic medical conditions, and hospital readmission. 8 –14 A study of hospitalization trends in the United States showed that the percentage of hospitalizations related to severe mental illness increased from 1.28% in 1979 to 2.96% in 2008, and the percentage of hospitalizations with co-occurring mental disorders and substance use disorders increased steadily from 0.07% in 1979 to 1.13% in 2008. 8
In addition, mental disorders and substance use disorders pose special risks for the health and well-being of women of reproductive age and their families. Women with mental disorders are at an increased risk of chronic disease, violence, sexually transmitted infections, and premature mortality. 15 –18 Children born to mothers with a mental disorder or substance use disorder have an increased risk of birth defects, infant mortality, low birth weight, mental illness, behavioral problems, chronic diseases, and learning disabilities. 19 –23 Of additional concern is that opioid-involved overdoses are increasing faster among women than among men. 24
Some state maternal and child health programs are addressing women’s mental health or substance use as part of the federal Title V Maternal and Child Health Services Block Grant Program. 25 During the 2015 needs assessment cycle, 16 states identified priority needs relating to mental health or substance use among women. 26 Title V guidance does not specify national outcome or performance measures for mental health or substance use concerns among women, so states prioritizing this topic must create their own measures 25 by relying on standardized indicators when they are available.
In December 2017, the Council of State and Territorial Epidemiologists released a revised report describing recommended surveillance indicators for substance abuse and mental health, based partially on measures from the Substance Abuse and Mental Health Services Administration. Some of the 18 recommended indicators are specific (eg, use of a specified substance), others are broad (eg, counting all mental disorders together, including autism spectrum disorder and Alzheimer’s disease), and none consider co-occurrence. 27 These surveillance indicators may be inadequate for state and local health programs to comprehensively measure, monitor, and address all aspects of mental health or substance use among women.
“Mental disorders” and “substance use disorders” are terms typically used to refer to patients with clinical diagnoses of recognized disorders, as defined by the Diagnostic and Statistical Manual of Mental Disorders (DSM-5). 28 In contrast, “mental health” and “substance use” are terms related more broadly to mental well-being and behavioral health. Our study uniquely identifies hospitalizations related to a broad range of mental health or substance use (MHSU) issues among women, not solely mental disorders or substance use disorders. For example, a suicide attempt is a mental health–related event, but it may occur in the absence of a diagnosed disorder. Including such events is important for comprehensively quantifying the burden of mental health and substance use concerns in the population. Our study uses this framework to describe the development of a standardized indicator that comprehensively identifies MHSU-related inpatient hospitalizations for women of reproductive age.
Materials and Methods
Data Sources
We used inpatient hospital discharge data for Illinois and Wisconsin for discharges occurring during the calendar years 2012, 2013, and 2014. Hospital discharge data are collected by the Illinois and Wisconsin hospital associations and provided to the state public health departments through data-sharing agreements. These data files include data on all inpatient discharges from all nonfederal acute-care hospitals in these 2 states, including psychiatric hospitals, encompassing approximately 200 facilities in Illinois and 150 facilities in Wisconsin. Data on 15 diagnosis code fields and 3 external cause of injury (E code) fields in the Illinois discharge data set were made available for our analysis. Nine diagnosis code fields and 2 E-code fields were made available in the Wisconsin discharge data set. Data files in both states specify a principal diagnosis code field, and the remaining diagnosis fields are deemed “other” diagnosis codes. During our study period, International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes were recorded in the diagnosis and E-code fields. 29
We limited our analyses to hospitalizations of women aged 15-44 at discharge among Illinois residents hospitalized in Illinois (n = 833 085) and Wisconsin residents hospitalized in Wisconsin or Minnesota (n = 340 673). We obtained data from Minnesota through an interstate agreement. We used postcensal population estimates 30 for 2012, 2013, and 2014 as denominators to estimate hospitalization rates per 10 000 women aged 15-44.
Development of MHSU-Related Hospitalization Indicator
We developed an algorithm to identify and classify hospitalizations principally related to MHSU diagnoses and events (Figure 1), drawing from established methodologies in MHSU surveillance. 14,31 –34 First, we used ICD-9-CM diagnosis codes from established Clinical Classification Software (CCS) diagnosis groupings 31 to identify hospitalizations with a principal diagnosis of a relevant mental disorder or substance use disorder (Table 1), as was done in previous studies. 14,32 We excluded hospitalizations with principal diagnoses in certain CCS mental health groupings (delirium, dementia, amnesic, and other cognitive disorders [653]; developmental disorders [654]; or disorders usually diagnosed in infancy, childhood, or adolescence [665]) because they are cognitive or developmental disorders, rather than psychological disorders. 32,33
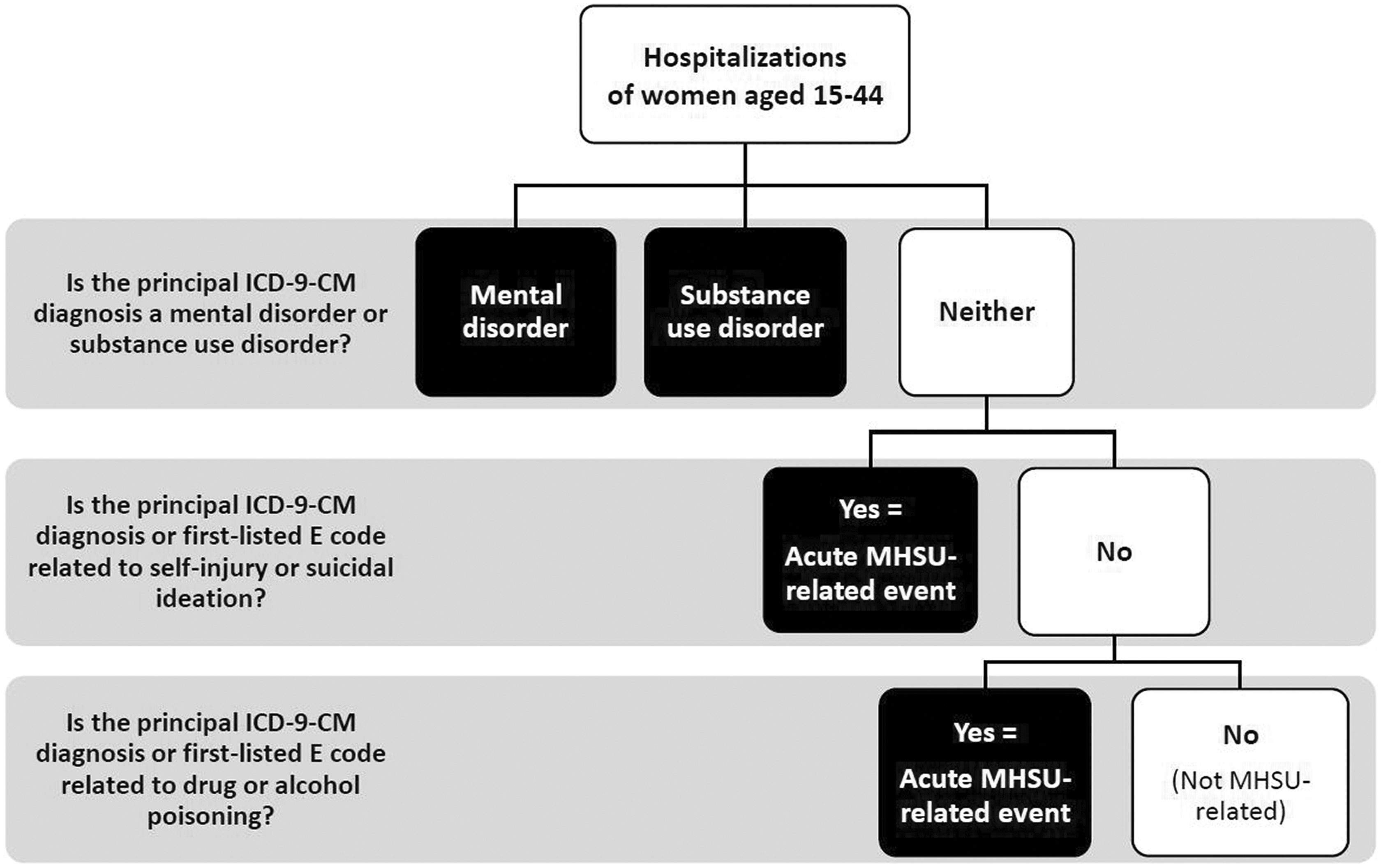
Hierarchy for classifying mental health or substance use (MHSU) hospitalizations among women of reproductive age (aged 15-44). Abbreviations: ICD-9-CM, International Classification of Diseases, Ninth Revision, Clinical Modification; MHSU, mental health or substance use.
International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) diagnosis codes and external cause of injury codes (E codes) used to identify mental health or substance use hospitalizations among women aged 15-44 residing in Illinois and Wisconsin, 2012-2014
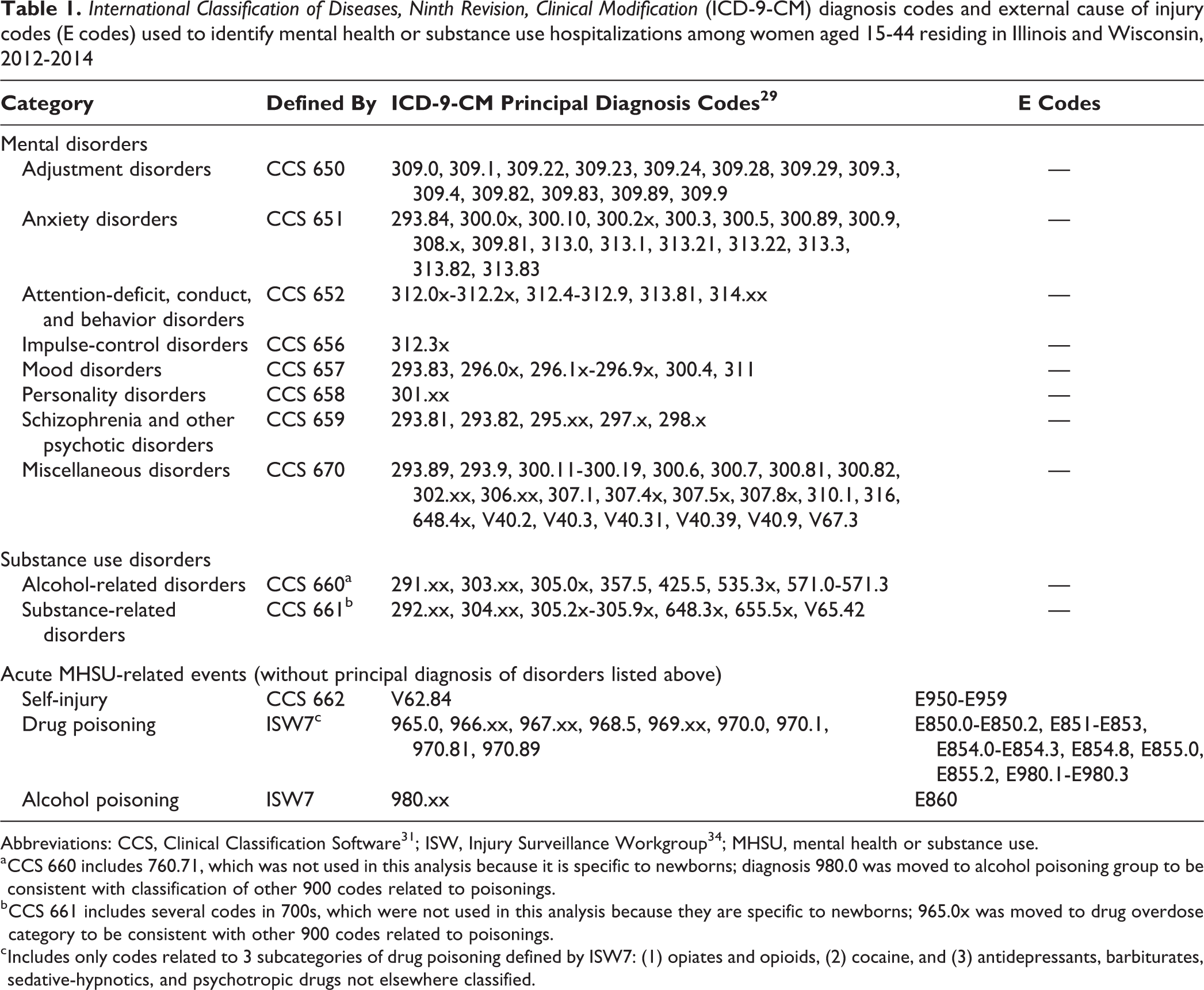
Abbreviations: CCS, Clinical Classification Software 31 ; ISW, Injury Surveillance Workgroup 34 ; MHSU, mental health or substance use.
a CCS 660 includes 760.71, which was not used in this analysis because it is specific to newborns; diagnosis 980.0 was moved to alcohol poisoning group to be consistent with classification of other 900 codes related to poisonings.
b CCS 661 includes several codes in 700s, which were not used in this analysis because they are specific to newborns; 965.0x was moved to drug overdose category to be consistent with other 900 codes related to poisonings.
c Includes only codes related to 3 subcategories of drug poisoning defined by ISW7: (1) opiates and opioids, (2) cocaine, and (3) antidepressants, barbiturates, sedative-hypnotics, and psychotropic drugs not elsewhere classified.
For the next stage of the algorithm, we identified hospitalizations related to self-injury and drug or alcohol poisoning that were not previously identified by a principal diagnosis of a mental disorder or substance use disorder. We defined these admissions as acute MHSU-related events. Among hospitalizations without a principal diagnosis of a mental disorder or substance use disorder, we reviewed principal diagnoses and first-listed E codes for other codes indicating MHSU-related events. We then identified hospitalizations related to self-injury and suicidal ideation by using the CCS definition (category 662). 14,31 –33 Next, we identified drug and alcohol poisonings by using codes from previously defined poisoning surveillance methods of the Safe States Alliance Injury Surveillance Workgroups related to the following: (1) opiates/opioids; (2) cocaine; (3) antidepressants, barbiturates, sedative-hypnotics, and psychotropic drugs not elsewhere classified; and (4) alcohol. 34 If the first-listed diagnosis code and first-listed E code referred to both drug and alcohol poisonings, we used the diagnosis code to classify the type of poisoning. We did not include poisonings by other classes of drugs (eg, nonopioid analgesics) and nondrugs (eg, carbon monoxide) in the MHSU-related hospitalization indicator because of their lower potential for abuse, dependence, or addiction. 24,34
We calculated the hospitalization rate by dividing the number of MHSU-related hospitalizations by the total number of women aged 15-44 in the population. 30 We did not correct for multiple admissions of the same woman, so the indicator is interpreted as the rate of hospitalizations, not the proportion of women who were hospitalized. We also calculated the proportion of MHSU-related hospitalizations by each subcategory (mental disorder, substance use disorder, acute MHSU-related event).
Co-occurrence of MHSU Disorders
Among MHSU-related hospitalizations, we examined all nonprincipal diagnosis codes for evidence of co-occurring mental health and substance use events. As was done in previous studies, we dichotomized ICD-9-CM codes (Table 1) as either mental health–related (mental disorders and self-injury categories) or substance use–related (substance use disorders, drug poisoning, or alcohol poisoning). 14,33 We defined co-occurrence in MHSU-related hospitalizations as the presence of both mental health–related and substance use–related diagnosis codes or E codes (Figure 2). For example, a hospitalization with a principal code of a mood disorder (mental health–related) was classified as co-occurring if we also found an alcohol use disorder, substance use disorder, or drug or alcohol poisoning (substance use–related) code in any of the diagnosis or E-code fields. We calculated the percentage of co-occurrence by dividing the number of MHSU-related hospitalizations with co-occurring mental health and substance use diagnoses by the total number of MHSU-related hospitalizations.
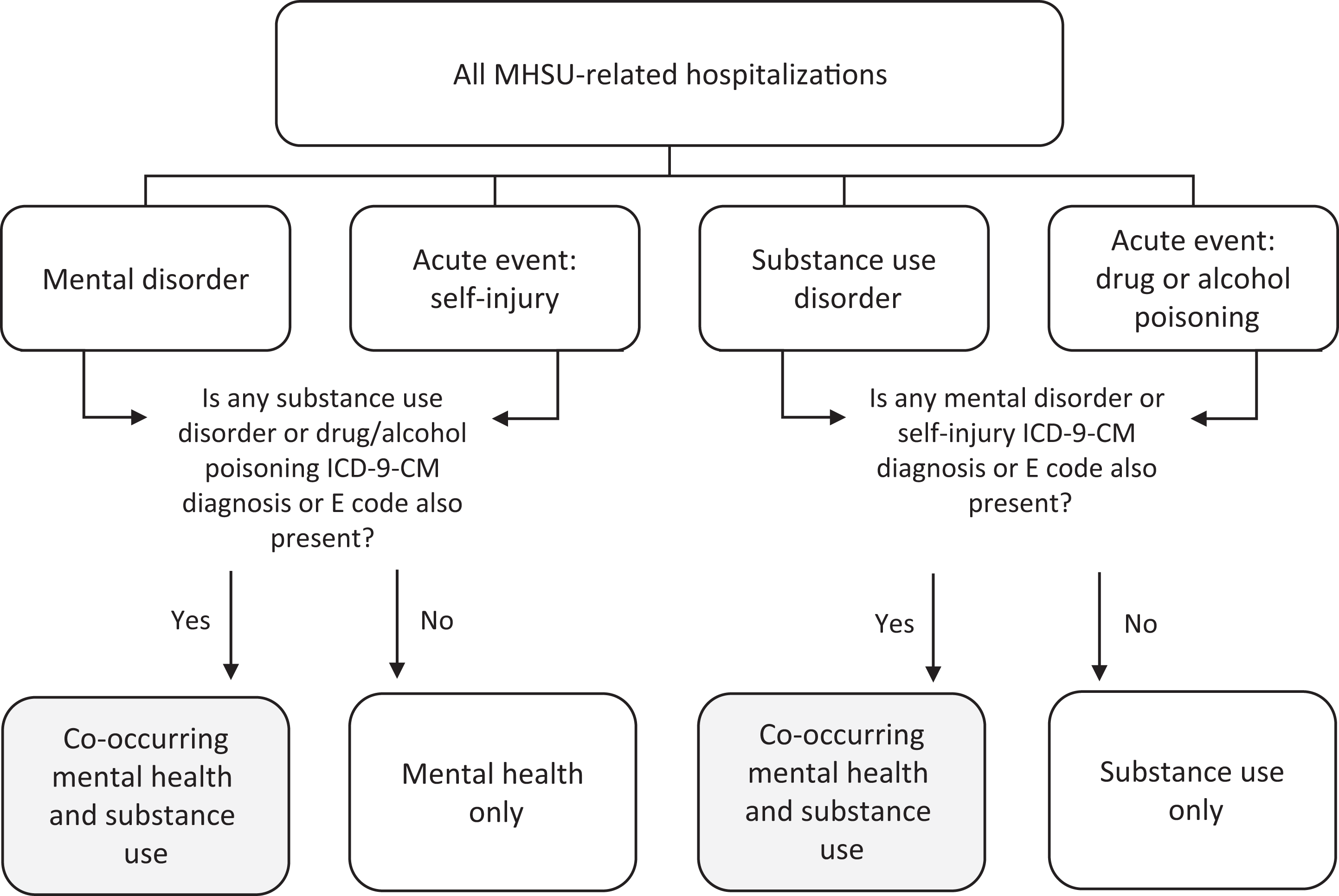
Methods for classifying co-occurrence of mental health and substance use conditions among principal MHSU-related hospitalizations. Abbreviations: ICD-9-CM, International Classification of Diseases, Ninth Revision, Clinical Modification; MHSU, mental health or substance use.
Our study was determined to be public health practice (nonresearch) by the Centers for Disease Control and Prevention and did not require institutional review board review.
Results
Of 1 173 758 inpatient hospitalizations for women of reproductive age in Illinois and Wisconsin during 2012-2014, 150 318 (12.8%) were principally related to MHSU, for a rate of 135.6 hospitalizations per 10 000 women. Among MHSU-related hospitalizations, 115 163 (76.6%) were for a mental disorder, 22 446 (14.9%) were for a substance use disorder, and 12 709 (8.5%) were for an acute MHSU-related event without a principal diagnosis of a mental disorder or substance use disorder (Table 2). Of all MHSU-related hospitalizations for women of reproductive age, more than half (56.7%) had a principal diagnosis of a mood disorder, such as depression or bipolar disorder. Other common causes of MHSU-related hospitalizations were schizophrenia and psychotic disorders (9.0%), drug use disorders (8.1%), alcohol use disorders (6.9%), and self-injury (6.5%). Each of the other MHSU subcategories composed fewer than 6% of the total number of MHSU-related hospitalizations for women of reproductive age.
Inpatient hospitalizations related to mental health or substance use (MHSU) among women of reproductive age (aged 15-44), Illinois and Wisconsin, 2012-2014a
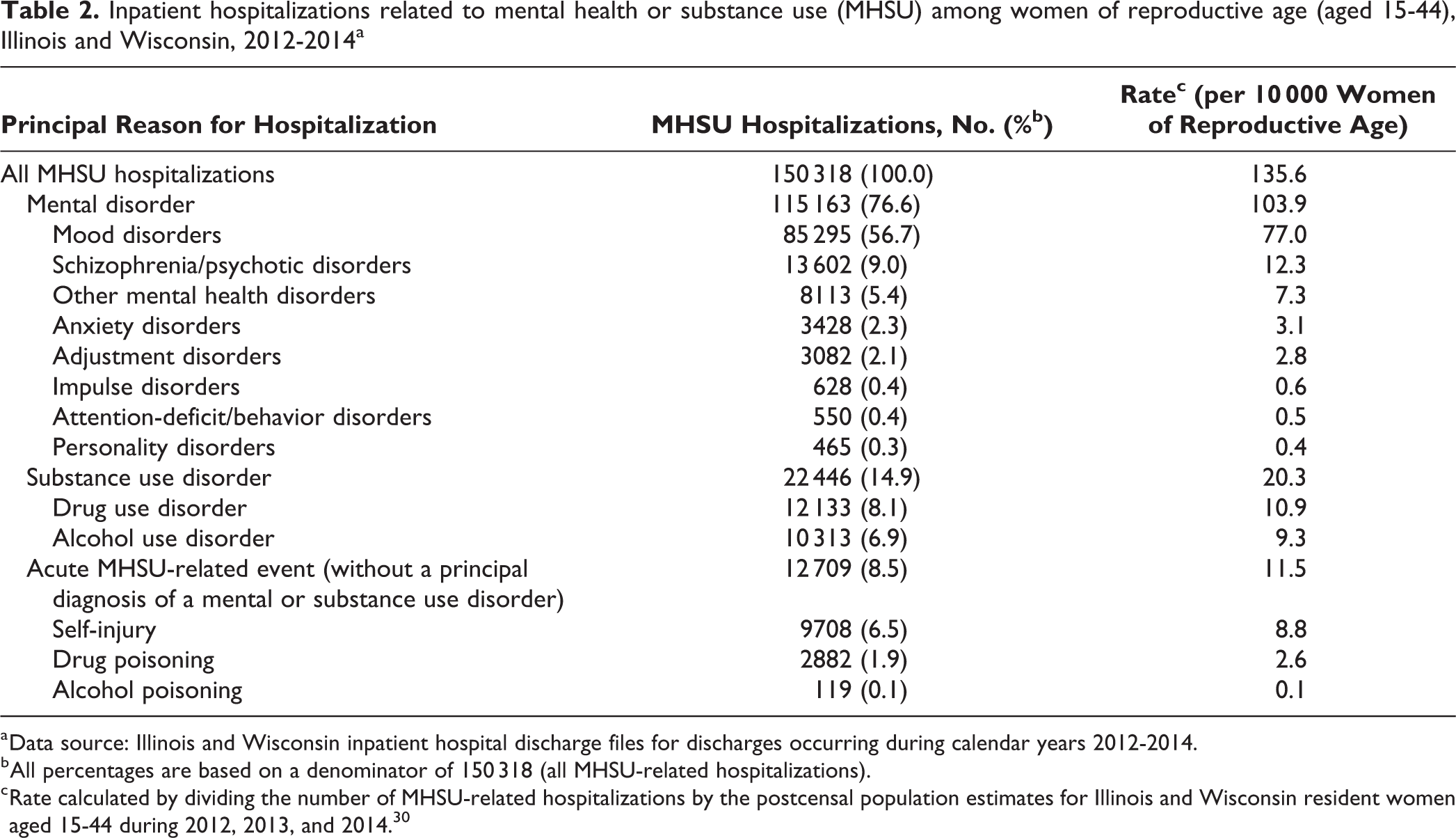
a Data source: Illinois and Wisconsin inpatient hospital discharge files for discharges occurring during calendar years 2012-2014.
b All percentages are based on a denominator of 150 318 (all MHSU-related hospitalizations).
c Rate calculated by dividing the number of MHSU-related hospitalizations by the postcensal population estimates for Illinois and Wisconsin resident women aged 15-44 during 2012, 2013, and 2014. 30
Of all MHSU-related hospitalizations, 42.4% had co-occurring mental health and substance use codes (Table 3). Co-occurrence ranged from 26.2% among hospitalizations for schizophrenia or psychotic disorders to 68.8% for hospitalizations related to an alcohol use disorder. Overall, hospitalizations principally related to substance use disorders had a higher co-occurrence percentage (65.9%) than those principally related to mental disorders (35.9%). Co-occurrence among hospitalizations for acute MHSU-related events was 52.9% for alcohol poisoning hospitalizations, 56.5% for self-injury hospitalizations, and 68.5% for drug poisoning hospitalizations.
Percentage of inpatient hospitalizations related to mental health or substance use (MHSU) among women of reproductive age (aged 15-44) with co-occurringa mental health and substance use disorders and events, by principal reason for hospitalization, Illinois and Wisconsin, 2012-2014b
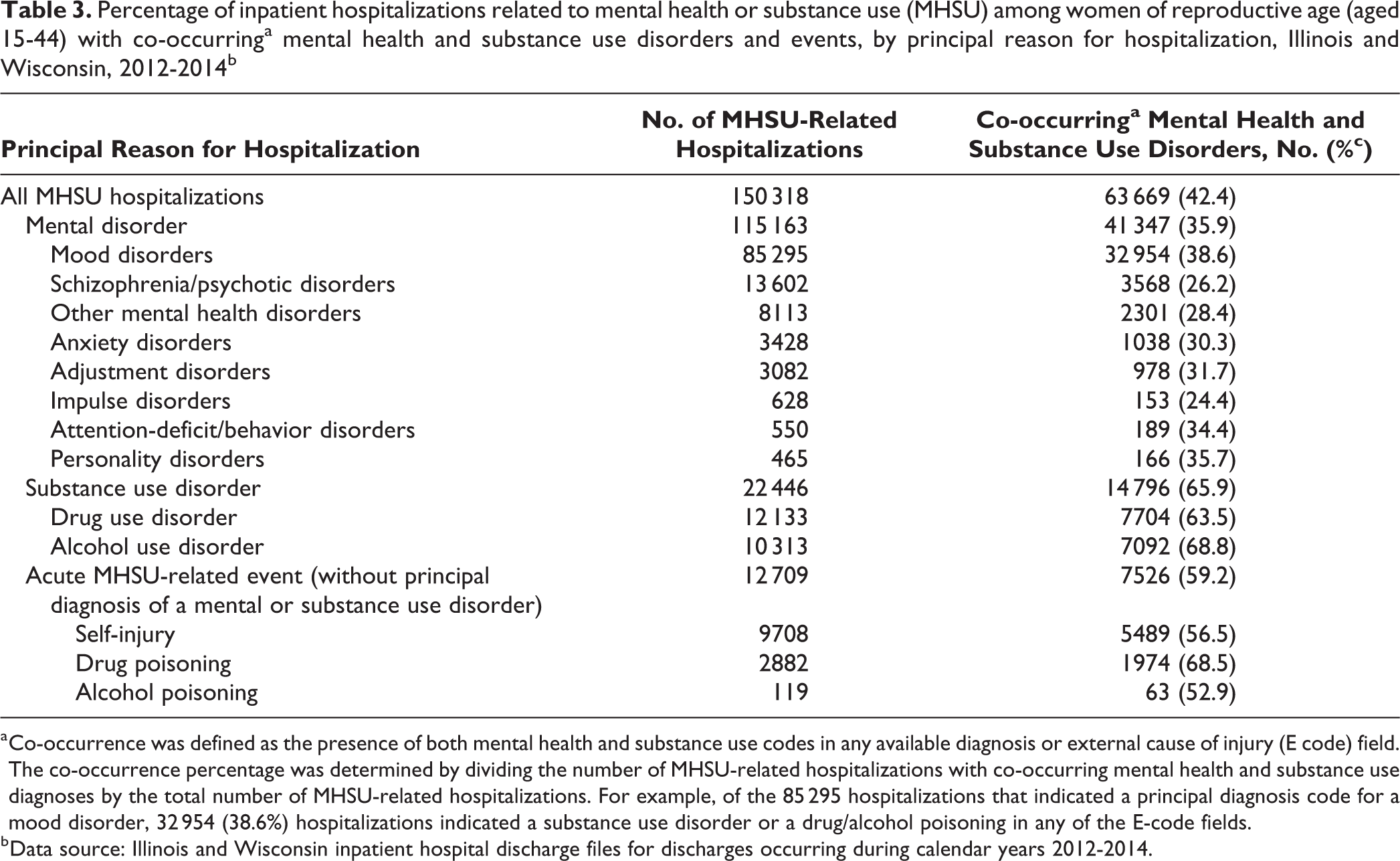
a Co-occurrence was defined as the presence of both mental health and substance use codes in any available diagnosis or external cause of injury (E code) field. The co-occurrence percentage was determined by dividing the number of MHSU-related hospitalizations with co-occurring mental health and substance use diagnoses by the total number of MHSU-related hospitalizations. For example, of the 85 295 hospitalizations that indicated a principal diagnosis code for a mood disorder, 32 954 (38.6%) hospitalizations indicated a substance use disorder or a drug/alcohol poisoning in any of the E-code fields.
b Data source: Illinois and Wisconsin inpatient hospital discharge files for discharges occurring during calendar years 2012-2014.
Discussion
Our study describes the creation and application of an indicator to estimate all MHSU-related hospitalizations among women of reproductive age. Hospitalizations represent the severe end of the MHSU-related spectrum, 35 and they can be monitored as sentinel events to demonstrate the need for investment in systems and infrastructure to support primary, secondary, and tertiary prevention. The proposed indicator is based on a combination of indicators described in established methodologies and previous studies, 14,31 –34 and it demonstrates that mental health and substance use are common causes of hospitalizations among women of reproductive age. For the 2 states in our study, MHSU-related hospitalizations among women of reproductive age occurred at a rate of approximately 1 hospitalization per 74 women, representing 12.8% of hospitalizations for this population. This proportion is higher than the proportion shown by a study of the general US adult population, in which only 6.7% of all hospitalizations were related to mental disorders or substance use disorders. 33 The inclusion of acute MHSU-related events in our indicator accounts for some of the difference between the 2 proportions. Among all US adults, patients aged 18-44 compose 51% of hospitalizations for principal mental disorders and substance use disorders, and women compose 58% of all hospitalizations related to principal mental disorders. 33 It is therefore plausible that women of reproductive age may have higher proportions of MHSU-related hospitalizations than the general adult population.
Our study defined a method for identifying co-occurrence of mental health and substance use conditions, and we found co-occurrence in almost half (42.4%) of MHSU-related hospitalizations. Although we used slightly different methods, our findings were similar to those of a previous study that showed a co-occurrence rate of 45.7% among MHSU-related hospitalizations. 33 We found that the percentage of co-occurrence varied according to the principal reason for hospitalization; co-occurrence was 65.9% for substance use disorder discharges, 59.2% for acute MHSU-related events, and 35.9% for mental disorder discharges. This variability by principal diagnosis was consistent with the variability found in previous studies. 36,37
The proposed MHSU-related hospitalization indicator is unique and offers several advantages over established surveillance indicators. The indicator identifies hospitalizations related to a range of psychological and behavioral health issues, and it includes both mental health–related and substance use–related diagnoses, which allows the monitoring of a combined burden. Many existing MHSU surveillance measures are specific to either a mental disorder or a substance use disorder, and they do not consider these disorders together. 27,34 In addition, the proposed indicator provides a method for establishing the burden of co-occurring mental health and substance use conditions by using administrative data, a data set rarely used by standard surveillance indicators. 27 A unique contribution of the proposed indicator is the inclusion of hospitalizations related to self-injury and drug or alcohol poisoning, rather than only the inclusion of diagnoses of mental disorders or substance use disorders recognized by the DSM-5. 28 We confirmed the appropriateness of including acute MHSU-related events by showing that most (93.5%) acute MHSU-related events had at least 1 mental disorder or substance use disorder diagnosis in a nonprincipal field. If our MHSU-related hospitalization indicator included only principal diagnoses of mental disorders or substance use disorders, we would have missed 8.5% of MHSU-related hospitalizations. Similarly, our study included discharge records from psychiatric hospitals, an important source of care for severe mental disorders and substance use disorders. Administrative databases that do not include behavioral health facilities may substantially underestimate the MHSU-related hospitalization rate.
Our study had several limitations. First, only 2 states were included in the development and testing of this indicator, so application of the indicator may not be generalizable to other US states. However, our study included data on all inpatient hospitalizations for women of reproductive age in the 2 study states and more than 1 million inpatient hospital records. Second, the hospital discharge data in Illinois and Wisconsin differed in the number of diagnosis and E-code fields available for analysis. Although the calculation of the overall MHSU-related hospitalization indicator would not be affected by the number of diagnosis and E-code fields (because the indicator involves only the first-listed ICD-9-CM diagnosis and E codes), the calculation of co-occurrence, which uses all diagnosis and E-code fields, could be affected by differences in state data files. Despite Illinois having more diagnosis codes and E codes available than Wisconsin, our findings of co-occurrence for the 2 states were similar: 42.2% in Illinois and 42.6% in Wisconsin. Third, because we did not have discharge data from federal hospitals, we may have underestimated the true burden of MHSU-related hospitalizations. Active military personnel and veterans, who may seek care at federal Veterans Affairs hospitals, have poorer overall mental health status than the civilian population and have a disproportionate burden of MHSU-related hospitalizations. 38,39 However, the extent of underestimation caused by exclusion of federal hospitals would be small in Illinois and Wisconsin, where fewer than 1% of women aged 18-34 and fewer than 2% of women aged 35-54 are veterans. 40 Finally, our methods for identifying hospitalizations for acute MHSU-related events were applied only to hospitalizations that did not have a mental disorder or substance use disorder as the principal diagnosis. The rate of hospitalizations for these acute events, therefore, does not represent prevalence estimates of all self-injury or poisoning hospitalizations but only additional hospitalizations not identified by a principal diagnosis code for a mental disorder or substance use disorder.
Hospital discharge data have several known limitations when used for public health surveillance. 8, 14, 41 First, discharge data are created for administrative purposes and may be influenced by coding conventions. Decisions about the ordering of diagnosis codes may be influenced more by reimbursement rates than by the relative importance of conditions. For example, in our study, the higher rates of co-occurrence for hospitalizations principally related to a substance use disorder (65.9%) compared with those related to a mental disorder (35.9%) may reflect a preference to bill for a substance use disorder when both types of disorders contribute to the hospitalization. Varying MHSU-related hospitalization rates across US states may reflect true differences in incidence but could also reflect differences in billing code practices or regional preferences for treating patients on an outpatient basis instead of admitting them to a hospital. Furthermore, we do not know the sensitivity and specificity of the MHSU codes in our discharge data because we did not review records to validate the diagnosis and E codes. A validation study of administrative hospital data showed that the sensitivity of ICD-9-CM codes for alcohol abuse, drug abuse, psychoses, and depression ranged from 53.6% to 57.6%, indicating substantial underreporting of these conditions in administrative data. However, positive predictive values for these conditions ranged from 73.7% to 93.9%, showing that when the codes were recorded, they usually indicated a true case. 42 However, the validation study did not validate whether the principal diagnosis code was truly the main reason for hospitalization. Hospital services related to substance use disorder may be further underreported because of restrictions on information disclosure by certain types of treatment centers. 43 Another limitation of our study was that we did not de-duplicate the hospitalization data at the patient level; therefore, multiple admissions may have occurred for the same women during the study period. As a result, the indicator is interpreted as the rate of hospitalizations rather than the proportion of women who were hospitalized.
Despite these limitations, hospital discharge data are becoming more commonly used than they were previously in epidemiology as a source for population-based surveillance. Some of the strengths of discharge data include a large sample size, availability in most states, the ability to ascertain population-based estimates, and the ability to perform cross-state comparisons and trend analyses. 41 The inclusion of neonatal abstinence syndrome and severe maternal morbidity as Title V national outcome measures reflects the shift toward the use of hospital discharge data for public health monitoring. 25,44,45 Our MHSU-related hospitalization indicator is a new measure that leverages discharge data for surveillance.
Future studies could apply the proposed MHSU-related hospitalization indicator in other populations and contexts. Although we conducted our study among women of reproductive age, the MHSU disorders in the proposed indicator are also relevant to other populations, such as adolescents, men, or the general adult population. Application to other state discharge data files or to the national inpatient file may enrich our findings. Although we developed the MHSU-related hospitalization indicator by using inpatient data, the general ICD-based algorithm could be applied to other claims-based data sources, such as emergency department visit data or Medicaid claims data. For states where longitudinally linked discharge data are available, the indicator could be used to identify readmissions after MHSU-related hospitalizations or to examine MHSU-related hospitalizations during women’s prenatal or postpartum periods. Future studies could extend the proposed MHSU categories to all diagnosis code fields, capturing a larger number of hospitalizations, albeit not necessarily reflecting MHSU as the main reason for the hospitalization. Future studies should continue to test our proposed indicator to evaluate its usefulness and validity as a surveillance measure.
Future work will translate this indicator to International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) codes. 46 CCS categories have already been cross-walked to ICD-10-CM codes by the Agency for Healthcare Research and Quality, 47 but the drug and alcohol poisoning categories will require translation. ICD-10-CM involves a substantial change in the structure and organization of diagnosis codes, particularly to the injury codes that encompass poisonings. Comparative studies of ICD-9-CM and ICD-10-CM codes will need to consider how coding changes affect the identification of MHSU-related hospitalizations.
Practice Implications
Our proposed MHSU-related hospitalization indicator allows for analysis of trends, comparisons between jurisdictions, and identification of high-risk groups for targeted interventions, supporting public health surveillance of mental health and substance use. Identifying MHSU-related hospitalizations can demonstrate the extent of behavioral health problems and support increased investment in behavioral health services and systems across the prevention spectrum. Given that billions of dollars are spent on hospitalizations for mental disorders in the United States each year, 7 opportunities exist to reduce costs. Early identification through screening and subsequent referral to treatment could prevent progression of mental disorders and substance use disorders and avoid the crisis events that lead to hospitalization. 35
Because nearly half of all MHSU-related hospitalizations had co-occurring mental health and substance use diagnosis or E codes, recognizing and understanding this interaction have important implications for treatment. Clinicians should be trained to recognize the symptoms of mental disorders among patients with substance use disorder and should consider psychological treatment while treating the concurrent effects of drug use. 10, 14, 48 Providers should also recognize that women with mental disorders, particularly mood disorders, may be at risk for development of substance use disorders and overdose events, and they should seek to prevent such comorbidities. 37
The proposed MHSU-related surveillance indicator can provide public health programs with a method to quantify the combined burden of mental health and substance use conditions in the population, including co-occurrence. These findings demonstrate the importance of prevention and may be used to support public health programs and policy development.
Footnotes
Acknowledgments
The authors thank the Illinois Department of Public Health, Division of Patient Safety and Quality, and the Wisconsin Department of Health Services, Division of Public Health, Office of Health Informatics, for providing discharge data used in this analysis. We also acknowledge the Wisconsin Hospital Association Information Center and the Illinois Health and Hospital Association for collecting state discharge data. The authors acknowledge the Maternal and Child Health Epidemiology Program, Field Support Branch, Division of Reproductive Health, National Center for Chronic Disease Prevention and Public Health Promotion, Centers for Disease Control and Prevention (CDC), for scientific guidance on this analysis and article. The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of CDC.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.