
Abstract
Keywords
Major advances have been made in reducing HIV-related morbidity and mortality since the first infections were reported in the United States more than 36 years ago. 1,2 However, racial/ethnic minority populations are disproportionately affected. 3,4 The Care and Prevention in the United States (CAPUS) Demonstration Project (hereinafter, CAPUS; 2012-2016) aimed to reduce HIV-related morbidity, mortality, and health disparities among these priority populations in 8 states: Georgia, Illinois, Louisiana, Mississippi, Missouri, North Carolina, Tennessee, and Virginia. 5 State health departments collectively received $42.8 million through the US Department of Health and Human Services Secretary’s Minority AIDS Initiative Fund 6 to expand and improve HIV testing capacity and optimize linkage to, retention in, and reengagement with care and prevention services for people with HIV (PWH). 5 Eligibility for funding was based on the high HIV disease burden among racial/ethnic minority populations, the disproportionate rate of AIDS diagnoses and associated mortality, and the pervasive effect of social and structural determinants of health within a jurisdiction.
To achieve the goals of CAPUS, which are consistent with the National HIV/AIDS Strategy goal to reduce HIV-related disparities and health inequities, 7 state health departments planned, implemented, and evaluated activities according to the following core CAPUS grantee program requirements: (1) increase HIV testing, linkage to, retention in, and reengagement with care and prevention; (2) use HIV surveillance data and other data systems to improve care and prevention; and (3) provide navigation services to people in racial/ethnic minority groups. A unique aspect of CAPUS was that grantees were required to address social and structural factors that directly affect access to and use of HIV care and prevention services. 8 -11 Because community-based organizations (CBOs; eg, AIDS service organizations, nonprofit community health centers) are uniquely positioned as stakeholders and resources 12 in HIV prevention and care, grantees were required to partner with CBOs and use a minimum of 25% of their total award to develop CBO capacity to implement CAPUS activities. Grantees collaborated with 117 organizations, including CBOs, local health departments, and other nonprofit organizations and businesses. While serving on advisory boards to guide program planning and implementation, conducting training to build capacity of service providers to provide HIV prevention and care services, and implementing project activities, these collaborators enhanced the overall project experience by offering subject matter expertise, access to priority populations, and resources (eg, staffing, HIV test kits, patient education materials) to support grantee programs.
Federal CAPUS staff members outlined expectations for the core grantee program requirements and cross-site monitoring and evaluation (Table) that were informed by national HIV prevention goals. 7 The core program requirements were used to guide development and implementation of grantees’ work plans and monitoring and evaluation. Grantees identified activities that, when combined, would have the greatest public health impact within their respective jurisdictions. Given the complex, interrelated nature of these activities, a multiagency federal partnership provided guidance and technical expertise and monitored grantees’ progress throughout the project. 14
Care and Prevention in the United States (CAPUS) Demonstration Projecta grantee program requirements and expectations, 8 states,b 2012-2016
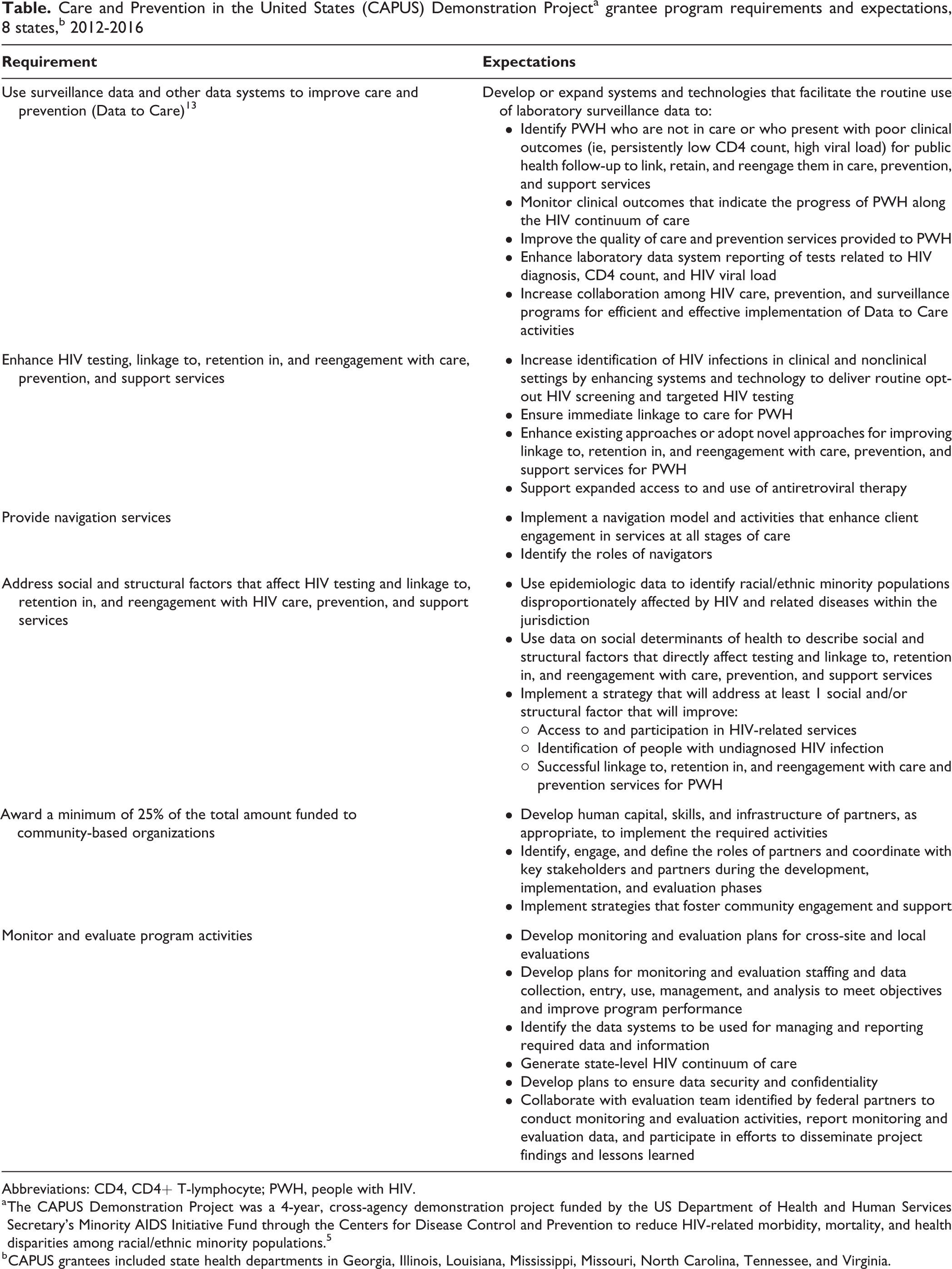
Abbreviations: CD4, CD4+ T-lymphocyte; PWH, people with HIV.
a The CAPUS Demonstration Project was a 4-year, cross-agency demonstration project funded by the US Department of Health and Human Services Secretary’s Minority AIDS Initiative Fund through the Centers for Disease Control and Prevention to reduce HIV-related morbidity, mortality, and health disparities among racial/ethnic minority populations. 5
b CAPUS grantees included state health departments in Georgia, Illinois, Louisiana, Mississippi, Missouri, North Carolina, Tennessee, and Virginia.
During the 4-year project period, grantees strengthened their statewide HIV prevention efforts by using innovative strategies, making systems-level and infrastructure improvements, leveraging essential resources, and establishing effective partnerships as they executed their work plans. As described in articles in this supplemental issue of Public Health Reports, these advancements led to improved organizational capacity and expanded service provision, which resulted in priority populations being successfully linked to, retained in, and reengaged in HIV medical care, prevention, and support services. Selected cross-site process and short-term outcome evaluation findings are reported by Mulatu and colleagues in this supplement. 15
This article is based on data collected during 2012-2016 that were obtained from grantee progress reports and presentations, federal partner presentations, and notes from site visits and grantee conference calls. These sources described program successes, factors that contributed to successes, challenges, and strategies implemented to address challenges. We report common lessons learned across multiple grantees and lessons that were most salient to grantee-specific project performance on the core grantee program requirements. The process we used to identify and document lessons learned was informed by the Centers for Disease Control and Prevention’s (CDC’s) Unified Process Practices Guide. 16 Implications for public health entities that implement HIV care and prevention work for racial/ethnic minority populations are also presented. Although this article presents lessons learned from the grantees’ experiences with planning, implementing, and evaluating CAPUS activities, this supplemental issue of Public Health Reports also includes lessons learned from federal staff members who provided oversight and technical expertise for CAPUS 14 and staff members of CDC’s Division of HIV/AIDS Prevention, who led and co-led multiple demonstration projects aimed at reducing new HIV infections and expanding prevention and care services for communities most affected by HIV. 17
We describe lessons learned based on grantees’ experiences with planning, implementing, and evaluating program activities. The lessons learned are organized by the core CAPUS grantee program requirements (Table).
Enhance HIV Testing
Strategies to Destigmatize and Normalize HIV Testing Are Effective for Reaching Racial/Ethnic, Sexual, and Gender Minority Populations
Grantees used various strategies to normalize HIV screening and decrease HIV-related stigma, a barrier they reported for reaching people with undiagnosed HIV infection. Having multiple options for reaching priority populations improved HIV testing access for people who, for example, were not comfortable testing at a local health department or CBO because of concerns about confidentiality and stigma. Grantees conducted testing in nontraditional settings, such as pharmacies, 18 and in several locations where no screening or minimal screening occurred in their jurisdictions (eg, jails and community-based settings that served priority populations). The project also supported routine, opt-out HIV testing in general health care settings, including hospital emergency departments. Integration of HIV screening into general health care settings (as part of routine prevention services) helped to normalize HIV screening and bridge the gap between HIV services and general health care. Successful integration was often facilitated by embedding a champion within the facility to ensure smooth integration of HIV testing into a clinic’s workflow. 19
Another activity that builds on relationships and trust is the social network strategy, which uses PWH and people at high risk for HIV infection from priority populations (eg, racial/ethnic minority groups, men who have sex with men) to recruit people from their social, sexual, or drug-using networks for HIV testing. The social network strategy was successfully used to engage a hard-to-reach population (ie, black men who have sex with men) and identify men with undiagnosed HIV infection and men who were previously diagnosed but not in care to facilitate linking and reengaging them with HIV medical care. 20 Grantees were also able to reach large numbers of priority populations through social marketing and social media campaigns that were intended to reduce stigma and promote HIV testing and immediate linkage to care. 15
Data-Informed Planning Improves Targeting and Tailoring of HIV Testing Activities
To assess gaps in HIV testing services and ensure that HIV screening efforts reached priority populations and underserved areas, grantees analyzed surveillance data alongside data on geospatial characteristics (eg, ZIP codes and census tracks), demographic characteristics, and pertinent social determinants of health (eg, poverty rates). Grantees shared with partner organizations data reports showing HIV tests conducted by client demographic characteristics (eg, gender, race/ethnicity, age) and transmission categories (eg, male-to-male sexual contact, injection drug use, heterosexual contact) to assess how accurately HIV testing activities matched targeting goals. Grantees supplemented surveillance and other social determinants of health data with focused discussions with community members and discovered that existing HIV testing campaigns were not resonating well with local communities (eg, images did not reflect members of their communities). To address these concerns, grantees consulted with key informants and community groups to develop or tailor campaigns to ensure that the images and language used in the social marketing and social media materials were locally relevant and representative of the priority populations.
Ongoing Training and Technical Assistance Improves Organizational Capacity for Conducting Testing Activities
Expanding HIV testing required grantees to partner with organizations that had access to priority populations, such as black and Hispanic/Latino men who have sex with men and transgender people. Occasionally, however, these partners had limited capacity to conduct testing, which resulted in delays in testing startup, interruptions in testing services, and fewer tests being conducted. Several grantees also had difficulty evaluating the effects of their social marketing campaigns on testing uptake because of limited experience conducting these evaluations, including identifying an appropriate evaluation design and developing data collection tools. To help improve grantee and partner organizational capacity, federal partners, contracting organizations (eg, AIDS Education and Training Centers), and grantees (through peer-to-peer exchanges) provided trainings and technical assistance and shared knowledge and experiences to improve HIV testing capacity. Common areas for technical assistance included identifying new HIV testing sites, improving outreach to priority populations, evaluating social marketing and social media campaigns, and making testing-related, systems-level enhancements (eg, integrating electronic health records and third-party billing). Common training topics included HIV testing strategies (eg, rapid testing, fourth-generation testing technology), quality assurance and quality control, and HIV prevention counseling. Grantees reported that this training and technical assistance helped them improve their organizational capacity for conducting HIV testing, improve their ability to reach priority populations by selecting appropriate testing venues, build knowledge and skills for conducting HIV tests using newer technologies, and improve capacity to evaluate testing campaigns.
Use Surveillance Data and Other Data Systems to Improve Care and Prevention
Increased Compliance With Laboratory Reporting Laws Provides a More Accurate Understanding of Access to HIV Care and Improves Resource Allocation for Client Outreach
As laboratory reporting systems matured and compliance with associated laws, regulations, and policies increased during the CAPUS period, the quality and timeliness of data used to identify people not in care improved. Complete reporting of all CD4+ T-lymphocyte (CD4) and viral load tests to state HIV surveillance programs facilitated identification of HIV cases and classification of disease stage at diagnosis. These data were also used to track the care status of PWH and evaluate HIV testing and prevention efforts. Compared with grantees who had been reporting CD4 and viral load tests to state HIV surveillance programs for a longer period, health departments in jurisdictions where laboratories were only recently required to report all CD4 and viral load tests to state HIV surveillance programs identified more reporting deficiencies (eg, incomplete data on laboratory results and care status). These deficiencies also resulted in field investigations that found substantial numbers of clients who were already in care, deceased, or living outside of the jurisdiction. Successful Data to Care programs—those in which HIV surveillance and other data are used to identify PWH who are not in care to facilitate linkage to care and other needed services—revised policies and procedures to improve compliance with laboratory reporting requirements to substantially improve data accuracy. 21 One grantee used laboratory data to identify PWH who were in care but not virally suppressed. After follow-up, the grantee reported that the majority of patients achieved viral suppression based on laboratory results from their last medical visit. 22 More complete reporting improved overall assessment of a jurisdiction’s HIV care continuum (eg, the proportion of PWH who were linked to care, retained in care, and virally suppressed), targeting of services, and use of limited resources needed for outreach and follow-up of PWH presumptively not in care.
Cross-Referencing HIV Surveillance Data With Other Data Systems Improves the Accuracy of Not-in-Care Lists and HIV Continuum-of-Care Data
Limitations of HIV surveillance data included reporting delays, incompleteness, and out-of-date contact information. To address these challenges, grantees used other data systems to supplement HIV surveillance data. 21 For example, grantees matched or integrated data from surveillance with data from the Ryan White HIV/AIDS Program, partner services, the AIDS Drug Assistance Program, sexually transmitted disease surveillance, state Medicaid data, or a commercially available people-search tool. Although verifying, cleaning, and integrating data was resource intensive, these processes allowed grantees to locate PWH efficiently, confirm their care status, and follow up with PWH who were not in care. Implementing procedures to update surveillance data with data obtained from other systems (eg, vital status, address) and through follow-up investigations by field staff members was instrumental for enhancing the quality of surveillance data and accuracy of HIV care continua.
Collaboration Among Surveillance, Prevention, and Care Units Supports Efficient and Effective Implementation of Data to Care Activities
Engaging surveillance, prevention, and care units during the project-planning phase was key to ensuring early identification of technical assistance and resources needed to implement Data to Care activities. Grantees that obtained information technology and data analytic expertise early during the project period reported improved efficiency in developing data systems, conducting data matches across systems, and cleaning and managing data. They noted that data-sharing agreements, memoranda of understanding, and procedural protocols helped streamline processes and improve communication among HIV surveillance, prevention, and care units. Grantees also observed that these tools clarified for them the roles and responsibilities of each unit, better described data-sharing and use processes, and helped them to keep personally identifiable information secure.
Provide Navigation, Linkage, Retention, and Reengagement Services
Establishing Multisector Partnerships Helps Grantees and Partners to Address Varied and Complex Client Needs Effectively
To adequately provide navigation, linkage, retention, and reengagement (NLRR) services, grantees needed to establish and strengthen their partnerships across various sectors to help PWH overcome or mitigate complex structural and personal barriers to accessing and using care and prevention services. It was important for staff members who provided NLRR services to know what resources were available in their jurisdictions, such as housing assistance programs, mental health service, substance use services, transportation services, financial assistance programs, interpretive services, and peer support services, to facilitate timely referral and linkages of clients to needed services. To be effective, staff members who provided NLRR services also had to develop strong relationships with people in the community, in health care settings, and in other settings (eg, organizations serving lesbian, gay, bisexual, transgender, queer, and questioning [LGBTQ] populations; correctional institutions). These relationships provided an in-depth understanding of the priority populations’ unmet needs and available resources needed to link them to care, prevention, and support services.
Integrating and Coordinating NLRR Services With Existing Systems Helps Grantees Avoid Duplication of Services and Ensure Continuity of Care for Clients
When NLRR programs were integrated into existing systems (eg, Ryan White HIV/AIDS Program) or used staff members who were trained to conduct NLRR activities, grantees reported improved linkage and reengagement to care. Grantees also instituted policies and procedures to standardize NLRR practices. Given the nature of the work, NLRR services often overlapped with the responsibilities of case managers, disease intervention specialists, and social workers. To avoid duplication of services and improve coordination, grantees clarified the roles of NLRR staff members (eg, developed job descriptions to distinguish the role of navigators from disease intervention specialists or case managers). Some grantees also adopted a team-based approach to facilitate case coordination and continuity of care among providers across systems to ensure clients’ ongoing care. As an example, case conferencing involving a care provider, case manager, and navigator provided coordinated and integrated services across multiple providers.
Providing Training and Peer Support to NLRR Staff Members Helps Them to Coordinate HIV Medical Care and Services, Address Client Needs, and Manage Administrative Tasks
Grantees provided training to NLRR staff members to ensure they could meet the demands of their new roles and support the needs of PWH. However, because there was no consensus-based model or standardized training for HIV NLRR services, service training content and methods varied among jurisdictions. However, trainings typically covered HIV care and case management, risk-reduction counseling, cultural sensitivity/humility, referral processes, partner services, and case documentation. Grantees, in collaboration with their program implementation partners, developed standardized training protocols to increase staff members’ knowledge, skills, and self-efficacy to perform their duties. Given the intensity of these positions (ie, time and level of effort needed to address complex barriers and successfully link and reengage PWH with care), grantees found it necessary to provide ongoing support (eg, self-care trainings, peer coaching) to prevent staff member fatigue and burnout. One innovative approach to enhance the overall skillset of peer navigators (ie, PWH and/or people who had similar demographic characteristics as people in the priority population) involved a grantee partnering with 2 community colleges to implement a formal community health worker training program for peer navigators. Through this program, peer navigators earned college credits toward community health worker certification and found employment as community health workers.
Address Social and Structural Factors Affecting Testing, NLRR Services, and Prevention Services
State and Local Data on Social Determinants of Health Are Useful for Identifying the Most Salient and Feasible Social and Structural Barriers to Address
Grantees used data on HIV prevalence alongside state and local data on social determinants of health (eg, poverty rates, education levels) to produce geocoded maps to target and tailor services. Analyses of US Census data, relevant reports (eg, community needs assessments, health equity reports, market research), and information on available resources and gaps in services helped grantees and implementation partners better understand the HIV risk context of priority populations and improve coordination of local resources. Based on these analyses, the most commonly reported barriers among racial/ethnic minority populations were HIV stigma and homophobia, followed by lack of access to quality health care, limited transportation options, provider bias, institutional racism (ie, the rules, processes, and opportunity structures that enable disparate impacts in organizational or institutional contexts), housing instability, confidentiality concerns, low HIV literacy, unemployment, language barriers, mistrust in the health care system, and fragmented health systems.
Addressing Social and Structural Barriers Affecting Access to and Use of HIV Prevention and Care Services Requires a Locally Tailored Approach
The selection of activities and programs implemented to address social and structural factors was largely based on the needs of the priority population and jurisdictions, available resources, and saliency of barriers to accessing and using HIV care and prevention services. As such, grantees’ activities were varied, addressed barriers at a systems level or community level, and generally fell into 3 categories: (1) increasing access to health care and service delivery, (2) implementing capacity-building activities, and (3) implementing social marketing and social media campaigns.
Activities that improved access to health care and service delivery included offering HIV screening at retail pharmacies, 18 co-locating HIV care and support services, establishing men’s clinics in priority neighborhoods, providing temporary housing and employment training for PWH, 23 and expanding care to venues where HIV-related services were not previously provided (eg, emergency departments, jails). Grantees used several other locally tailored approaches to address social and structural barriers to the use of HIV prevention and care services. For example, capacity-building activities for state health department, clinic, and CBO staff members addressed institutional racism and its effects on health care delivery 24 and bias among providers working with racial/ethnic minority populations, LGBTQ communities, and PWH. 25,26 Social marketing and social media campaigns were tailored for priority populations and were implemented to address HIV stigma, homophobia, and transphobia and to promote HIV testing and reengagement in HIV medical care. 27 Grantees and their partners also reported that increasing their workforce diversity helped to increase clients’ comfort with accessing services. One grantee that implemented an incentive-based strategy shown to be effective for improving engagement and retention in HIV medical care reported that patients used their financial incentives to pay for transportation, housing, and medication costs not covered by insurance (ie, poverty-related barriers to participation in HIV care). 28
Addressing the Social and Structural Barriers to HIV Care and Prevention Is Feasible Through Collaboration With Multisector and Nontraditional Partners
To develop programs and activities that aimed to reduce HIV-related disparities, grantees collaborated with various public and private partners (eg, departments of corrections, transitional housing programs, faith-based organizations, schools, and local businesses) to identify and leverage local resources beyond the public health sector. These partners provided lessons learned from their work and shared ideas about what factors led to disparities and how to develop locally tailored and acceptable HIV intervention programs for priority populations.
Conduct Monitoring and Evaluation Activities
Developing a Comprehensive Monitoring and Evaluation Plan Before Program Implementation Establishes Clear, Reasonable Program Expectations and Ensures the Feasibility of Monitoring and Evaluation Activities
According to grantees, engaging evaluators and data managers at project startup improved their overall program efficiency. It also helped to facilitate agreement on monitoring and evaluation strategies, including developing logic models, identifying appropriate process and outcome measures and data sources, developing data collection tools, and addressing concerns about reporting burden to funders. Delayed monitoring and evaluation planning limited grantees from fully capturing data to establish baseline measures in the early stages of program implementation. Grantees that adequately invested in their monitoring and evaluation capacity early on reported improvements in the overall quality of their plans, the quality of data reported, and the assurance that reasonable targets were set. It was also important for grantees to have the flexibility to modify their monitoring and evaluation plans, because many programs were new to them and evolved over time.
Expanding Monitoring and Evaluation Capacity Through Training, Technical Assistance, and Contracting With External Evaluators Increases Grantees’ Capacity to Implement Their Evaluation Plan
Capacity to implement monitoring and evaluation varied based on staffing, expertise, and skills to capture, process, analyze, and report data. Grantees also reported difficulty in hiring and retaining monitoring and evaluation staff members. Several grantees reported that project staff members, including program implementation partners, had limited experience and capacity to develop and implement monitoring and evaluation activities, including developing evaluation questions, identifying appropriate measures, setting performance targets, and collecting, managing, analyzing, and reporting monitoring and evaluation data. Persistent challenges included tracking data for referrals and linkage to HIV medical care and other support services and inserting timely, accurate data into tracking systems. Grantees addressed these difficulties by providing technical assistance and training to staff members or by contracting monitoring and evaluation activities to external evaluators. According to grantees, both efforts improved program monitoring and data quality.
Incorporating Quality Assurance Procedures and Allowing the Use of Varied Data Collection Methods Improves the Overall Quality of Program Monitoring and Evaluation
A substantial challenge reported by grantees was inconsistently reported and incomplete data, which made it difficult to manage client data and determine whether service objectives were being met. To capture needed data and streamline the process for monitoring progress and tracking client-level data (including referrals, linkage, and other outcomes), grantees established new databases or created new fields within existing databases. When access to databases was restricted for certain staff members (eg, some NLRR staff members), grantees collected data by using standardized hard-copy reporting forms. Grantees reported that these steps resulted in more complete data tracking and improved data quality and accuracy. They also observed that incorporating quantitative and qualitative data collected from multiple sources (eg, implementation site reports, conference calls with implementation partners, quality assurance site visits) greatly improved monitoring and evaluation and the overall quality of program activities. Quality assurance processes identified data collection and reporting challenges, which led to improvements in data collection templates, procedures, and staff training.
The Quality of the Monitoring and Evaluation Activities Affects Current Programs, Dissemination, Translation, and Sustainability Plans
In addition to monitoring and tracking key indicators for performance and accountability, the quality of the monitoring and evaluation plan affected the interpretation and reporting of data for dissemination and translation products (eg, reports, presentations, publications, implementation tools). Having quality monitoring and evaluation practices in place helped to strengthen the evidence base to improve current programs, advocate for future funds, and inform decisions about which strategies to prioritize and sustain at the end of the project.
Other Lessons Learned
Effective Leadership at All Levels Improves Strategic Project Planning and Decision Making for Program Implementation
Early and continuous engagement of leadership within the state health departments was key to gaining buy-in from a diverse group of stakeholders and staff members, securing resources, and facilitating partner engagement. Commitment from leadership was particularly important when engaging large and complex systems (eg, corrections departments, health care organizations). Regularly scheduled conference calls and meetings with collaborators helped collaborators work with a common purpose. Grantees that were able to appoint and sustain a dedicated lead for the project (eg, project manager) began planning and program implementation quickly and were able to establish a project team, set clear project goals, and define roles and responsibilities for timely development of jurisdictional work plans.
Assessing Organizational Capacity Early Allows Grantees to More Effectively Plan Activities and Budgets
Organizational readiness to execute work plans varied across health departments. Although a standardized process to assess organizational readiness across all grantees was lacking, each grantee assessed its organizational capacity by, for example, conducting needs assessments and convening meetings with key internal and external stakeholders on management and operational capacity to implement planned activities. Grantees that undertook a systematic process and conducted assessments early were able to launch activities quickly and ensure that the programs were feasible and sufficiently resourced.
Implementing Strategies to Mitigate Staff Member Turnover Decreases Interruptions in Program Delivery
Staff member turnover was a major challenge for grantees throughout the project. Health departments addressed this challenge by developing detailed program manuals and communication plans, offering trainings throughout the year for new staff members, training multiple people on tasks so that knowledge was not lost because of staff member turnover, and, where possible, reassigning staff members who had previous project knowledge or experience to vacated positions.
Project Plans Must Be Adaptable to Accommodate Systems-Level Changes and Other Unplanned Events That Might Affect Project Timelines and Budgets
Many CAPUS activities were new to grantees and required complex systems-level changes to implement. Setting up these programs involved instituting policy and procedural changes for new project management structures, establishing new partnerships, issuing contracts, and hiring and training staff members. Because these efforts were time- and resource-intensive, implementation of some activities was delayed. Moreover, unexpected challenges beyond grantees’ control included delays with contract execution, inflexible state budget and policy issues (eg, budget impasses, rapid privatization of hospitals, strict cost reimbursement models for CBOs), and even major weather events. Grantees found it helpful to consider various contingency plans early on in case they had to modify program design and implementation plans to lessen the impact on their project timelines and budgets.
Implications for Future Programs, Research, and Evaluation
Local, state, and national organizations worldwide recognize the need to address health inequities in a systematic way, moving beyond solely addressing individual-level factors to incorporating a social determinants of health approach. 29 -32 CAPUS offered the opportunity to demonstrate how addressing social and structural barriers might improve outcomes for racial/ethnic minority populations along the HIV care continuum. CAPUS grantees implemented several promising and feasible approaches for improving testing, NLRR services, and prevention services, which have clear implications for future policy and programming and highlight the need for additional research and evaluation to improve HIV service delivery for racial/ethnic minority populations.
Because no single approach can be used to reduce disparities, grantees implemented tailored strategies based on the needs of the jurisdiction, priority populations, and available resources. CAPUS grantees expanded access to HIV testing in underserved areas and reached an appreciable number of PWH who were unaware of their status or who were previously diagnosed but not in care. However, several barriers to early diagnosis of HIV and entry into care remain for the most vulnerable populations. Stigma, provider bias, and concerns about confidentiality, particularly in rural settings, impede testing efforts. Future projects should address these barriers. The challenge and complexity of linking and retaining PWH in care has also been well documented. 33,34 CAPUS grantees implemented several strategies that improved linkage and reengagement and addressed the complex factors that impede clients’ access to and use of HIV prevention and care services. However, more rigorous evaluation is needed to refine and improve these strategies. Grantees found that successful implementation of Data to Care activities required several infrastructure and systems-level changes to improve laboratory reporting, integrate data from multiple systems, and facilitate data sharing and collaboration across prevention, care, and surveillance. 21 The efficiency and effectiveness of future Data to Care efforts will likely improve with prioritization of this activity by state health departments and allocation of resources aimed at improving infrastructure and organizational capacity to implement Data to Care activities.
CAPUS successes were largely attributed to effective leadership and the engagement of existing and new partners early, regularly, and throughout the project. The importance of strong leadership in designing, supporting, implementing, and sustaining partnerships mirrors several key lessons from the federal CAPUS collaboration. 14 State health departments leveraged the knowledge and resources of strategic partners to implement comprehensive strategies. These collaborations were viewed as an asset that supported creative problem solving and enhanced the overall project experience by increasing project capacity. In particular, collaborations with new, multisector, and nontraditional partners improved access to priority populations, ensured the cultural appropriateness of project activities, and led to the development of new approaches to address social and structural factors. Future efforts to intervene on social and structural barriers should maximize the use of partnerships to best align resources and coordinate efforts locally to increase program effectiveness and sustainability, improve HIV-related outcomes, and reduce disparities. It is likely that the various collaboration models implemented under CAPUS will serve as catalysts for future jurisdictional collaborations and offer the potential for replication in future health program efforts.
Although CAPUS offers preliminary evidence of how social and structural barriers can be addressed to improve care, prevention, and health outcomes of PWH and people at risk for HIV infection, additional evaluations are needed to determine best practices from these real-world experiences to optimize service delivery. Context shapes how HIV interventions and programs work. 8,32,35,36 Future assessments of the effectiveness of these interventions should incorporate information on local social and structural systems that create the contexts within which programs are implemented. Action research (a reflective process of problem solving led by individuals working in teams or as part of a community of practice to improve the way they address issues and solve problems), nonexperimental observational and participatory methods (research that occurs in natural settings and does not involve manipulation of an independent variable and random assignment of participants to conditions), quasi-experimental designs, and realistic evaluation (a method used to identify the underlying generative mechanisms that explain “how” the outcomes were caused and the influence of context) 37,38 can be used to assess the independent, synergistic, and modifying effects of social and structural barriers and how they can be modified to have a meaningful impact on HIV morbidity and mortality among racial/ethnic minority populations.
Conclusion
Addressing HIV-related health disparities requires an important shift in our thinking about how health is produced and what solutions are needed to promote health. CAPUS grantees implemented innovative approaches that aimed to decrease HIV-related health disparities and improve health outcomes among racial/ethnic minority populations. Only with time will the full impact of CAPUS activities be realized; however, the lessons learned from this demonstration project have the potential to strengthen the capacity of health departments and other agencies that aim to reduce HIV-related health disparities.
Footnotes
Authors’ Note
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention (CDC).
Acknowledgments
The authors acknowledge the Care and Prevention in the United States (CAPUS) grantees and their collaborating partners for their demonstrated commitment to addressing HIV-related health disparities in their communities and the members of the CAPUS federal collaboration (Office of HIV/AIDS and Infectious Disease Policy, Office of Minority Health, Office on Women’s Health, the Health Resources and Services Administration’s HIV/AIDS Bureau, the Substance Abuse and Mental Health Services Administration [SAMHSA], and CDC’s Division of HIV/AIDS Prevention), project officers, site team members, the CAPUS Core Management Team, Division of HIV/AIDS Prevention Senior Leadership Advisory Committee (CDC), the CAPUS Senior-Level Federal Partnership Committee, and the National Alliance of State and Territorial AIDS Directors for their valuable contributions in guiding and supporting this demonstration project.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The CAPUS Demonstration Project was supported by the US Department of Health and Human Services Secretary’s Minority AIDS Initiative Fund and led by CDC (PS 12-1210).