
Abstract

Keywords
Racial/ethnic minority groups, particularly African American and Hispanic people, have a disproportionate burden of HIV infection and poor health outcomes despite substantial federal investment to address HIV-related health disparities. 1,2 In spring 2011, the US Department of Health and Human Services (HHS) Office of HIV/AIDS and Infectious Disease Policy (OHAIDP) initiated the first of several cross-agency brainstorming discussions on a demonstration project to be funded through the Secretary’s Minority AIDS Initiative Fund (SMAIF) that would address racial/ethnic disparities in HIV/AIDS morbidity and mortality. These discussions, which involved federal staff members from several HHS operating and staff divisions, were the foundation for a new initiative—the Care and Prevention in the United States (CAPUS) Demonstration Project (hereinafter, CAPUS).
In 2012, the Centers for Disease Control and Prevention (CDC) awarded $14.2 million to 8 state health departments in states with a high number of HIV cases among African American and Latino people. CAPUS was a 4-year (2012-2016) cross-agency demonstration project with the aim of reducing HIV/AIDS-related morbidity and mortality among racial/ethnic minority groups in the United States. The primary goals of the project were to (1) increase the proportion of racial/ethnic minority groups with HIV who have diagnosed infection by expanding and improving HIV testing capacity and (2) optimize linkage to, retention in, and reengagement with care and prevention services for people with newly diagnosed and previously diagnosed HIV in racial/ethnic minority groups. 3 In addition, 2 features set CAPUS apart from other similar projects: (1) its goals were to be achieved by addressing social and structural factors directly affecting access to and use of HIV care and prevention services, and (2) a cross-branch, cross-agency collaboration was established to improve coordination across CDC branches and agencies and to help grantees plan, implement, and evaluate their program activities. Grantees were also required to fund community-based organizations (CBOs) by using a minimum of 25% of their funding award for capacity building and program implementation. This requirement would avail to the grantees the unique expertise and experience of the identified CBOs, particularly in working with racial/ethnic minority communities.
The literature contains few articles on federal collaborations of the complexity and scope of collaboration that CAPUS involved. Our article fills an important gap in the literature. CAPUS gave HHS agencies an opportunity to work together and offer the 8 grantees their collective expertise and experience to positively affect HIV prevention and care programming. In this commentary, we describe the federal collaboration of CAPUS 4 and summarize (1) participating federal staff members’ experiences and reflections on the structure of the collaboration; (2) expectations for each collaborating partner; (3) outcomes of the collaboration, including successes and challenges; and (4) lessons learned and implications for future cross-agency collaborations and public health. 5
Formation and Structure of the Collaboration
Assembly of CAPUS federal collaboration was intentional, strategic, and anchored by a project-management plan that defined collaborators’ roles and responsibilities and a staffing structure formed by senior-level cross-agency staff members (Table). From the beginning, OHAIDP leveraged the subject-matter and technical expertise of partnering agencies, including CDC’s Division of HIV/AIDS Prevention (DHAP), the Health Resources and Services Administration (HRSA) HIV/AIDS Bureau and Bureau of Primary Health Care, the Substance Abuse and Mental Health Services Administration (SAMHSA), and the Office of the Assistant Secretary for Health (OASH). Each agency has expertise in HIV prevention and/or care and a history of addressing HIV-related health disparities using SMAIF resources. Each agency was also well positioned to provide important insights into the social and structural barriers (eg, poverty, stigma, housing, employment, and transportation) that confound HIV prevention and care efforts. 6
Missions and project roles of HHS agencies, divisions, and branches participating in the Care and Prevention in the United States (CAPUS) Demonstration Project, 2012-2016a
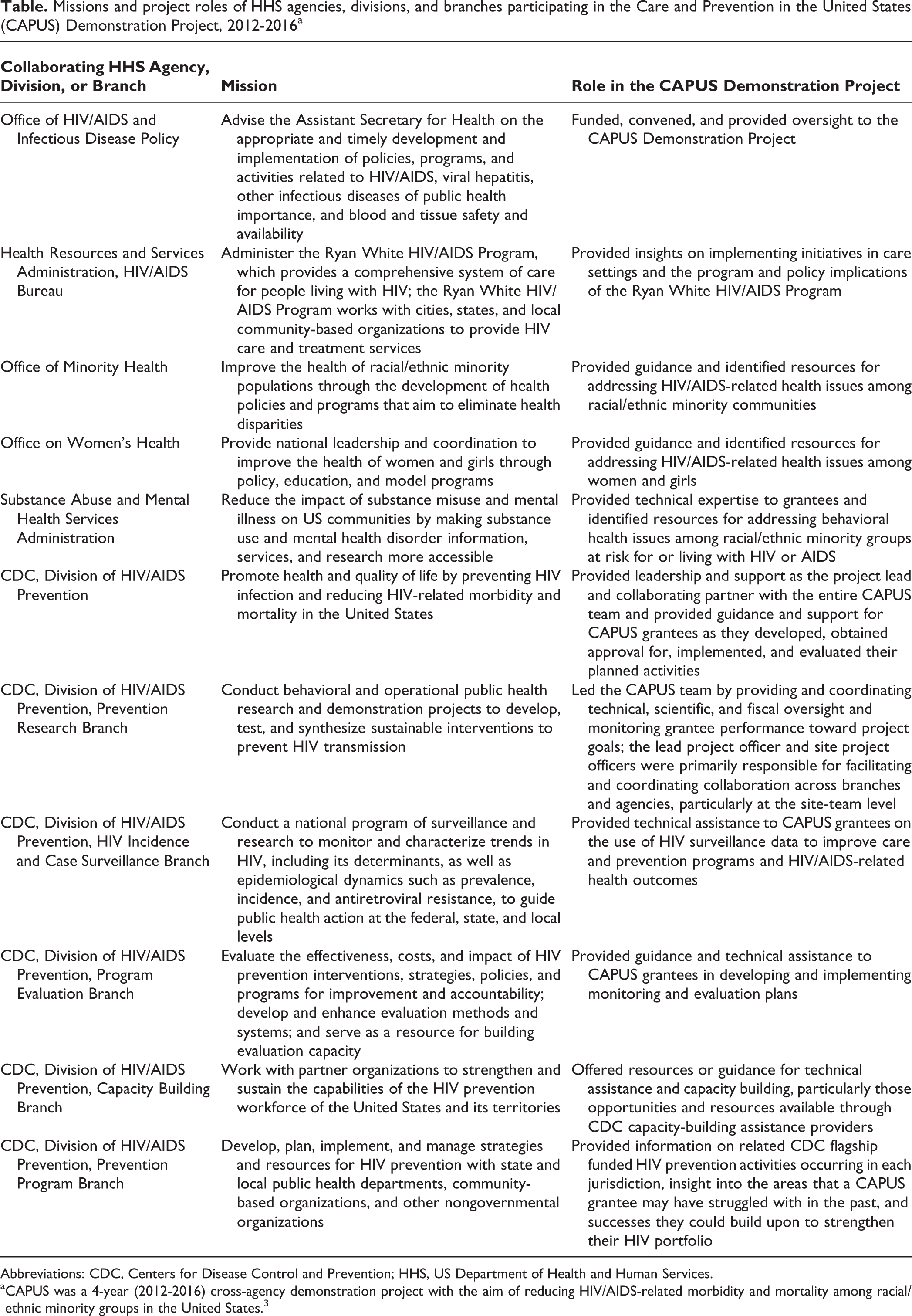
Abbreviations: CDC, Centers for Disease Control and Prevention; HHS, US Department of Health and Human Services.
aCAPUS was a 4-year (2012-2016) cross-agency demonstration project with the aim of reducing HIV/AIDS-related morbidity and mortality among racial/ethnic minority groups in the United States. 3
OHAIDP recognized that CAPUS’s success would depend on cross-agency partnerships and that one agency would need to lead development of the funding opportunity announcement (FOA) and shepherd the demonstration project from concept to completion. OHAIDP identified CDC as the lead agency because of the important role that HIV testing and linkage to care played in CAPUS, as well as CDC’s history of, and well-developed mechanisms for, funding both health departments and CBOs. As the lead agency, CDC provided leadership and support to its federal partners and guidance and support for CAPUS grantees as they developed, obtained approval for, implemented, and evaluated their planned activities. At the center of the collaboration was DHAP’s Prevention Research Branch, which provided overall leadership for the project; other DHAP branches also contributed their expertise. An organizational chart shows the CAPUS staffing plan and management structure and how the federal collaborators relate to each other (Figure).
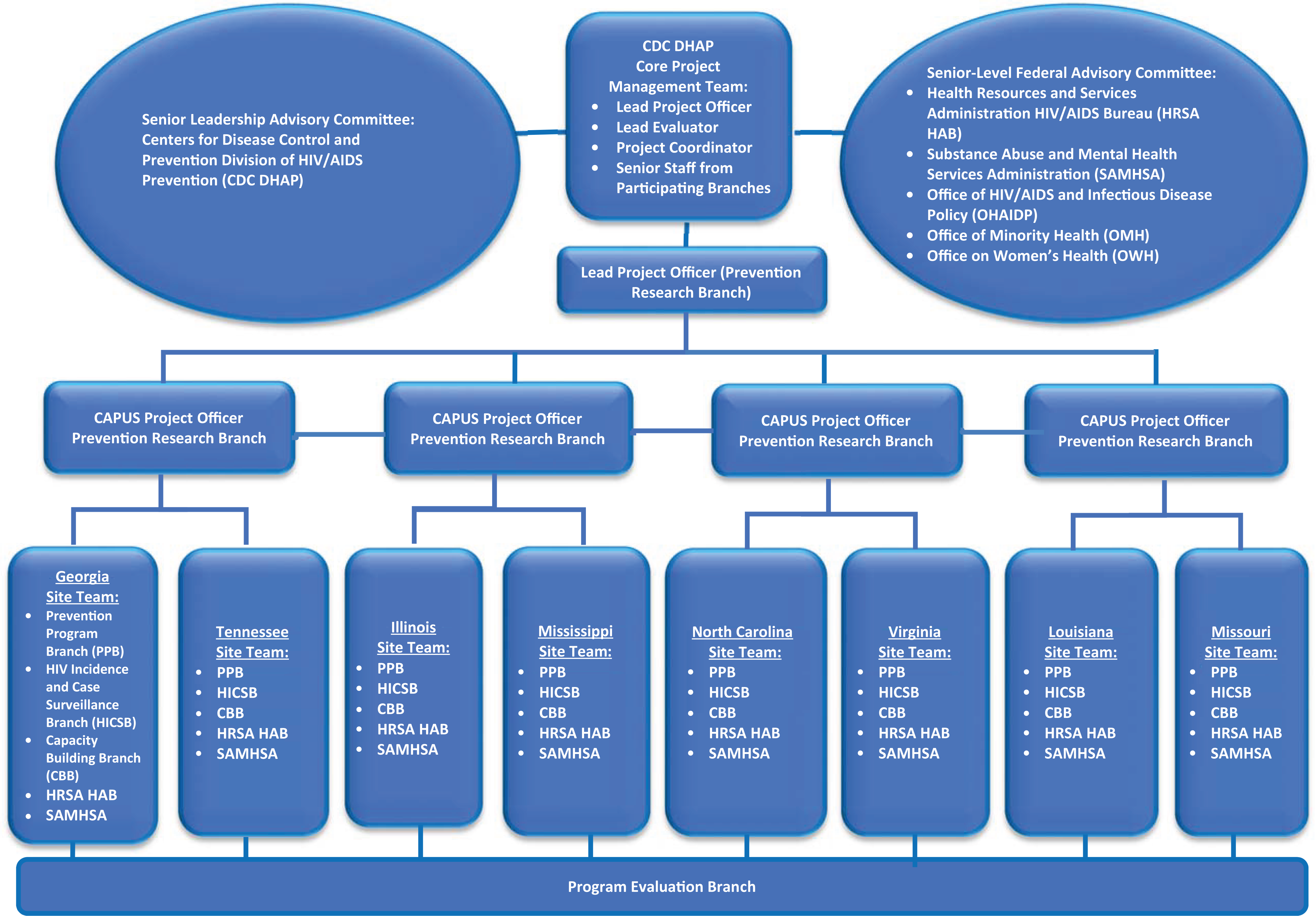
Staffing plan and management structure for the Care and Prevention in the United States (CAPUS) Demonstration Project, 2012-2016. CAPUS was a 4-year cross-agency demonstration project with the aim of reducing HIV/AIDS-related morbidity and mortality among racial/ethnic minority groups in the United States. 3
CDC established the Core Project Management Team—comprising the lead project officer, lead evaluator, project coordinator, and several senior staff members from participating branches—to advise project leads on day-to-day management issues and provide conceptual guidance on strategies and agency resources for overall project management. The CDC/DHAP Senior Advisory Committee, which comprised DHAP leadership, provided guidance to the Core Project Management Team on priorities and decision making for high-level project-management issues, communication strategies, and identifying and accessing agency resources. The Senior-Level Federal Partner Advisory Committee—representing 7 federal staff members from CDC, HRSA, SAMHSA, and OASH—facilitated collaboration among partner agencies and served as a resource and gatekeeper for agency- and jurisdiction-specific information and activities related to CAPUS. All collaborating agencies were expected to identify available resources from their agencies and branches (ie, federally funded activities in the state that grantees could leverage, other funding opportunities, potential collaborators), address jurisdiction-specific challenges, and develop strategies to enhance the work of CAPUS.
Federal staff members from the HRSA HIV/AIDS Bureau, SAMHSA, the Office of Minority Health, OHAIDP, and 5 branches of CDC’s DHAP committed their expertise, experiences, and resources to activities considered essential to planning, implementing, monitoring, and evaluating CAPUS. Often, expertise and experience came together to chart a cross-agency collaborative process that was new to many participants. The expectation of federal collaboration was apparent during each phase of CAPUS, including during cross-agency development and review of the FOA; inclusion of HRSA, SAMHSA, and OASH staff members in CDC’s applicant objective review process; cross-agency review of work plans and grantee progress reports; and participation in joint site visits. Although HIV-related outcomes are addressed in other articles in this supplemental issue of Public Health Reports, we highlight successes and challenges of CAPUS collaboration.
Successes of the Collaboration
During CAPUS, grantees were responsible for implementing activities detailed in their work plans. The federal collaboration supported the delivery of a comprehensive array of important HIV prevention and care services. CAPUS grantees, CDC/DHAP branches, and HHS collaborating partners integrated staff member time, expertise, and skill sets to complete important project tasks, including delivery of CAPUS’s 4 required components and any supplemental components grantees determined were needed to achieve the project goals. Federal CAPUS staff members identified 25 collaborative activities. We highlight a subset of these activities that federal partners indicated as central to CAPUS.
During the CAPUS planning phase, CDC branches and other partnering agencies collaborated to conceptualize and develop the FOA; include cross-agency representation on the objective review panel, which reviewed and scored the health department applications for CAPUS; develop a staffing plan, management structure, and initial draft of roles and responsibilities for collaborating agencies and branches; develop work plan guidance; review grantee work and evaluation plans and provide feedback; and develop guidance and reporting templates for the annual project report and interim project reports.
Cross-branch and cross-agency collaborations increased during the implementation and evaluation phases for a number of key activities: actively promoting the integration of HIV prevention, care, and surveillance; prompting federal staff members to collaborate across branch or agency and grantees to collaborate within and across their own agencies and with partners; advising and coordinating technical assistance for grantees; and working collaboratively with grantees to develop and implement monitoring and evaluation plans. Collaborative teams were also responsible for reviewing and providing feedback on annual progress reports and interim progress reports, participating in joint conference calls, meeting with site team members and grantee staff members, participating in planning, and conducting joint site visits. Finally, collaborative activities extended to providing technical advice on how to disseminate project findings, developing a publication agreement, and advising grantees on how to continue some of the services and programs after CAPUS funding ended.
Each agency shared its knowledge of HIV surveillance, program, care, behavioral health, and evaluation to enhance CAPUS grantees’ capacity to address HIV/AIDS-related morbidity and mortality. For example, SAMHSA contributed resources related to substance use and mental health disorder prevention and treatment providers, and HRSA provided information on care activities in the jurisdictions (eg, Ryan White HIV/AIDS Program). In addition, the Core Project Management team helped CAPUS grantees and site team members identify service gaps in jurisdictions and implement activities to address these gaps.
Anecdotal evidence from CAPUS highlights the importance of federal collaboration in events that contributed to CAPUS’s success. For example, multiagency, multibranch federal collaborations established early in the project signaled to grantees that CAPUS implementation required working collaboratively and leveraging available resources. One example was the collaboration among all grantees’ care, prevention, and surveillance staff members and their community partners for multiple CAPUS activities during program planning and implementation, meetings, and site visits. Federal collaborators consulted with each other to provide technical assistance and capacity-building assistance to grantees through webinars and peer-to-peer exchanges on topics such as patient navigation, Data to Care 7 (a public health strategy that uses HIV surveillance data to identify people with HIV not in care, link them to care, and support the HIV care continuum), HIV testing, and addressing the social determinants of health.
In addition, federal staff members from multiple agencies discussed issues and made recommendations to resolve those issues, including whether CAPUS-funded care services would be sustainable under existing HRSA funding mechanisms. Improvements in grantees’ service delivery, which can have a direct effect on health outcomes for target populations, is just one example of the influence of the federal collaboration.
Challenges of the Collaboration
CAPUS had numerous challenges. During the planning, implementation, and evaluation phases, federal CAPUS staff members encountered a dynamic project, eager and committed grantees, and federal staff members from several CDC DHAP branches and partnering HHS agencies. However, there was also some uncertainty as to how the federal collaboration was to be built and executed during CAPUS. The most common challenges were the following: Although the collaborating branches and agencies shared the same goals of increasing access to and use of HIV care and prevention services and reducing racial/ethnic disparities in HIV/AIDS-related morbidity and mortality, differences in organizational priorities and, to a lesser extent, organizational cultures, led to challenges in collaboration. For example, although SAMHSA participated in FOA development and in CAPUS site teams, SAMHSA staff members indicated that behavioral health was not adequately addressed among HIV prevention and care activities planned or implemented by grantees, which made the inclusion of SAMHSA staff members on site visits and on the Senior-Level Federal Advisory Committee essential. With 5 CDC branches, 5 partnering agencies, and an additional layer of senior leadership involved in CAPUS, it was challenging to manage decision-making processes, such as identifying how decisions were being made, who was making them, how they were being disseminated to partners, and how to ensure that everyone was speaking with the same voice. Grantees indicated early on that they were getting mixed and/or contradictory messages about points of emphasis or priority as they attempted to refine their work plans. Collaborating agencies and branches often had limited knowledge of each other’s organizational structure, mission, goals, resources, and relevant activities in CAPUS jurisdictions. For example, some collaborators faced a steep learning curve on how HRSA’s Ryan White HIV/AIDS Program operated in the 8 CAPUS jurisdictions. Federal staff members’ limited experience with participating in a multiagency, multibranch collaborative project and/or limited formal training in facilitating and engaging in effective collaborations also may have led to uncertainties about how to navigate some of the project’s administrative activities. For example, work plan review and approval processes were more extensive and complex than originally anticipated and involved multiple federal partners, causing some delays for grantees in meeting preestablished deadlines. Collaboration challenges that arose for grantees during planning and implementation included limited guidance on, knowledge of, and experience with implementing newer program requirements (eg, Data to Care, patient navigation, social and structural interventions). In addition, federal team members were uncomfortable with advising grantees on issues that fell outside of their area of expertise. Staff turnover and limited time available for staff members to participate in collaborative CAPUS activities because of competing agency or branch demands and priorities challenged the consistency and reliability of staff member engagement. CAPUS staff members had some difficulty reaching consensus about what, when, and how to monitor and evaluate CAPUS when multiple stakeholders were advocating for differing monitoring and evaluation approaches familiar to them.
Lessons Learned From the Collaboration
The following lessons learned may guide others who wish to use CAPUS as a model for cross-agency collaboration. Secure agency buy-in, commit to continuous engagement in the collaborative process, and identify supportive leaders at all levels. Without a clear road map for what the CAPUS collaboration would entail, it was difficult at times to sustain interest and involvement among all federal partners throughout the project. However, senior leaders played important roles in designing, supporting, implementing, and sustaining collaborations. Senior leaders identified key collaborators (which was particularly important given that many program requirements were new to federal partners and grantees); designed the project management and staffing structure; and defined and facilitated discussions about roles, responsibilities, and expectations for the collaboration. Senior leaders also monitored CAPUS progress through conference telephone calls, emails, site visits, and participation in annual grantee meetings and internal agency or branch meetings. Establish a shared vision for FOA goals and clarify staff member roles and responsibilities as soon as collaborators are identified and before the project is implemented. Clarifying project goals and staff member roles helps to prevent confusion and duplication of effort and increase staff member productivity. It also helps collaborators understand and value each other’s contributions and share in project responsibility. As CAPUS progressed and collaborators shared agency- and branch-specific expertise and resources, expectations became clearer through discussions and negotiations with collaborators. Plan, organize, and set goals internally among branches and with partnering agencies before grantees get involved. All partners should speak with one voice and use consistent messaging when providing guidance to grantees. Doing so ensures clarity and prevents the delivery of conflicting or contradictory messages that could impede project progress—something that several grantees identified as a problem during the work plan revision process. Collaborating partners need regularly scheduled internal communication (eg, telephone calls, meetings) that focuses on the collaboration, including relevant organizational structures, available resources, and other pertinent issues. This internal communication allows for a more coordinated response when advising grantees and addressing issues in a timely fashion. The frequency and need for communication will vary during the course of the project. Be realistic about expectations for collaboration, including recognizing competing demands, the need to provide partnership-supporting resources, and changes in workloads. Prioritize the greatest needs for collaboration and be flexible. Understand that when the needs of the project change, the collaborators’ roles and level of engagement may also change. For example, the frequency of meetings for the CDC-DHAP Senior Leadership Advisory Committee, the Senior-Level Federal Advisory Committee, and site teams decreased as the project progressed. Maintain a viable communications plan that ensures key project staff members and collaborators have the information they need, including project expectations, roles, and responsibilities; timely updates; and appropriate communication channels. The communications plan should include, for example, strategies for reviewing work plans and progress reports, processes for providing regular project updates, and notifications about changes in scheduled times for conference calls and dates for site visits. Cross-agency partners should visit sites to help ensure diverse expertise and experience at project sites. Encourage (or ensure) that all partners engage in in-depth, collaborative discussions with grantees about their goals, progress, challenges, problem-solving strategies, and future activities. Plan an agenda for site visits and conduct debriefing sessions with the cross-agency site team after the visit to make recommendations and plan next steps. Under CAPUS, CDC/Prevention Program Branch and HRSA/Ryan White HIV/AIDS Program project officers informed discussions on leveraging resources and sustaining activities using prevention and care resources. In addition, grantees and federal partners found the joint site visits useful for identifying viable strategies, resources, and opportunities to advance project goals.
Public Health Implications
Several federal agencies, their subdivisions, and dozens of federal staff members participated in CAPUS. The collaboration brought together public health professionals with a range of expertise, training, and perspectives in several relevant disciplines (eg, epidemiologists, psychologists, social workers, physicians, and policy analysts). The merging of such diverse knowledge is a testament to the feasibility and opportunity of a sustained cross-agency effort designed to improve the health outcomes of racial/ethnic minority groups disproportionately affected by HIV/AIDS. Successful cross-agency federal partnerships, particularly those with the level of complexity required for CAPUS, can be challenging. Fortunately, the experience of CDC’s Enhanced Comprehensive HIV Prevention Planning (ECHPP) project helped to inform the level of federal cross-agency collaboration seen in CAPUS. 8 ECHPP was a 3-year, CDC-led demonstration project that used enhanced planning, coordination, data reporting, and implementation strategies to maximize the impact of HIV prevention in 12 metropolitan statistical areas with the highest prevalence of HIV/AIDS in the United States. 9
In CAPUS, as with the ECHPP project, multiple federal partners collaborated to change public health practice in HIV prevention and care. However, the level of collaboration and engagement in CAPUS was more intensive at the project and site team level than with the ECHPP project and other projects. Ultimately, collaborative efforts helped to improve targeting, coordination, and continuity of care for people living with HIV in CAPUS jurisdictions. HRSA and SAMHSA worked with grantees and site teams on how to sustain CAPUS activities using Ryan White HIV/AIDS Program funding to support community health workers, patient navigators, and behavioral health services funded by SAMHSA-supported clinics. CAPUS challenged federal agencies and branches to build a shared vision, develop a cross-agency FOA, reach consensus in work plan reviews, and allocate staff member time and resources. Grantees benefited from wide-ranging expertise in HIV prevention and care to develop innovative, comprehensive approaches to address challenges that arose during CAPUS.
The CAPUS structure created opportunities for continued cross-agency and/or cross-branch collaborations. For example, CDC, HRSA, and OHAIDP built on their experiences and improved mutual understanding to launch other SMAIF-funded cross-agency collaborative projects. One such undertaking was Partnerships for Care, a 3-year project (2014-2017) initiated by CDC/DHAP and HRSA’s Bureau of Primary Health Care that supported expanded HIV service delivery in communities highly affected by HIV. 10 In June 2015, HRSA and CDC also released the joint Integrated HIV Prevention and Care Plan Guidance, which provides a framework for state grantees to support collaboration and coordination in the use of data to better inform HIV prevention and care program planning, resource allocation, and evaluation in jurisdictions. 11 The lessons from CAPUS suggest how federal collaboration may be an essential and strategic component in addressing the racial/ethnic HIV-related health disparities that continue to challenge us.
Footnotes
Authors’ Note
The findings and conclusions of this article do not necessarily reflect the official position of the US Department of Health and Human Services’ Office of HIV/AIDS and Infectious Disease Policy, the Centers for Disease Control and Prevention, the Health Resources and Services Administration, the Substance Abuse and Mental Health Services Administration, or the Office of Minority Health.
Acknowledgments
The authors acknowledge the CAPUS grantees and their collaborating partners for their demonstrated commitment to addressing persistent HIV-related health disparities in their communities. The authors also recognize all members of the federal collaboration, including project officers, site team members, the Core Management Team, the Department of HIV/AIDS Prevention’s Senior Leadership Advisory Committee, the Senior-Level Federal Advisory Committee, and the National Association of State and Territorial AIDS Directors for their valuable contributions in guiding this project.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Care and Prevention in the United States (CAPUS) Demonstration Project was supported by the Secretary’s Minority AIDS Initiative Fund and led by the Centers for Disease Control and Prevention (PS 12-1210).