
Abstract
Objectives:
The Care and Prevention in the United States Demonstration Project included implementation of a Data to Care strategy using surveillance and other data to (1) identify people with HIV infection in need of HIV medical care or other services and (2) facilitate linkages to those services to improve health outcomes. We present the experiences of 4 state health departments: Illinois, Louisiana, Tennessee, and Virginia.
Methods:
The 4 state health departments used multiple databases to generate listings of people with diagnosed HIV infection (PWH) who were presumed not to be in HIV medical care or who had difficulty maintaining viral suppression from October 1, 2013, through September 29, 2016. Each health department prioritized the listings (eg, by length of time not in care, by viral load), reviewed them for accuracy, and then disseminated the listings to staff members to link PWH to HIV care and services.
Results:
Of 16 391 PWH presumed not to be in HIV medical care, 9852 (60.1%) were selected for follow-up; of those, 4164 (42.3%) were contacted, and of those, 1479 (35.5%) were confirmed to be not in care. Of 794 (53.7%) PWH who accepted services, 694 (87.4%) were linked to HIV medical care. The Louisiana Department of Health also identified 1559 PWH as not virally suppressed, 764 (49.0%) of whom were eligible for follow-up. Of the 764 PWH who were eligible for follow-up, 434 (56.8%) were contacted, of whom 269 (62.0%) had treatment adherence issues. Of 153 PWH who received treatment adherence services, 104 (68.0%) showed substantial improvement in viral suppression.
Conclusions:
The 4 health departments established procedures for using surveillance and other data to improve linkage to HIV medical care and health outcomes for PWH. To be effective, health departments had to enhance coordination among surveillance, care programs, and providers; develop mechanisms to share data; and address limitations in data systems and data quality.
Keywords
People with diagnosed HIV infection (PWH) who receive treatment can improve their health outcomes by maintaining viral suppression and preventing further transmission. Goals of the National HIV/AIDS Strategy and other HIV prevention goals have focused on increasing access to HIV care and treatment and improving health outcomes for PWH. 1,2 The Care and Prevention in the United States (CAPUS) Demonstration Project (hereinafter, CAPUS) was a 4-year (2012-2016), cross-agency demonstration project funded by the US Department of Health and Human Services Secretary’s Minority AIDS Initiative Fund through the Centers for Disease Control and Prevention (CDC). The primary goals of CAPUS were to (1) increase the proportion of racial/ethnic minority groups whose HIV infection was diagnosed and (2) optimize linkage to, retention in, and reengagement in care for people with newly diagnosed HIV infection or previously diagnosed HIV infection by addressing social, economic, clinical, and structural factors that influence HIV health outcomes. CAPUS funded 8 state health department programs to improve HIV care and prevention outcomes by using HIV surveillance and other data. 3,4
Health departments use HIV surveillance data to monitor trends in HIV diagnoses, stage the progression of disease, and describe the epidemiology of HIV disease; they also may use these data for public health interventions. 2,5 -7 Data to Care (D2C) is a high-impact public health strategy that uses HIV surveillance and other data to identify PWH who are in need of HIV medical care and other services and link them to those services. 8 -10 D2C programs at each health department use CD4+ T-lymphocyte (CD4) and HIV viral load laboratory data routinely reported through HIV surveillance as markers of HIV care. 2,11 PWH without reported test results during a specified period are classified as not in care. D2C programs follow up with PWH not in care and offer to help link them to medical care or reengage them with medical care. In addition, D2C programs may identify PWH who are in care but who have persistently high (ie, unsuppressed) viral load results and offer treatment adherence support or other services. This article summarizes the experiences of 4 of the 8 CAPUS grantees—the state health departments of Illinois, Louisiana, Tennessee, and Virginia—that initiated their D2C programs earlier and reported complete data while CAPUS was implemented.
Materials and Methods
Preimplementation Activities
The 4 health departments began preparing for D2C activities as early as 2011. These pre-CAPUS activities were implemented by using funds from other HIV prevention and care projects supported by CDC and the Health Resources and Services Administration (HRSA). The Illinois, Louisiana, and Tennessee state health departments focused on HIV medical care engagement activities, and the Virginia Department of Health focused on planning and developing an integrated Care Markers Database.
During preimplementation, D2C programs evaluated laboratory reporting laws and procedures, quality and completeness of HIV surveillance and laboratory data, and availability of additional data sources. All 4 health departments had requirements in place in 2012 or earlier for reporting CD4 and HIV viral load test results as part of routine surveillance activities. 12 Each health department reviewed data-sharing laws and policies and the need for new data-sharing agreements and partnerships, and prioritized data (eg, by length of time not in care, by viral load) to generate lists of PWH who were not in care (ie, not-in-care lists). The health departments found that memoranda of understanding as well as data-sharing, coordinated-care, and services agreements were important for initiating D2C processes. D2C programs leveraged partnerships with medical facilities, HRSA-funded Ryan White HIV/AIDS Program care providers, and community-based organizations—particularly those with patient navigation programs—to conduct investigations and linkage activities, identify resources and technical assistance needs, and minimize duplication of services. D2C programs also held partner meetings to increase awareness and buy-in of D2C initiatives. CDC determined this project constituted nonresearch activity; therefore, institutional review board approval was not required.
Implementation Activities
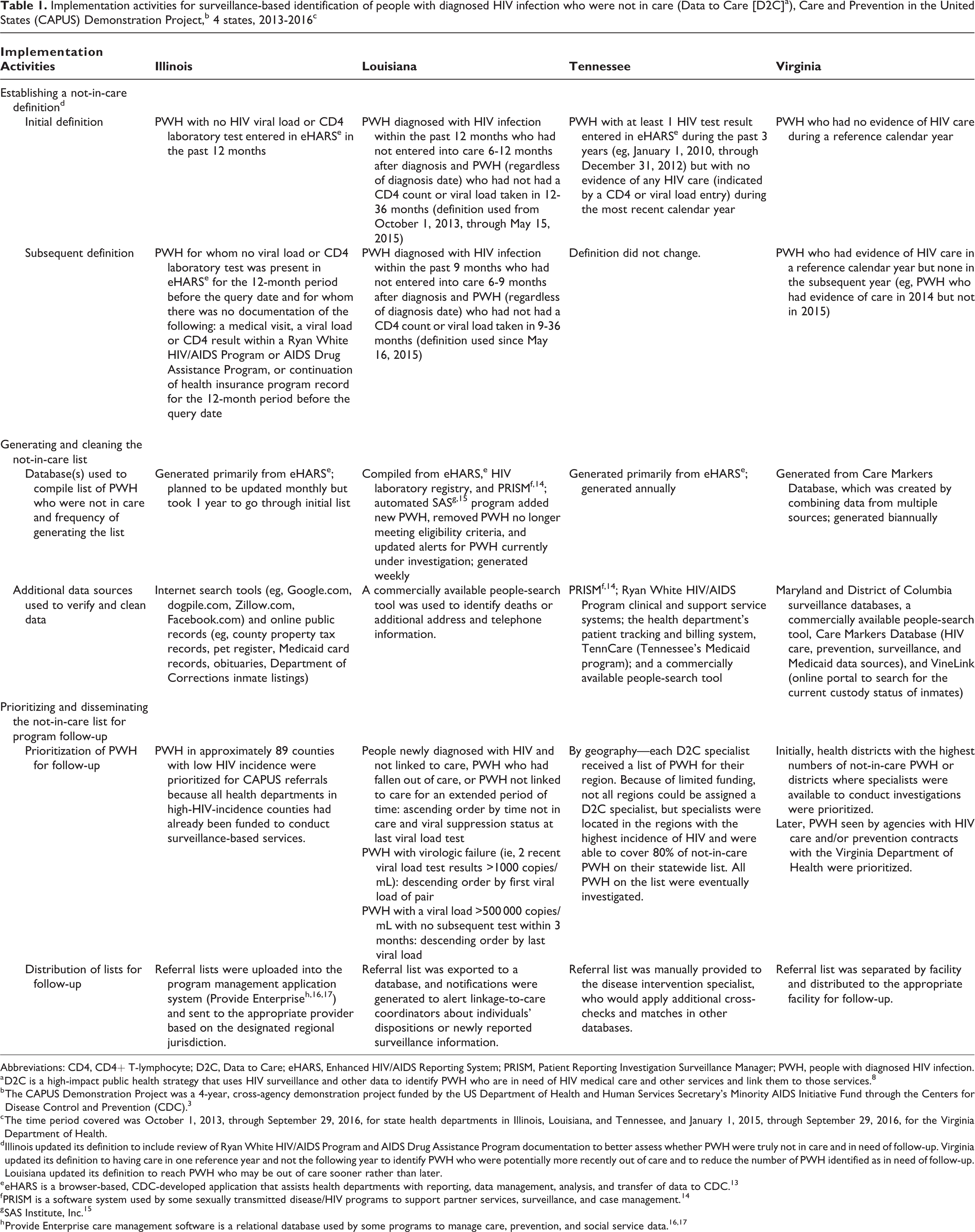
The Illinois, Louisiana, and Tennessee state health departments implemented the project during a 3-year period (2013-2016), and the Virginia Department of Health implemented the project during a 2-year period (2014-2016). D2C implementation activities included establishing a not-in-care definition and generating and cleaning the not-in-care list, prioritizing and disseminating the not-in-care list for program follow-up (Table 1), and providing linkage and reengagement services to PWH not in care (Table 2).
Implementation activities for surveillance-based identification of people with diagnosed HIV infection who were not in care (Data to Care [D2C]a), Care and Prevention in the United States (CAPUS) Demonstration Project,b 4 states, 2013-2016c
Abbreviations: CD4, CD4+ T-lymphocyte; D2C, Data to Care; eHARS, Enhanced HIV/AIDS Reporting System; PRISM, Patient Reporting Investigation Surveillance Manager; PWH, people with diagnosed HIV infection.
a D2C is a high-impact public health strategy that uses HIV surveillance and other data to identify PWH who are in need of HIV medical care and other services and link them to those services. 8
b The CAPUS Demonstration Project was a 4-year, cross-agency demonstration project funded by the US Department of Health and Human Services Secretary’s Minority AIDS Initiative Fund through the Centers for Disease Control and Prevention (CDC). 3
c The time period covered was October 1, 2013, through September 29, 2016, for state health departments in Illinois, Louisiana, and Tennessee, and January 1, 2015, through September 29, 2016, for the Virginia Department of Health.
dIllinois updated its definition to include review of Ryan White HIV/AIDS Program and AIDS Drug Assistance Program documentation to better assess whether PWH were truly not in care and in need of follow-up. Virginia updated its definition to having care in one reference year and not the following year to identify PWH who were potentially more recently out of care and to reduce the number of PWH identified as in need of follow-up. Louisiana updated its definition to reach PWH who may be out of care sooner rather than later.
e eHARS is a browser-based, CDC-developed application that assists health departments with reporting, data management, analysis, and transfer of data to CDC. 13
f PRISM is a software system used by some sexually transmitted disease/HIV programs to support partner services, surveillance, and case management. 14
g SAS Institute, Inc. 15
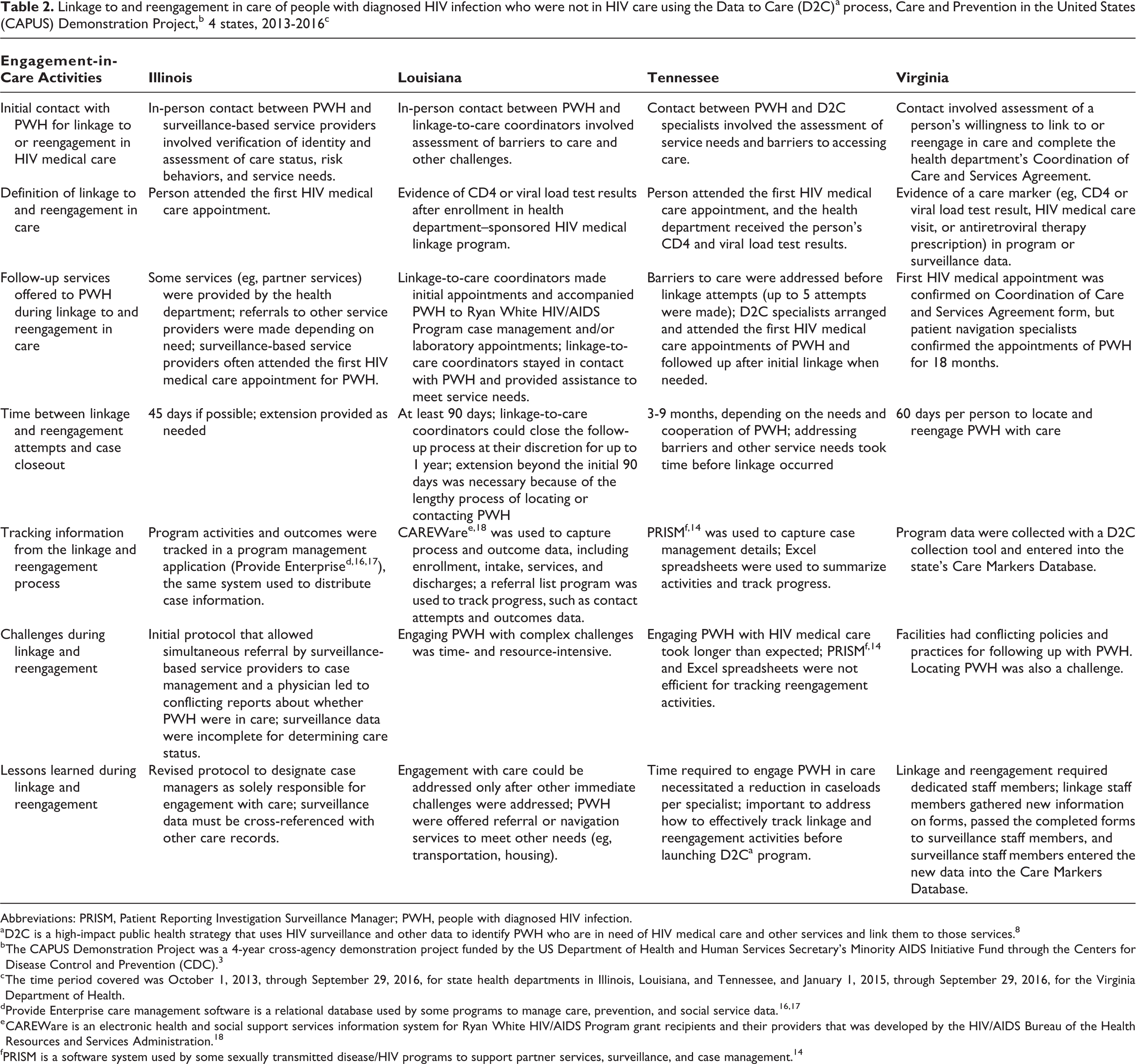
Linkage to and reengagement in care of people with diagnosed HIV infection who were not in HIV care using the Data to Care (D2C)a process, Care and Prevention in the United States (CAPUS) Demonstration Project,b 4 states, 2013-2016c
Abbreviations: PRISM, Patient Reporting Investigation Surveillance Manager; PWH, people with diagnosed HIV infection.
a D2C is a high-impact public health strategy that uses HIV surveillance and other data to identify PWH who are in need of HIV medical care and other services and link them to those services. 8
b The CAPUS Demonstration Project was a 4-year cross-agency demonstration project funded by the US Department of Health and Human Services Secretary’s Minority AIDS Initiative Fund through the Centers for Disease Control and Prevention (CDC). 3
c The time period covered was October 1, 2013, through September 29, 2016, for state health departments in Illinois, Louisiana, and Tennessee, and January 1, 2015, through September 29, 2016, for the Virginia Department of Health.
d Provide Enterprise care management software is a relational database used by some programs to manage care, prevention, and social service data. 16,17
e CAREWare is an electronic health and social support services information system for Ryan White HIV/AIDS Program grant recipients and their providers that was developed by the HIV/AIDS Bureau of the Health Resources and Services Administration. 18
f PRISM is a software system used by some sexually transmitted disease/HIV programs to support partner services, surveillance, and case management. 14
The health departments used various definitions to identify PWH as not in care. However, all 4 departments used the following criteria to identify PWH as not in care: currently alive, an HIV diagnosis or laboratory test reported within a certain period, and no evidence of HIV care (ie, no reported CD4 or viral load test) during a defined reference period (the number of months in each period varied by health department). The Illinois and Virginia state health departments also incorporated documentation of a medical visit or a prescription for antiretroviral therapy into their not-in-care definitions. The Illinois, Tennessee, and Virginia state health departments defined the not-in-care period as 12 months without evidence of care; the Virginia Department of Health defined not in care as evidence of care in 1 reference calendar year with no evidence of care in the following year (eg, evidence of care in 2014 but not in 2015).
The Louisiana Department of Health’s definition for not in care included people diagnosed with HIV infection within the past 12 months who had not entered into care 6-12 months after diagnosis and PWH (regardless of diagnosis date) who had not had a CD4 count or viral load taken in 12-36 months (definition used from October 1, 2013, through May 15, 2015). On May 16, 2015, the definition was updated to include PWH diagnosed with HIV infection within the past 9 months who had not entered into care 6-9 months after diagnosis and PWH (regardless of diagnosis date) who had not had a CD4 count or viral load taken in 9-36 months. In addition, Louisiana followed PWH who potentially had virologic failure (ie, 2 viral load test results >1000 copies/mL with no clinically significant decrease or a viral load >500 000 copies/mL with no subsequent test within 3 months). 19
Steps in the Data to Care Process
Implementation of D2C programs required multiple activities in each step of the D2C process.
Step 1: PWH presumed to be not in care
The health departments generated listings of PWH presumed to meet the selection criteria from surveillance data and other sources. Illinois and Tennessee used their HIV surveillance database only, whereas Louisiana and Virginia combined their surveillance databases with other data sources, such as HIV laboratory data systems or partner services data systems. Louisiana updated its list weekly in an iterative automated process that also checked against its most recent referrals to identify which PWH were eligible for follow-up of linkage and reengagement activities. 20 Virginia created a Care Markers Database by combining data from multiple sources (eg, Medicaid, electronic provider records, electronic laboratory reports, and the AIDS Drug Assistance Program, among others) and used the database biannually to generate a list of PWH not in care. 21,22 Tennessee generated its list annually, and Illinois generated its list monthly. 23
Step 2: Verify data and prioritize PWH for follow-up
Every program cleaned data before determining eligibility for follow-up. Data cleaning included matching preliminary listings of PWH presumed to be not in care with other data sources to remove PWH who (1) had died, (2) had moved out of the jurisdiction, (3) were found to be in care, (4) were incarcerated, (5) were homeless (or were otherwise hard to reach), or (6) were currently under not-in-care investigation. The health departments used various data sources in this step, including databases for Ryan White HIV/AIDS Program services, the AIDS Drug Assistance Program, partner services, Medicaid, and health department patient services or billing systems. Information from ongoing not-in-care investigations or linkage efforts also informed data cleaning. Three jurisdictions used a commercially available people-search tool to obtain current contact information, such as addresses and telephone numbers. Health departments obtained additional contact information from other health databases (eg, sexually transmitted disease surveillance, partner services, Ryan White HIV/AIDS Program services, Medicaid) or through publicly available online searches (eg, Google, tax records, obituaries, corrections listings).
When data-cleaning activities involved manipulating electronic data (ie, matching databases rather than manual look-up), having a master’s-level data analyst with experience in managing relational databases and statistical software on staff improved efficiency. Manual data cleaning could be performed by staff members with a college degree and some public health experience.
Each program prioritized PWH for follow-up in its own way. Because resources for D2C program specialists were limited, Tennessee prioritized not-in-care PWH living in geographic regions where D2C program specialists were assigned (ie, in regions with the highest incidence of HIV, which covered 80% of PWH not in care in the state). Louisiana prioritized PWH who had been out of care for a long time or whose last viral load was detectable. Illinois prioritized PWH living in regions that were not covered by previously funded HRSA or CDC HIV prevention and care projects. Virginia prioritized PWH living in health districts with the highest numbers of not-in-care PWH, with available specialists to conduct investigations, and where agencies had HIV services contracts with the Virginia Department of Health to perform follow-up.
Steps 3 and 4: Contact PWH and determine care status
After verifying, cleaning, and prioritizing the listings of not-in-care PWH, the health departments distributed the listings to linkage-to-care coordinators, disease intervention specialists, or other designated health department or partner agency staff members. Designated staff members attempted to contact PWH to confirm their care status as being in care or not in care and tracked the number of contact attempts. Some PWH were not contacted because the program determined they were deceased, out of jurisdiction, incarcerated, or for other reasons (eg, unable to locate).
Steps 5 and 6: Provide linkage or reengagement services and confirm engagement in care
In general, the linkage and reengagement process (Table 2) began with face-to-face or telephone contact with PWH. During the interviews, health department staff members assessed individuals’ needs for, and barriers to, accessing HIV medical care. Because PWH who had never received treatment or who had dropped out of HIV medical care often had multiple unmet needs (eg, food, housing, employment) and barriers to care (eg, transportation, health insurance, and behavioral health issues), they were offered referral or navigation services to meet these nonmedical needs before or while they were provided linkage to medical care. In all the D2C programs, staff members accompanied PWH to their initial medical appointments and offered assistance after the initial appointment. Follow-up data were captured in locally developed or existing systems modified for D2C purposes.
D2C programs reported similar definitions for linkage to and reengagement in care, which included keeping medical appointments (indicated mostly by laboratory markers, such as CD4 or viral load test results). However, the time between linkage-to-care attempts and case closeout ranged from 1.5 months in Illinois to 9 months in Tennessee; some D2C programs provided additional time as needed.
Linkage and reengagement staff members had various job titles (eg, surveillance-based service providers, linkage-to-care coordinators, and D2C specialists), education levels (eg, <college degree, college degree, or graduate degree), experience (eg, disease intervention, case management, nursing, social work, or patient navigation), and training (eg, risk-reduction counseling, treatment adherence).
Step 7: Enter information acquired into surveillance system
After completing linkage activities, program staff members entered new information obtained through D2C activities into the surveillance database to correct erroneous information (eg, PWH wrongly identified as not in care), increase data completeness, and improve overall program efficiency. All 4 D2C programs provided updated information to the HIV surveillance program, such as changes in names, dates of birth, current gender, telephone number, current address, vital status, transmission risk, test results, and incarceration status. Information about PWH’s awareness of their HIV status, whether they were taking antiretroviral therapy, and whether they wished to be contacted for HIV medical care engagement services was also shared. In Louisiana and Virginia, linkage or reengagement workers completed the Adult HIV Confidential Case Report Form or a similar form with new information and then submitted the forms either electronically or manually to the surveillance unit. Illinois developed an easily queried electronic system that expedited reporting, lessened the burden on D2C program and data management staff members, and improved the capacity to summarize the number of updated records.
Results
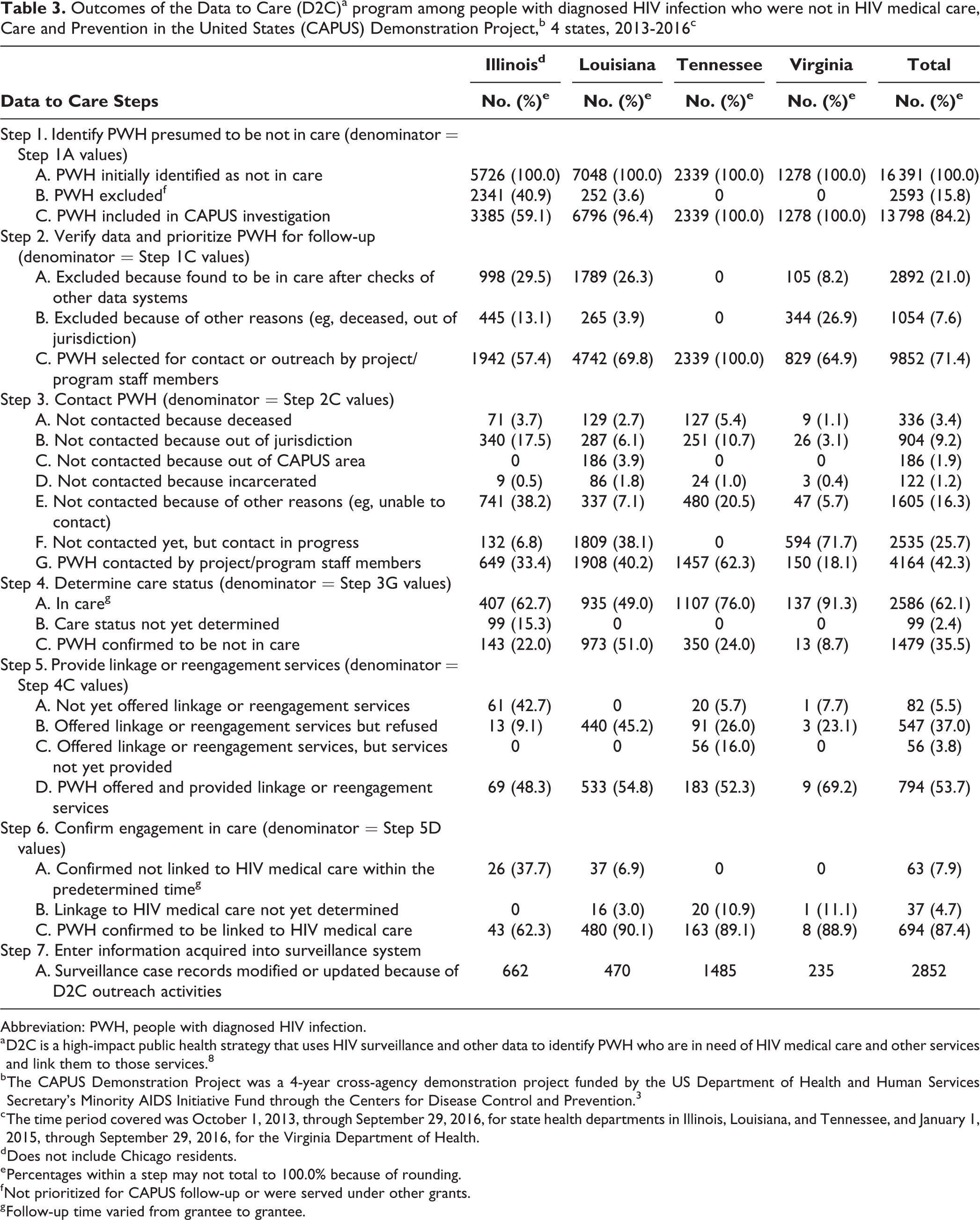
A total of 16 391 PWH (range, 1278-7048 per program) were initially presumed to be not in care by the 4 state health departments. Of 16 391 PWH presumed to be not in care, D2C programs excluded 2593 (15.8%) because they were being served under other grants or were not prioritized for CAPUS follow-up, which left 13 798 (84.2%) for follow-up (Figure 1; Table 3). Reviewing data on PWH and matching them to other available data led to the exclusion of 1054 (7.6%) PWH who were deceased or out of jurisdiction and 2892 (21.0%) PWH already in care. After exclusions, the D2C programs prioritized 9852 of 13 798 (71.4%) not-in-care PWH, or 9852 of 16 391 (60.1%) PWH initially presumed to be not in HIV care, for follow-up.
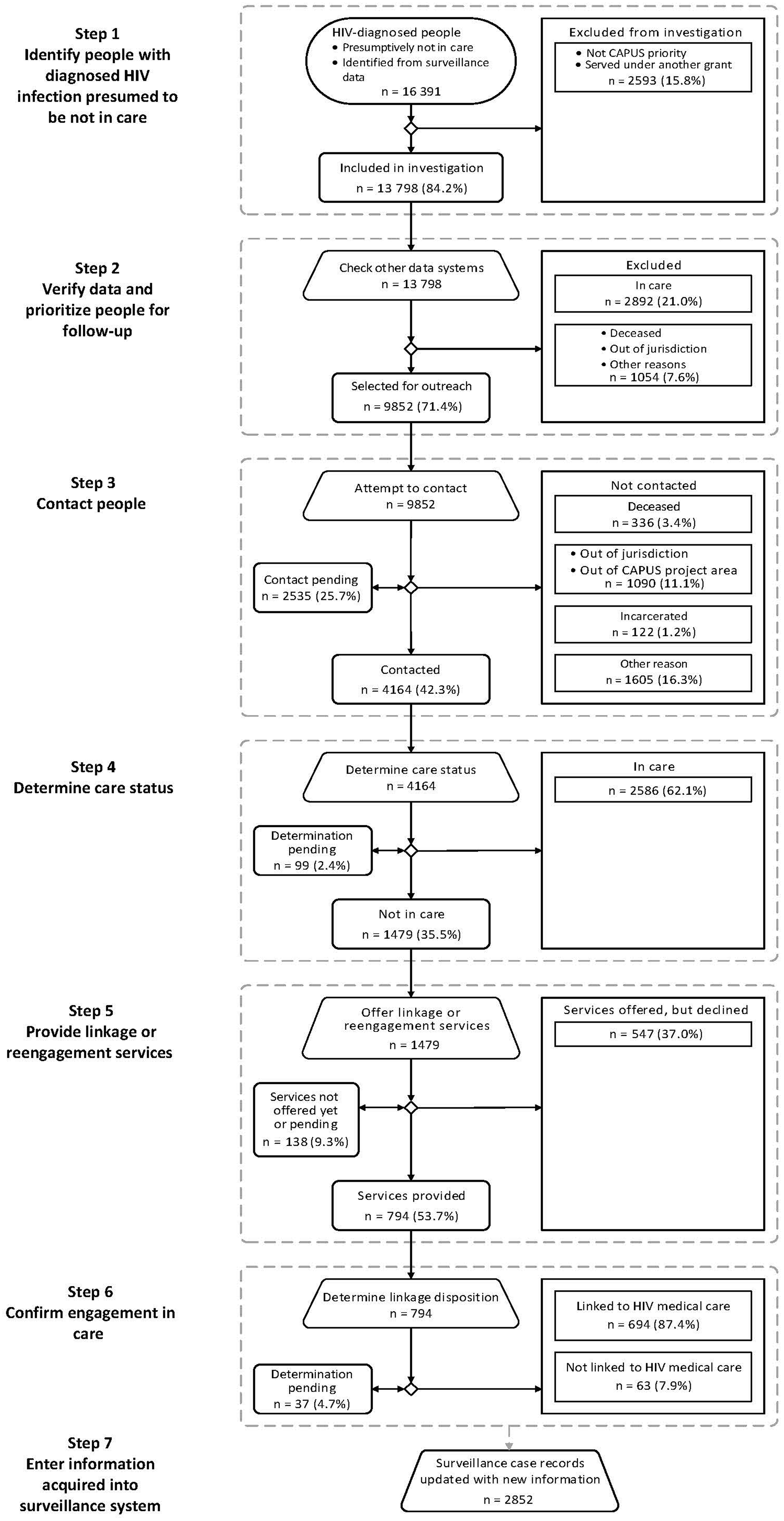
Data to Care (D2C) process and overall outcomes among people with diagnosed HIV infection and not in HIV medical care, Care and Prevention in the United States (CAPUS) Demonstration Project, Illinois, Louisiana, Tennessee, and Virginia state health departments, 2013-2016. D2C is a high-impact public health strategy that uses HIV surveillance and other data to identify people with diagnosed HIV infection who are in need of HIV medical care and other services and link them to those services. 8 The CAPUS Demonstration Project was a 4-year cross-agency demonstration project funded by the US Department of Health and Human Services Secretary’s Minority AIDS Initiative Fund through the Centers for Disease Control and Prevention. 3 The time period covered was October 1, 2013, through September 29, 2016, for state health departments in Illinois, Louisiana, and Tennessee, and January 1, 2015, through September 29, 2016, for the Virginia Health Department.
Outcomes of the Data to Care (D2C)a program among people with diagnosed HIV infection who were not in HIV medical care, Care and Prevention in the United States (CAPUS) Demonstration Project,b 4 states, 2013-2016c
Abbreviation: PWH, people with diagnosed HIV infection.
a D2C is a high-impact public health strategy that uses HIV surveillance and other data to identify PWH who are in need of HIV medical care and other services and link them to those services. 8
b The CAPUS Demonstration Project was a 4-year cross-agency demonstration project funded by the US Department of Health and Human Services Secretary’s Minority AIDS Initiative Fund through the Centers for Disease Control and Prevention. 3
c The time period covered was October 1, 2013, through September 29, 2016, for state health departments in Illinois, Louisiana, and Tennessee, and January 1, 2015, through September 29, 2016, for the Virginia Department of Health.
d Does not include Chicago residents.
e Percentages within a step may not total to 100.0% because of rounding.
f Not prioritized for CAPUS follow-up or were served under other grants.
g Follow-up time varied from grantee to grantee.
The 4 state health departments successfully contacted 4164 of 9852 (42.3%) PWH selected for contact during the D2C program. Of the 9852 PWH whom staff members attempted to contact, 2535 (25.7%) were still being contacted at the end of the program period, 904 (9.2%) were out of jurisdiction, 336 (3.4%) were deceased, 122 (1.2%) were incarcerated, and 1605 (16.3%) were not contacted for other reasons (eg, unable to contact). Of 4164 PWH contacted, 1479 (35.5%) were not in care. Of the 1479 PWH confirmed as not in care, 794 (53.7%) were offered and provided linkage or reengagement services, 547 (37.0%) refused services, and 138 (9.3%) were in process and had not yet been offered or provided services by the end of the project period. The percentage of PWH confirmed linked to care was higher when calculated among PWH who accepted services (87.4%, 694 of 794) than among all PWH confirmed as not in care and contacted by program staff members (46.9%, 694 of 1479). A total of 2852 surveillance records were updated because of D2C program investigations.
In Louisiana, of 1559 PWH initially identified from surveillance data as being in care but having difficulty maintaining viral suppression, 962 (61.7%) were selected for follow-up (Figure 2). A total of 198 of 962 (20.6%) PWH were excluded because they had a viral load measure taken <90 days before the previous viral load measure, no longer had virologic failure, were deceased, or were out of jurisdiction. D2C program staff members successfully contacted 434 of 764 (56.8%) PWH selected for contact by the end of the reporting period to determine treatment adherence status. Of these 434 PWH, 165 (38.0%) were adhering to treatment or working on issues with their physician (self-reported), and 269 (62.0%) had a potential treatment adherence issue. Of the 269 PWH with potential treatment adherence issues, 153 (56.9%) were offered and provided adherence and support services, and 116 (43.1%) refused services. Overall, 104 of 153 (68.0%) PWH who accepted services were confirmed to have a substantially improved viral load (ie, a 3-fold decrease in viral load).
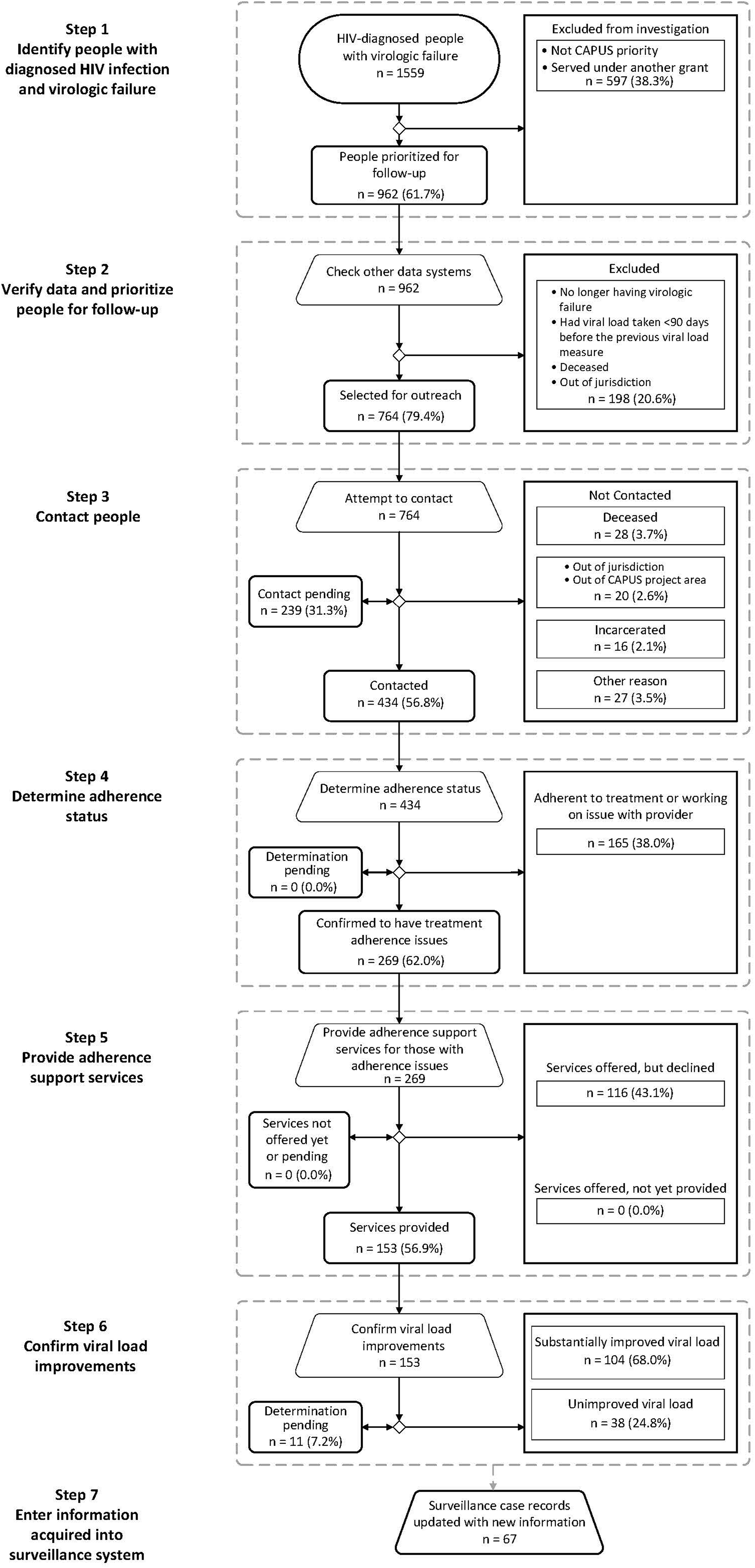
Steps and outcomes of the Data to Care (D2C) process among people with diagnosed HIV infection (PWH) who had virologic failure, Care and Prevention in the United States (CAPUS) Demonstration Project, Louisiana Department of Health, 2012-2016. D2C is a high-impact public health strategy that uses HIV surveillance and other data to identify PWH who are in need of HIV medical care and other services and link them to those services. 8 The CAPUS Demonstration Project was a 4-year cross-agency demonstration project funded by the US Department of Health and Human Services Secretary’s Minority AIDS Initiative Fund through the Centers for Disease Control and Prevention (CDC). 3 Virologic failure was defined as 2 consecutive viral load test results >1000 copies/mL at least 90-365 days apart in the past year with no clinically significant decrease between results (defined as a 3-fold decrease in viral load) or a viral load >500 000 copies/mL with no subsequent test within 3 months. PWH with an undetectable viral load within the past year and a subsequent viral load (taken at least 90 days later) that was >1000 copies/mL were excluded. This criterion was in place from October 1, 2013, through July 7, 2014, to exclude PWH who had minor changes in their viral load or other treatment-related issues unrelated to adherence. This D2C activity was implemented between October 1, 2013, and September 29, 2016, by the Louisiana Department of Health. A substantially improved viral load was defined as a 3-fold decrease in viral load. Data source: Panel on Antiretroviral Guidelines for Adults and Adolescents. 19
Lessons Learned
CAPUS implementation identified gaps in data and set the groundwork for establishing new data-sharing processes, procedures, and partnerships to improve data quality. More complete laboratory reporting and updated data on vital status, address, risk behaviors, and other key information provided through the feedback process improved surveillance data in these jurisdictions. Data gaps might not have been identified and addressed if health departments had not implemented the D2C program. In addition, the feedback process created opportunities for increased communication, understanding of roles, and collaboration between prevention program and surveillance units.
The D2C program required intensive data verification, cleaning, and integration of information from various public health data sources to narrow the number of PWH eligible for contact, which eliminated a large proportion of PWH who were ineligible because they were deceased, out of jurisdiction or project area, or incarcerated. Cleaning data and creating iterative processes that incorporated information learned from investigations created new efficiencies.
Leveraging other data systems to supplement surveillance data was important. Two jurisdictions created systems that combined data from multiple health department programs to produce a better record of the HIV care status and contact information for PWH. Obtaining the current address for PWH was challenging, particularly for PWH who moved frequently. Integrating data sources to identify incarcerated PWH was also worthwhile. Other databases, such as partner services, Medicaid, Ryan White HIV/AIDS Program services, and commercially available people-search databases, were useful for completing and updating contact information. Health departments found that communication with field staff members was key to identifying potential errors, assigning appropriate dispositions, and improving reports.
The Louisiana Department of Health implemented a promising D2C program that focused on identifying PWH who were not virally suppressed (ie, had virologic failure) and were in need of treatment adherence support services. Staff members had greater success contacting those PWH who were already in medical care than contacting PWH who were not in care. The program successfully provided services to PWH who had treatment adherence issues, which led to improvements in viral suppression for two-thirds of the PWH who were provided services. However, a large percentage of PWH contacted refused treatment adherence services. Some PWH refused services because they were switching medications or working with their physicians on adherence. The reasons for refusing adherence or linkage-to-care services should be further explored, because our data suggest that once PWH accept linkage and navigation services, they are typically linked to HIV medical care, and PWH who accept adherence support services may be more likely to reduce their viral load than PWH who refuse such services. Addressing unmet needs and barriers to care, such as transportation and housing, may be important to address before offering HIV medical care services. 24 -26 The small number of PWH who were offered but not yet provided linkage-to-care services suggests that linkage to care may be a long process for some PWH who have multiple needs.
Implementation challenges included staffing, providing timely linkage to services for PWH with multiple unmet needs, and navigating differences in the follow-up policies and procedures of facilities. Limitations in completeness of care status information in data systems also posed challenges to implementation. For example, 2 programs had difficulty in tracking the care status of PWH because data systems did not capture complete data on laboratory results or use of services. Staff member training; having dedicated D2C program staff members to bridge HIV prevention, care, and surveillance; and having other staff members assigned to data integration, cleaning, and quality assurance were important for implementation of D2C programs. Jurisdictions noted the benefits of having staff members in various positions (eg, disease intervention specialists, linkage personnel, case managers, and medical clinic staff members) working together. This collaboration resulted in better service delivery (eg, more timely referrals) and fostered better relationships between service providers and health department staff members.
Limitations
Our findings had several limitations. First, implementation practices varied across the 4 state health departments, which may have affected D2C program outcomes at each step of the D2C process. Each D2C program started at a different level of capacity in terms of staffing, resources, and data systems, and each program had unique implementation challenges, including data sharing, data system development, and prioritization of activities. In addition, the D2C program focusing on PWH with virologic failure who were in need of treatment adherence services was only implemented in one state. Therefore, differences in implementation could affect outcomes, and findings should be interpreted with caution. Second, data-reporting requirements were not set at the beginning of the project; as a result, data collection and categorization of investigation and linkage outcomes varied. Third, data included in this article did not include follow-up information for PWH who refused services or final outcomes for PWH who were not yet provided services by the end of the reporting period, which could affect interpretation of linkage and reengagement outcomes. Finally, delayed or incomplete reporting of laboratory information resulted in some PWH being initially categorized as not in care and later found to be in care. If they had been found to be in care sooner, these PWH would not have been included in the initial not-in-care lists. The availability and use of additional data sources for verification and cleaning varied by jurisdiction and may also have affected each program’s ability to update care status and other information in not-in-care lists.
Practice Implications
D2C is a proactive strategy that, when implemented as part of a comprehensive HIV prevention program, can help address disparities in access to HIV care, particularly among hard-to-reach communities that are underserved by health care systems. Future D2C programs should consider leveraging resources (eg, funding, relationships with care providers, information technology systems) and staff members to implement D2C programs. The D2C program provides important opportunities to work collaboratively with care providers and health care organizations to improve care outcomes. Care providers may benefit from obtaining viral suppression data on their patient population to gauge success of their patients’ care, as well as the linkage and reengagement assistance provided by health departments. In addition, D2C program activities may provide important opportunities to intervene when progress is stalled or viral suppression is not achieved or maintained. To be most efficient, D2C programs must improve data quality early in the process by integrating data-sharing and data-matching procedures to ensure current care status is known before generating not-in-care lists and contacting PWH. The number of deaths and the number of PWH in care revealed during these D2C program investigations suggest that surveillance programs need to assess the timeliness of current death ascertainment procedures and the completeness of laboratory reporting before implementing D2C programs.
D2C programs often required specific memoranda of understanding, data-sharing agreements, and supportive policies to conduct surveillance-based services. Agreements may be required between state and local health departments or within state health departments where care, prevention, and surveillance programs are not integrated. D2C programs should partner with correctional facilities to obtain data for matching purposes, because many incarcerated PWH appeared as not in care, and this population is not always eligible for follow-up. Asking PWH at the time of linkage if other services are needed, such as transportation or behavioral health support, and providing assistance in obtaining these services are likely to improve long-term retention in care.
CAPUS demonstrated progress toward national prevention goals by helping states improve health outcomes among PWH and laid important groundwork for data systems, protocols, and procedures for D2C programs. In particular, these lessons learned may be adapted by other health departments as they incorporate D2C program activities during the next 5 years as part of the flagship funding program to support HIV surveillance and prevention efforts under a new CDC funding opportunity announcement. 27 Programmatic and research efforts are underway to identify additional models for D2C program collaborative processes and data sharing through the CDC and HRSA co-led Partnerships for Care project, and evaluation of linkage-to-care interventions and their cost effectiveness in the Cooperative Re-Engagement Controlled Trial (CoRECT) will also assist health departments as they implement their D2C programs. 28,29 Our experience with CAPUS suggests that programs must address limitations in data systems to implement D2C programs efficiently. Additional research will be necessary to explore reasons for accepting or refusing services. Linking PWH to behavioral health and social services in addition to providing medical care may be important for PWH who face multiple barriers to care. Building on CAPUS, D2C program activities currently underway will further inform best practices. 27 -30
Footnotes
Acknowledgments
The authors acknowledge Kim Williams (Prevention Research Branch [PRB]/Centers for Disease Control and Prevention [CDC]) and the contributions of the following people to the implementation of Data to Care activities reported in this article: Catherine Adelakun, Andrea Danner, Fangchao Ma, Annie McGowan, Jeremy Thomas, Alvey Walbert, Zhi Wang, Cheryl Ward, and Mildred Williamson, Illinois Department of Health; Mary Boutte, Althea Fryson, DeAnn Gruber, Heather Horton, and Valerie Thomas-White, Louisiana Department of Health; Kayla Burgess, Veronica Calvin, David Fields, Sabrina Gandy, Gabrielle Hamilton, Dana Hughes, Jalesa Sutton, Kimberly Truss, and Carolyn Wester, Tennessee Department of Health; Patrice Armstrong, Shaunda Bonner, Jan Hill, Debbie Isby, and Rosalind Knight, Shelby County (Tennessee) Health Department; Rochelle Roberts, Davidson County (Tennessee) Health Department; Susan Carr, Bryan Collins, Fatima Elamin, Diana Jordan, Elaine Martin, and Amanda Saia, Virginia Department of Health, and the rest of the Virginia Department of Health CAPUS team; William Adih (HIV Incidence and Case Surveillance Branch [HICSB]/CDC), Stephanie Celestain (Prevention Program Branch [PPB]/CDC), Nicole Crepaz (HICSB/CDC), Frank Ebagua (Capacity Building Branch [CBB]/CDC), George Hill (PPB/CDC), William Jeffries IV (PRB/CDC), Raekiela Taylor (PRB/CDC), Kim Thierry-English (Substance Abuse and Mental Health Services Administration [SAMHSA]), and Candace Webb (HIV/AIDS Bureau [HAB]/Health Resources and Services Administration [HRSA]) from the CAPUS Federal Site Team in Illinois; William Bryant (HAB/HRSA), Ted Duncan (CBB/CDC), Kirk James (SAMHSA), Laura Kearns (PPB/CDC), Alexandra Oster (HICSB/CDC), Thomas Painter (PRB/CDC), and Lamont Scales (Office of Health Equity [OHE]/Division of HIV/AIDS Prevention [DHAP]/CDC) from the CAPUS Federal Site Team in Louisiana; Jonny Andia (CBB/CDC), Dwayne Banks (PPB/CDC), Wendy Briscoe (HAB/HRSA), Stacy Cohen (HICSB/CDC), Kristen Hess (HICSB/CDC), Cynthia Prather (PRB/CDC), Kim Thierry-English (SAMHSA), and Cheryl Williams (HICSB/CDC) from the CAPUS Federal Site Team in Tennessee; and Kim Brown (HAB/HRSA), Emilio German (OHE/DHAP/CDC), Kirk Henny (PRB/CDC), Laura Kearns (PPB/CDC), Benjamin Laffoon (HICSB/CDC), Ilze Ruditis (SAMHSA), Pilgrim Spikes (PRB/CDC), and David Whittier (CBB/CDC) from the CAPUS Federal Site Team in Virginia.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Care and Prevention in the United States (CAPUS) Demonstration Project was supported by the US Department of Health and Human Services Secretary’s Minority AIDS Initiative Fund and led by CDC (PS12-1210). The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of CDC.