
Abstract
Objectives:
Social determinants of health (SDHs) are the complex, structural, and societal factors that are responsible for most health inequities. Since 2003, the National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention (NCHHSTP) has researched how SDHs place communities at risk for communicable diseases and poor adolescent health. We described the frequency and types of SDHs discussed in articles authored by NCHHSTP.
Methods:
We used the MEDLINE/PubMed search engine to systematically review the frequency and type of SDHs that appeared in peer-reviewed publications available in PubMed from January 1, 2009, through December 31, 2014, with a NCHHSTP affiliation. We chose search terms to identify articles with a focus on the following SDH categories: income and employment, housing and homelessness, education and schooling, stigma or discrimination, social or community context, health and health care, and neighborhood or built environment. We classified articles based on the depth of topic coverage as “substantial” (ie, one of ≤3 foci of the article) or “minimal” (ie, one of ≥4 foci of the article).
Results:
Of 862 articles authored by NCHHSTP, 366 (42%) addressed the SDH factors of interest. Some articles addressed >1 SDH factor (366 articles appeared 568 times across the 7 categories examined), and we examined them for each category that they addressed. Most articles that addressed SDHs (449/568 articles; 79%) had a minimal SDH focus. SDH categories that were most represented in the literature were health and health care (190/568 articles; 33%) and education and schooling (118/568 articles; 21%).
Conclusions:
This assessment serves as a baseline measurement of inclusion of SDH topics from NCHHSTP authors in the literature and creates a methodology that can be used in future assessments of this topic.
There are social conditions that predispose particular populations to diseases via “the conditions in which people are born, grow, work, live, and age,” as well as “the wider set of forces and systems shaping the conditions of daily life.” 1 –4 These social conditions result in disparities in health care access, educational achievement, and economic status that influence the health of populations. For example, people of low socioeconomic status are often less likely than those of higher socioeconomic status to adhere to HIV medication regimens. This lack of adherence may be caused by difficulties in maintaining medical appointments (due to lack of transportation and inflexible work schedules) and an inability to pay for prescriptions. Social factors that cause health disparities are generally referred to as social determinants of health (SDHs). 5 –7 Increasingly, in the past 30 years, public health researchers have examined SDHs and their impact on health outcomes. 8 –14 SDHs are included among the goals of Healthy People 2020 (HP2020). HP2020 uses the following categories to conceptualize how SDHs affect health: economic stability, education, social or community context, health and health care, and neighborhood or built environment. 15 In 2003, the National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention (NCHHSTP) at the Centers for Disease Control and Prevention (CDC) established an Office of Health Disparity to consider how SDHs put particular communities at risk for HIV/AIDS, viral hepatitis, sexually transmitted diseases (STDs), tuberculosis (TB), and poor adolescent health. 16,17
To understand the drivers of health disparities and the persistence of diseases among people in certain racial/ethnic minority groups and those of low socioeconomic status, NCHHSTP held external consultations and promoted policy and research investigations of the impact of SDHs. 18 –20 These efforts culminated in the NCHHSTP’s strategic plan (2010-2015), a document that emphasized SDHs and the reduction of health disparities as a top priority. 21 To establish a baseline toward achievement of this priority, we systematically measured the types of SDHs discussed in the peer-reviewed literature available in PubMed with an NCHHSTP affiliation and how frequently these SDHs were discussed.
Methods
We used the MEDLINE database of biomedical and life science references through PubMed to systematically identify articles of interest. We identified all eligible articles in PubMed by using the following search criteria: (1) published in English; (2) published during January 1, 2009–December 31, 2014; and (3) included an author whose affiliation was listed as NCHHSTP (Box). The dates were chosen to correlate with the development and release of the NCHHSTP strategic plan for 2010-2015 that highlighted the importance of SDHs. We included articles that named one of the NCHHSTP divisions in the author’s affiliation. In articles that had 2 or more NCHHSTP authors from multiple CDC centers or divisions, we attributed the article to the division of the highest-ranked author. Search terms included the divisions within NCHHSTP: Division of Adolescent and School Health, Division of HIV/AIDS Prevention, Division of STD Prevention, Division of Tuberculosis Elimination, and Division of Viral Hepatitis. If an article listed only a center affiliation, we attributed the article to the division of the first-listed author. Articles authored by people in the Program Collaboration and Service Integration effort (a program that was designed to integrate interrelated health issues, activities, and prevention strategies to facilitate comprehensive delivery of services among diseases of the center) or by people in offices of the Associate Director of Health Equity were attributed to the Office of the Director.
PubMed search terms used in a 2-stage search process to (1) identify articles authored by the National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention (NCHHSTP) and (2) identify articles with a focus on the social determinants of health, January 2009 through December 2014.
((((“centers for disease control and prevention”[Affiliation])) AND (“2009/01/01”[Date - Create]: “2014/12/31”[Date - Create]))) AND (“Division of Adolescent and School Health”)
((((“centers for disease control and prevention”[Affiliation])) AND (“2009/01/01”[Date - Create]: “2014/12/31”[Date - Create]))) AND “Division of Tuberculosis Elimination”)
((((“centers for disease control and prevention”[Affiliation])) AND (“2009/01/01”[Date - Create]: “2014/12/31”[Date - Create]))) AND “Division of HIV/AIDS Prevention”)
((((“centers for disease control and prevention”) AND (“2009/01/01”[Date - Create]: “2014/12/31”[Date - Create]))) AND “Division of STD Prevention”)
((((“centers for disease control and prevention”[Affiliation])) AND (“2009/01/01”[Date - Create]: “2014/12/31”[Date - Create])) AND “Division of Viral Hepatitis”)
(((((((National Center for HIV/AIDS, Hepatitis, STD and TB Prevention) AND (“2009/01/01”[Date - Create]: “2014/12/31”[Date - Create])))) NOT (“Division of STD Prevention”[Affiliation] OR “Division of Viral Hepatitis”[Affiliation] OR “Division of Tuberculosis Elimination”[Affiliation] OR “Division of HIV/AIDS Prevention”[Affiliation] OR “Division of Adolescent and School Health”[Affiliation]))))
AND ((“poverty”[MeSH Terms] OR “poverty”[All Fields]) OR (“income”[MeSH Terms] OR “income”[All Fields]) OR deprivation[All Fields] OR (“health resources”[MeSH Terms] OR (“health”[All Fields] AND “resources”[All Fields]) OR “health resources”[All Fields] OR “resources”[All Fields]) OR “wealth” [All Fields] OR (material[All Fields] AND “resources”[All Fields] OR “material resources”[All Fields]) OR “wages”[All Fields] OR (“Salary”[All Fields] OR “employment”[All Fields] OR “unemployment”[All Fields]))
AND (house[All Fields] OR home[All Fields] OR (“homeless persons”[MeSH Terms] OR (“homeless”[All Fields] AND “persons”[All Fields]) OR “homeless persons”[All Fields] OR “homeless”[All Fields]) OR (“housing”[MeSH Terms] OR “housing”[All Fields] OR “residence characteristics”[MeSH Terms] OR (“residence”[All Fields] AND “characteristics”[All Fields]) OR “residence characteristics”[All Fields] OR “foreclosure”[All Fields] OR “home ownership”[All Fields]))
AND ((“schools”[MeSH Terms] OR “schools”[All Fields] OR “school”[All Fields]) OR (“education”[Subheading] OR “education”[All Fields])
AND (“Stigma”[All Fields] OR “discrimination”[All Fields] OR “segregation”[All Fields] OR “prejudice”[All Fields] OR “prejudice”[MeSH Terms] OR “racism”[All Fields] OR “racism”[MeSH Terms] OR “homophobia”[All Fields])
AND (“social context”[All Fields] OR “community”[All Fields] OR “cohesion”[All Fields] OR “participation”[All Fields] OR “neighborhood”[All Fields] OR “neighbor”[All Fields] OR “incarceration”[All Fields] OR “jail”[All Fields] OR “institutionalized”[All Fields] OR “prisons”[All Fields] OR “prisons”[MeSH Terms]))
AND (“health services”[MeSH Terms] OR (“health”[All Fields] AND “services”[All Fields]) OR “health services”[All Fields]) OR (“primary health care”[MeSH Terms] OR (“primary”[All Fields] AND “health”[All Fields] AND “care”[All Fields]) OR “primary health care”[All Fields] OR (“primary”[All Fields] AND “care”[All Fields]) OR “primary care”[All Fields]) OR (“Health Services Accessibility”[All Fields] OR “Health Services Accessibility”[MeSH Terms]) OR “Outpatient Clinics, Hospital”[MeSH] OR “Outpatient Clinics, Hospital”[All Fields] OR (“Ambulatory Care Facilities”[Mesh] AND “Ambulatory Care Facilities”[All Fields]) OR “outpatient”[All Fields] OR “inpatient”[all fields] OR “Appointments and Schedules”[MeSH Terms] OR “Appointments and Schedules”[All Fields] OR (“appointments”[All Fields] AND “schedules”[All Fields]) OR “appointments”[All Fields] OR “schedule”[All Fields]
AND (“neighborhood”[All Fields]) OR “catchment area” OR “block”[All Fields] OR “town”[All Fields] OR (“cities”[MeSH Terms] OR “cities”[All Fields] OR “city”[All Fields]) OR (“censuses”[MeSH Terms] OR “censuses”[All Fields] OR “census”[All Fields]) AND “tract”[All Fields] OR (“environment”[MeSH Terms] OR “environment”[All Fields]) OR (“crime”[MeSH Terms] OR “crime”[All Fields]) OR (“violence”[MeSH Terms] OR “violence”[All Fields]) OR “urban”[All Fields] OR “rural”[All Fields] OR “zoning”[All Fields])
We further subdivided several of the original HP2020 categories to create 7 total categories of SDHs, as opposed to the 5 given in HP2020. 15 We made the decision to use 7 categories a priori based on our knowledge of NCHHSTP research and SDH factors that were likely to be associated with particular diseases or divisions. We examined 7 categories of SDHs in this systematic review: income and employment, housing and homelessness, education and schooling, stigma or discrimination, social or community context, health and health care, and neighborhood or built environment. After we identified eligible articles, we searched the article titles and abstracts again in PubMed by using SDH-specific terms that correlated to these 7 categories (Table 1). We included articles in an SDH category if we identified them via PubMed title and abstract search using the terms related to each SDH category (Box).
Categories of social determinants of health used in Healthy People 2020 and categories used in a review of articles authored by NCHHSTP in the peer-reviewed literaturea
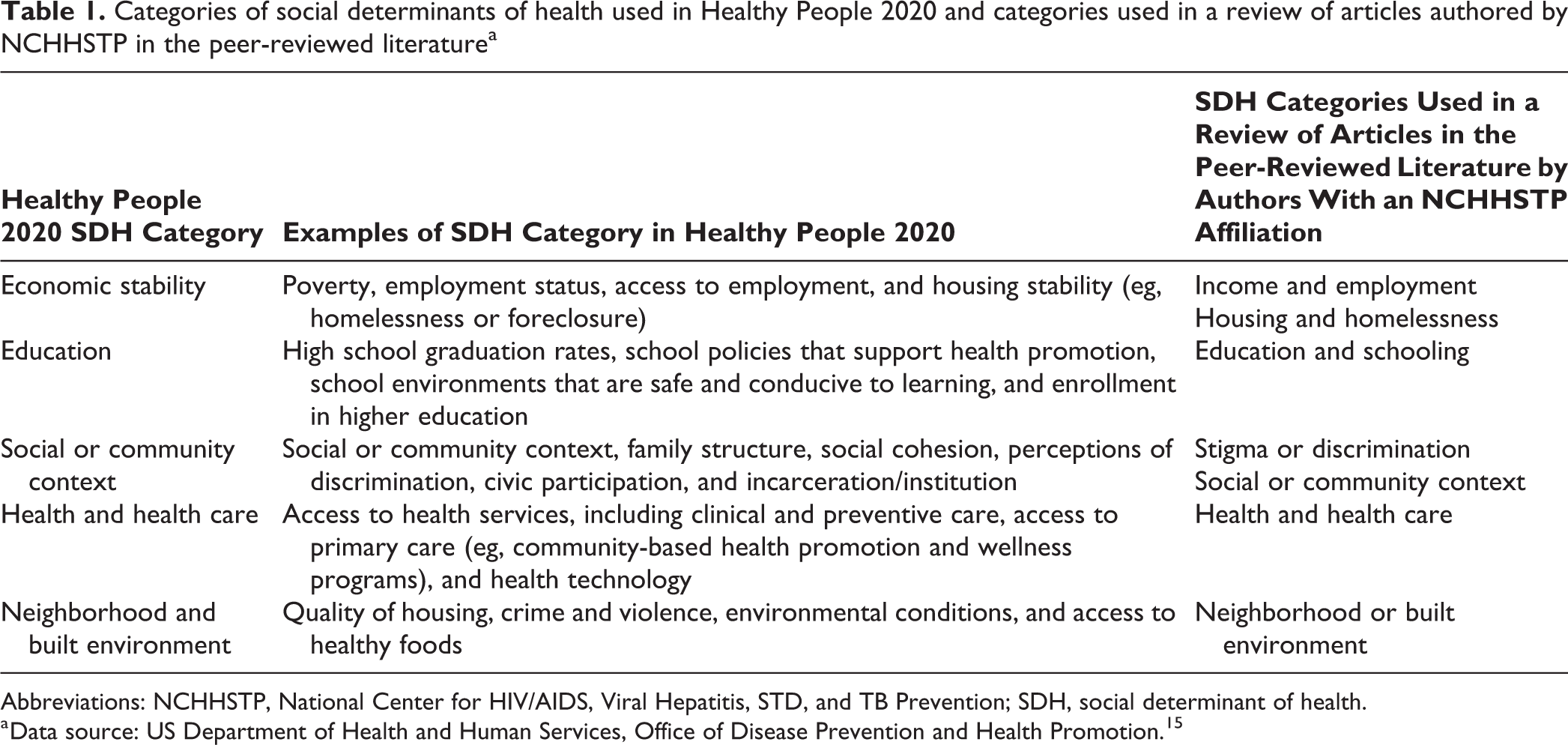
Abbreviations: NCHHSTP, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention; SDH, social determinant of health.
a Data source: US Department of Health and Human Services, Office of Disease Prevention and Health Promotion. 15
We retrieved full-text articles identified by using the SDH search terms and assessed them to ensure that (1) all articles met the eligibility criteria, (2) the content of articles addressed diseases or affiliated health conditions covered by NCHHSTP (eg, HIV/AIDS, STDs, TB, adolescent health, and viral hepatitis), and (3) the articles discussed SDHs. We reviewed each article for each SDH category with which it was identified. We excluded from further analysis articles that were identified via PubMed using SDH search terms but that did not discuss the relevant SDH. To ensure consistency in inclusion or exclusion of identified articles, we searched full-text articles by using Adobe XI Reader (version 11.0.12, Adobe Systems Incorporated) for the same terms used in PubMed.
If an article did address the SDH categories of interest, we described it as having either a “substantial” focus or a “minimal” focus on the SDH category. We classified an article as having a substantial SDH focus if the SDH factor was 1 of 3 or fewer foci of the article. We classified the article as having a minimal SDH focus if the SDH topic was mentioned briefly in the introduction or discussion or was examined as part of 4 or more foci of the article.
Although the HP2020 framework creates separate SDH categories, it is not uncommon for people in a particular population group or area to be disadvantaged in multiple ways. For example, people living in rural areas may be poor and lack medical services. 22,23 Given that many SDHs are interrelated, we included articles in every SDH category in which they were identified. This methodology resulted in some articles being counted multiple times. One author (EEF) reviewed and classified articles into minimal or substantial categories.
Results
We identified 868 articles as having authors with an NCHHSTP affiliation in the MEDLINE database with publication dates from January 1, 2009, through December 31, 2014. Six articles had authors from multiple divisions within NCHHSTP and were assigned to a single division or the Office of the Director based on the first-listed NCHHSTP author’s affiliation, resulting in a total of 862 unique articles. By using the search terms created for each SDH category, we identified 547 unique articles. We identified some articles in more than one SDH category, resulting in these 547 articles appearing 777 times across all SDH categories (Figure). We excluded the other 315 unique articles from further analysis because no SDH-specific search terms appeared in the title and abstract review.
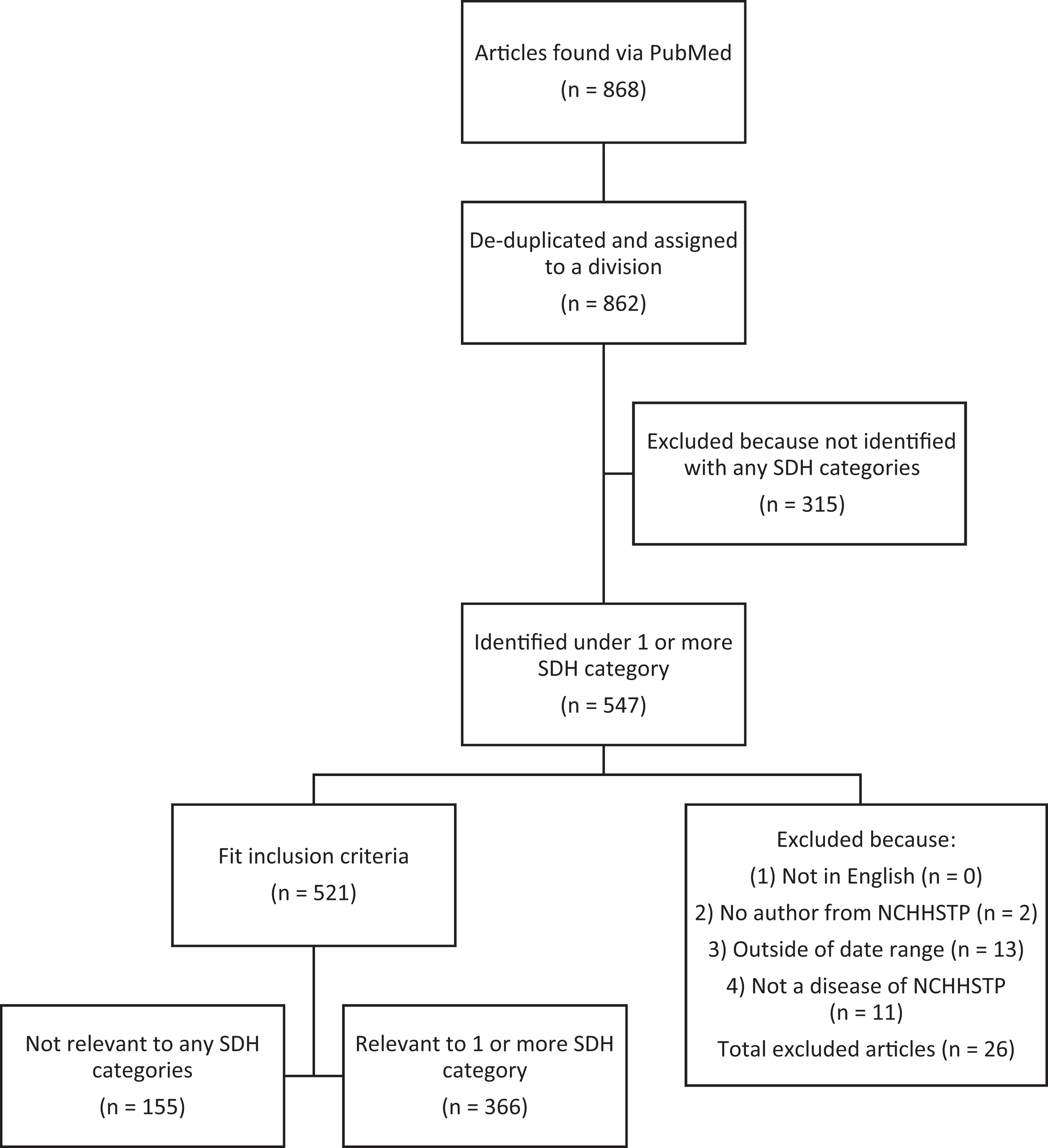
Flowchart of articles with a National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention (NCHHSTP) affiliation that address the social determinants of health (SDHs) in the peer-reviewed literature, United States, 2009-2014. Articles had to address 1 of 7 Healthy People 2020 15 categories: income and employment, housing and homelessness, education and schooling, stigma or discrimination, social or community context, health and health care, and neighborhood or built environment. Articles could appear in more than 1 SDH category. Numbers refer to the number of unique articles located.
Upon full-text review, 155 articles identified by using SDH search terms did not discuss SDHs. We excluded these articles from further analysis, leaving 366 unique articles, which appeared 568 times across all SDH categories.
The search terms that identified the most articles were those for the SDH categories of health and health care (190/568 articles; 33%) and education and schooling (118/568 articles; 21%). The Division of Adolescent and School Health was the NCHHSTP division that was most closely associated with a particular SDH category: 49 of 52 (94%) published articles focused on education and schooling were authored by someone from the Division of Adolescent and School Health (Table 2). Across all SDH categories, 449 of 568 (79%) relevant articles only briefly discussed the SDH topic and were therefore classified as having a minimal SDH focus.
Frequencya of social determinants of health categories by affiliation of author within NCHHSTP, in a systematic review of the peer-reviewed literature in PubMed, United States, 2009-2014b
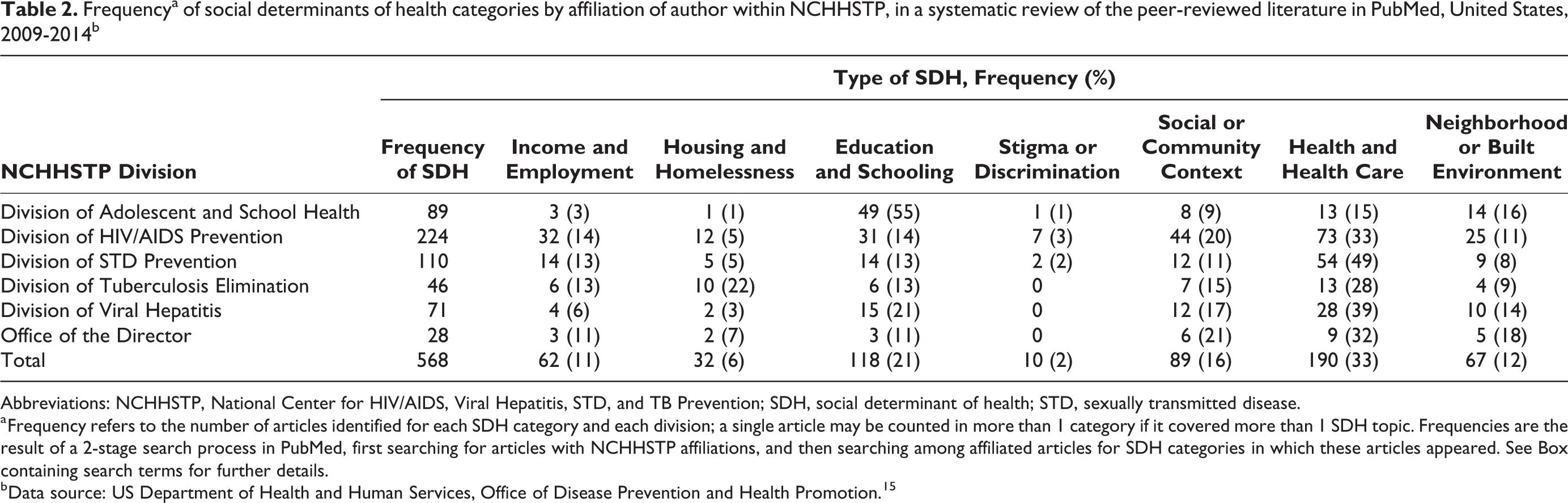
Abbreviations: NCHHSTP, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention; SDH, social determinant of health; STD, sexually transmitted disease.
a Frequency refers to the number of articles identified for each SDH category and each division; a single article may be counted in more than 1 category if it covered more than 1 SDH topic. Frequencies are the result of a 2-stage search process in PubMed, first searching for articles with NCHHSTP affiliations, and then searching among affiliated articles for SDH categories in which these articles appeared. See Box containing search terms for further details.
b Data source: US Department of Health and Human Services, Office of Disease Prevention and Health Promotion. 15
Income and Employment
Of the 62 articles that discussed income and employment, 56 (90%) had a minimal SDH focus 17,24 –78 and 6 (10%) had a substantial SDH focus. 79 –84 The identified articles focused on income in various ways, including as a personal median or annual income, being above or below the income threshold for the federal poverty level, household income level, and proportion of households below the federal poverty level in a community. Most articles reported employment as individual employment or unemployment or as the proportion of people unemployed in a community.
Housing and Homelessness
Of the 32 articles that discussed housing or homelessness, 25 (78%) had a minimal focus 33,45,63,68,73,78,85 –103 and 7 (22%) had a substantial focus. 44,79,81,104 –107 Articles measured and discussed housing and homelessness in several ways depending on the NCHHSTP division and contents of the identified articles, including if participants were currently marginally housed, had been homeless in the past year, or had a parent in the home. Other discussions of housing included in-home testing for STDs or HIV, households used as the unit of randomization in clinical trials, and the housing vacancy proportion in a census tract.
Education and Schooling
We identified 118 articles in the SDH category of education and schooling. Of the 118 articles, we classified 81 (69%) as having a minimal SDH focus 24 –26,28,32,33,35,36,38,40,42,45,49,50,59,61,70,73,74,85,108 –168 and 37 articles as having a substantial focus on education and schooling, including those that used schools or education levels as a major variable in analysis, examined school-based health interventions, described health programs and policies at school, discussed health training for educators, or discussed in-depth school-based activities (eg, physical education class). 37,44,81,169 –202 Articles discussed and measured education and school-related factors in various ways, including the level of parental education, level of participant education, activities at school, proportion with a high school degree in a community or census tract, design and use of health education campaigns, and health interventions conducted in school settings.
Stigma or Discrimination
We identified 10 articles that addressed stigma or discrimination, 6 of which had a minimal SDH focus. 39,49,94,203 –205 The 4 articles that had a substantial SDH focus were evenly distributed between those that discussed stigma and those that discussed discrimination. 29,88,115,206 Seven articles discussed stigma related to HIV/AIDS, TB, or STDs, in particular stigma associated with testing and treating disease. Three articles discussed racism, segregation, or racial discrimination. 29,39,115
Social or Community Context
We identified 89 articles that addressed social or community context. We included search terms related to jails, prisons, and incarceration in this category, and many articles discussed issues related to incarceration. Most articles (64/89; 72%) covered factors related to the social or community context at minimal depth. 28,38,39,44,50,51,61,74,78,84,89,96,101,110,111,117,119,126,127,141,148,149,151,152,158,159,164,168,175,180,189,192,197,198,204,207 –235 The 25 articles with a substantial focus on social or community context included those that focused on testing for disease (eg, HIV, STDs) in communities, prevention campaigns or interventions designed for communities or incarcerated populations, and community-level associations. 43,45,52,53,87,88,94,106,139,193,236 –250 Articles discussing social or community context included those that discussed geographic communities, larger communities composed of racial/ethnic minority groups, and community-based health care organizations. Few articles discussed the importance of social support or group membership (eg, church or social organizations).
Health and Health Care
We identified 190 articles on health and health care, most of which had a minimal SDH focus (162/190; 85%). 26,28,42,47,52 –54,56,59,64,73,82,84,86,91,93,102,106,116,117,127,128,139,141,144,147,148,151 –153,160 –162,164,165,167,169,172,174,175,179,183,186,187,192,197,198,202 –204,213,217 –219,226,229,233,235,236,243 –245,247 –249,251 –347
The 28 articles that had a substantial SDH focus included those that discussed in-depth health care provision, health care disparities, delays or refusal to enter into care, retaining patients in care, and health care costs. 31,50,57,74,105,107,124,146,170,208,214,215,223,348 –362 The identified articles addressed health and health care in 2 main ways: (1) the use of health care services and/or health care-seeking behaviors and (2) health care access and affordability or health care provision. Additional topics included disease transmission in health care settings and health care workers as an at-risk group.
Neighborhood or Built Environment
The category of neighborhood or built environment included search terms related to violence and crime. Of 67 articles identified as having a focus on neighborhood or built environment, 50 (75%) had a minimal focus 17,39,73,84,89,103,105,109,114,116 –118,120,127,132,147,171,173,178,179,198,200,203,219,243,252,267,328,341,345,347,356,363 –380 and 17 (25%) had a substantial focus. 45,81–83,104,119,184,228,359,381 –388 In general, articles addressed the neighborhood and/or the built environment in 1 of 3 ways: as violence (especially intimate partner violence), geography (census tracts, multistate areas, regional areas), or urbanicity (the degree to which an area was urban, rural, or suburban).
Discussion
This systematic review is the first to examine the number of articles on SDHs incorporated into research to provide a baseline quantifiable mechanism for determining improvement in SDH research and reducing health disparities. This assessment measured the frequency and depth of articles discussing SDH among authors with an NCHHSTP affiliation, and created a methodology that can be used in future assessments of SDHs in peer-reviewed publications. Most of the identified articles in this systematic review had a minimal focus on SDHs. The lack of articles with a substantial SDH focus is of interest given the importance of SDHs to HIV/AIDS, STDs, TB, and viral hepatitis disease acquisition, treatment, morbidity, and mortality, 389 –393 as well as the prioritization of health equity and SDHs in the NCHHSTP’s strategic plan (2010-2015). Because the Patient Protection and Affordable Care Act, the subprime mortgage crisis, and US economic recession dominated public and scientific discourse during 2009-2014, 394,395 we anticipated that more articles would have an upstream focus on policy areas such as income and employment or housing and homelessness. The lack of articles with a substantial focus on these topics may represent a missed opportunity for in-depth publication of the effects of these social circumstances on diseases of interest to NCHHSTP.
Even in the most well-represented category, health and health care, fewer than 25% of the articles had a substantial focus on SDHs. This lack of substantial focus may be due to our examination of only the peer-reviewed scientific literature produced by NCHHSTP, rather than including SDH concepts in all of NCHHSTP’s work. In this review, we found that most articles identified via PubMed that discussed health and health care focused on routine disease prevention and clinical activities (surveillance, outbreak investigation, and testing or treatment of disease). Research into patient and community SDHs could inform these efforts by identifying factors associated with disease outbreaks and persistence, as well as barriers to implementation and success of disease-fighting programs.
Although each SDH category in this assessment included multiple related factors, such as income and employment, one factor in an SDH category often was covered more extensively than others. For example, in the SDH category stigma or discrimination, articles overwhelmingly focused on stigma (particularly testing or treatment of stigma associated with HIV/AIDS or STDs), with limited focus on discrimination, homophobia, racism, or xenophobia, all of which can increase stigma and disease transmission. 396,397 Although the focus on disease-related stigma is important, it is an incomplete representation of the factors that permit and drive health disparities in these diseases.
Limitations
This systematic review had several limitations. First, although we created a comprehensive list of search terms in an effort to cover all components of each SDH category, important components may have been omitted. Second, we examined only articles that were published during 2009-2014 in peer-reviewed journals contained in the MEDLINE database. It is impossible to predict whether the articles not included (eg, internal reports or those in non–peer-reviewed journals) would have contained more articles on SDH topics. Third, reviewer bias in classifying SDH categories during content analysis was possible. Although we checked articles multiple times to confirm categorization as minimal or substantial in focus, a single reviewer made these determinations, which may have resulted in nondifferential misclassification. Fourth, we classified each article as having a minimal or substantial focus based on the depth of discussion within each SDH category under which it was identified rather than based on the overall number of SDHs that were discussed in the article. Had we used a different assessment method, some articles classified as minimal might have been considered substantial. Fifth, this review did not qualify the type of SDH information or discussion beyond categorization of minimal and substantial. We did not assess the translation of substantial or minimal discussion into policy, research, or program interventions in this study. Future work should examine the extent to which the SDH information included in NCHHSTP articles is actionable or contributes to the formation of policy. An examination of actionable SDH information from NCHHSTP articles might be quantified by conducting a review of guidance or policy documents or grantee reports generated after publication of the peer-reviewed article. Finally, both the total number of articles identified and the number of articles identified for each SDH category were likely an underestimate of the actual number of published articles produced by each NCHHSTP division, because certain journals allow only the highest organizational unit (ie, CDC) as the affiliation. Our review included only those articles that listed the center (NCHHSTP) or division affiliation in PubMed.
Conclusions
Knowing the importance of SDHs to the health outcomes of NCHHSTP, we encourage public health departments and other health agencies to allocate resources and time to the topic areas we identified as minimally covered in this analysis. These systematic search methods can serve as a model for other public health agencies that wish to assess the content of their published SDH research.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication was supported by cooperative agreement number U36/CCU300430 from the Centers for Disease Control and Prevention (CDC) and the Association of Schools and Programs of Public Health (ASPPH). The findings and conclusions of this publication are those of the authors and do not necessarily represent the official position of CDC or ASPPH.