
Abstract
Physical inactivity among children is a public health problem associated with low levels of fitness, obesity, and increased risk of chronic diseases. Public health experts have identified policies targeting physical activity as a promising strategy to address this challenge. Understanding the process by which such policies are adopted may help to facilitate progress nationally. To examine lessons learned from the passage of the Student Health and Physical Education Act in Georgia, we conducted 15 interviews with people engaged in the adoption of the act. We found that several factors were vital to policy adoption: a shifting social and political climate, the organization and mobilization of diverse partners behind a common agenda, and the development of strategies to overcome impediments to legislative progress. These findings suggest that engagement and cooperation with partners, establishment of mutual interests as a basis for collaboration, and grassroots outreach and advocacy can facilitate adoption of policies that promote physical activity.
The consequences of physical inactivity and low fitness levels are well documented. 1 Low levels of fitness among children are associated with higher rates of obesity and a greater risk for chronic diseases, whereas regular physical activity and high fitness levels are associated with a reduced risk of developing chronic diseases. 2 Evidence suggests that 60 minutes of daily moderate-to-vigorous physical activity promotes healthy weight and minimizes the risk for obesity, cardiovascular diseases, and diabetes. 2,3 Approximately half of all children in Georgia are not meeting the recommendations for daily physical activity. 4 In 2011, 30.6% of children and adolescents in Georgia aged 6-17 participated in vigorous physical activity every day, 5 and in 2013, 33.6% of high school students participated in daily physical education in school. 4
Experts have identified policies targeting physical activity in schools as a promising strategy for childhood obesity prevention. 6 In response, states have emphasized policies that increase physical activity in schools. In 2009, Georgia’s General Assembly adopted House Bill 229, also known as the Student Health and Physical Education (SHAPE) Act. 7 The SHAPE Act requires annual fitness assessments for public school students in grades 1 through 12 who are enrolled in a physical education course taught by a certified physical education teacher and requires school systems to provide the minimum requirements for physical education as prescribed by the Georgia State Board of Education. 7,8
The policy-making process is complex and not well documented by public health researchers. 9 Understanding the process by which physical activity policies are adopted may help to facilitate progress on childhood obesity prevention in other states. The purpose of this study was to use key informant interviews to understand the context and strategies that led to the passage of the SHAPE Act by synthesizing the experiences of multiple stakeholders and identifying lessons learned.
Methods
Sample and Design
We conducted key informant interviews to understand the context surrounding passage of the SHAPE Act. We identified participants through purposive sampling, a technique that targets people who are knowledgeable about the study topic, 10 and included people who played a key role in the development, advocacy, or passage of the SHAPE Act.
Of 21 key informants who were invited to participate, 15 participated in the study. During 2014-2015, we conducted 13 interviews in person and 2 by telephone. Participants represented sectors that played a key role in the development, advocacy, and passage of the SHAPE Act, including state legislature (n = 1), public health (n = 4), academia (n = 4), state government (n = 1), and nonprofit organizations (n = 5). Interviews focused on the 6 years leading up to passage of the SHAPE Act (2004-2009), which was the approximate time period in which organized advocacy efforts took place in the state.
Procedures
We conducted 60-minute, semi-structured interviews to allow for exploration of salient factors related to the SHAPE Act. The interview guide contained 23 open-ended questions and assessed 5 factors: (1) the social and political environment, (2) childhood obesity prevention activities occurring statewide, (3) influential community leaders and champions (appointed and informal) involved in the passage of the SHAPE Act, (4) challenges and barriers, and (5) strategies to facilitate progress (Box). The Georgia State University Institutional Review Board approved this study.
Georgia State University School of Public Health interview guide to understand the context surrounding passage of the SHAPE Act,7 key informant interviews, Georgia, 2014-2015a
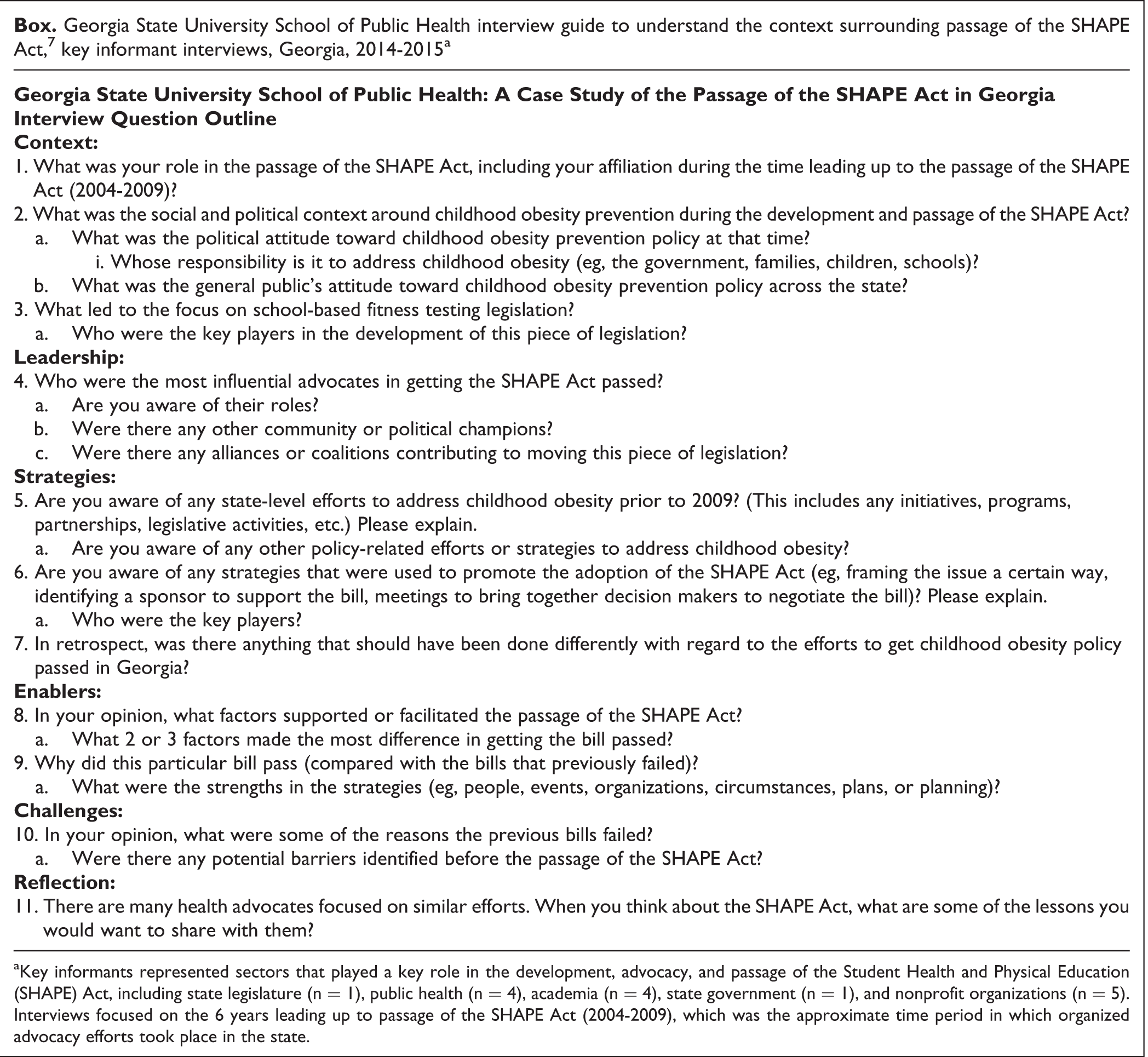
aKey informants represented sectors that played a key role in the development, advocacy, and passage of the Student Health and Physical Education (SHAPE) Act, including state legislature (n = 1), public health (n = 4), academia (n = 4), state government (n = 1), and nonprofit organizations (n = 5). Interviews focused on the 6 years leading up to passage of the SHAPE Act (2004-2009), which was the approximate time period in which organized advocacy efforts took place in the state.
Analysis
Interviews were audio-recorded, transcribed, and analyzed using NVivo10. 11 We used thematic analysis to code interviews and identify common themes. Two coders began the coding process by developing a coding framework informed by the interview guide, and 2 trained researchers independently coded the interview transcripts. The 2 coders reached consensus on the assignment of codes, and we abstracted and categorized codes according to emergent themes. We consolidated similar categories into 3 main themes. The results presented here reflect these themes and are supported by quotes from study participants.
Outcomes
Study participants described a variety of social and political challenges that hindered the passage of legislation for childhood obesity prevention and the strategies that were implemented to increase awareness of the problem and garner support from key stakeholders. Outcomes are organized under 3 prominent themes that emerged from the interviews: (1) challenging social and political climate, (2) organizing and mobilizing key stakeholders, and (3) strategic action to promote policy.
Theme 1: Challenging Social and Political Climate
In reflecting on the social and political climate, respondents reported that progress was initially challenging because policy makers were not receptive to government taking a leading role in prevention efforts. In 2004, the release of national reports highlighting Georgia’s high obesity rates served as an impetus for state-level efforts. 12 One respondent stated, “We looked at F as in Fat [Trust for America’s Health report 12 ] and some of the data that [were] coming out nationally, and folks started to see Georgia being at the very, very bottom. So that kind of encouraged some movement.” According to participants, these reports served as a “wake-up call to leaders about obesity in Georgia” and helped get “some dialogue started about what to do.”
Policy and advocacy efforts emerged in 2005 with the introduction and failure of 3 bills focused on childhood obesity prevention in schools (Table). In 2005, House Bill 497 (HB497)
13
was dubbed the “Fat Bill” and, as stated by multiple participants, generated considerable opposition because policy makers rejected the idea that schools should measure children’s body mass index (BMI). Some respondents reported that the House Education Committee felt “blindsided,” found the bill “intrusive and stigmatizing,” and felt it represented “government overstep.” According to 1 participant, Legislatively, it was very tough. You’re talking about a climate that was predominantly far-right Republicans, and they were all about reducing government interference in people’s lives.…And we had a lot of these folks [who] were pushing from that perspective—that they didn’t want to force this issue down people’s throats, and it wasn’t the schools’ business to be taking BMI measurements.
Timeline of childhood obesity policy and legislative activities in Georgia, 2004-2009a
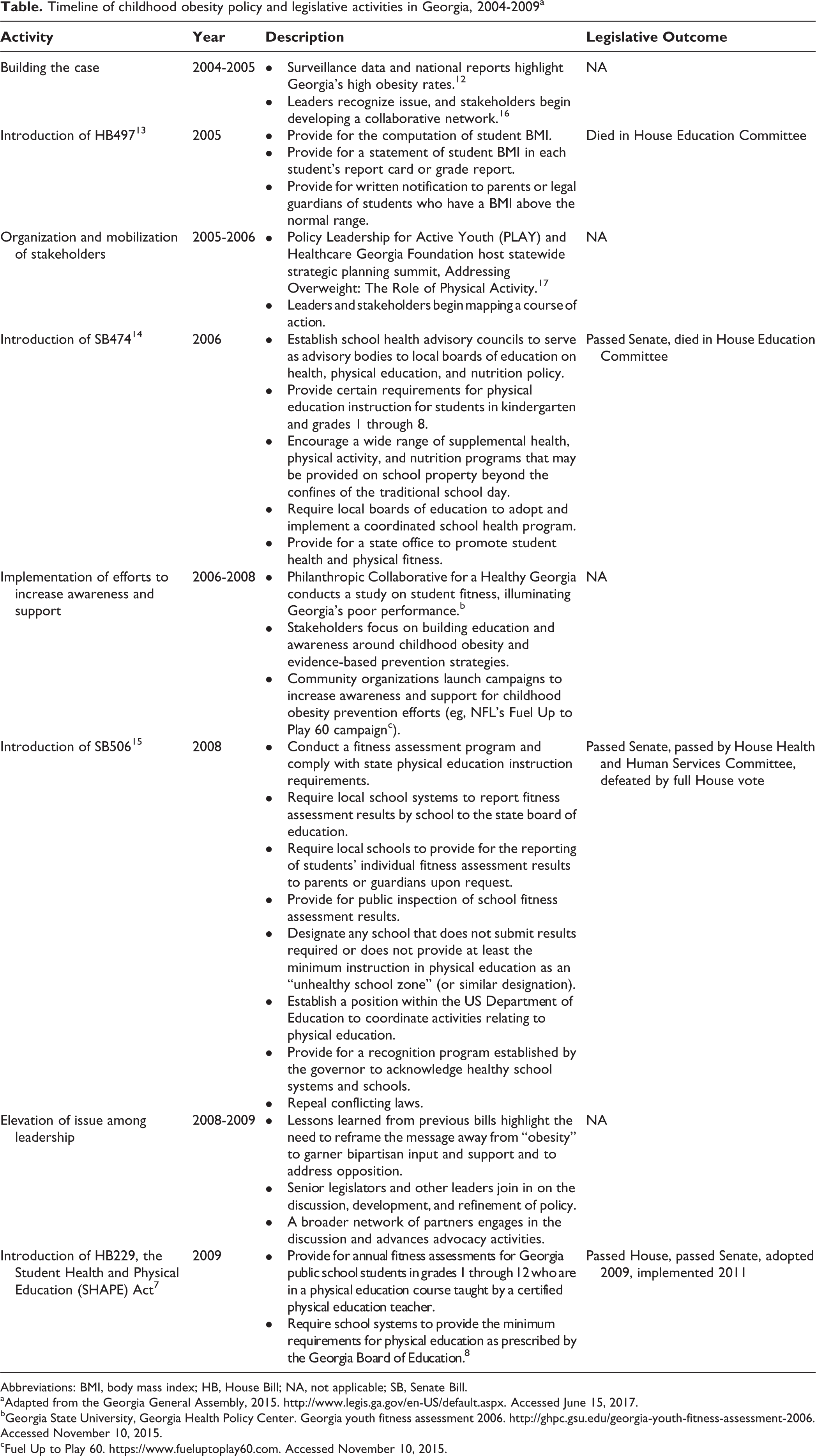
Abbreviations: BMI, body mass index; HB, House Bill; NA, not applicable; SB, Senate Bill.
aAdapted from the Georgia General Assembly, 2015. http://www.legis.ga.gov/en-US/default.aspx. Accessed June 15, 2017.
bGeorgia State University, Georgia Health Policy Center. Georgia youth fitness assessment 2006. http://ghpc.gsu.edu/georgia-youth-fitness-assessment-2006. Accessed November 10, 2015.
cFuel Up to Play 60. https://www.fueluptoplay60.com. Accessed November 10, 2015.
Subsequently, 2 more bills were introduced and rejected: Senate Bill 47414 and Senate Bill 506. 15 Most respondents believed that unaddressed opposition generated from HB497 led to the failure of these bills. These failures exposed the importance of “bipartisan support” and the “need for widespread support and an influential political champion” in passing legislation.
Participants suggested that these early efforts led to increased awareness of childhood obesity among policy makers and the potential role policy could play in prevention. “Many stakeholders invested a great deal of resources to educate the public and our leaders,” explained a respondent. These early legislative failures helped tailor strategies to the prevailing advocacy climate. One respondent stated, We were able to build off of the things that we learned from [House Bill] 497 and [Senate Bills] 474 and 506 and pull that together. I would say there were some things that we knew we could do better. We capitalized on the knowledge that we had from those failures, and we put it all together; and that’s why we had the success that was [the SHAPE Act].
Theme 2: Organizing and Mobilizing Key Stakeholders
Participants indicated that the successful passage of the SHAPE Act was attributable, in part, to the longstanding effort to engage, organize, and mobilize key stakeholder groups that had influence on the legislature, including lobbyists who could “build trusting relationships with legislators.” Georgia State University, the University of Georgia, and the Medical College of Georgia collaborated with statewide partners through a multisector initiative called Policy Leadership for Active Youth (PLAY), supported by the Healthcare Georgia Foundation. 16 Respondents indicated that PLAY “served as a neutral convener” and “helped organize stakeholders to highlight the problem, build awareness, and coordinate diverse partners.” Many participants suggested that PLAY “established a consortium of individuals who developed a trusting relationship with one another” where organizations could “leverage and coordinate their strengths.” Stakeholders were able to “unite behind a common mission.”
The initiative built upon existing efforts that were occurring in isolation and developed an “environment of collaboration.” In 2005, PLAY hosted a statewide strategic planning summit, Addressing Overweight: The Role of Physical Activity. 17 The statewide summit “convened workgroups and identified the most promising strategies” for increasing physical activity among Georgia’s children and adolescents. Participants suggested that the summit was “central to mapping a course” for childhood obesity prevention policy in Georgia. The recommendations that emerged informed dialogue, policy priorities, and advocacy activities on physical activity in schools.
Theme 3: Strategic Action to Promote Policy
Participants stated that stakeholders used strategies to address challenges within the social and political environment to generate widespread, bipartisan support. One important and effective strategy for addressing opposition was reframing obesity as a problem of fitness. According to respondents, Dr. Ken Cooper from the Cooper Institute, who was invited to speak to legislators, played a key role in changing the narrative. He was a “trusted, public face [who] connected well with legislators around this issue.” He was able to make the connection between academic performance and the physical fitness of children, which resonated with legislators. “Ken Cooper is known as the father of aerobics; and you know, [the] Cooper Institute created FitnessGram and the fitness testing protocol. So, I think there was just this move toward, ‘Have we thought about fitness rather than fatness?’” One respondent stated, “I don’t think it would have happened without a change in the framing.”
Respondents identified the role of grassroots outreach and advocacy as a vital strategy for increasing support. The Georgia Coalition for Physical Activity and Nutrition was “instrumental in advancing grassroots efforts” by developing a network of civically engaged residents.
18
According to 1 respondent, “I think the messaging and outreach led grassroots members to continue to confront their representatives. I felt it was really necessary for them to communicate with each legislator, with each senator, about what the community wanted.” Another participant echoed this sentiment: “We need grassroots organizing because, ultimately, policy makers respond to pressure from their constituents.” As a result of the broad outreach and advocacy, an alliance was established with a senior Republican legislator, who ultimately became the lead sponsor. One participant stated, “I think any strategies that get a senior legislator to take up an issue and invite lobbyists and academics to the table to discuss a solution are important.” Another participant asserted, “I can’t overstate the importance of having full-time professional lobbyists [who] have relationships with legislators, constituents, and academics and can have conversations with them about moving these issues forward.” One respondent captured the sentiments of the group: Their names being tied to it meant a lot. [Representative] Brooks [Coleman] was on the House side, and Dr. Don Thomas was on the Senate side. Those individuals were terrific in persuading their committee members to vote, get it out of committee…and without their individual help, this could not have been done.
Lessons Learned
This case study sought to identify the lessons learned in the development, advocacy, and passage of the SHAPE Act in Georgia. Data collected from key informants indicate that the adoption of the SHAPE Act was the culmination of a 6-year campaign focused on increasing knowledge and awareness of community members and leaders, addressing and overcoming opposition, and building the social and political will for policy solutions. We found that several factors were vital to policy adoption: a shifting social and political climate, the organization and mobilization of diverse partners behind a collective mission, and the use of strategies that facilitated progress. Surveillance data on childhood obesity were reported to play an important role in increasing awareness of the problem. Study participants reported that surveillance data and state reports such as the F as in Fat report, 12 which illuminated Georgia’s poor ranking among state obesity rates, were important tools. This finding highlights the value of national and state surveillance data and the potential they hold when communicated strategically.
Our findings also suggest that early legislative failures may have been due, in part, to framing the problem as obesity prevention. The shift toward fitness (rather than fatness) helped reduce opposition within the social and political environment, especially as it related to the surveillance of children. In Arkansas, researchers found that childhood obesity prevention legislation focused on BMI faced greater opposition than bills focused on fitness because of the potential stigma that BMI testing could have on overweight and obese children and adolescents. 19 Our findings indicate that support for obesity prevention legislation increased among policy makers once explicit monitoring of BMI was removed. This finding is consistent with Bombak, 20 who found that people were increasingly more supportive of approaches focused less on weight and more on health.
While addressing opposition, the need to organize and mobilize diverse stakeholders behind a collective mission became apparent. Childhood obesity prevention requires broad engagement from multiple stakeholders. 21 Our findings suggest that engaging a diverse collaborative network helped to educate the public, raise awareness, and build the political will among policy makers. Previous studies suggest that collaborative groups are often better positioned to translate emerging research to policy and practice because of their ability to address the issue from diverse perspectives. 19,22,23 Likewise, data from our study revealed the need for bipartisan support. Our findings suggest that the engagement of well-respected political champions, in both the House and Senate, were key factors for successful policy adoption. Previous studies found that obesity legislation with bipartisan political support and sponsorships is more likely to be adopted and implemented than legislation without backing from both major political parties. 24,25 Taken together, these findings suggest a need to seek out support across political parties, with a focus on engaging influential legislators.
Our findings also emphasized the importance of mobilizing the right people and groups in the policy process, including diverse community partners, citizens reached by grassroots outreach and advocacy, and influential policy makers. In this case, policy makers did not initially recognize obesity as a problem warranting action. As stakeholders and grassroots advocates built awareness and promoted support for policy solutions, they influenced the social and political climate through advocacy activities that created more favorable circumstances for policy proposals to be passed. Kingdon 26 suggests that when problem recognition, policy development, and political action converge, a policy window is created—an opportune and favorable environment for the adoption of legislation. The literature also suggests that public opinion is a powerful factor in obtaining legislators’ support for policy proposals. 27 Our findings suggest that the advocacy activities of legislators’ constituents influenced their decisions to sponsor or support the SHAPE Act. Future efforts are likely to benefit from the engagement of constituents who can pressure their elected officials.
Implementation of the SHAPE Act began in the 2011-2012 school year. At the time of this study, the relationship between this legislation and the obesity rates in Georgia had not yet been investigated. Although finding a linkage between the 2 was beyond the scope of this article, future research should explore the effect that state policies have on health outcomes.
Public policy is increasingly recommended as a strategy for addressing physical inactivity among children and adolescents. Guidance on effective approaches to advocating for such policies is vital to ensuring continued progress. Our findings suggest that engagement and collaboration among diverse partners, establishment of mutual interests as a basis for collaboration, and identification of realistic and evidence-based solutions hold promise for facilitating progress toward adopting policies that promote physical activity.
Public health professionals and policy advocates should consider the social and political environment in which they are operating, develop and coordinate an engaged network of diverse partners, employ grassroots outreach and advocacy, and work collaboratively with legislators to develop locally tailored policy solutions.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.