
Abstract
When food handlers become ill with hepatitis A virus (HAV) infection, state and local health departments must assess the risk of HAV transmission through prepared food and recommend or provide postexposure prophylaxis (PEP) for those at risk for HAV infection. Providing PEP (eg, hepatitis A [HepA] vaccine or immunoglobulin), however, is costly. To describe the burden of these responses on state and local health departments, we determined the number of public health responses to HAV infections among food handlers by reviewing public internet sources of media articles. We then contacted each health department to collect data on whether PEP was recommended to food handlers or restaurant patrons, the number of PEP doses given, the number of HepA vaccine or immunoglobulin doses given as PEP, and the mean number of health department person-hours required for the response. Of 32 public health responses identified from Twitter, HealthMap, and Google alerts from January 1, 2012, to December 31, 2014, a total of 27 (84%) recommended PEP for other food handlers or restaurant patrons or both. Per public health response, the mean cost per dose of the HepA vaccine or immunoglobulin was $34 139; the mean personnel cost per response was $7329; and the total mean cost of each response was $41 468. PEP is expensive. Less aggressive approaches to PEP, such as limiting PEP to fellow food handlers in nonoutbreak situations, should be considered in the postvaccination era. HepA vaccine for PEP provides long-term immunity and can be used when immunoglobulin is unavailable or cannot be administered within 14 days of exposure to HAV.
Hepatitis A virus (HAV) causes an acute illness that varies in severity according to age, immune status, and underlying comorbidities. It is transmitted through the fecal-oral route, typically through close personal contact or the consumption of food prepared by someone shedding the virus. HAV illness can be prevented by the hepatitis A (HepA) vaccine, which is safe and effective. The Advisory Committee on Immunization Practices (ACIP) first recommended HepA vaccine in 1996. 1 For susceptible patients (ie, those who have not been infected with the virus or vaccinated against it) who are exposed to the virus, the risk of infection can be reduced through the use of postexposure prophylaxis (PEP) if administered within 14 days of exposure. 2 The 2007 ACIP recommendation for PEP states that single-antigen HepA vaccine should be administered to healthy people aged 12 months to 40 years to prevent infection after exposure to HAV. 3 For people aged >40, immunoglobulin is preferred; however, the vaccine can be used if immunoglobulin cannot be obtained within 14 days. HepA vaccine provides at least 20 years of immunity, whereas immunity from HAV after immunoglobulin is only 3 months at most. For children aged <12 months and people who are immunocompromised, who have known chronic liver disease, or for whom vaccine is contraindicated, immunoglobulin should be used. 4
HAV-infected food handlers can spread the illness to people who consume their prepared food. Local or state public health departments recommend and/or provide PEP to patrons at risk for HAV illness in some situations. 5 Estimates suggest that public health departments spend approximately $340 per food handler case. 6 However, since the introduction of the HepA vaccine, the number of HAV infections has decreased, including those among food handlers. 7 Age characteristics of people with HAV infection and the financial burden of disease have also changed since universal infant vaccination was implemented. 8 Data on the true financial burden of food handler cases to state and local health departments have been limited since introduction of the HepA vaccine 9 because these data are not systematically collected. The objective of this study was to assess the financial burden, especially the cost of administering PEP, of public health responses to HAV infections among food handlers.
Methods
We collected data from reports of public health responses to HAV infections among food handlers daily and weekly from January 1, 2012, to December 31, 2014, through Twitter keywords, Google alerts, and HealthMap alerts. To maximize the chances of discovering all food handler–related public health responses in the United States during this period, we performed a LexisNexis database search of all US published news media paper and wire headlines using the keywords “hepatitis A” and “food” or “food handler” or “case” or “outbreak” or “investigation.” We attempted to confirm all information from these data sources by contacting state and local health departments; we obtained additional data on PEP, such as the number of HepA vaccine and immunoglobulin doses and the number of person-hours required to administer them. We asked state health officials to report any additional unique public health responses that we did not find by using the internet alert and social media or LexisNexis database searches. We calculated the total cost of each public health response to food handler–associated HAV infections by adding the cost of vaccination and/or administration of immunoglobulin and the cost of the person-hours required to respond. We assumed a single dose of HepA vaccine to cost approximately $40 (based on the 2016 Centers for Disease Control and Prevention price list). 10 We assumed a single dose of immunoglobulin to cost $60 10,11 ; we based person-hour costs on an hourly wage of $17.80. 12 We did not seek institutional review board review of this study because it involved only publicly available data.
Results
A review of Google alerts, Twitter, and HealthMap alerts from January 1, 2012, to December 31, 2014, resulted in 32 unique public health responses to HAV-infected food handlers in 16 US states; 37 people were affected (Table). The LexisNexis database search produced 512 results that described 23 distinct public health responses of food handler–related HAV illness, of which 22 public health responses overlapped with responses found in our initial search. State health officials did not report any additional HAV-infected food handler responses not reported in our searches.
Cost of public health investigations of HAV-infected food handlers reported by state and local health departments, including secondary cases among patrons and other food handlers, United States, 2012-2014a,b
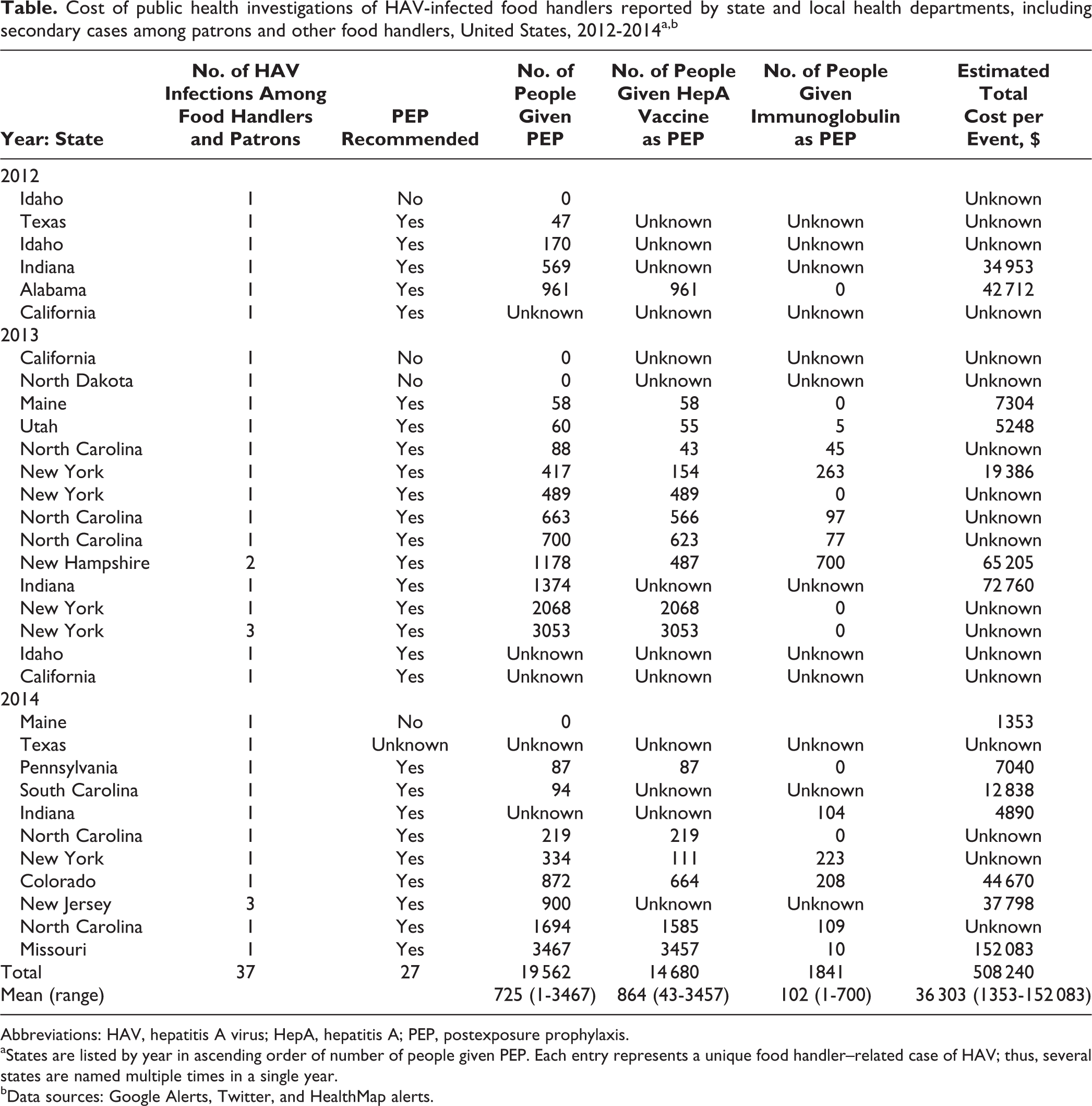
Abbreviations: HAV, hepatitis A virus; HepA, hepatitis A; PEP, postexposure prophylaxis.
aStates are listed by year in ascending order of number of people given PEP. Each entry represents a unique food handler–related case of HAV; thus, several states are named multiple times in a single year.
bData sources: Google Alerts, Twitter, and HealthMap alerts.
Of the 32 public health responses, 29 (91%) involved a single HAV-infected food handler; only 3 (9%) responses involved secondary cases among close contacts, including other food handlers and patrons. Public health departments recommended PEP for food handlers or patrons or both in 27 (84%) public health responses. PEP recommendations from public health departments varied by response. Of the 27 responses for which PEP was provided for food handlers, state and local health departments reported using HepA vaccine only for 7 (26%) responses; the main reason for providing HepA vaccine only was an inability to administer immunoglobulin within 14 days. In the 5 public health responses in which PEP was not recommended, 2 involved workers who were found to not have had contact with food; 2 were reported to the health department after the 14-day window for PEP had passed; and the reason was unknown for the other public health response (Table).
We were able to obtain data on the extent to which PEP was administered in 23 of 27 (85%) public health responses in which PEP was recommended; per response, the mean number of people receiving PEP was 725 (range, 0-3467). Based on information from health departments in 18 of 27 (67%) public health responses, a mean of 102 doses of immunoglobulin and 863 doses of HepA vaccine were administered. The mean cost of HepA vaccine or immunoglobulin per public health response was $34 139. Of public health responses with confirmed data, the mean person-hours per public health response was 411 hours (range, 41-1016), giving an estimated mean personnel cost of $7329. Based on these results, the mean calculated cost of a public health response to a reported case of an HAV-infected food handler was $41 468.
Discussion
The cost to health departments of investigating HAV infections among food handlers from 2012 to 2014 likely exceeded $40 000 per response; most investigations involved only 1 case (the infected food handler). Meltzer et al estimated the cost to the public health department—including evaluation of reported cases, administration of immunoglobulin, education efforts, and other outbreak control efforts—to be approximately $340 in 2001 for each exposure associated with an HAV-infected food handler case. However, that study’s data included costs to society, and its methods were different from ours; furthermore, that study was published before ACIP recommended universal infant vaccination, when case rates were much higher. 6 Our data, which included data from reported outbreaks, suggest that the cost to health departments per food handler case was much higher in 2014 than in 2001, likely because HAV infections among food handlers are usually isolated cases, such outbreaks are rare, and PEP is offered to all people who potentially consumed contaminated food.
Another study showed that in 1997 dollars, one HAV infection in an adolescent or adult cost $740 when the patient was not hospitalized and $6914 when the patient was hospitalized. 13 Cases from contaminated food or secondary to food handler contact were rare because of immunity among the exposed, timely PEP, or low risk of exposure (ie, the infected food handler did not contaminate the food that he or she prepared, because of good hygiene or not being symptomatic at the time of working). Universal childhood vaccination contributes to increased immunity among children and the subsequent lack of secondary HAV infections among children 9 ; however, childhood vaccination and subsequent reductions in circulating virus to provide lifelong immunity have also led to increased susceptibility among adults who were never vaccinated nor exposed to infected children. 8
Although data on the efficacy of PEP for adults aged >40 are limited, 14,15 some states allow HepA vaccination for PEP when immunoglobulin cannot be administered within 14 days. 16 This permissive policy is likely informed by difficulties in obtaining immunoglobulin, actual or perceived shortages of immunoglobulin, and inadequate time available for shipping immunoglobulin to the location where administration is taking place. Additionally, unlike immunoglobulin, HepA vaccine protects people from future exposures. If immunoglobulin and/or HepA vaccine cannot be given within 14 days, it is unlikely that protection will be provided. The low number of reported secondary cases suggests that giving HepA vaccine when immunoglobulin is not available for people aged >40 is effective, although the risk of exposure cannot be determined.
Limitations
Our study had several limitations. First, we used the 2016 price list for HepA vaccine, which would have overestimated the cost of PEP during outbreaks before 2016. Second, we relied on media reports, and several years had passed since many of the responses had occurred, making our study susceptible to recall bias. Third, we examined only the cost associated with the health department public health response; we did not consider the cost to the food establishment affected, vaccine-related adverse events, other outbreak-related expenses, or any savings associated with prevention of HAV disease (ie, hospitalizations and deaths, medical and work loss), which were outside the scope of this study. Fourth, we did not consider data on the age of people receiving PEP, HepA vaccine, and immunoglobulin, because these data were unavailable. Last, our study likely did not include all public health responses to HAV that occurred during this period, because we included only those reported in the media.
Conclusion
The administration of PEP to food handlers and restaurant patrons during a public health response to HAV is costly to public health departments. Less aggressive approaches to PEP administration should be considered, such as administering PEP only to the HAV-infected food handler’s coworkers or limiting the administration of PEP of patrons (1) when poor food handler hygiene is suspected or known (ie, direct contact with food without gloves or other barriers while symptomatic), (2) when repeated exposures to potentially contaminated food occurred, or (3) where an outbreak has occurred. 9 HepA vaccine should be given in appropriate populations for PEP because it provides long-term immunity that immunoglobulin does not provide. More data on the effectiveness of HepA vaccine for PEP among people aged >40 is needed to guide public health interventions during outbreaks.
Footnotes
Authors’ Note
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Acknowledgments
We thank Kathleen Winter, California Department of Public Health; Patricia Bosse, Maine Centers for Disease Control and Prevention; Rachel Wiseman, Texas Department of State Health Services; Tess Gordon, Indiana State Department of Health; John Bos, Missouri Department of Health and Senior Services; Alicia Lepp, North Dakota Department of Health; Daniel Kuhles, New York State Department of Health; Leslie Tengelsen, Idaho Department of Health and Welfare; Vasudha Reddy, New York City Department of Health and Mental Hygiene; Kimberly Warren, Pennsylvania Department of Health; Elizabeth Daly, New Hampshire Department of Health and Human Services; Alicia Cronquist, Colorado Department of Public Health and Environment; Sherri Davidson, Alabama Department of Public Health; Kenny Davis, Utah Department of Health; Rosemary Kidder, New Jersey Department of Health; and David Young, South Carolina Department of Health and Environmental Control.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.