
Abstract
Objectives:
Preventive health services are important for child development, and parents play a key role in facilitating access to services. This study examined how parents’ reasons for not having a usual source of care were associated with their children’s receipt of preventive services.
Methods:
We used pooled data from the 2011-2014 National Health Interview Survey (n = 34 843 participants). Parents’ reasons for not having a usual source of care were framed within the Penchansky and Thomas model of access and measured through 3 dichotomous indicators: financial barriers (affordability), attitudes and beliefs about health care (acceptability), and all other nonfinancial barriers (accessibility, accommodation, and availability). We used multivariable logistic regression models to test associations between parental barriers and children’s receipt of past-year well-child care visits and influenza vaccinations, controlling for other child, family, and contextual factors.
Results:
In 2014, 14.3% (weighted percentage) of children had at least 1 parent without a usual source of care. Children of parents without a usual source of care because they “don’t need a doctor and/or haven’t had any problems” or they “don’t like, trust, or believe in doctors” had 35% lower odds of receiving well-child care (adjusted odds ratio = 0.65; 95% CI, 0.56-0.74) and 23% lower odds of receiving influenza vaccination (adjusted odds ratio = 0.77; 95% CI, 0.69-0.86) than children of parents without those attitudes and beliefs about health care. Financial and other nonfinancial parental barriers were not associated with children’s receipt of preventive services. Results were independent of several factors relevant to children’s access to preventive health care, including whether the child had a usual source of care.
Conclusions:
Parents’ attitudes and beliefs about having a usual source of care were strongly associated with their children’s receipt of recommended preventive health services. Rates of receipt of child preventive services may be improved by addressing parents’ attitudes and beliefs about having a usual source of care. Future studies should assess causes of these associations.
Keywords
Parental factors play a role in children’s health service use. 1 For example, mothers’ patterns of health service use are strongly linked with their children’s patterns, 2 even after accounting for other determinants of access to care. 3 Parents’ access to health care is also related to their children’s health care in that children of parents without a usual source of care are more likely to have unmet medical or prescription needs than children with at least 1 parent with a usual source of care. 4 In view of rising rates of adults without a usual source of care (from 17.8% in 1999-2000 to 19.7% in 2012-2013), this latter finding is concerning. 5
Two preventive health services that are particularly important for children are well-child care visits and annual influenza vaccinations. The American Academy of Pediatrics recommends at least 1 well-child care visit each year beginning at birth and 1 influenza vaccination each year beginning at age 6 months. 6,7 In 2007-2008, just 58.9% of children had the recommended number of well-child care visits. 8 During the 2011-2012 influenza season, just 52% of children received an influenza vaccine. 9 Deficiencies in the receipt of these and other preventive services disproportionately occur among children in racial/ethnic minority groups and disadvantaged socioeconomic groups. 10 Although several explanations for disparities in children’s receipt of health services have been proposed, 11,12 few studies have examined the barriers to accessing health care that parents report for themselves.
Barriers to health care can be assessed with the framework developed by Penchansky and Thomas, which defines access to health care as a multidimensional construct reflecting the fit between patients’ expectations and the availability, accessibility, accommodation, affordability, and acceptability of services provided. 13 Policy makers typically focus on the affordability of access 14 (eg, via legislation such as the Affordable Care Act, which focuses on increasing health insurance coverage and reduces patients’ out-of-pocket costs for preventive care). 15 Health insurance coverage improves health care access. 16 However, it does not address nonfinancial barriers (ie, availability, accessibility, accommodation, and acceptability), 17 which also contribute to disparities and inequalities in access and may sometimes have stronger effects than financial barriers. 18 For example, in a study that asked a nationally representative sample of parents for the primary reason why their children did not have a usual source of care, 10% of respondents reported financial barriers and 74% cited nonfinancial barriers. Among parents reporting nonfinancial barriers, most (89%) cited that the primary reason their children did not have a usual source of care was that they were “seldom or never sick.” 19 A study of a nationally representative sample of adults reported similar barriers when asked about their own usual source of care; only 14% cited financial barriers as the major reason why they were unable to access a usual source of care, whereas 86% identified nonfinancial barriers. Of those citing nonfinancial barriers, 77% reported that they did not have a usual source of care, because they were “seldom or never sick.” 20 This attitude toward having a usual source of care (ie, not having a usual source of care because of not being sick) was the primary barrier reported by adults across all racial/ethnic groups and was independent of poverty status and health insurance status. 21 Thus, although removing financial barriers to health care is critical for improving access to care and reducing health disparities, nonfinancial barriers to health care, particularly patient and family attitudes and beliefs toward care, should also be considered.
We examined whether parental barriers to accessing a usual source of care were associated with the receipt of 2 children’s preventive services. We examined financial barriers, parental attitudes and beliefs toward health care, and other nonfinancial barriers in relation to children’s receipt of well-child care visits and influenza vaccination. To assess independent associations between parental barriers and children’s receipt of preventive services, we controlled for several child, family, and contextual variables, including child’s access to care (health insurance status and usual source of care status), nativity status, family size, family structure, marital status, and indicators of socioeconomic status (parents’ education level and household income).
Methods
Data
This study used pooled data from the 2011-2014 National Health Interview Survey (NHIS). The NHIS is an annual household interview survey administered by the National Center for Health Statistics to better understand the health of the US civilian noninstitutionalized population. 22 The NHIS uses a multistage probability sampling design and oversamples African American and Hispanic households. In-person interviews conducted by trained US Census Bureau interviewers address a range of health topics affecting the whole family. In-depth questions are also administered to 1 sample adult (“adult core interview”) and 1 sample child (“child core interview”) from each household. Questions about children are answered by a knowledgeable adult family member.
From 2011 to 2014, a total of 52 365 families completed a child core interview, and 35 773 of those included an adult core interview with a parent (biological, adoptive, step, in-law, or foster). Data from foster parents were excluded (n = 32) because information on foster parent status was unavailable in 2013 and 2014. Also excluded from our sample were 621 families in which the parent did not report usual source of care status or the parent identified an emergency department as the usual source of care. Emergency departments do not meet the standard definition of a usual source of care, 23 but they were treated as such in the NHIS; therefore, questions about barriers to accessing a usual source of care were skipped, making key data from these families unavailable. Because our study focused only on children living with at least 1 parent, we excluded 277 families without a mother or a father. Data from the remaining 34 843 families were used for this study. Listwise deletion for item missingness, which was ≤2% for all variables, reduced the final analytic samples to 34 617 families for the model of well-child visits and 34 234 families for the model of influenza vaccinations.
Dependent Variables
We measured children’s receipt of preventive health services with 2 dichotomous variables (coded yes = 1 and no = 0) derived from responses to the following questions: (1) “During the past 12 months, did the child receive a well-child check-up; that is, a general check-up when he/she was not sick or injured?” and (2) “During the past 12 months, has the child had a flu vaccination?” We identified both H1N1 and seasonal flu vaccinations as influenza vaccinations. 24
Primary Independent Variables: Parental Barriers to Accessing a Usual Source of Care
We identified parents as having a usual source of care if they indicated that they had a place where they usually went when they were sick or in need of health advice; those who responded “no” were later asked to choose from 9 preselected options to indicate all reasons for not having a “regular source of medical care.” 25 Building on previous work, 18,26,27 we classified parental barriers to accessing a usual source of care into financial barriers and nonfinancial barriers, with nonfinancial barriers separated into parental attitudes and beliefs and all other nonfinancial barriers. Financial barriers correlate with the affordability dimension of Penchansky and Thomas’s framework and indicate the relationship of service costs to the patient’s ability to pay (eg, not having a usual source of care because of a lack of health insurance). 25 Parental attitudes and beliefs correlate with the acceptability dimension of access and included the following reasons for not having a usual source of care: “don’t like/trust/believe in doctors” and “don’t need a doctor/haven’t had any health problems.” Other nonfinancial barriers included all other dimensions of access, such as availability (eg, “previous doctor not available/moved”), accommodation (eg, “put it off/didn’t get around to it”), and accessibility (eg, “care too far away/not convenient”). 13 We operationalized these barriers with 3 nonexclusive dichotomous variables, all coded as 1 = yes and 0 = no.
Covariates
The selection of child, family, and contextual variables was guided by previous studies of parents’ impact on health service use 4 and included children’s sex, race/ethnicity, age, nativity status (US born/foreign born), health insurance status (public/private/no), usual source of care status (yes/no), functional limitation status (yes/no), and health status (ordinal scale, where 4 = excellent, 3 = very good, 2 = good, and 1 = fair/poor). Children were considered to have a functional limitation if they had any limitation in normal play activities because of physical, mental, or emotional problems. 28 Family and contextual characteristics included in the analysis were family structure (1-parent/2-parent household), marital status (married/not married), reported household income as a percentage of the federal poverty level, household education level measured as a dichotomous variable indicating whether at least 1 parent completed high school, US Census region (Midwest, Northeast, South, or West), and the number of children aged <18.
Two-parent families included married parents, unmarried parents, and families with at least 1 parent and 1 stepparent or cohabiting partner; parents could be biological or adoptive. 29 Family structure is particularly important because 1-parent families have higher rates of access-to-care barriers than 2-parent families. 30,31 However, some studies show that children in 1-parent families have equal or higher rates of receipt of preventive care when compared with children in 2-parent families. 31,32 Differences in the allocation of resources (eg, financial, time available to organize and execute daily tasks, social support) between 1- and 2-parent families likely require different strategies to overcome access barriers, supporting the hypothesis—which we tested—that relationships between parental barriers and receipt of child preventive services may vary depending on family structure.
Statistical Analysis
We merged household, family, and sample adult data with sample child data and used weights provided with child data to adjust for the complex study design and survey nonresponse. 33 We compared characteristics of families having at least 1 parent with a usual source of care with children of parents without a usual source of care, stratified by family structure, using Pearson’s χ 2 tests for categorical variables and t tests for continuous variables. We calculated the percentage of children living with at least 1 parent without a usual source of care for each parental barrier for the total sample and by family structure. We tested differences over time through simple logistic regression analysis, with 2014 as the referent year. We then used multivariable logistic regression models for each dependent variable to estimate associations with all primary independent variables, while including all aforementioned covariates. To account for temporal variation in receipt of preventive services, we included a categorical variable for survey year, with 2011 as the referent year. We examined whether associations between parental barriers and receipt of children’s preventive services varied by family structure by including an interaction term (parental barrier by family structure) in the multivariable logistic regression models. We computed variance inflation factors to test for multicollinearity in all models, and multicollinearity was not detected. We conducted all analyses with Stata version 14.1 svy procedures, 34 using survey weights and NHIS design characteristics to adjust standard errors through the Taylor linearized variance estimator. 35 –37 We adjusted survey weights to account for the pooled data. 38
The protocol for this secondary analysis was approved by the Institutional Review Board at San Diego State University.
Results
In 2014, 53.4% (708 of 1327) of parents without a usual source of care reported not having one because of attitudes and beliefs about health care; specifically, 51.2% (679 of 1327) of parents reported that they “don’t need a doctor/haven’t had any problems” and 2.9% (38 of 1327) reported that they “don’t like, trust, or believe in doctors” (Table 1). Of the 34 843 children in the sample, 28 311 (weighted percentage = 82.6%) had a well-child visit, and 16 021 (weighted percentage = 46.4%) received an influenza vaccination during the year in which they were surveyed between 2011 and 2014 (Table 2). Among 2-parent families, fewer children of parents without a usual source of care received a well-child care visit (weighted percentage = 75.2% vs 84.4%) or influenza vaccination (weighted percentage = 43.3% vs 48.4%) than children of parents with a usual source of care; the same pattern was present among 1-parent families. Similarly, all characteristics except for sex, functional status, and marital status (for 1-parent families only) differed by whether parents had a usual source of care. The most notable difference was that children who did not have a usual source of care were >6 times more likely than children with a usual source of care to have a parent who did not have a usual source of care (weighted percentage = 2.2% vs 14.6%, respectively, for children in 1-parent families; weighted percentage = 1.8% vs 12.2%, respectively, for children in 2-parent families).
Parental reasons for not having a usual source of medical care among parents without a usual source of care (n = 5975a), by year, National Health Interview Survey, 2011-2014b
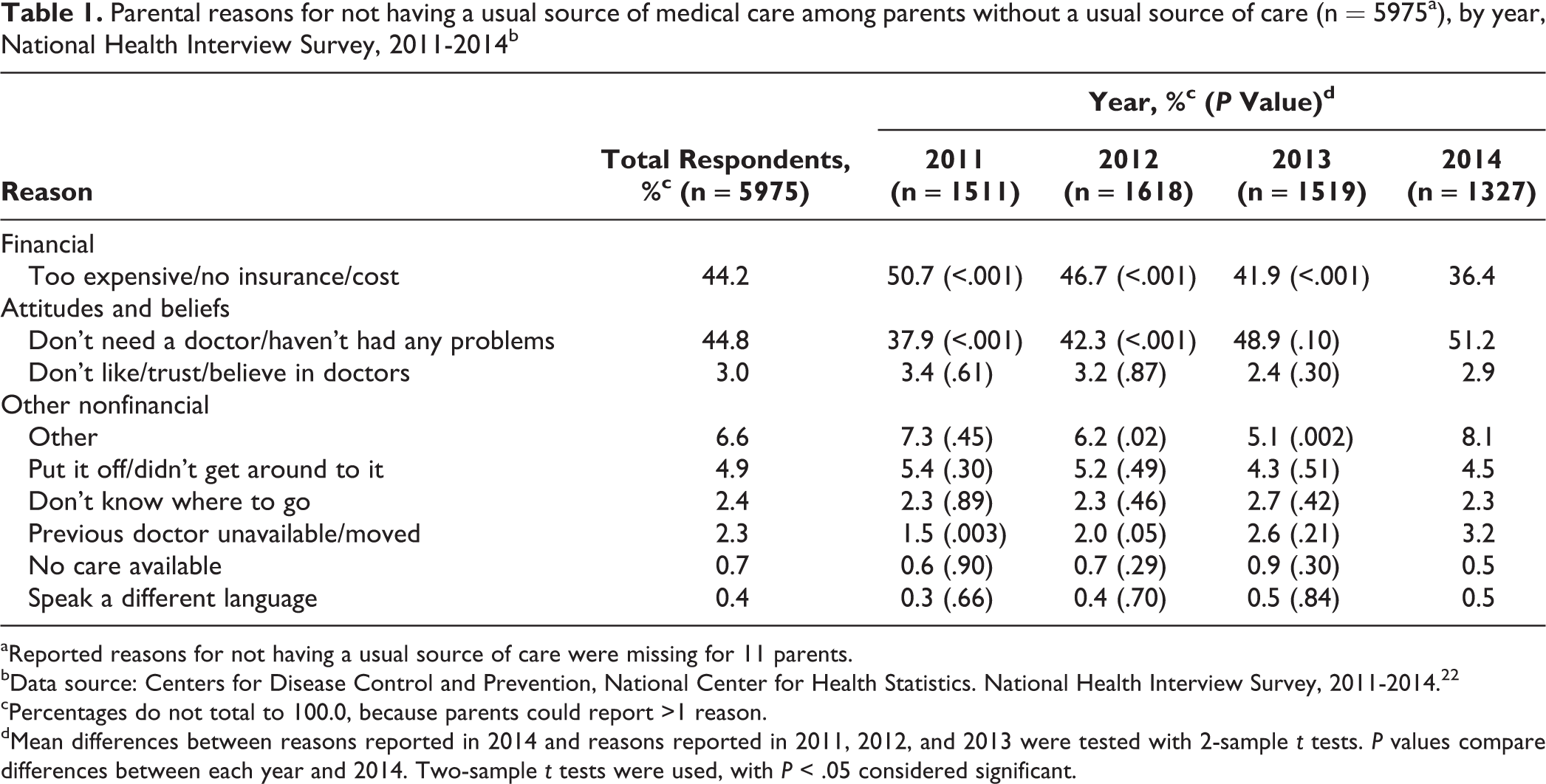
aReported reasons for not having a usual source of care were missing for 11 parents.
bData source: Centers for Disease Control and Prevention, National Center for Health Statistics. National Health Interview Survey, 2011-2014. 22
cPercentages do not total to 100.0, because parents could report >1 reason.
dMean differences between reasons reported in 2014 and reasons reported in 2011, 2012, and 2013 were tested with 2-sample t tests. P values compare differences between each year and 2014. Two-sample t tests were used, with P < .05 considered significant.
Child and family characteristics of US children aged 0-17 from 1- and 2-parent families, by whether or not parents have a usual source of care, National Health Interview Survey, 2011-2014a
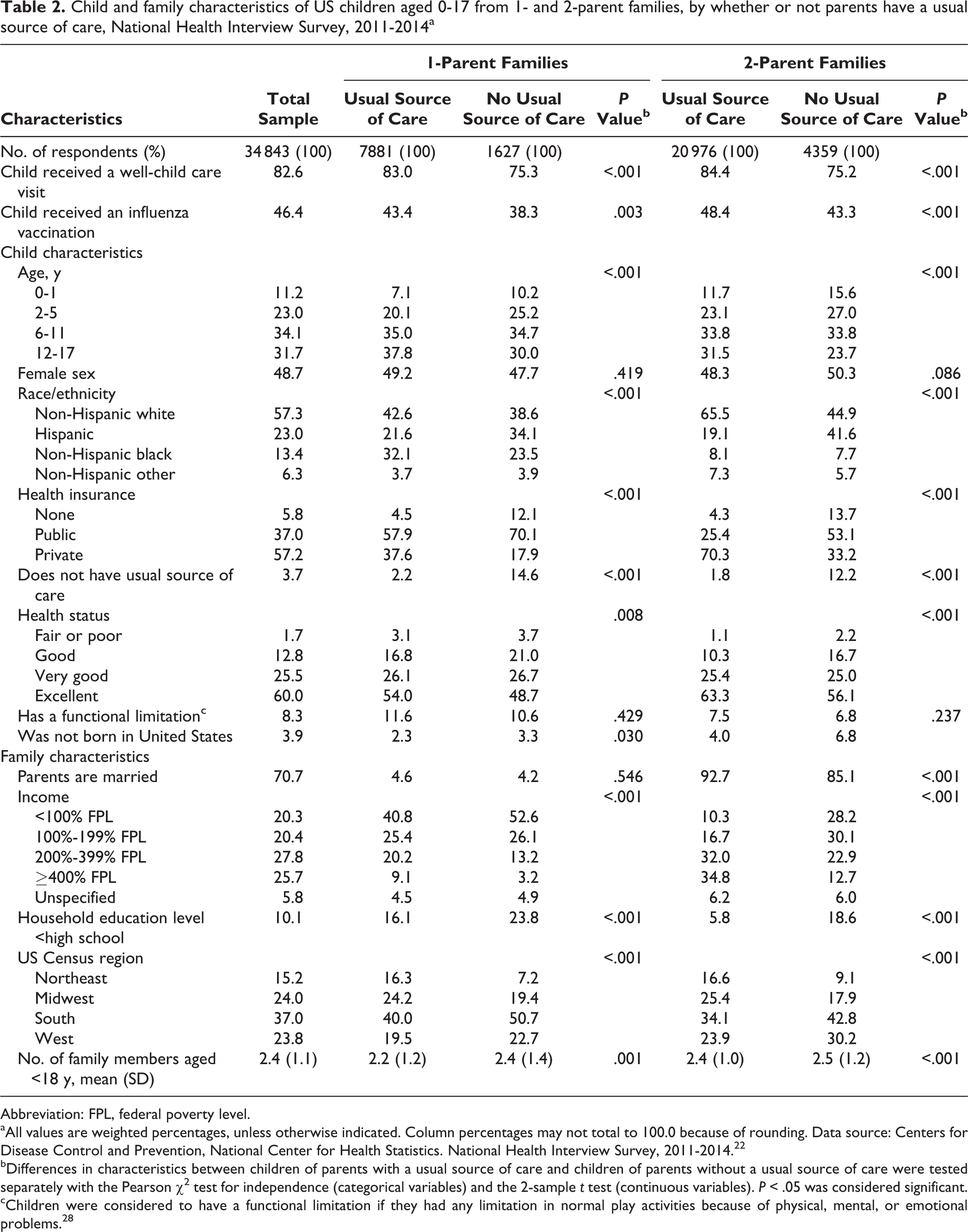
Abbreviation: FPL, federal poverty level.
aAll values are weighted percentages, unless otherwise indicated. Column percentages may not total to 100.0 because of rounding. Data source: Centers for Disease Control and Prevention, National Center for Health Statistics. National Health Interview Survey, 2011-2014. 22
bDifferences in characteristics between children of parents with a usual source of care and children of parents without a usual source of care were tested separately with the Pearson χ 2 test for independence (categorical variables) and the 2-sample t test (continuous variables). P < .05 was considered significant.
cChildren were considered to have a functional limitation if they had any limitation in normal play activities because of physical, mental, or emotional problems. 28
Between 2011 and 2014, 14.3% (95% CI, 13.3%-15.4%) to 17.5% (95% CI, 16.5%-18.6%) of children lived with at least 1 parent without a usual source of care (Table 3). Rates of children living with parents who had financial barriers to care were lower in 2014 than in 2011-2013 for both 1- and 2-parent families (all P values ≤ .01). We did not observe consistent temporal patterns for parental attitudes and beliefs or other nonfinancial barriers. The percentages of children living with a parent without a usual source of care were similar for 1- and 2-parent families (except for during 2012), although more 1- than 2-parent families reported financial barriers each year, and more 2- than 1-parent families reported attitudes and beliefs toward health care as barriers each year.
Percentage of children aged 0-17 living with at least 1 parent without a usual source of care, by parental barrier type, for the total sample, 1-parent families, and 2-parent families: National Health Interview Survey, 2011-2014a
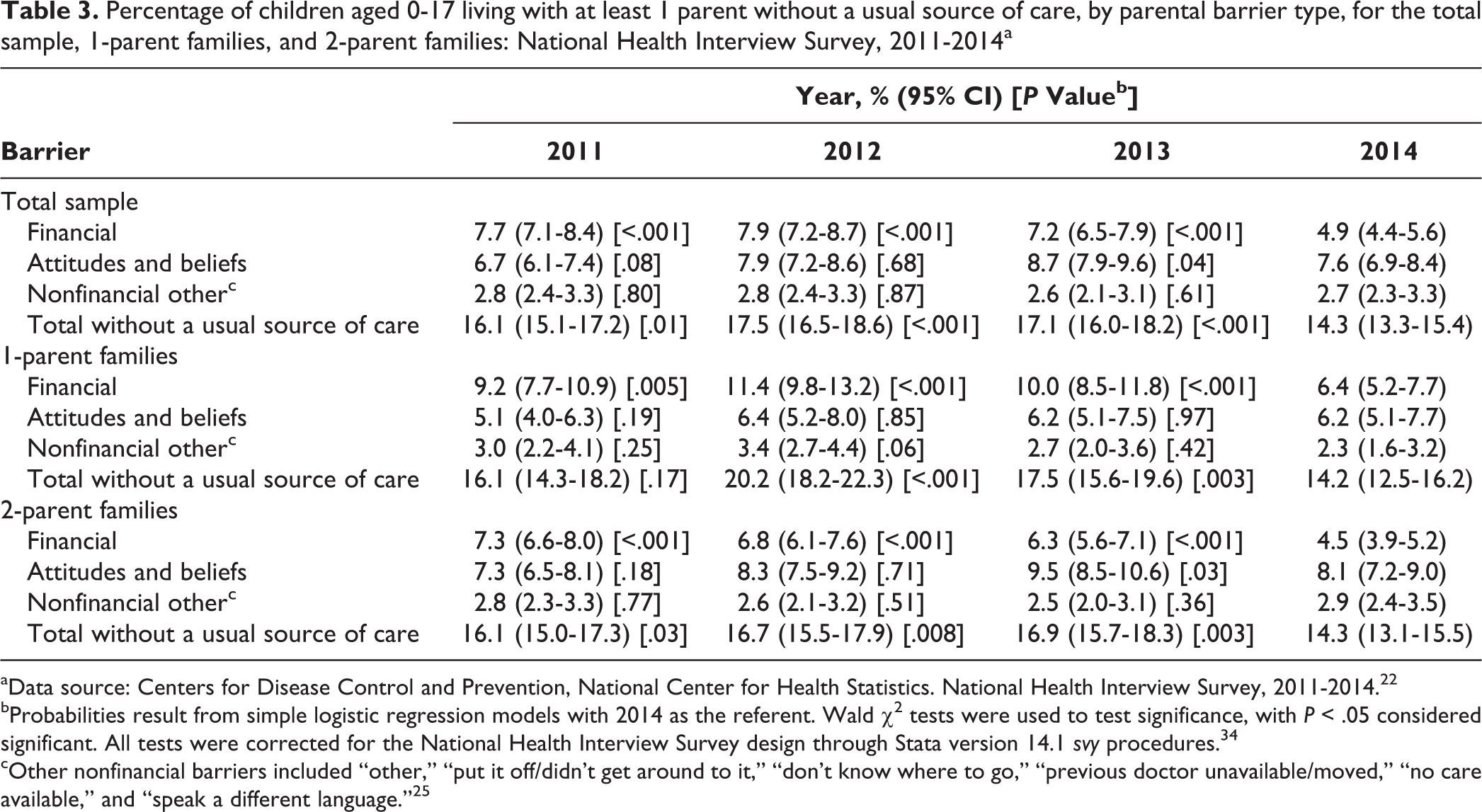
aData source: Centers for Disease Control and Prevention, National Center for Health Statistics. National Health Interview Survey, 2011-2014. 22
bProbabilities result from simple logistic regression models with 2014 as the referent. Wald χ2 tests were used to test significance, with P < .05 considered significant. All tests were corrected for the National Health Interview Survey design through Stata version 14.1 svy procedures. 34
cOther nonfinancial barriers included “other,” “put it off/didn’t get around to it,” “don’t know where to go,” “previous doctor unavailable/moved,” “no care available,” and “speak a different language.” 25
Associations between parental barriers and children’s receipt of preventive services did not differ by family structure (all P values for interaction terms ≥.22, data available upon request). Therefore, results from the multivariable models are reported for 1- and 2-parent families combined. Parents’ attitudes and beliefs about having a usual source of care were associated with their children’s receipt of preventive care; specifically, children of parents without a usual source of care because of attitudes and beliefs had 35% lower odds of receiving a well-child care visit (adjusted odds ratio = 0.65; 95% CI, 0.56-0.74) and 23% lower odds of receiving an influenza vaccination (adjusted odds ratio = 0.77; 95% CI, 0.69-0.86) than children of parents not reporting attitudes and beliefs, after controlling for relevant child, family, and contextual characteristics (Table 4). Other parental financial and nonfinancial barriers were not associated with children’s receipt of preventive services.
Multivariable logistic regression results for the associations between parental barriers for having a usual source of care and children’s receipt of 2 preventive services in the past year: National Health Interview Survey, 2011-2014a (n = 34 843b)
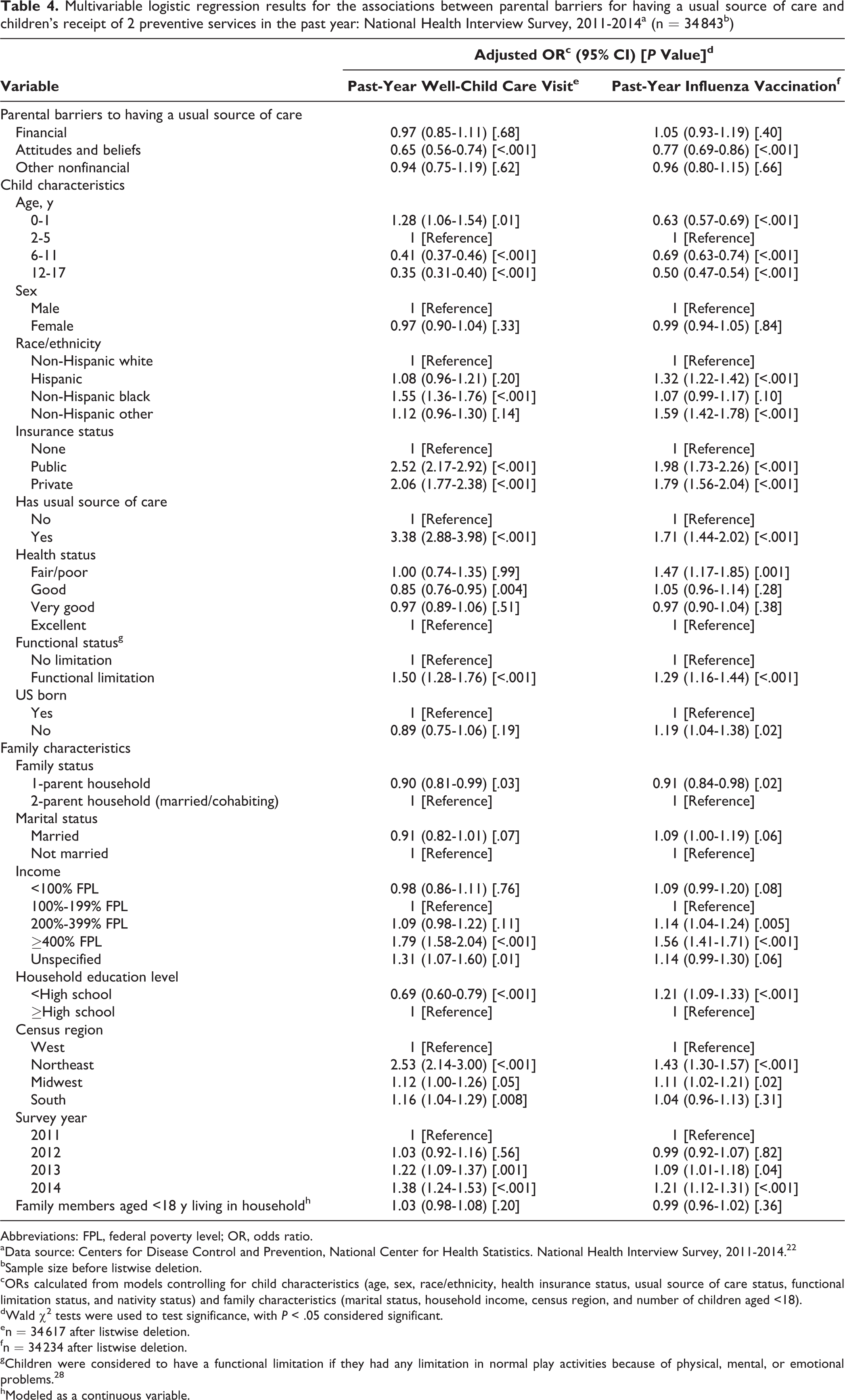
Abbreviations: FPL, federal poverty level; OR, odds ratio.
aData source: Centers for Disease Control and Prevention, National Center for Health Statistics. National Health Interview Survey, 2011-2014. 22
bSample size before listwise deletion.
cORs calculated from models controlling for child characteristics (age, sex, race/ethnicity, health insurance status, usual source of care status, functional limitation status, and nativity status) and family characteristics (marital status, household income, census region, and number of children aged <18).
dWald χ2 tests were used to test significance, with P < .05 considered significant.
en = 34 617 after listwise deletion.
fn = 34 234 after listwise deletion.
gChildren were considered to have a functional limitation if they had any limitation in normal play activities because of physical, mental, or emotional problems. 28
hModeled as a continuous variable.
Discussion
This study was the first to examine how parental barriers to accessing a usual source of care were associated with children’s receipt of 2 recommended preventive health services. Parental financial barriers were not associated with children’s receipt of preventive services. Parents who reported that they did not have a usual source of care because they “don’t need a doctor and/or haven’t had any problems” or because “they don’t like/trust/or believe in doctors” had children with lower odds of receiving annual well-child care or influenza vaccination than children of parents who did not report these reasons. Children’s receipt of preventive services was not related to other nonfinancial barriers. Our results were controlled for several factors relevant to child health service use, including whether children had health insurance and whether they had a usual source of care.
Attitudes and beliefs toward health care have been the predominant reason for not having a usual source of care for the whole noninstitutionalized US population, 19,21,39 for adults only, 20 and for children only. 40 Parents’ attitudes and beliefs about their children’s preventive health care (specifically well-child care visits 41 and influenza vaccinations 42 ) have previously been related to reduced rates of receipt of care. Our study provides the first evidence that parents’ attitudes and beliefs about their own health care may play a role in their children’s receipt of recommended preventive health services.
The results presented here corroborate previous findings that living with a parent who does not have a usual source of care is related to children’s receipt of preventive health services. 4,43 Our estimates for the prevalence of children living with a parent without a usual source of care (ranging from 14.3% to 17.5%) were lower than the 2009-2010 estimates for the total US population aged 18-44 (20.3%) 5 and substantially lower than estimates by a study using 2002-2007 data from the Medical Expenditure Panel Survey; in those data, approximately 31.8% of children were identified as living with at least 1 parent without a usual source of care. 5 Differences in the survey designs of the Medical Expenditure Panel Survey and NHIS likely contribute to some of this variance. However, as reflected in the NHIS data (Table 3), the number of parents without a usual source of care has decreased over time possibly because of efforts by policy makers and others to improve access to care.
Our study findings also indicate that a larger proportion of our total sample reported nonfinancial barriers than financial barriers to accessing care. These findings are consistent with previous research 20 and confirm the need for policy makers to consider more than affordability of care in efforts to address disparities in health care access and maximize family well-being. 44
Practice Implications
It is intuitive that parents’ access to health care is related to their children’s receipt of health care services. However, most children in our study received recommended well-child care visits regardless of whether their parents had a usual source of care. For the remaining children, addressing nonfinancial barriers to care may be critical to ensuring that recommended services are received. For families reporting nonfinancial barriers to accessing care, sick-child visits may serve as an important point of contact and represent an underused opportunity to increase future receipt of preventive services by children and parents. For example, during these visits, physicians or other health care staff members could administer brief interventions, such as the Right Question Project (http://rightquestion.org), which are intended to improve adults’ engagement in care by having them play a more active role in medical decision making. 45 This model of engaging parents during their children’s health care visits can be seen as an extension of the opportunistic preventive care delivery model that has proven to be both efficient and effective at improving uptake of preventive services in other settings and populations. 46,47
Limitations
This study had several limitations. First, the cross-sectional design of the NHIS and this study allowed for identification of associations rather than causes. Our estimates relied on self-reports—the primary methods for assessing access barriers—and were subject to recall and social desirability biases.
Second, this study was a secondary analysis of publicly available data that limited analyses to information provided in the NHIS. We obtained data on parents’ usual source of care and barriers with the sample adult questionnaire administered to 1 adult in each household. As a result, data on usual source of care were unavailable for the second parent in 2-parent families. Having data on usual source of care from both parents, when present, would provide a more complete picture of family dynamics that may influence children’s access to care. 31 Future research should examine these issues in more detail. Third, data on receipt of other preventive services and the participant’s state of residence were also not available. Fourth, the adult questionnaire did not measure barriers for parents who classified emergency departments as their usual source of care. Consequently, this relatively small sample (n = 458) was excluded from analyses.
Fifth, we were limited to assessing the barriers listed in the NHIS, which may not encompass all barriers preventing parents from accessing a usual source of care. However, the financial barriers listed (ie, too expensive, no insurance, cost) were broad enough to depict the relationship between the total price of accessing a usual source of care and the respondents’ ability to pay. Nonfinancial barriers could include a wide array of reasons for not accessing a usual source of care, and although only 7 unique categories were provided in the NHIS, nonfinancial barriers not fitting those preselected reasons were measured by the “other” response category.
Last, parents play a key role in ensuring that their children receive appropriate curative and preventive health care. Parents’ attitudes and beliefs about accessing care may or may not be similar to their attitudes and beliefs toward their children’s preventive care, which were not measured by the NHIS.
Conclusion
Parental attitudes and beliefs toward their own health care are associated with their children’s receipt of recommended preventive services, but financial and other nonfinancial barriers were not. Future studies could investigate the degree to which parents’ attitudes and beliefs toward their own care reflect their attitudes and beliefs about their children’s care and, most important, whether changing parents’ attitudes and beliefs results in improved rates of receipt of preventive services among their children.
Footnotes
Acknowledgments
We thank Sandy Liles for his critical review of this study and its methods.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded in part by the Center for Behavioral Epidemiology and Community Health, Graduate School of Public Health, San Diego State University.