
Abstract
Objectives:
The primary objective of this study was to identify patients with heat-related illness (HRI) using codes for heat-related injury diagnosis and external cause of injury in 3 administrative data sets: emergency department (ED) visit records, hospital discharge records, and death certificates.
Methods:
We obtained data on ED visits, hospitalizations, and deaths for Florida residents for May 1 through October 31, 2005-2012. To identify patients with HRI, we used codes from the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) to search data on ED visits and hospitalizations and codes from the International Classification of Diseases, Tenth Revision (ICD-10) to search data on deaths. We stratified the results by data source and whether the HRI was work related.
Results:
We identified 23 981 ED visits, 4816 hospitalizations, and 140 deaths in patients with non–work-related HRI and 2979 ED visits, 415 hospitalizations, and 23 deaths in patients with work-related HRI. The most common diagnosis codes among patients were for severe HRI (heat exhaustion or heatstroke). The proportion of patients with a severe HRI diagnosis increased with data source severity. If ICD-9-CM code E900.1 and ICD-10 code W92 (excessive heat of man-made origin) were used as exclusion criteria for HRI, 5.0% of patients with non–work-related deaths, 3.0% of patients with work-related ED visits, and 1.7% of patients with work-related hospitalizations would have been removed.
Conclusions:
Using multiple data sources and all diagnosis fields may improve the sensitivity of HRI surveillance. Future studies should evaluate the impact of converting ICD-9-CM to ICD-10-CM codes on HRI surveillance of ED visits and hospitalizations.
Keywords
Record-breaking summer temperatures and deadly heat waves in recent years have led to an increased awareness, particularly among public health workers, of adverse heat-related outcomes.
1,2
As a result, public health surveillance efforts have increased, with the goal of reducing heat-related morbidity and mortality. Such surveillance has been conducted with
Heat-health warning systems—when a trigger criterion is met (eg, ≥x expected deaths or a priori temperature intensity or duration threshold), jurisdictions activate prevention activities
3
Syndromic surveillance—near real-time surveillance (eg, every 12 hours), often with emergency department (ED) chief complaint keywords to identify heat-related illness (HRI)
4,5
Retrospective analysis—analyzing historical morbidity and mortality data and potentially combining them with environmental data (eg, temperature)
1,6
–10
Active follow-up—contacting patients for additional information
11,12
Because high environmental heat may affect multiple body systems, some surveillance systems have measured adverse heat-related outcomes with all-cause morbidity or mortality; others have measured these outcomes with cause-specific morbidity or mortality. 7,8,13 When used to measure heat-related health outcomes, all-cause morbidity or mortality may have a high sensitivity but a low specificity, whereas cause-specific morbidity or mortality may have a high specificity but a low sensitivity. Neither is ideal. Furthermore, the use of either outcome measure in this setting may be suboptimal because both require the use of a baseline (or low-heat exposure) estimate for comparison and both rely on the assumption that all cases above that baseline are related to exposure to high outdoor heat, which may not be accurate.
Alternately, numerous surveillance systems have used HRI as the preferred outcome to be measured. 5,13,14 Although HRI may underestimate the incidence of adverse heat-related outcomes, 13 its use has been supported by cause-specific analyses in which HRI is the outcome with the largest relative increase during a heat wave or when ambient outdoor heat increases. 15 –18 A logical assumption is that if the HRI rate or count is increasing, then other heat-related outcomes are also increasing.
HRI has typically been identified by using different coding schemes, such as the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM), 19 or emergency medical services categories, 18,20 or by using keywords in free-text fields (eg, ED chief complaint notes). Even so, little has been published about the proportion of patients with HRI identified by specific code queries and keyword searches, how results with these methods may vary by data source, or how the proportion of patients with HRI identified by the query components may vary by whether or not the HRI was work related. 1,5,21 –25
The primary objective of this study was to identify patients with HRI through ICD codes for heat-related diagnosis and external cause of injury in 3 large state administrative data sets often used for HRI surveillance: ED visits, hospital discharge records, and death certificates. A secondary objective was to stratify the analysis by whether or not the HRI was work related. Findings could contribute to a discussion about outcome measures used for heat-related morbidity and mortality surveillance and provide a framework by which other jurisdictions could explore their data and refine their HRI surveillance efforts.
Methods
We obtained unpublished data on ED visits and hospital discharges from the Florida Agency for Health Care Administration for 2005 through 2012. The ED data set contained only the visits of patients who were treated and released, and the hospital discharge data set contained data on all patient hospitalizations, regardless of the admission source (via ED or directly to the hospital). We obtained unpublished data on deaths for the same years from the Florida Department of Health, Office of Vital Statistics. The University of North Carolina Institutional Review Board approved the study. The Florida Department of Health Institutional Review Board determined that the study fell within the purview of public health practice and surveillance activities and waived board review.
By focusing on the warm season, HRI surveillance typically captures data on patients with morbidity and mortality that are most likely related to outdoor environmental heat exposure. 26 –28 Thus, we restricted our investigation to Florida residents with HRI during the Florida warm season (May 1 to October 31). 29 For ED patients who were treated and released and for hospitalized patients admitted through the ED, we used the date of the ED visit (rather than the date of hospitalization) as the date of symptom onset. For patients who died, we used the date of injury (instead of the date of death), if available, as the date of symptom onset.
To identify patients with HRI, we used ICD-9-CM codes to search ED and hospital discharge data, and we used codes from the International Classification of Diseases, Tenth Revision (ICD-10) 30 to search mortality data. We defined HRI as occurring when a patient’s record showed (1) the presence of an ICD injury diagnosis code for the effects of heat and light (ICD-9-CM codes 992 or 992.0-992.9 or ICD-10 codes T67 or T67.0-T67.9) in any of the ED or hospital discharge diagnosis fields (ie, primary or secondary diagnoses) or in the fields for cause of death (ie, underlying, contributing, or immediate) and/or (2) the presence of an ICD-9-CM or ICD-10 code for external cause of injury for excessive heat due to weather conditions (E900.0 or X30, respectively), excessive heat due to man-made conditions (E900.1 or W92, respectively), or excessive heat of unspecified origins (E900.9) or ICD-9-CM E900. 10,25,27
We stratified our data by work relatedness. We classified HRI as work related in those aged ≥16 when the expected primary payer for care was workers’ compensation or when the patient’s record specified certain work-related ICD-9-CM codes for external cause of injury (Table 1). 25,31 We classified deaths as work related in those aged ≥16 when the “injury at work” field on their death certificate was marked yes. All HRI patients and deaths not classified as work related were considered to be non–work related.
ICD-9-CM codes and definitions used to identify whether heat-related illnesses in patients were work related during emergency department visits and hospitalizations, Florida, May 1 through October 31, 2005-2012a
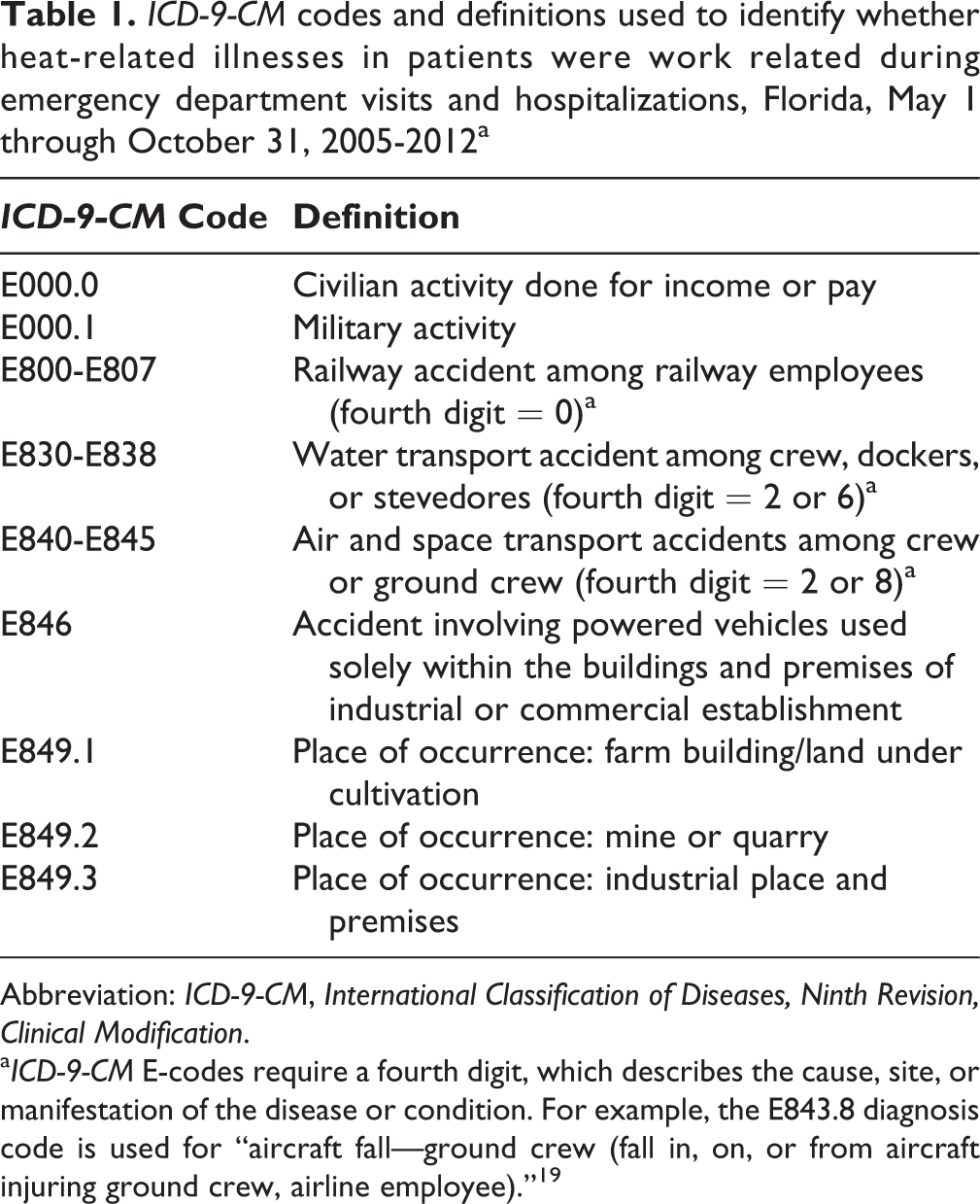
Abbreviation: ICD-9-CM, International Classification of Diseases, Ninth Revision, Clinical Modification.
aICD-9-CM E-codes require a fourth digit, which describes the cause, site, or manifestation of the disease or condition. For example, the E843.8 diagnosis code is used for “aircraft fall—ground crew (fall in, on, or from aircraft injuring ground crew, airline employee).” 19
The records of patients who died with an injury or poisoning are required to contain free-text information, provided by the medical certifier, explaining how the death occurred (eg, specific activity or situation). 32 We reviewed this free-text field in the records of all patients who died with HRI, and we manually summarized the information into the following a posteriori categories: alcohol use, confined in car, exertional, illicit drug use, or other.
Demographic information and descriptive statistics about the study population are published elsewhere. 33 Briefly, males, those in racial/ethnic minority groups, and rural residents had the highest relative rates of HRI. Among patients treated in the ED, those aged 15-35 had the highest rates of work-related and non–work-related HRI. For patients who were hospitalized or died, non–work-related HRI rates increased with age, whereas work-related HRI rates were stable across all ages.
Results
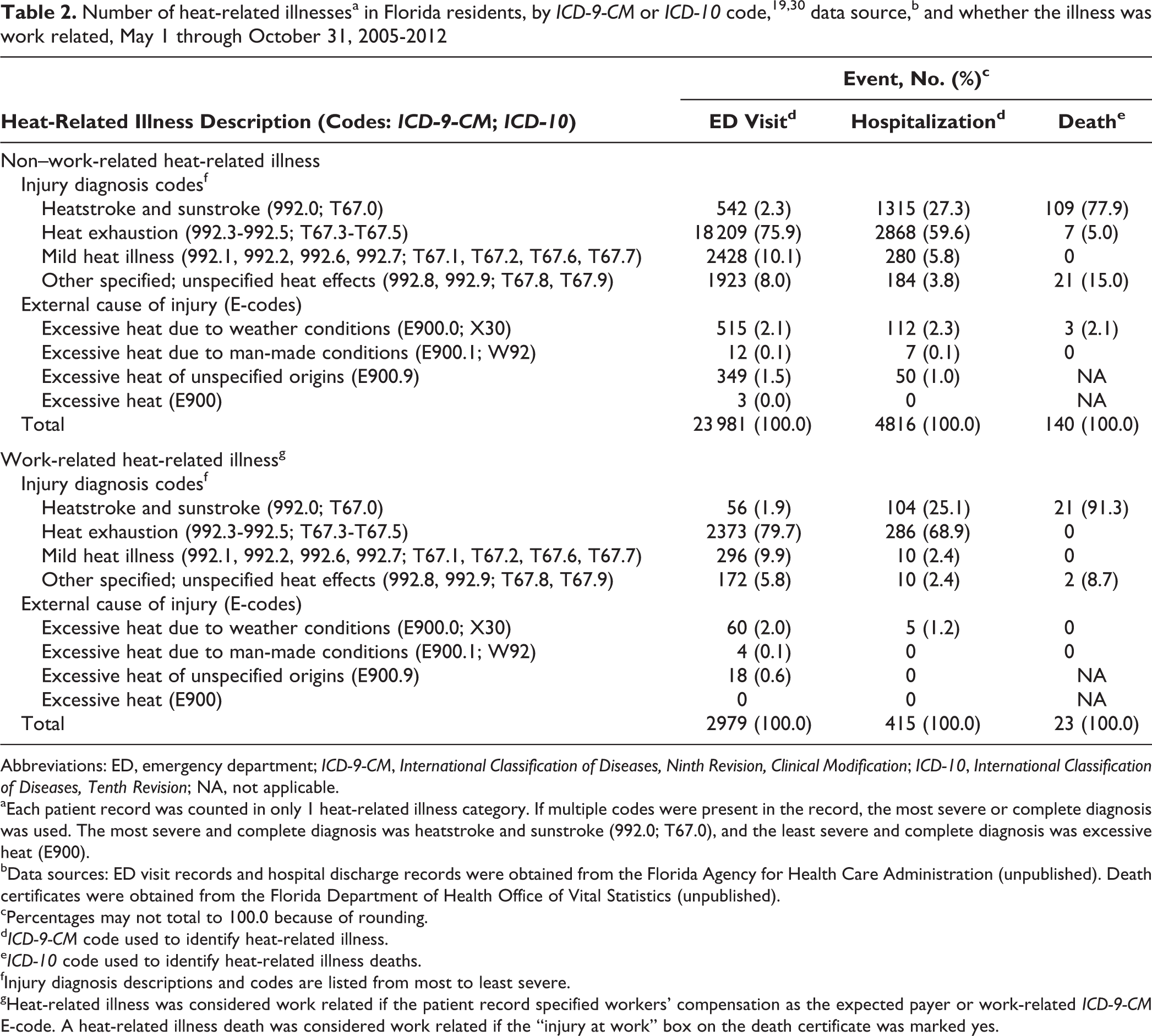
A total of 32 354 patients with HRI were identified in Florida during the warm seasons of 2005 through 2012 (Table 2). Of those, we classified 28 937 as having non–work-related HRI (23 981 from EDs, 4816 from hospitals, and 140 deaths) and 3417 as having work-related HRI (2979 from EDs, 415 from hospitals, and 23 deaths). We identified 911 patients with non–work-related HRI and 82 patients with work-related HRI who were admitted to the hospital via the ED; the mean latencies between ED visits and hospital admissions of these 2 groups were 0.2 days (SD = 0.5, maximum = 4) and 0.1 days (SD = 0.4, maximum = 2), respectively.
Abbreviations: ED, emergency department; ICD-9-CM, International Classification of Diseases, Ninth Revision, Clinical Modification; ICD-10, International Classification of Diseases, Tenth Revision; NA, not applicable.
aEach patient record was counted in only 1 heat-related illness category. If multiple codes were present in the record, the most severe or complete diagnosis was used. The most severe and complete diagnosis was heatstroke and sunstroke (992.0; T67.0), and the least severe and complete diagnosis was excessive heat (E900).
bData sources: ED visit records and hospital discharge records were obtained from the Florida Agency for Health Care Administration (unpublished). Death certificates were obtained from the Florida Department of Health Office of Vital Statistics (unpublished).
cPercentages may not total to 100.0 because of rounding.
dICD-9-CM code used to identify heat-related illness.
eICD-10 code used to identify heat-related illness deaths.
fInjury diagnosis descriptions and codes are listed from most to least severe.
gHeat-related illness was considered work related if the patient record specified workers’ compensation as the expected payer or work-related ICD-9-CM E-code. A heat-related illness death was considered work related if the “injury at work” box on the death certificate was marked yes.
A total of 96 non–work-related HRI and 22 work-related HRI deaths had both the date of injury and the date of death recorded on the death certificate. In these decedents, the mean latency between injury and death was 1.3 days (SD = 3.6, maximum = 22) for those whose HRI deaths were non–work related and 2.5 days (SD = 1.8, maximum = 39) for those whose HRI deaths were work related. There was 1 non–work-related HRI death in which the date of injury occurred between May 1 and October 31, but the date of death occurred outside of this period.
Most patients and deaths in our study were identified by using ICD-9-CM and ICD-10 injury diagnosis codes for HRI (ICD-9-CM codes 992-992.9, ICD-10 codes T67-T67.9). Although we did not use only primary diagnosis codes to identify patients with HRI, we found a primary diagnosis of HRI in 64.9% (15 554 of 23 981) of patients with ED visits for non–work-related HRI and in 42.5% (2046 of 4816) of patients with hospitalizations for non–work-related HRI. Similarly, we found a primary diagnosis of HRI in 75.4% (2245 of 2979) of patients with ED visits for work-related HRI and in 49.6% (206 of 415) of patients with hospitalizations for work-related HRI.
Among the 140 patients who died with non–work-related HRI, the underlying cause of death was excessive heat due to weather conditions (ICD-10 code X30) in 83 (59.3%), excessive heat due to man-made conditions (ICD-10 code W92) in 6 (4.3%), another code for non–heat-related external cause of injury in 21 (15.0%), or a non–heat-related diagnosis code in 30 (21.4%) deaths. Among the 23 patients who died with work-related HRI, the underlying cause of death was excessive heat due to weather conditions in 22 deaths and chronic heart disease in 1 death.
We considered heatstroke and sunstroke (ICD-9-CM code 992.0 or ICD-10 code T67.0) and heat exhaustion (ICD-9-CM codes 992.3-992.5 or ICD-10 codes T67.3-T67.5) to be the most severe forms of HRI. 34 Among patients with non–work-related HRI, 1 of these diagnoses was present in 78.2% (18 751 of 23 981) of ED patients, 86.9% (4183 of 4816) of hospitalized patients, and 82.9% (116 of 140) of those who died. Among patients with work-related HRI, 1 of these diagnoses was present in 81.5% (2429 of 2979) of ED patients, 94.0% (390 of 415) of hospitalized patients, and 91.3% (21 of 23) of those who died (Table 2).
Patients with non–work-related HRI were identified only by an excessive heat code for external cause of injury (ICD-9-CM codes E900, E900.0, E900.1, or E900.9 or ICD-10 codes X30 or W92) in 3.7% (879 of 23 981) of ED visits, 3.5% (169 of 4816) of hospitalizations, and 2.1% (3 of 140) of deaths. Patients with work-related HRI were identified only by a code for an external cause of injury in 2.8% (82 of 2979) of ED visits, 1.2% (5 of 415) of hospitalizations, and no deaths (Table 2).
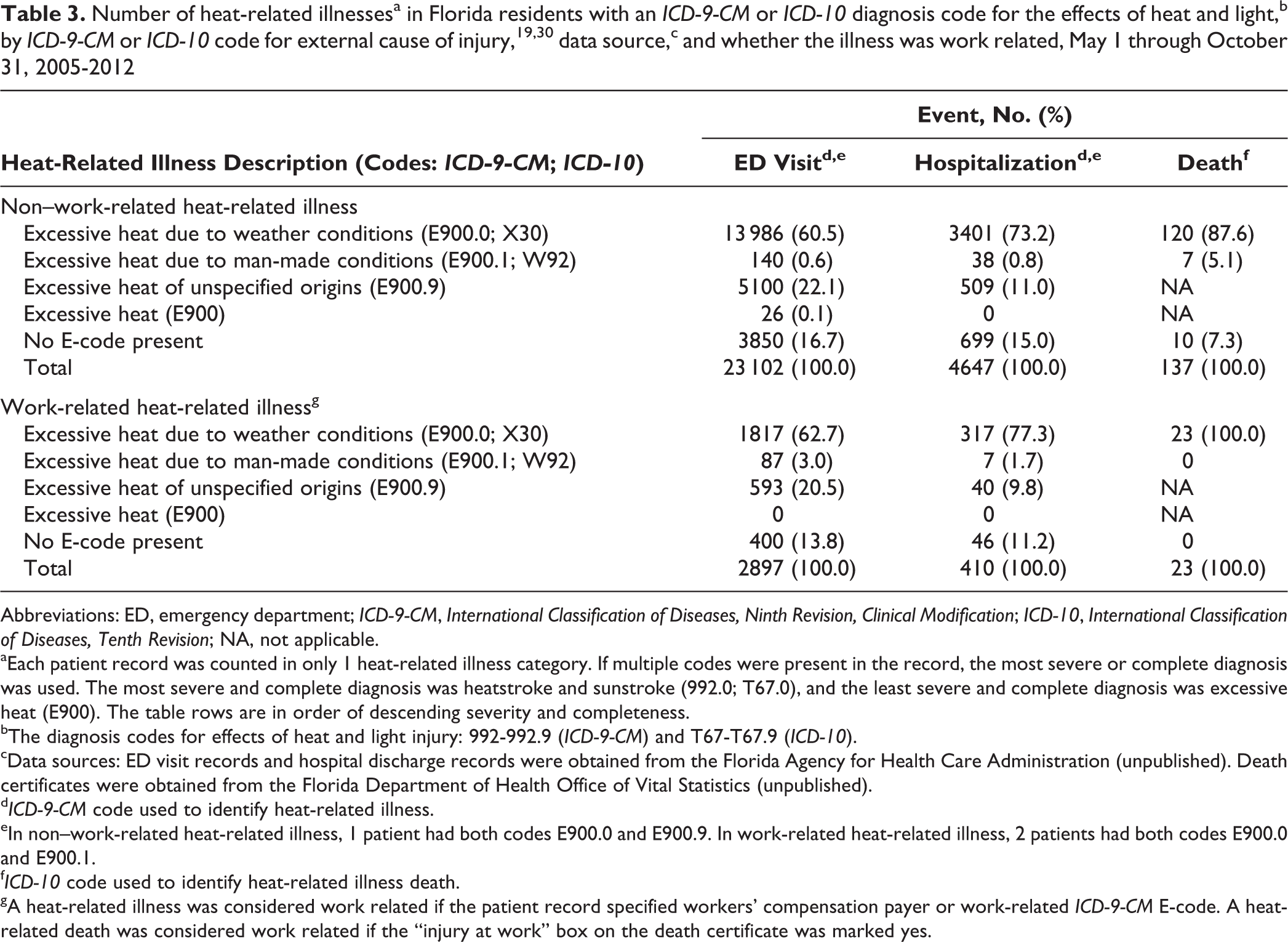
Among non–work-related HRI patients who were identified by using an ICD-9-CM HRI diagnosis code, 16.7% (3850 of 23 102) of ED patients and 15.0% (699 of 4647) of hospitalized patients had no corresponding heat-related code for external cause of injury in their records (Table 3). Of the 137 non–work-related HRI deaths identified by an ICD-10 HRI diagnosis code, 10 (7.3%) had no heat-related code for external cause of injury listed in their records. Among work-related HRI patients who were identified by ICD-9-CM HRI diagnosis codes, 13.8% (400 of 2897) of ED patients and 11.2% (46 of 410) of hospitalized patients had no corresponding heat-related code for external cause of injury in their records. Of the 23 work-related HRI deaths, all had both an ICD-10 diagnosis code and the code for heat-related external cause of injury (X30) listed in their records. Finally, of the 7 patients with non–work-related HRI who died and had the code for external cause of injury W92 (excessive heat due to man-made conditions) in their records, the death certificates indicated that 4 were in a car, 2 were in an attic, and 1 occurred where an air conditioner had been set too high.
Abbreviations: ED, emergency department; ICD-9-CM, International Classification of Diseases, Ninth Revision, Clinical Modification; ICD-10, International Classification of Diseases, Tenth Revision; NA, not applicable.
aEach patient record was counted in only 1 heat-related illness category. If multiple codes were present in the record, the most severe or complete diagnosis was used. The most severe and complete diagnosis was heatstroke and sunstroke (992.0; T67.0), and the least severe and complete diagnosis was excessive heat (E900). The table rows are in order of descending severity and completeness.
bThe diagnosis codes for effects of heat and light injury: 992-992.9 (ICD-9-CM) and T67-T67.9 (ICD-10).
cData sources: ED visit records and hospital discharge records were obtained from the Florida Agency for Health Care Administration (unpublished). Death certificates were obtained from the Florida Department of Health Office of Vital Statistics (unpublished).
dICD-9-CM code used to identify heat-related illness.
eIn non–work-related heat-related illness, 1 patient had both codes E900.0 and E900.9. In work-related heat-related illness, 2 patients had both codes E900.0 and E900.1.
fICD-10 code used to identify heat-related illness death.
gA heat-related illness was considered work related if the patient record specified workers’ compensation payer or work-related ICD-9-CM E-code. A heat-related death was considered work related if the “injury at work” box on the death certificate was marked yes.
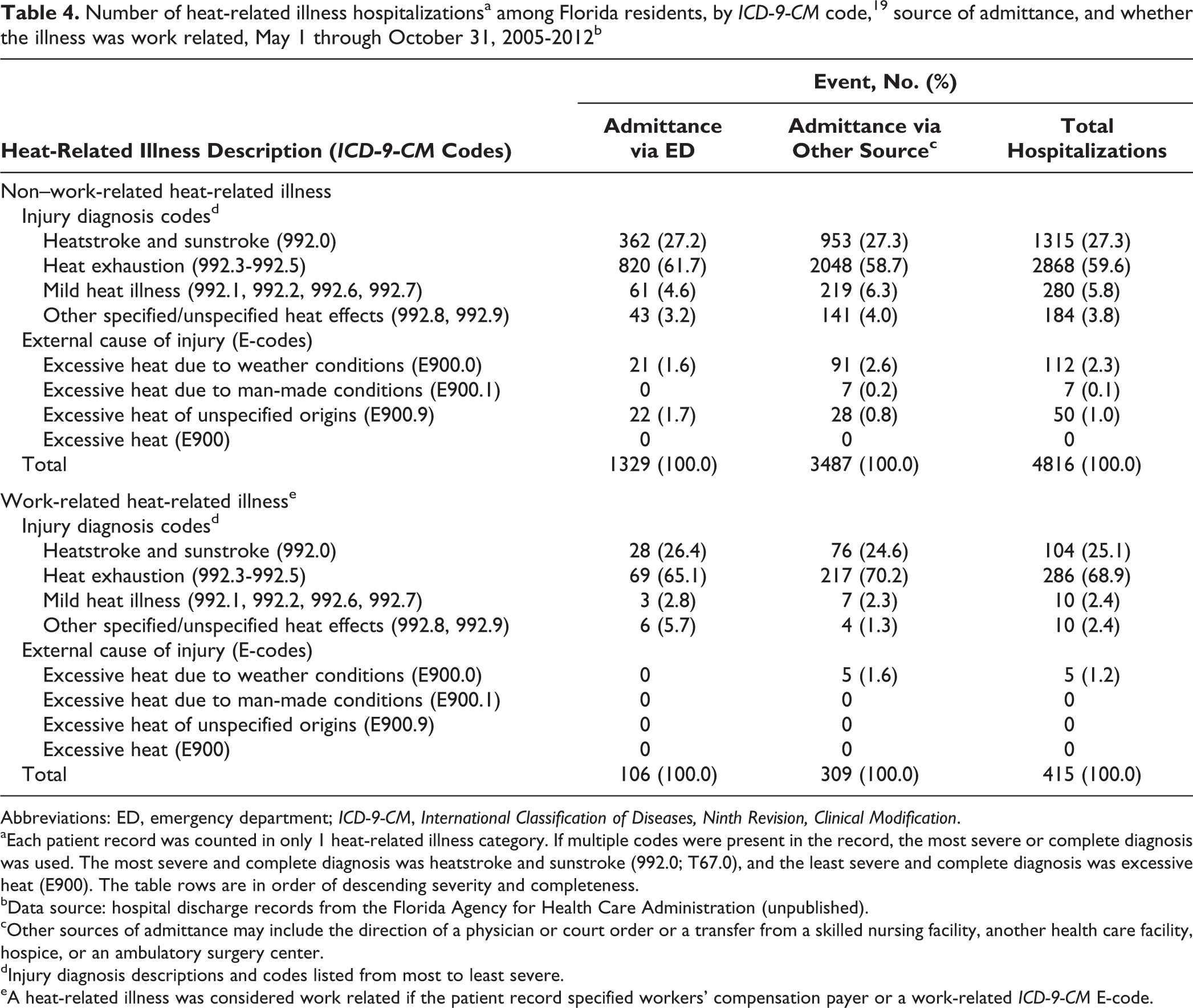
We also looked at proportion of hospitalizations stratified by admittance (Table 4). The distribution of patients was similar except that among HRI patients admitted via the ED, 65.1% (69 of 106) were work-related heat exhaustion, whereas among HRI patients admitted via another source, 70.2% (217 or 309) were work-related heat exhaustion.
Number of heat-related illness hospitalizationsa among Florida residents, by ICD-9-CM code, 19 source of admittance, and whether the illness was work related, May 1 through October 31, 2005-2012b
Abbreviations: ED, emergency department; ICD-9-CM, International Classification of Diseases, Ninth Revision, Clinical Modification.
aEach patient record was counted in only 1 heat-related illness category. If multiple codes were present in the record, the most severe or complete diagnosis was used. The most severe and complete diagnosis was heatstroke and sunstroke (992.0; T67.0), and the least severe and complete diagnosis was excessive heat (E900). The table rows are in order of descending severity and completeness.
bData source: hospital discharge records from the Florida Agency for Health Care Administration (unpublished).
cOther sources of admittance may include the direction of a physician or court order or a transfer from a skilled nursing facility, another health care facility, hospice, or an ambulatory surgery center.
dInjury diagnosis descriptions and codes listed from most to least severe.
eA heat-related illness was considered work related if the patient record specified workers’ compensation payer or a work-related ICD-9-CM E-code.
Discussion
HRI surveillance is often conducted through administrative morbidity data sets and death certificates. However, an HRI diagnosis identifies patients with heat exposure, but it does not capture all HRI patients. Records often list the presenting symptom or condition of HRI (eg, myocardial infarction event) or the chronic condition exacerbated by HRI. 13,35 To improve heat-related surveillance, it is essential to increase the identification of HRI patients.
HRI that was diagnosed in approximately 33% of ED visits, 56% of hospitalizations, and 31% of deaths would have been missed by our analysis if only the primary diagnosis (or underlying cause) field was queried. Furthermore, although administrative data sets (eg, ED or hospital discharge records) often include ICD codes in ordered diagnosis fields, syndromic surveillance system (near real-time surveillance) data sets that include ICD codes do not always contain a diagnosis order. Therefore, we agree with others who have noted that to capture data on as many patients with HRI as possible, HRI ICD codes should be collected from all fields indicating diagnosis (primary/secondary) and cause of death (underlying, immediate, or contributing). 21,36,37
We observed that the severity of HRI varied by data source. For example, heatstroke was identified in the death certificates of most patients who died of HRI (77.9%-91.3%), but it was noted in the records of few HRI-related ED visits (1.9%-2.3%). This finding is consistent with the fact that heatstroke is considered one of the most severe forms of HRI 34 and that patients with heatstroke may be more likely to be admitted from the ED to the hospital rather than treated and released. 21,22
In addition to the variation in HRI severity by data source, for the morbidity data sets, ≤10% of patients were diagnosed with mild HRI. These findings indicate that the full burden of HRI may not be captured and that the data (ie, ED visit and hospital discharge records) most likely include only those patients whose HRI is severe enough to require immediate medical attention. Consequently, when conducting HRI surveillance, public health professionals should consider using multiple data sources to capture the full spectrum of HRI severity, including nontraditional data sources, such as records from urgent care facilities.
A small but important proportion of patients and deaths (up to 3.7%) with HRI were identified only by their heat-related code for external cause of injury. The number of HRI patients identified by a code for external cause of injury may be due to Florida regulations mandating that codes for external cause of injury be reported by all health care facilities. 38 It may also have been related to the high rates of compliance with this regulation in Florida. Between 2007 and 2012, 95% to 98% of all nonfatal injury ED visits and hospital discharge records had a code for external cause of injury. 39 Furthermore, the 3 available fields for external cause of injury in the Florida ED and hospital discharge data allowed for separate characterization of the injury mechanism, intent, location, and activity. For injury-related deaths, a code for external cause of injury (rather than an ICD-10 injury diagnosis code) should be recorded as the underlying cause of death on the death certificate. 40 However, 7% of death certificates among Florida residents had an HRI diagnosis code but no corresponding heat-related code for external cause of injury. Nevertheless, it may not be possible to generalize our results to all jurisdictions, because the completeness, accuracy, and specificity of code for external cause of injury reporting vary by state. 38 Still, although the magnitude of improvement will vary by jurisdiction, the additional use of ICD codes for external cause of injury for HRI surveillance should increase the number of patients identified with HRI. During the assignment of codes in administrative data, the use of specific and multiple codes for external cause of injury should be encouraged. 41
We elected to include the ICD code for external cause of injury for excessive heat due to man-made conditions (E900.1 from ICD-9-CM and W92 from ICD-10) in our analysis. When HRI surveillance is conducted, these codes are not often included or are even used by some jurisdictions as exclusion criteria. 21,27,28,42 It has been argued that the purpose of HRI surveillance is to track patients affected by or deaths caused by outdoor environmental heat exposure rather than those exposed to indoor heat in areas such as boiler rooms, kitchens, or factories. 19,21 However, indoor temperature has been positively correlated with outdoor temperature. 43 –45 In addition, previous studies of workers in aluminum smelters or underground mining facilities reported more adverse heat-related outcomes as outdoor temperature increased. 46 –48 Others have reported that when indoor work environments were not cooled or ventilated properly, the outdoor ambient temperature added considerably to the level of indoor heat. 1 Moreover, according to the ICD-9-CM manual, the code for excessive heat due to man-made conditions includes excessive heat generated in transport vehicles. 19 As such, this code might reasonably be applied, for example, to those with an HRI as a result of being trapped in a vehicle during periods of high outdoor temperatures. Finally, when we examined free-text notes associated with the code W92 on death certificates of patients in our study, 6 of the 7 deaths reported the presence of heat exposure exacerbated by outdoor environmental heat.
Taken together, the previous arguments support inclusion of the codes E900.1 and W92 for HRI surveillance. Nevertheless, at most, 0.1% of the patients in our study were identified as having HRI solely through the use of 1 of these 2 codes. However, we determined that if we had used these 2 codes instead as exclusion criteria, 5.0% of patients with non–work-related HRI deaths, 3.0% of patients with work-related HRI ED visits, and 1.7% of work-related HRI hospitalizations would have been removed. Because the use of codes for external cause of injury in HRI surveillance varies by jurisdiction, the additional proportion of patients with HRI that would potentially be captured by including these codes (or by not using them as exclusion criteria) may vary. 38 Given the findings in this study, we recommend that, at a minimum, codes E900.1 and W92 not be used as exclusion criteria for HRI surveillance. Furthermore, we also suggest that the use of these codes be strongly considered as a way to potentially increase the sensitivity of HRI surveillance.
In our data, as typical of administrative data sets, the exact timing of injury (ie, HRI onset) was unknown, leading to varying degrees of bias in the timing of injury. 49,50 For data on ED visits and hospitalizations, we inferred that the date closest to symptom onset was the date of the ED visit. Patients admitted to the hospital via the ED may not always be admitted the same day; instead, prior to hospital admission, patients may be placed on observation status. 51 The date with the potential to be furthest from symptom onset is the date of death. An extreme example from our data was the decedent who was hospitalized for >1 month before death. Although the date of injury is required to be noted on the death certificate for injury-related deaths, 32 we found that it was not always done. To reduce the bias in the timing of HRI onset, if available, it is recommended that the ED visit date or the date of injury be used for hospitalizations and deaths, respectively.
Our HRI morbidity surveillance used ICD-9-CM codes, but in October 2015, the US coding system shifted to the International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM). The ICD-9-CM codes used in this analysis all have corresponding ICD-10-CM codes (Table 5). 52 It is currently unclear how the switch to ICD-10-CM will affect HRI surveillance. In ICD-10-CM, 2 potential HRI codes were not available in ICD-9-CM. Additionally, for each heat-related ICD-10-CM code, the seventh character indicates the encounter: initial, subsequent, sequela. 53 In the case of sequela, in ICD-9-CM, a sequela code for external cause of injury (ie, E929.5, late effects of accident due to natural and environmental factors) would have been required in conjunction with the injury diagnosis. 19 However, many morbidity systems may only have 1 external cause of injury field. As a result, HRI diagnoses may not have been coded as sequela. It is recommended that future studies examine (1) how HRI surveillance based on ICD-10-CM codes varies among and within jurisdictions, (2) how the seventh character is being assigned and its impact on HRI surveillance, and (3) how the proportion of patients identified by each ICD-9-CM or ICD-10-CM HRI code may affect HRI time trends.
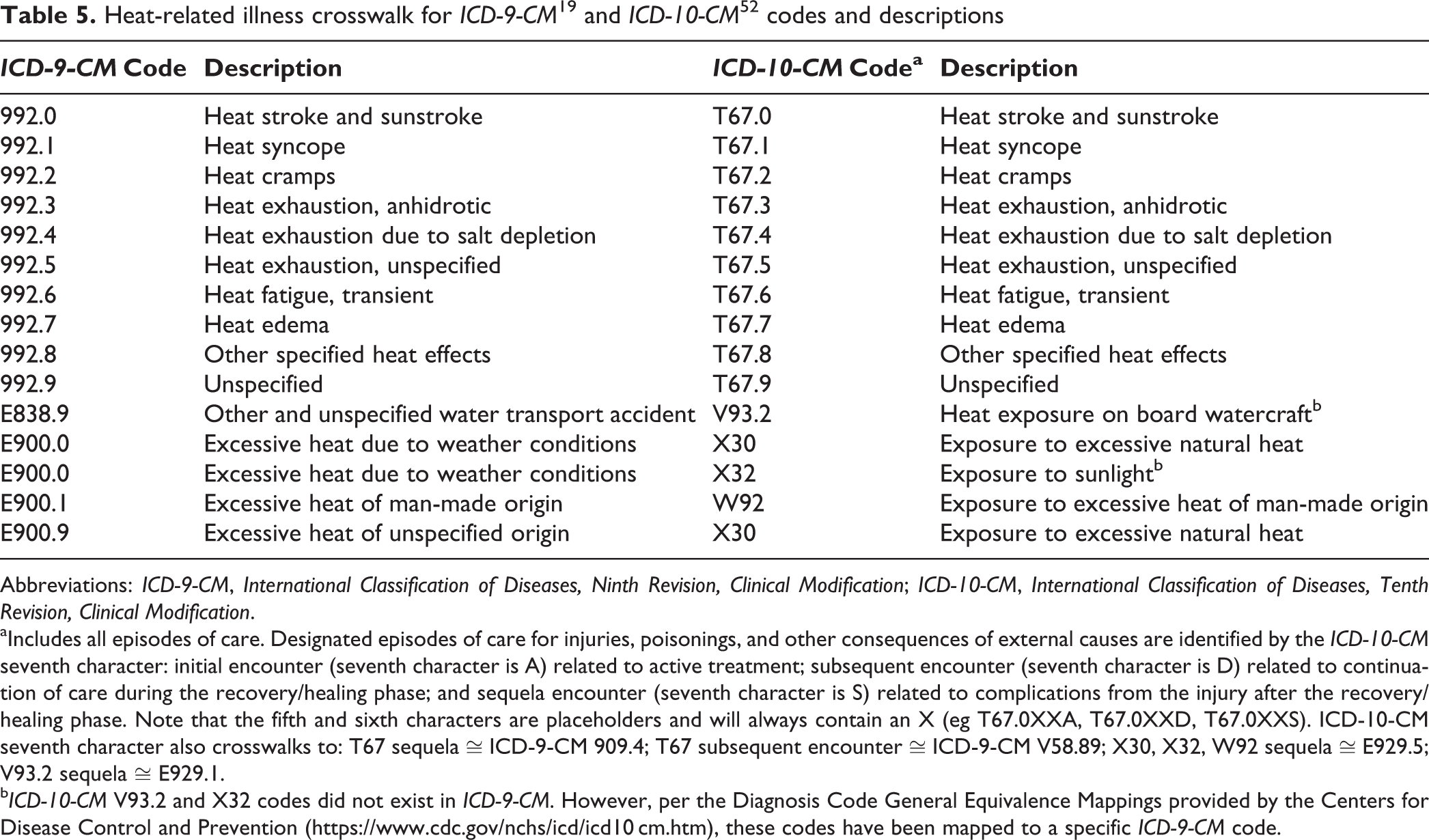
Abbreviations: ICD-9-CM, International Classification of Diseases, Ninth Revision, Clinical Modification; ICD-10-CM, International Classification of Diseases, Tenth Revision, Clinical Modification.
aIncludes all episodes of care. Designated episodes of care for injuries, poisonings, and other consequences of external causes are identified by the ICD-10-CM seventh character: initial encounter (seventh character is A) related to active treatment; subsequent encounter (seventh character is D) related to continuation of care during the recovery/healing phase; and sequela encounter (seventh character is S) related to complications from the injury after the recovery/healing phase. Note that the fifth and sixth characters are placeholders and will always contain an X (eg T67.0XXA, T67.0XXD, T67.0XXS). ICD-10-CM seventh character also crosswalks to: T67 sequela ≅ ICD-9-CM 909.4; T67 subsequent encounter ≅ ICD-9-CM V58.89; X30, X32, W92 sequela ≅ E929.5; V93.2 sequela ≅ E929.1.
bICD-10-CM V93.2 and X32 codes did not exist in ICD-9-CM. However, per the Diagnosis Code General Equivalence Mappings provided by the Centers for Disease Control and Prevention (https://www.cdc.gov/nchs/icd/icd10 cm.htm), these codes have been mapped to a specific ICD-9-CM code.
Limitations
This study had several limitations. First, restricting the study to warmer months (May 1 to October 31) may have underestimated the number of patients who had HRI. Second, our study focused on HRI from outdoor environmental heat exposure. Even by restricting our investigation to the warm season, some patients identified with HRI may not have had this exposure. For example, 2 deaths in our study were in patients who developed HRI from being in saunas. Similarly, a publication from Maricopa County, Arizona, reported on 3 patients during the summers of 2009-2012 who died of HRI from being in excessively hot bath water. 53 Third, although using ICD-9-CM codes in HRI surveillance is helpful, these codes are designed to be used for billing purposes rather than surveillance purposes. Additionally, the choice of codes is subjective and may vary by medical provider and facility, which could introduce bias or inconsistency. Fourth, we used the identification of payer equal to workers’ compensation to determine work-related and non–work-related HRI. However, others have reported that workers’ compensation coverage is generally underused 25 ; as such, we may have underestimated the number of patients with work-related HRI. We attempted to minimize this underestimation by using various work-related codes for external cause of injury.
Conclusions
Our results support the use of multiple data sources, all relevant data fields (including primary and secondary diagnoses, as well as underlying and contributing cause of death), and specific ICD injury diagnosis and codes for external cause of injury to improve HRI surveillance sensitivity. Our findings also suggest that codes E900.1 and W92 should not be used as exclusion criteria. This study of Florida HRI data could be used to help public health practitioners in other jurisdictions improve their heat-related surveillance systems and make them aware of the components and limitations of their current systems. We recommend evaluating the impact of the recent conversion from ICD-9-CM to ICD-10-CM codes on HRI surveillance of ED visits and hospitalizations.
Footnotes
Acknowledgments
We thank Kristina Kintziger and Meredith Jagger for their support, technical input, and review of this manuscript and Melissa Jordan for her assistance in obtaining the data.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded in part by a training grant from the National Institute of Environmental Health Sciences (T32 ES007018); by the North Carolina Occupational Safety and Health and Education and Research Center, National Institute for Occupational Safety and Health (5T42OH008673-09); and by the National Center for Environmental Health, Centers for Disease Control and Prevention (project 5UE1EH001047-03).