
Abstract
Exertional heat illness can be a serious consequence of sports or exercise in hot environments. Participants can possess intrinsic or face extrinsic risk factors that may increase their risk for heat-related illness. Knowledge of the physiology and pathology of heat illness, identification of risk factors, and strategies to combat heat accumulation will aid both the practitioner and the participant in preparing for activities that occur in hot environments. Through preparation and mitigation of risk, safe and enjoyable wilderness adventure can be pursued.
Introduction
The ultimate goal of the preparticipation examination is to allow for safe participation in sport and exercise and to screen for predisposing factors that could place individuals at further risk. The preparticipation exam for wilderness and adventure athletes should include specific questions regarding exposure to hot ambient conditions. Of particular interest is history of exertional heat illnesses (EHI), as this is a strong predictor of future EHI. Asking encompassing questions regarding a variety of wilderness athlete-specific circumstances is crucial in ensuring safe athletic participation.
Physical activity and exercise can typically be performed in hot environments without injury; however, individuals who participate in wilderness and outdoor adventure sports are often exposed to variable and prolonged extreme weather conditions, including heat. Individuals exposed to hot ambient conditions for extended periods of time, such as ultraendurance athletes and wilderness hikers, have an increased likelihood of suffering heat-related injuries due to extended periods of time with high internal body temperature. These injuries can range from benign conditions such as heat edema and heat cramps to potentially fatal conditions such as exertional heat stroke (EHS). Definitions1,2 are as follows: Heat edema: extremity swelling caused by peripheral vasodilation and interstitial pooling Heat cramps: exercise-associated muscle spasms during or immediately after exercise Heat syncope: a transient loss of consciousness due to pooling of blood in the extremities usually after ending exercise suddenly Heat exhaustion: the inability to continue exercise in heat due to exertional heat stress and low central blood volume impairing heat dissipation Exertional heat stroke: extreme exercise-induced hyperthermia, thermoregulatory failure, and profound central nervous system dysfunction
The majority of EHI can be prevented with education, preparation, and purposeful adjustment to hot conditions. Identifying modifiable factors that contribute to heat injuries such as hydration status, wearing improper, excessive or heavy clothing, and sleep loss can assist with prevention. Athletes should be educated to recognize early signs and symptoms of heat illnesses such as fatigue, cramps, nausea, and dizziness so that they may take steps to prevent worsening such as increasing rest intervals, seeking shade, ensuring proper hydration, and decreasing activity intensity.
Methods
Multiagency position statements, consensus guidelines, and textbooks as well as the references cited in those documents/texts were reviewed for use in this article. Where possible, the best available evidence was used.
Physiology
Although the human body has remarkable resilience against cold, it can tolerate only minor temperature elevations (9°F) before developing systemic dysfunction, which eventually leads to multiorgan failure and death if body temperature cannot be lowered. The human body has multiple mechanisms to dissipate heat
3
: Evaporation occurs when water vaporizes from the skin and respiratory tract. This is the body’s most effective mechanism for dissipating excess heat and is the primary means for athletes exercising in hot environments. Radiation is the emission of electromagnetic heat waves. This energy transfer does not require direct contact or air motion. Convection is the transfer of heat to a gas or liquid moving over the body. Heat dissipation occurs when the gas or liquid is cooler than the body and is especially important to athletes through circulating air, the speed of air circulation, and the amount of body surface area exposed. Conduction is direct heat transfer to an adjacent cooler object.
During exercise, the human body dissipates excess heat generated by the skeletal muscle. This requires an intact cardiovascular system that uses blood to transfer heat from the body core to the skin, where the mechanisms for dissipating heat can take effect. However, when the ambient temperature is higher than the body’s internal temperature, convection, conduction, and radiation are no longer effective. Environmental conditions also can affect evaporative cooling. A water vapor pressure gradient must exist for sweat to evaporate and release heat into the environment. In high humidity (relative humidity >75%), evaporation becomes ineffective for transferring heat. Thus, in hot and humid conditions, athletes become susceptible to EHI.
Limitations of heat dissipation in hot and humid weather are exacerbated during intense exercise by a finite supply of blood that must fulfill multiple functions, including meeting metabolic demands of active skeletal muscle and transporting heat to the skin surface for cooling. Dehydration that develops in individuals during intense exercise in the heat further complicates matters by decreasing plasma volume. Studies suggest that during intense exercise in the heat, for every 1 percent of body mass lost from dehydration, there is a concomitant increase in core body temperature of 0.21°C (0.4°F). 4 –7 A number of additional factors influence the rate at which a person’s internal body temperature rises during vigorous activity including fitness level, hydration status, degree of heat acclimatization, clothing/equipment, and physiologic responses (eg, degree of tachycardia). 8
Heat stress refers to the environmental and host conditions that increase body temperature, whereas heat strain is the physiological and psychological consequence of heat stress. Heat stress is further categorized as compensable or uncompensable. During exercise, body temperature elevates in response to an increase in metabolic heat production. A modest rise in temperature is thought to represent a favorable adjustment that optimizes physiologic functions to mobilize cooling mechanisms. With compensable heat stress, the body achieves a new steady-state internal temperature that is proportional to the increased metabolic rate and available means for dissipating heat. Uncompensable heat stress results when cooling capacity is exceeded and the athlete cannot maintain a steady temperature. 8 Continued exertion in the setting of uncompensable heat stress increases heat retention, causing a progressive rise in internal body temperature and increasing the risk for severe heat illnesses.
Acclimatization is the body’s ability to improve its response and tolerance of heat stress over time, and it is the most important factor that determines how well an athlete withstands extreme heat.
2
Thus, allowing sufficient time and using optimal training strategies that enable athletes to acclimatize are critical for improving performance and mitigating the risk for EHI. Observational studies have found that the first week of athletic practice in high heat and humidity is the period of greatest risk for developing EHI.
9
Full acclimatization requires at least 10 to 14 days of exercise at an intensity that raises body temperature to at least 38.5°C for at least 60 minutes.
10
This can be accomplished in either hot environmental conditions or cooler conditions if clothing or equipment is worn and exercise intensity is high. However, any improved tolerance of heat stress generally dissipates within 2 to 3 weeks of returning to a more temperate environment.10,11 The major physiologic adjustments that occur during heat and humidity acclimatization include
10
Plasma volume expansion Improved cutaneous blood flow Lower threshold for initiation of sweating Increased sweat output Lower salt concentration in sweat Lower skin and core temperatures for a standard exercise
These adaptations allow for better dissipation of heat during exercise and limit increases in body temperature compared with athletes who have not acclimatized. Unlike with traditional sports such as football practice in late summer, many wilderness and adventure athletes reside and train in variable outdoor and mountain conditions, making consistent heat exposure in training more challenging.
Risk Factors
Understanding an individual’s risk factors for EHI can help athletes and medical professionals anticipate challenges and prepare for specific medical conditions that place individuals at risk during exercise. Risk factors for EHI can be broken down into 4 broad categories: individual factors, environmental factors, medication and drug use, and chronic conditions (Figure 1).
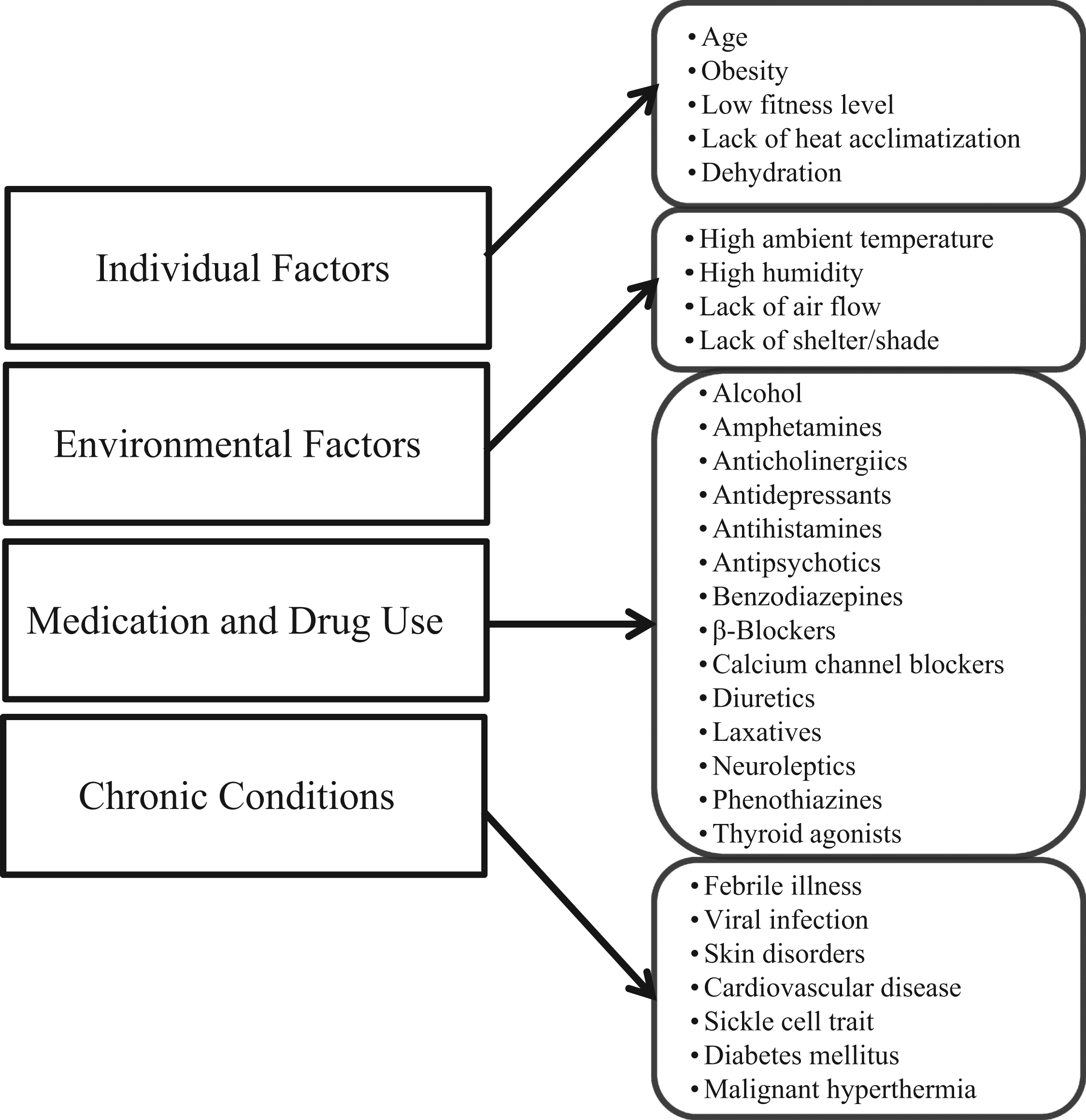
Individual and environmental predisposing factors to exertional heat illnesses.
Individual risk factors such as personal medical history should be screened first, as the greatest risk of future EHI is a history of previous heat illness. 12 Patients who are elderly, young, obese, or have been previously affected by EHI are at higher risk of these conditions due to dysregulation of thermoregulatory factors. 12 –15 Sweat mechanisms change with age which decreases sweat rate, lowering one’s evaporative capacity. 16 Those who are less physically trained or of lower physical fitness are also more likely to suffer from EHI due to completing similar absolute work, resulting in a greater relative workload compared with trained individuals, and possibly due to excessive sodium loss.14,17 This has been demonstrated in unfit and overweight Marine Corps recruits who were at an 8-fold higher risk of EHI compared with their leaner more aerobically fit counterparts. 17 Other factors such as concurrent dehydration and lack of proper heat acclimatization also place athletes at an increased risk of developing EHI. 2 Direct sun exposure, especially in high altitude and mountain environments, can be intense and may contribute to heat illness.
The environment in which athletes exercise can provide challenges. Hot environmental conditions decrease the gradient between the skin and air, decreasing heat transfer to the environment. High humidity also decreases heat transfer through evaporation that mitigates heat dissipation. The calculation of wet-bulb globe temperature (WBGT) can be useful in helping to predict the risk of heat-related illness. 2 The WBGT is calculated based on air temperature, humidity, and radiant energy indicated through black globe temperature to holistically determine heat stress placed upon the body. As suggested by many organizations including the American College of Sports Medicine and National Athletic Trainers’ Association, work to rest ratios should be modified or physical activity should be canceled as WBGT increases.2,18 Other environmental factors include the lack of shade, shelter, or air movement.
Medication and drug use can put patients at increased risk of developing EHI. Alcohol and some commonly used medications (eg, diuretics, laxatives) can contribute to dehydration, in turn increasing body temperature during exercise. 12 Other drugs listed in Figure 1 may affect the athlete by either increasing heat production or compromising thermoregulation. 12
Certain illnesses can cause increased risk of EHI such as any febrile illness or conditions that affect the skin and alter thermoregulation. 19 For example, sun burns can decrease the amount of sweat produced and therefore evaporate and alter sodium losses through sweat. This can be seen up to 21 days after the initial burn, leading to difficulty in dissipating metabolic heat. 20 Other medical conditions that alter one’s thermoregulatory capacity include uncontrolled diabetes, hypertension, thyroid disorder, sleep deprivation, and eating disorders. 14 Acute gastrointestinal distress during endurance, ultraendurance, and adventure events can contribute to dehydration by impairing the athlete’s ability to consume fluids in appropriate volumes and at regular intervals.
Environmental Challenges
Individuals who partake in physical activities from leisure to multiday wilderness adventure sports are potentially at greater risk of heat-related illness when participating in warm to hot ambient environments. Independent of previously mentioned EHI risk factors (Figure 1), there are many other aspects that need to be considered while preplanning for outdoor activities. These include fitness level, heat acclimatization, length and number of rest breaks, shade opportunities, protection from sun (ie, clothing and sunscreen), terrain changes resulting in moderate to extreme exertion, amount of water carried, access to potable water or the ability to filter water for hydration, physical limitations, and mental preparation for participation in austere/remote environments.
Take for example one unique environmental challenge, hiking in the Grand Canyon. During the months of April to September, approximately 400 000 individuals day hike into the canyon down long, steep terrain. 21 A seemingly easy 2-hour hike down the canyon becomes an extremely exhausting 4-hour hike coming back up the trail, with many individuals unprepared physically and mentally for the level of exertion and duration required, leading to EHI or the exacerbation of an existing medical condition. Additionally, 190 000 hikers conduct overnight camping below the rim near the river, taking 4 to 5 hours to reach their campsite. On a subsequent day, it takes approximately 8 hours to return back up the steep terrain. Summer month temperatures can exceed 100°F at the canyon rim to over 120°F at the canyon bottom. 21 Thus, EHI span the breath from mild to life threatening including EHS, exercise-associated hyponatremia, acute renal failure, rhabdomyolysis, disseminated intravascular coagulation, and death. 22 Due to the remote environment and extreme terrain, park Emergency Medical Services personnel frequently conduct high-risk patient ground and air evacuations at all locations in the Canyon.
This example of an environmental challenge is intensified during warmer times of the year, which accelerates EHI across all age groups and genders. The typical profile is middle-aged individuals with cardiovascular risk factors who presents with signs and symptoms of heat exhaustion. Consequently, whether it is in the Grand Canyon or other austere locations, exposure to extreme heat as an environmental challenge is a much expanding national problem as the increasing population, at all age groups, seeks to be physical active in these environments.
Preparticipation Examination
Clinicians should consider adopting a standardized preparticipation evaluation (PPE) that ensures safe participation in warm to hot ambient temperature environments. During the PPE, the physician should assess the patient for any recent or current medical conditions (eg, pertinent history, significant risk factors, or specific history of EHI) that might predispose to EHI or sudden death or become exacerbated with acute or chronic high ambient temperature exposure. 23 The clinician needs to perform a careful individualized assessment that addresses history of previous EHI and known risk factors (Figure 1) and comorbidities. Athletes with medical comorbidities require careful individual assessment relative to how heat stress may affect underlying illness. In general, recommendations and mitigation strategies follow preparticipation guidelines for the individual comorbidities and EHI prevention strategies.17,18
Wilderness athletes with a history of a previous EHI, in particular heat stroke, present a special challenge as they may be at increased risk for a future event. If the illness was caused by extrinsic risk factors such as a lack of acclimatization, poor hydration strategies, infection, or fatigue, participation may be permitted with an appropriate risk mitigation strategy. However, if the event was associated with an intrinsic risk factor such as a skin disorder or medication and the risk factor is not modifiable, consideration should be given for limited or tailored participation. Wilderness athletes who sustained single or multiple previous significant EHI events without an obvious cause should be considered for further evaluation by a provider with expertise in heat illness and participation should be restricted until evaluation is complete. Further testing in these instances may involve heat tolerance testing.
The physical examination should include a general assessment of age, gender, and percent body fat as these are known to affect exercising heat tolerance. It should also include the cardiovascular, respiratory, and integumentary systems; thyroid; peripheral pulses; and sensation. Cardiac stress testing should be considered for at-risk individuals. 24
All individuals with a previous EHI do not need to be restricted from future activity in hot ambient conditions. Consideration should be given to environmental conditions (eg, high ambient temperature, high humidity, wind velocity), duration (eg, hours to days), individual, group or team sport activities (eg, camping, hiking, mountain biking, team event), and physical intensity of activities (eg, passive, low, moderate to high intensity) that will be undertaken by the individual. These targeted questions (Table 1) can help guide physicians to determine level of risk and also lead to EHI prevention and physical activity risk mitigation strategies.
Example preparticipation examination medical history questions 23
Return to Activities In Heat
Many times adventurers or athletes will seek to return to hot weather activities after sustaining a heat injury. Return to activities in moderate to high heat environments after EHI can be complex, and the final decision is most commonly concluded with the clinician’s final recommendations for safe participation. These recommendations range from permitting full activity with standard precautions, permitting limited activity with appropriate restrictions, and finally, recommending restriction from participation. These assessments are highly individualized and require a systematic and integrated analysis by the recommending provider of the individual, with his/her intrinsic and extrinsic risk factors, external environmental challenges, intensity and duration of exercise, and the availability of countermeasures (eg, access to fluids, shelter, medical support) to mitigate risk. It is important to note that the wilderness environment presents unique environmental challenges where underestimating risk and the inability to execute countermeasures, and sometimes extrication measures, can result in significant morbidity and mortality to the individual, and potentially the team.
Several guidelines are available to return individuals to physical activity after a diagnosis of heat intolerance.25,26 Although these guidelines are not comprehensive, most are considered common sense recommendations that require the patient to be without symptoms with normal laboratory parameters before cautious controlled reintroduction to physical activity. The decision-making process ultimately requires a fundamental understanding of both the pathophysiology of the underlying disorder and the recovery process. Exertional heat stroke is challenging because of the incomplete understanding of the pathophysiological processes involved in the development of and recovery from this disorder. 26 Most individuals recover completely from EHS within a week when prompt and effective treatment is initiated to lower internal body temperature, but patients who received inappropriate care may have long-term complications of multiple organ systems and neurological sequelae, resulting in subsequent reduced exercise capacity and heat intolerance. Some individuals affected by EHS may be permanently affected by impaired thermoregulation, even after the proper initial treatment27–28 (Table 2) provides guidelines from the ACSM to return individuals to physical activity after EHS. 25
Screening guidelines for individuals returning to physical activity following heat stroke 18
Prevention of future EHI in individuals predisposed to thermal intolerance is critical for wilderness and adventure athletes. Arguably the most important aspect of prevention is executing heat acclimatization before activity in a harsh climate. If traveling from a cool environment, ideally travel is well in advance to the location of the intended event to optimize thermoregulatory function for the warm environment. This is more easily accomplished in consistently hot adventure environments such as the desert opposed to variable weather environments such as in the mountains or at high altitude. Another EHI prevention strategy for an individual is knowledge of the environment. The WGBT assessment allows individuals to assess daily risk of EHI events, with risk increasing as WBGT increases. Additional critical environmental information includes altitude, which may compound solar radiation and additionally stress the cardiovascular system, and the availability of shade and water.
As EHI has been strongly associated with heat accumulation over several days, knowledge of the availability of air-conditioned facilities and running cooling water for periodic “heat dumping” is important. 29 During ultraendurance events and multiday exposures, simple advice such as “seek the shade” during participation and rest breaks (eg, tree cover or shade on one side of a trail or road) can reduce the cumulative effects to heat, even for intermittent short periods of time. Occasional partial submersion, a quick dip, or dousing the head or head band in a cool stream or mountain like may help reduce heat stress and can provide and often-needed psychological boost. Knowledge of the environment and terrain will allow the provider to execute an appropriate work-rest-hydration intervention. Other prevention methods include executing a good buddy system, carrying a rectal thermometer to assess potential EHS in the field, and identifying emergency resources to execute an emergency action plan. The plan should identify a mechanism for potential emergency cooling on site and an evacuation plan to the nearest medical facility for further management.
Summary and Conclusions
Exertional heat illnesses can occur in many environmental conditions but are most common with sustained extreme heat and humidity exposure. Wilderness athletes are faced with various unique challenges in their sports and adventures, especially in regard to extreme environmental conditions for intermittent and extended periods of time. Heat illnesses are commonly seen in adventure races, rock climbing, hiking, cycling races, and ultraendurance road races, which are all becoming more popular. Preparticipation evaluation and screening allows for identification of at-risk individuals, provides the opportunity for intervention and education, and helps establish a safe and successful athletic participation.
Preparing for exercise in hot environmental conditions can mitigate the risk of developing EHI. This includes planning rest and hydration breaks based on terrain, carrying or ensuring access (eg, natural water sources or aid stations) to an appropriate amount of water to maintain proper hydration, undergoing a heat acclimatization protocol before competition, considering heat stress testing or staged exposure as needed, and having an emergency action plan for emergency situations such as EHS. Implementing a comprehensive PPE and prevention strategies allows for the greatest prospect for safe participation in hot climates.
Footnotes
☆
B. L. Bennett is a board member and paid invited speaker for the Wilderness Medical Society. The remaining authors report no conflicts of interest.This article appears in a “Care of the Wilderness and Adventure Athlete” special issue, jointly published by Clinical Journal of Sport Medicine and Wilderness & Environmental Medicine.