
Abstract
Objectives
Maricopa County, Arizona (2017 population about 4.3 million), is located in the Sonoran Desert. In 2005, the Maricopa County Department of Public Health (MCDPH) established a heat-associated mortality surveillance system that captures data on circumstances of death for Maricopa County residents and visitors. We analyzed 2006-2016 surveillance system data to understand the characteristics and circumstances of heat-associated deaths.
Methods
We classified heat-associated deaths based on International Classification of Diseases, Tenth Revision codes (X30, T67.X, and P81.0) and phrases (heat exposure, environ, exhaustion, sun, heat stress, heat stroke, or hyperthermia) in part I or part II of the death certificate. We summarized data on decedents’ demographic characteristics, years lived in Arizona, location of death (indoors vs outdoors), presence and functionality of air conditioning, and whether the decedent had been homeless. We examined significant associations between variables by using the Pearson χ2 tests and logistic regression.
Results
During 2006-2016, MCDPH recorded data on 920 heat-associated deaths, 912 of which included location of injury. Of 565 (62%) heat-associated deaths that occurred outdoors, 458 (81%) were among male decedents and 243 (43%) were among decedents aged 20-49. Of 347 (38%) heat-associated deaths that occurred indoors, 201 (58%) were among decedents aged ≥65. Non-Arizona residents were 5 times as likely as Arizona residents to have a heat-associated death outdoors (P < .001). Of 727 decedents with data on duration of Arizona residency, 438 (60%) had resided in Arizona ≥20 years.
Conclusions
Ongoing evaluation of interventions that target populations at risk for both outdoor and indoor heat-associated deaths can further inform refinement of the surveillance system and identify best practices to prevent heat-associated deaths.
Prevention of heat-associated deaths is a public health priority in Maricopa County, Arizona. 1 During 1999-2017, approximately 13% of all heat-related deaths in the United States occurred in Maricopa County, 2 which accounted for only about 1% of the US population. Maricopa County is located in the Sonoran Desert and is predictably hot during May through October; annually during 2006-2016, Maricopa County had a mean of 140 days (range, 129-149 days) with daily maximum temperatures ≥90 °F (32 °C) and a mean of 57 days (range, 34-70 days) with daily maximum temperatures ≥105 °F (40.5 °C). 3 The population in Maricopa County has grown rapidly in recent years, 4 increasing about 11.2% from 2010 (population 3 817 117) to 2016 (population 4 233 383), as compared with an estimated 4.7% population increase in the United States overall. 5 Population growth in Maricopa County has been accompanied by increasing urbanization, potentially exacerbating the urban heat island effect in densely populated areas. 6
In 2005, temperatures in Maricopa County were exceptionally high (maximum, 116 °F [46.6 °C]), which contributed to 35 deaths during a 9-day period 7 ; a subsequent study of 2000-2005 heat-associated deaths highlighted the vulnerability of people experiencing homelessness. 8 The 2005 heat event prompted the formation of a heat-relief network 1 and the creation of a novel surveillance system for heat-associated deaths at the Maricopa County Department of Public Health (MCDPH) in 2006. MCDPH’s surveillance system also captures data on residents of other jurisdictions, including visitors, and on the location and circumstances of death.
The combination of a large urban population, predictably hot weather, and an established, robust surveillance system makes Maricopa County an ideal place to explore circumstances associated with heat-associated deaths. Regional studies have demonstrated associations between heat-associated mortality and contextual factors, such as weather and temperature, neighborhood socioeconomic status, social isolation, and land cover. 8 -11 MCDPH’s heat-associated death surveillance system provides a valuable complement to these place-based analyses with detailed data on the demographic characteristics of decedents and circumstances of death. We describe findings of the Maricopa County heat-associated death surveillance system in the 11-year period (2006-2016) since its implementation to understand the circumstances of heat-associated deaths and compare these results with the findings of studies and projects that occurred during the same period.
Methods
Study Population and Data Sources
MCDPH’s heat-associated death surveillance system captures data on deaths that occur as a result of exposure to environmental heat among residents and nonresidents of Maricopa County. Heat-associated deaths are classified as either heat caused or heat related. For heat-caused deaths, environmental heat directly contributed to the sequence of conditions causing death (part I of the death certificate). For heat-related deaths, environmental heat was a contributing cause of death (part II of the death certificate). Heat-caused and heat-related deaths together comprise heat-associated deaths. MCDPH surveillance data are obtained from the Arizona State Vital Records Registry and the Maricopa County Office of the Medical Examiner (OME). All Maricopa County death certificates are registered in the vital records database of the Arizona Department of Health Services according to Arizona Revised Statutes §36-325. 12 MCDPH searches this database weekly to identify heat-associated deaths by using International Classification of Diseases, Tenth Revision (ICD-10) codes X30 (exposure to excessive natural heat), T67.X (effects of heat and light), and P81.0 (environmental hyperthermia of newborn). 13 To identify heat-associated deaths, MCDPH searches for the key phrases heat exposure, environ, exhaustion, sun, heat stress, heat stroke, and hyperthermia.
Maricopa County’s OME securely emails data on suspected heat-associated deaths to MCDPH, including data on the demographic characteristics of the decedent, preliminary data on how the death occurred, and circumstances of the death. After final OME certification of death, MCDPH classifies deaths as heat caused or heat related. We conducted this analysis during 2017, and we included data on heat-associated deaths during 2006-2016. The Centers for Disease Control and Prevention determined this project to be nonresearch.
We directly retrieved data from death certificates on case classifications, age, sex, race/ethnicity, residency (Maricopa County resident, Arizona resident, or non-Arizona resident), alcohol and substance use (any mention of alcohol or any federally illicit substance in the free text of the death certificate), and years lived in Arizona. We recorded circumstances of the heat-associated injury leading to death (including location where the injury occurred), presence and functionality of air conditioning, and homelessness based on explicit notations made in the preliminary report of death or death certificate; if variables were included in both sources, the death certificate data superseded information from the OME preliminary report of death. We classified location of injury as an urban area if the injury occurred in a field, park, urban mountain area, driveway, golf course, or shed.
We classified the location of heat-associated injury as outdoors if the decedent was found anywhere outside of a building, including in a front yard, backyard, or driveway; we classified all other locations within a residence, including garage, as having occurred indoors. We classified location of injury as indoors if the injury occurred in a business or associated building. OME death investigators determined whether air conditioning was present; MCDPH classified presence of air conditioning as undetermined if the presence of air conditioning was not recorded. OME investigators also verified the status and functionality of the air-conditioning unit, classified as turned off (not running), not working (blowing hot air or tested and found to not turn on or cool), or no electricity. For OME preliminary reports of death that included the terms transient or homeless or an unknown address, MCDPH investigated further to determine whether a decedent was homeless. We classified a decedent as homeless if the home address on the death certificate was unknown or matched a homeless shelter, government agency, business, or intersection of 2 streets. MCDPH classified decedents who were experiencing homelessness as Maricopa County residents because they were living in Maricopa County at the time of death. We combined racial/ethnic groups into the following: non-Hispanic white, non-Hispanic black, non-Hispanic American Indian, non-Hispanic Asian/Pacific Islander, and Hispanic of any race.
Statistical Analysis
For Maricopa County residents, we calculated annual rates of heat-associated deaths by sex, age group, and racial/ethnic group for all deaths and each case classification (heat-caused death or heat-related death) by using Maricopa County population 1-year estimates from the US Census Bureau. 5,14 We calculated the average annual rates of death separately for each year during 2006-2016 and averaged during the 11-year period.
We summarized variables using frequencies and percentages for the population overall and stratified by residency (Maricopa County residents vs nonresidents) and location of heat-associated injury leading to death (indoors vs outdoors). We used the Pearson χ2 test to identify associations between age group and location of injury separately among female and male decedents. We also used the Pearson χ2 test to determine whether Arizona residency, homelessness, substance use, or alcohol use were associated with location of injury. In addition, we used logistic regression to calculate odds ratios (ORs), ORs adjusted for conceptualized demographic confounders (adjusted ORs [aORs]), and 95% confidence intervals (CIs) for location of heat-associated injury leading to death by Arizona residency. We considered P < .05 to be significant. We performed all data analysis by using SAS Enterprise Guide version 7.1. 15
Results
During 2006-2016, MCDPH recorded 920 heat-associated deaths; 812 (88.2%) were among Maricopa County residents and 105 (11.4%) were among nonresidents (Table 1). Thirty-four of 105 nonresidents were residents of Arizona, and 3 decedents had unknown residency. The 11-year average annual rate of heat-associated deaths per 100 000 population among Maricopa County residents was 1.9 (range, 1.1-3.3; Figure).
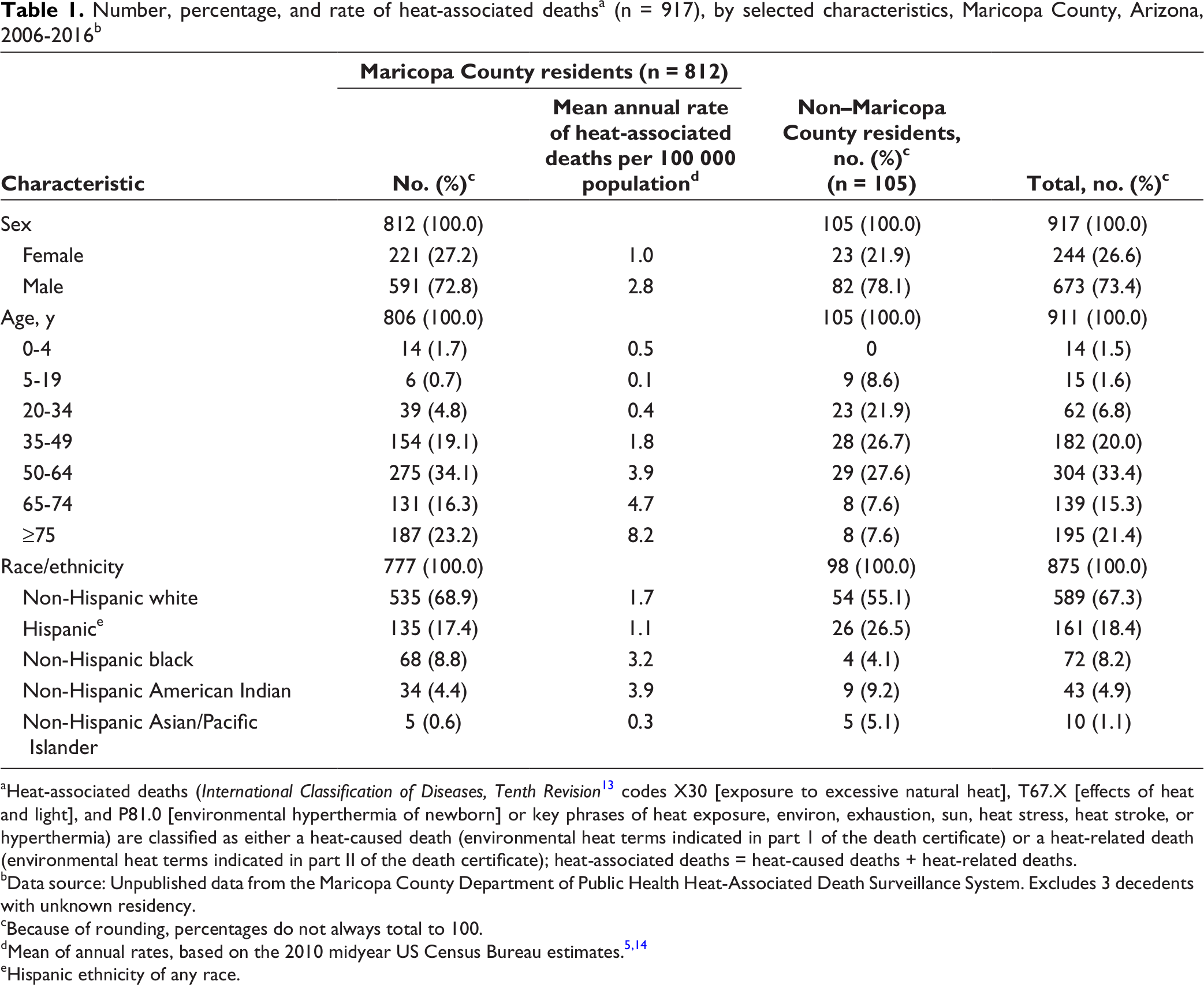
aHeat-associated deaths (International Classification of Diseases, Tenth Revision 13 codes X30 [exposure to excessive natural heat], T67.X [effects of heat and light], and P81.0 [environmental hyperthermia of newborn] or key phrases of heat exposure, environ, exhaustion, sun, heat stress, heat stroke, or hyperthermia) are classified as either a heat-caused death (environmental heat terms indicated in part 1 of the death certificate) or a heat-related death (environmental heat terms indicated in part II of the death certificate); heat-associated deaths = heat-caused deaths + heat-related deaths.
bData source: Unpublished data from the Maricopa County Department of Public Health Heat-Associated Death Surveillance System. Excludes 3 decedents with unknown residency.
cBecause of rounding, percentages do not always total to 100.
eHispanic ethnicity of any race.

Rates of heat-associated, heat-caused, and heat-related deaths, by year, among residents of Maricopa County, Arizona, 2006-2016. Heat-associated deaths (International Classification of Diseases, Tenth Revision 13 codes X30 [exposure to excessive natural heat], T67.X [effects of heat and light], and P81.0 [environmental hyperthermia of newborn] or key phrases about heat exposure, environ, exhaustion, sun, heat stress, heat stroke, hyperthermia) are classified as either a heat-caused death (environmental heat terms indicated in part 1 of the death certificate) or a heat-related death (environmental heat terms indicated in part II of the death certificate); heat-associated deaths = heat-caused deaths + heat-related deaths. Data source: US Census Bureau 5,14 and unpublished data from the Maricopa County Department of Public Health Heat-Associated Death Surveillance System.
A higher percentage of heat-associated deaths occurred among male decedents (n = 673, 73.4%) than among female decedents (n = 244, 26.6%) and among younger age groups of nonresidents (aged 5-49) than among Maricopa County residents (Table 1). Of 777 Maricopa County residents with data on race/ethnicity, the highest proportion of deaths occurred among non-Hispanic white (n = 535, 68.9%) and Hispanic (n = 135, 17.4%) residents; the highest rates of heat-associated deaths per 100 00 population occurred among non-Hispanic American Indian (3.9) and non-Hispanic black (3.2) residents. Non-Hispanic white people comprised more than half (55.1%) of heat-associated deaths among nonresidents. The proportion of heat-associated deaths among Hispanic (26.5%) and non-Hispanic American Indian (9.2%) nonresidents was higher than among Hispanic (17.4%) and non-Hispanic American Indian (14.4%) residents.
Most (565 of 912, 62.0%) heat-associated injuries leading to death occurred outdoors; Maricopa County residents were significantly more likely than nonresidents to be injured indoors (P < .001; Table 2). Of 347 heat-associated injuries that occurred indoors, 344 (99.1%) occurred in a residence. Of 14 children aged 0-4 years who died from a heat-associated injury, 11 were injured in a parked car.
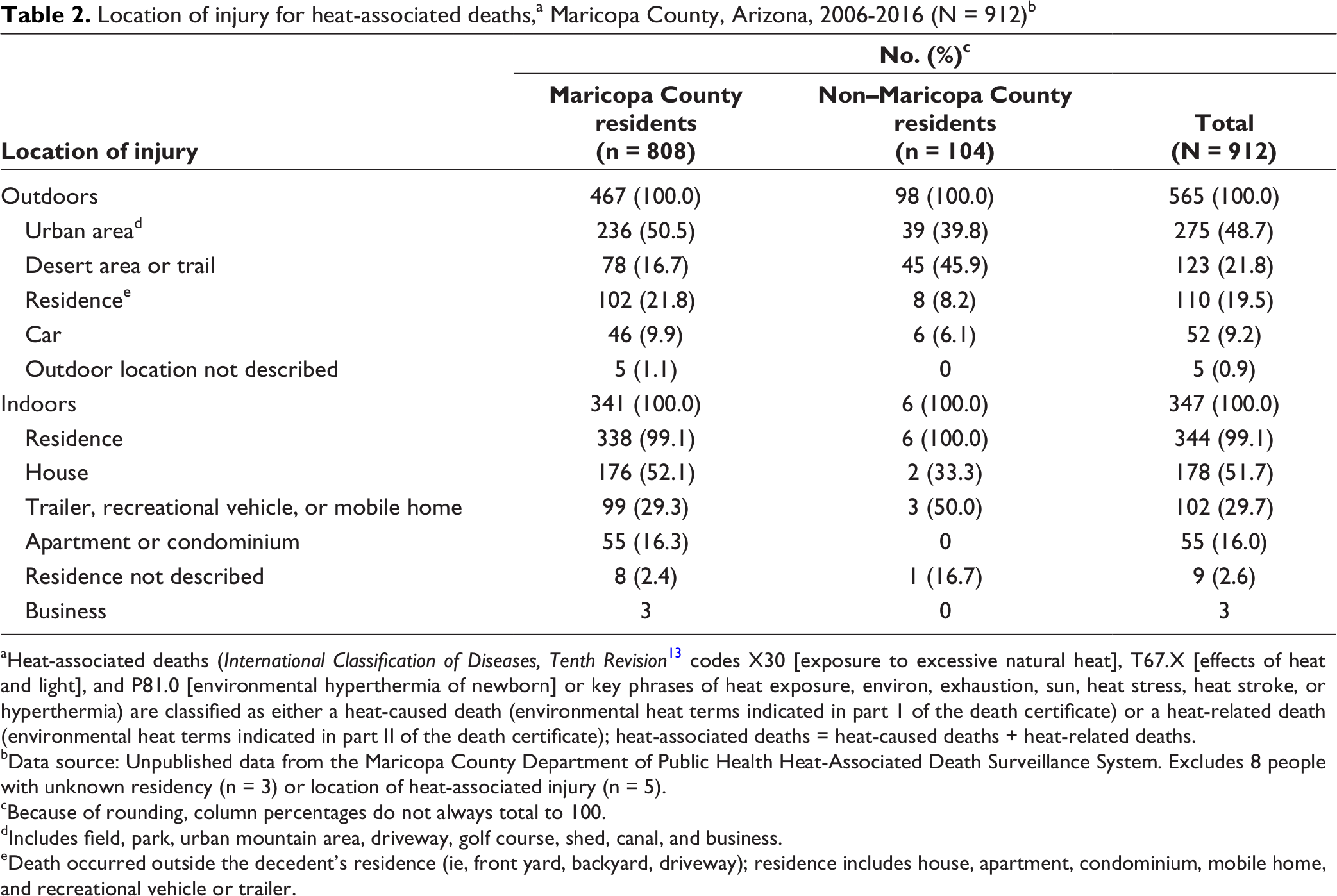
aHeat-associated deaths (International Classification of Diseases, Tenth Revision 13 codes X30 [exposure to excessive natural heat], T67.X [effects of heat and light], and P81.0 [environmental hyperthermia of newborn] or key phrases of heat exposure, environ, exhaustion, sun, heat stress, heat stroke, or hyperthermia) are classified as either a heat-caused death (environmental heat terms indicated in part 1 of the death certificate) or a heat-related death (environmental heat terms indicated in part II of the death certificate); heat-associated deaths = heat-caused deaths + heat-related deaths.
bData source: Unpublished data from the Maricopa County Department of Public Health Heat-Associated Death Surveillance System. Excludes 8 people with unknown residency (n = 3) or location of heat-associated injury (n = 5).
cBecause of rounding, column percentages do not always total to 100.
dIncludes field, park, urban mountain area, driveway, golf course, shed, canal, and business.
eDeath occurred outside the decedent’s residence (ie, front yard, backyard, driveway); residence includes house, apartment, condominium, mobile home, and recreational vehicle or trailer.
Of 347 heat-associated injuries leading to deaths that occurred indoors, the presence or absence of air conditioning was documented for 287 (82.7%) deaths, all of which occurred in an indoor space that was inadequately cooled. An air-conditioning unit was absent in 59 (20.6%) deaths and present in 228 (79.4%) deaths. Of these 228 deaths, the air-conditioning unit was turned off (but documented to be functional) for 78 (34.2%) deaths and nonfunctioning for 120 (52.6%) deaths; the electricity in the residence was turned off for 30 (13.2%) deaths.
For male decedents in all age groups <65, a higher proportion of heat-associated injury leading to death occurred outdoors as compared with indoors (Table 3). Female decedents aged ≤49 were also more likely to have an injury outdoors than indoors; however, women aged ≥65 were significantly more likely to be injured indoors than outdoors (68.3% vs 31.7% P < .001). Of the 97 women aged ≥65 who died indoors, an air-conditioning unit was present in 71 (73.2%) deaths but was either not functioning (n = 33, 46.5%) or not in use (n = 26, 36.6%).
Demographic characteristics of heat-associated deaths (N = 917), by location of death, Maricopa County, Arizona, 2006-2016 a
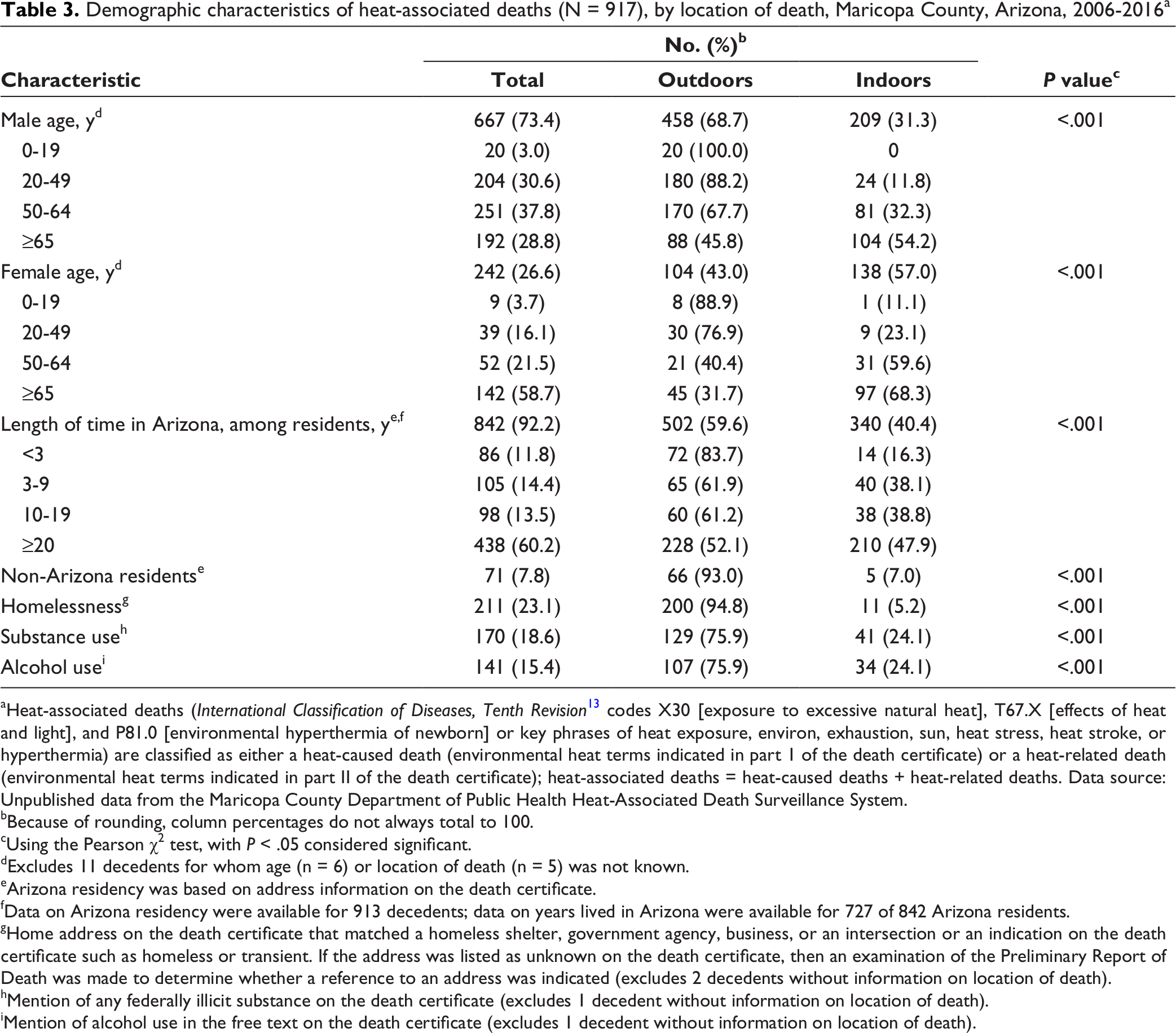
aHeat-associated deaths (International Classification of Diseases, Tenth Revision 13 codes X30 [exposure to excessive natural heat], T67.X [effects of heat and light], and P81.0 [environmental hyperthermia of newborn] or key phrases of heat exposure, environ, exhaustion, sun, heat stress, heat stroke, or hyperthermia) are classified as either a heat-caused death (environmental heat terms indicated in part 1 of the death certificate) or a heat-related death (environmental heat terms indicated in part II of the death certificate); heat-associated deaths = heat-caused deaths + heat-related deaths. Data source: Unpublished data from the Maricopa County Department of Public Health Heat-Associated Death Surveillance System.
bBecause of rounding, column percentages do not always total to 100.
cUsing the Pearson χ2 test, with P < .05 considered significant.
dExcludes 11 decedents for whom age (n = 6) or location of death (n = 5) was not known.
eArizona residency was based on address information on the death certificate.
fData on Arizona residency were available for 913 decedents; data on years lived in Arizona were available for 727 of 842 Arizona residents.
gHome address on the death certificate that matched a homeless shelter, government agency, business, or an intersection or an indication on the death certificate such as homeless or transient. If the address was listed as unknown on the death certificate, then an examination of the Preliminary Report of Death was made to determine whether a reference to an address was indicated (excludes 2 decedents without information on location of death).
hMention of any federally illicit substance on the death certificate (excludes 1 decedent without information on location of death).
iMention of alcohol use in the free text on the death certificate (excludes 1 decedent without information on location of death).
Two hundred thirteen (23.2%) deaths occurred among people experiencing homelessness, 211 (99.1%) of whom had information on the location of injury that led to death (Table 3). Of these, 200 (94.8%) deaths were the result of injuries that occurred outdoors. The proportion of heat-associated deaths that occurred among people experiencing homelessness decreased from 37.6% (32 of 85) of deaths in 2006 to 6.5% (3 of 46) of deaths in 2008 and then increased to 36.2% (54 of 149) of deaths in 2016.
During 2006-2016, 842 (91.8%) heat-associated deaths occurred among Arizona residents and 71 of 913 (7.8%) occurred among non–Arizona residents (Table 3). Among all heat-associated deaths, the odds of being injured outdoors were higher among non–Arizona residents than among Arizona residents (OR = 8.2; 95% CI, 3.4-19.4). This association remained significant after adjusting for age, sex, and race/ethnicity (aOR = 5.1; 95% CI, 2.0-13.1). The number of years of residence in Arizona was known for 727 decedents; 438 (60.2%) had lived in Arizona for ≥20 years. Among all heat-associated deaths, people who had lived in Arizona for <3 years had higher odds of having been injured outdoors than people who had lived in Arizona for ≥20 years (OR = 4.6; 95% CI, 2.5-8.4); this association remained significant after adjusting for age, sex, and race/ethnicity (aOR = 2.4; 95% CI, 1.2-4.7).
Discussion
The heat-associated death surveillance system in Maricopa County includes data on key variables that allow for understanding the circumstances of death among residents and nonresidents. The 2 populations identified to be at most risk for heat-associated death were unchanged since a 2005 analysis. 8 These populations included young and middle-aged people, most commonly male, who were injured outdoors and people aged ≥65 years who were injured indoors, most frequently inside their residence. The establishment of the MCDPH surveillance system in 2006 that describes the circumstances of death supported implementation of public health interventions and projects that target populations at risk for both outdoor and indoor heat-associated death. 1,16,17
In contrast to other urban locations in the developed world where most heat-associated injuries leading to death occur indoors, 18 -21 most heat-associated deaths in Maricopa County occurred outdoors. In addition, during 2006-2016, approximately one-third of outdoor deaths occurred among people experiencing homelessness. The most dramatic drop in the proportion of heat-associated deaths among people experiencing homelessness occurred during the years after the 2005 heatwave. This drop coincided with the early years after formation of the Maricopa Association of Governments (MAG) heat-relief network in 2005. However, the surveillance data also show that the proportion of heat-associated deaths that occurred among people experiencing homelessness increased to 36% in 2016. In 2004, MAG began collecting data on the number of people experiencing sheltered and unsheltered homelessness in Maricopa County through a point-in-time homeless count. The proportion of people experiencing unsheltered homelessness increased during 2014 (18%; 1053 of 5918 homeless people) through 2016 (29%; 1646 of 5702 homeless people). 22 Unsheltered homelessness is an important risk factor for heat-associated injuries leading to death, 11 because most heat-associated deaths among people experiencing homelessness occur outdoors.
Consistent with patterns observed in urban heat waves, in which older people and those without access to air conditioning are most vulnerable, 18,20 women aged ≥65 were injured in an uncooled indoor environment more commonly than women of all other age groups and men aged 65 and older. Of 287 heat-associated deaths that occurred indoors and for which the presence or absence of an air-conditioning unit was documented, an air-conditioning unit was present in 79% (228) of decedents’ homes; on average, approximately 99% of homes in the Phoenix, Arizona, metropolitan area have air conditioning in the home. 23 Although fewer people with heat-associated injuries leading to death in our study had access to air conditioning compared with the average population in the Phoenix Metropolitan Service Area and nationally, 23 other factors likely played an important role in the death of 228 people, despite the presence of air conditioning. Circumstances that restrict the use of air conditioning were further explored in a 2014 survey of Maricopa County cooling center visitors. 1 Among 515 respondents with an air-conditioning unit at home, 86 (16%) stated that they did not use air conditioning at home because of cost, and 21 (4%) stated that their air-conditioning unit was broken. One-quarter of respondents stated that they had used a utility assistance program in the past, providing evidence that the cost of electricity might be an important underlying factor in indoor heat-associated deaths. Data from the 2015 cooling center survey supported the need for a 2016 survey 16 of homebound people that assessed barriers to using home cooling systems and knowledge and use of community assistance programs. Barriers identified included cost of electricity bills (81%; 105 of 130 respondents) and cost of repairs (27%; 35 of 130 respondents). The survey also identified a potential need for better advertising, application support, and more funding for energy assistance programs in the target community. The federally funded low-income home energy assistance program (LIHEAP) can help people who are unable to afford electricity for heating or cooling. 24 However, in 2014, LIHEAP funding supported fewer than 5% (n = 50 520) of 617 000 eligible Arizona households 25 ; by comparison, an estimated 16% of eligible households nationally receive benefits from LIHEAP. 24
The largest proportion of heat-associated deaths during the study period occurred among people who had lived in Arizona for ≥20 years. Although long-term Arizona residents might be better acclimated to heat than the average population, 9 acclimation does not eliminate the risk for death from heat-associated illness. Approximately equal proportions of decedents who had lived in Arizona for ≥20 years had a heat-associated injury leading to death outdoors as indoors. In contrast, decedents who had lived in Arizona for <3 years were at increased odds of having had a heat-associated injury outdoors, possibly because people who have moved to Arizona more recently might underestimate the effects of high outdoor ambient temperatures. Providing messaging about heat-associated illness prevention to this group could address this factor. Messaging about the risks of heat-associated illness to people who have lived in Arizona for ≥20 years might be challenging because it requires altering perception of risk, exertion, and personal susceptibility relative to age and health status.
MCDPH’s mission is to promote the health and well-being of Maricopa County residents and visitors, which is substantial in a region that hosts >22 million overnight visitors annually 26 ; MCDPH’s heat-associated death surveillance system captures data on heat-associated deaths among Maricopa County visitors. Decedents who were not residents of Maricopa County were more likely than Maricopa County residents to have incurred a heat-associated injury outdoors, most commonly on desert areas or trails or in urban areas. MCDPH heat-associated death surveillance data supported a 2015 hiking safety campaign by the city of Phoenix and the placement of highly visible heat safety signage at 41 official trailheads in Phoenix. 17
MCDPH weekly updates and yearly summaries of heat-associated death surveillance data have been used to develop interventions and studies that focus on groups at high risk for heat-associated mortality. Data were used to identify the need for and location of cooling stations, established as part of the MAG heat-relief network. Although heat-associated deaths initially decreased during 2006-2008, an increase during 2009-2012 prompted the 2014 cooling center survey to more fully understand which groups were using cooling centers. 1 Approximately one-third (33%; 192 of 582) of respondents were not currently residing in a permanent residence, suggesting that these centers were being used by people experiencing homelessness. The assessment determined that cooling center use could be improved through increased signage and by extending operational hours to include nights and weekends, especially on excessive heat warning days. 1
Limitations
This study had several limitations. First, we reported data during an 11-year period. Coding practices among medical examiners, who have discretion in assigning heat-associated death classifications, might have changed during this period, resulting in inconsistencies in classification; however, no formal policy changes were made in the coding process at the Maricopa County OME during this period, and a medical examiner’s assessment of cause of death is considered the gold standard. Second, MCDPH classified heat-associated deaths based on all information available from the death investigation. It is possible that the quality of data available varied by the circumstances of death that we considered, thereby resulting in misclassification. In particular, the prevalence of factors such as substance use and alcohol use might have been underestimated. However, we do not expect this potential misclassification of factors to differ for deaths that occurred indoors versus outdoors or for Maricopa County residents versus nonresidents. Third, data from the Maricopa County heat-associated death surveillance system might differ from data published by the National Vital Statistics System 27 and from other surveillance systems and research studies that use broader definitions (additional ICD-10 codes associated with secondary effects of environmental heat, such as cardiovascular disease) of heat-associated mortality, thereby limiting comparability with other studies. Finally, results of this analysis were intended to guide local policies and interventions and are not generalizable beyond Maricopa County.
Conclusions
Heat-associated mortality is preventable in Maricopa County. Over time, annual data collected from heat-associated death reports have been used to support implementation of public health interventions and projects that target populations at risk for both outdoor and indoor heat-associated injury and death. Findings from this analysis and associated projects indicate a need for additional resources, particularly for the expansion of the heat-relief network and cooling center hours and the prevention of heat-associated deaths in uncooled residences, including those that have air conditioning. Increasing awareness and Arizona’s funding for energy-assistance programs should be considered to prevent mortality among the population of older, income-limited residents. Surveillance data could be used to help assess the effects of long-term strategies and policies aimed at mitigating the urban heat-island effect, such as shade and urban greening projects. Ongoing evaluation of interventions can further inform refinement of the surveillance system and identify best practices to prevent heat-associated deaths.
Footnotes
Acknowledgments
The authors acknowledge the work of colleagues at the Maricopa County Department of Public Health and the Office of the Medical Examiner in the development of the heat-associated mortality surveillance system, as well as partnerships with the National Weather Service, Arizona State University, Maricopa Association of Governments, the City of Phoenix, and Arizona Department of Health Services in the refinement of the system and implementation of interventions described. The authors also thank Kristine Bisgard and Fuyuen Yip for their review of this article.
Authors’ Note
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Sally Ann Iverson was partially supported during the article preparation phase by the Centers for Disease Control and Prevention’s Environmental Public Health Tracking Program, grant 1 NUE1EH001339-01-00.