
Abstract
Objectives:
This study, measuring the prevalence of chronic obstructive pulmonary disease (COPD), examined (1) whether a single survey question asking explicitly about diagnosed COPD is sufficient to identify US adults with COPD and (2) how this measure compares with estimating COPD prevalence using survey questions on diagnosed emphysema and/or chronic bronchitis and all 3 survey questions together.
Methods:
We used data from the 2012-2014 National Health Interview Survey to examine different measures of prevalence among 7211 US adults who reported a diagnosed respiratory condition (ie, emphysema, chronic bronchitis, and/or COPD).
Results:
We estimated a significantly higher prevalence of COPD by using a measure accounting for all 3 diagnoses (6.1%; 95% CI, 5.9%-6.3%) than by using a measure of COPD diagnosis only (3.0%; 95% CI, 2.8%-3.1%) or a measure of emphysema and/or chronic bronchitis diagnoses (4.7%; 95% CI, 4.6%-4.9%). This pattern was significant among all subgroups examined except for non-Hispanic Asian adults. The percentage difference between measures of COPD was larger among certain subgroups (adults aged 18-39, Hispanic adults, and never smokers); additional analyses showed that this difference resulted from a large proportion of adults in these subgroups reporting a diagnosis of chronic bronchitis only.
Conclusions:
With the use of self- or patient-reported health survey data such as the National Health Interview Survey, it is recommended that a measure asking respondents only about COPD diagnosis is not adequate for estimating the prevalence of COPD. Instead, a measure accounting for diagnoses of emphysema, chronic bronchitis, and/or COPD may be a better measure. Additional analyses should explore the reliability and validation of survey questions related to COPD, with special attention toward questions on chronic bronchitis.
Keywords
Chronic obstructive pulmonary disease (COPD) includes several conditions that limit airflow (a limitation that is not fully reversible) 1 and is associated with chronic cough, exertional dyspnea (shortness of breath), expectoration, and wheeze. 2 –4 Although progress has been made in COPD prevention in the United States, 1 COPD is a leading cause of morbidity and mortality worldwide. 5 In 2013, chronic lower respiratory diseases were the third-leading cause of death in the United States, 6 with 144 637 deaths (45.8 per 100 000 population) attributable to COPD. 7
US researchers estimating the percentage of US adults who have COPD generally rely on self-reported diagnoses collected in large-scale national surveys, such as the National Health Interview Survey (NHIS). This method may be the best for collecting data that are representative of the US population, compared with other methods, such as postbronchodilator spirometry, because of its financial and logistical benefits. Despite the benefits of using self-reported data, research suggests that prevalence rates based on self-reported data are underestimates. 2,8 –10 These underestimates may be caused by several factors, including underdiagnosis and differences in which conditions are used to define COPD. 11
COPD prevalence rates based on self-reported data have often been estimated by using data on reported diagnosis of emphysema and/or chronic bronchitis. 2,7,12 This method was applied to 1997-2011 NHIS data to estimate COPD prevalence: respondents were classified as having diagnosed COPD if they answered yes to 1 or both survey questions asking if they had ever been diagnosed with emphysema or chronic bronchitis in the previous 12 months. Although use of the term COPD and public awareness of it are historically low, increases in direct-to-consumer advertising and COPD education and awareness efforts suggest that a language shift is occurring. 13 In 2012, a survey question was added to the NHIS asking if adults had ever been diagnosed with COPD, with the potential for the questions asking about emphysema and chronic bronchitis to be dropped in the future. However, it is unknown whether people understand that emphysema and chronic bronchitis are synonymous with COPD or what may happen to prevalence rates of diagnosed COPD if this change in questions would occur.
The objective of this study was to determine whether 1 survey question asking about diagnosed COPD is sufficient to identify adults with COPD and how use of this 1 question compares with the traditional approach of using questions on diagnosed emphysema and chronic bronchitis and an approach that combines all 3 diagnoses. We examined prevalence rates for all adults and subgroups using various demographic characteristics and COPD risk factors. Based on these results, we conducted additional analyses to examine the validity and reliability of the NHIS question on diagnosed chronic bronchitis. We then made recommendations for estimating COPD prevalence using self-reported diagnosis data from health surveys such as the NHIS.
Methods
The NHIS, a multistage continuous survey, is a source of nationally representative health data on the civilian, noninstitutionalized US population. The survey consists of an in-person interview conducted in the respondent’s home, 14 with occasional follow-up by telephone. One randomly selected adult from each interviewed family answers questions about his or her health unless he or she is unable to do so (1.4% use proxies). Data for 105 779 adult respondents aged ≥18 were available from the 2012-2014 NHIS (final response rates: 61.2% for 2012 and 2013, 58.9% for 2014). 14 Our study was considered exempt from institutional review board review.
Measures of Diagnosed COPD Prevalence
The NHIS has 3 COPD-related questions: (1) “Have you ever been told by a doctor or other health professional that you had emphysema?” (asked from 1997 onward), (2) “Have you ever been told by a doctor or health professional that you had chronic obstructive pulmonary disease, also called COPD?” (a new question added in 2012), and (3) “During the past 12 months, have you ever been told by a doctor or other health professional that you had chronic bronchitis?” (asked from 1997 onward). During the interview, these questions were asked in the order listed, although not immediately following one another. We generated 3 estimates of diagnosed COPD from these questions. The first estimate identified adults as having COPD if they responded yes to either survey question asking about emphysema or chronic bronchitis diagnoses, the traditional approach in using data from NHIS. 1,2 The second estimate identified adults as having COPD if they responded yes to the survey question asking only about a COPD diagnosis. The third estimate identified adults as having COPD if they answered yes to any of the 3 questions. We also created a final categorical measure to discern which selected respiratory conditions respondents had: emphysema only, chronic bronchitis only, COPD only, or >1 condition.
Demographic and Health Characteristics
We estimated the prevalence of diagnosed COPD across various subgroups, including sex, race/ethnicity, and age. We also estimated the prevalence of diagnosed COPD across subgroups related to 3 health characteristics linked to COPD by previous research 5,12 : (1) smoking status—classified as never, former, or current smokers; (2) ever having had asthma—a condition correlated with COPD but not itself a risk factor 5 ; and (3) having an occupation with a heightened risk of exposure to pollutants in the previous 12 months (ie, occupations with a significantly higher prevalence of exposure than the US national estimate, based on findings by Calvert and colleagues 15 ). Such occupations included protective services; food preparation and service; building and grounds cleaning/maintenance; farming, fishing, and forestry; construction and extraction; installation, maintenance, and repair; production; and transportation/material moving.
Analyses
We used Stata version 13.0 for all analyses. 16 We used survey weights that allowed for generalization to the US adult, civilian, noninstitutionalized population and sampling design variables to account for the complex cluster sampling design. We calculated descriptive estimates of measures of interest for US adults and for adults who reported diagnoses of emphysema, chronic bronchitis, and/or COPD (n = 7211; Table 1). We also calculated differences in national prevalence rates of diagnosed COPD according to the questions used to define COPD and relative and absolute percentage differences between the prevalence rates resulting from the different measures of COPD (Table 2). We examined the prevalence of COPD among all adults and by demographic and health characteristics. Finally, we determined percentage distributions for diagnosed emphysema only, for chronic bronchitis only, for COPD only, and for >1 of these conditions (Table 3). We used 2-tailed significance tests to test for differences between percentages, with P ≤ .05 considered to be significant. The significance tests used to compare estimates for prevalence of diagnosed COPD with different measures (in Table 2) were adjusted to account for dependent samples per methodology that is detailed elsewhere. 17
Prevalence of 3 selected respiratory condition diagnoses and demographic and health characteristics of the US adult population, National Health Interview Survey, 2012-2014
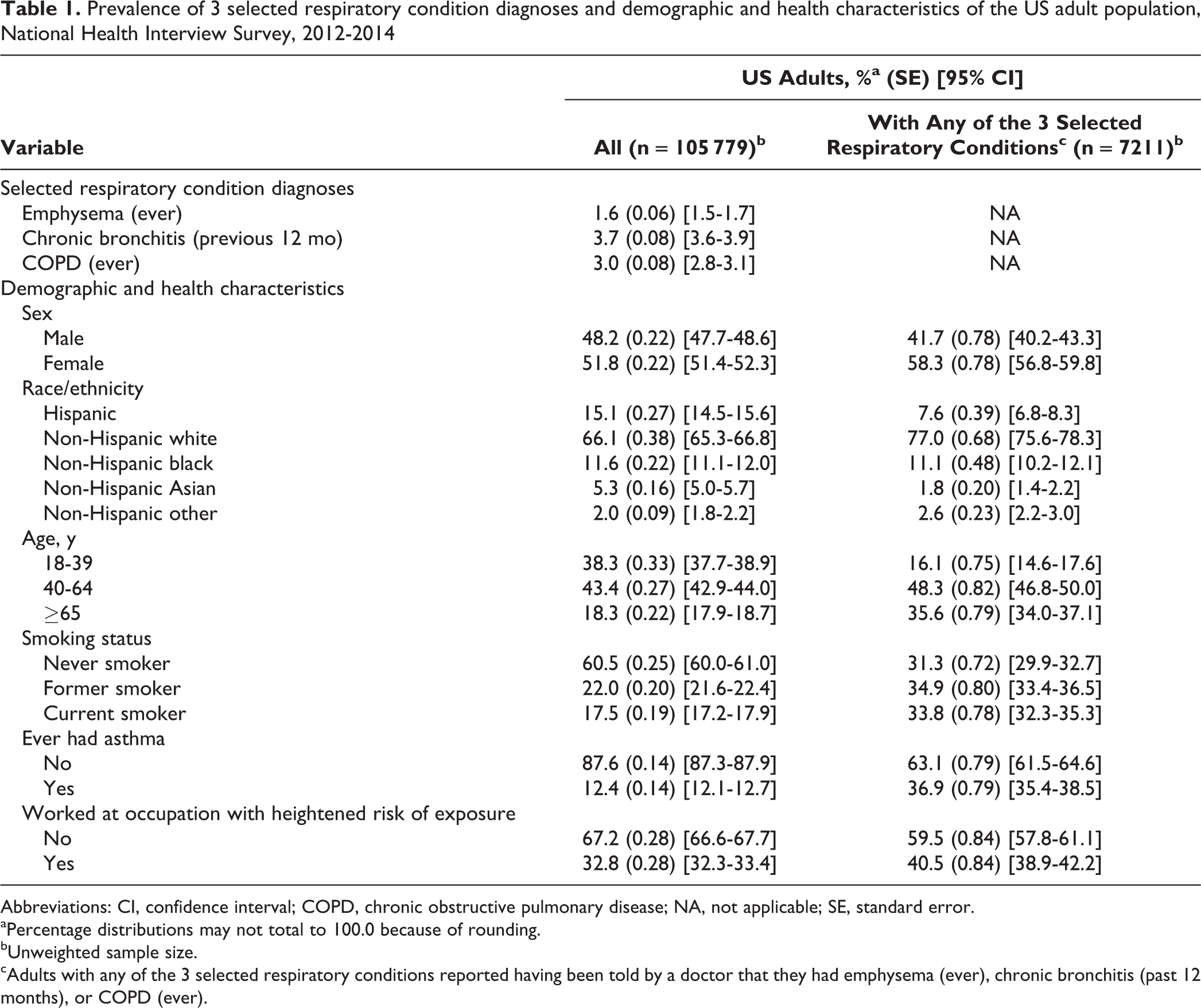
Abbreviations: CI, confidence interval; COPD, chronic obstructive pulmonary disease; NA, not applicable; SE, standard error.
aPercentage distributions may not total to 100.0 because of rounding.
bUnweighted sample size.
cAdults with any of the 3 selected respiratory conditions reported having been told by a doctor that they had emphysema (ever), chronic bronchitis (past 12 months), or COPD (ever).
Percentage of US adults with diagnosed COPD, by demographic and health characteristics, based on different survey questions, National Health Interview Survey, 2012-2014a
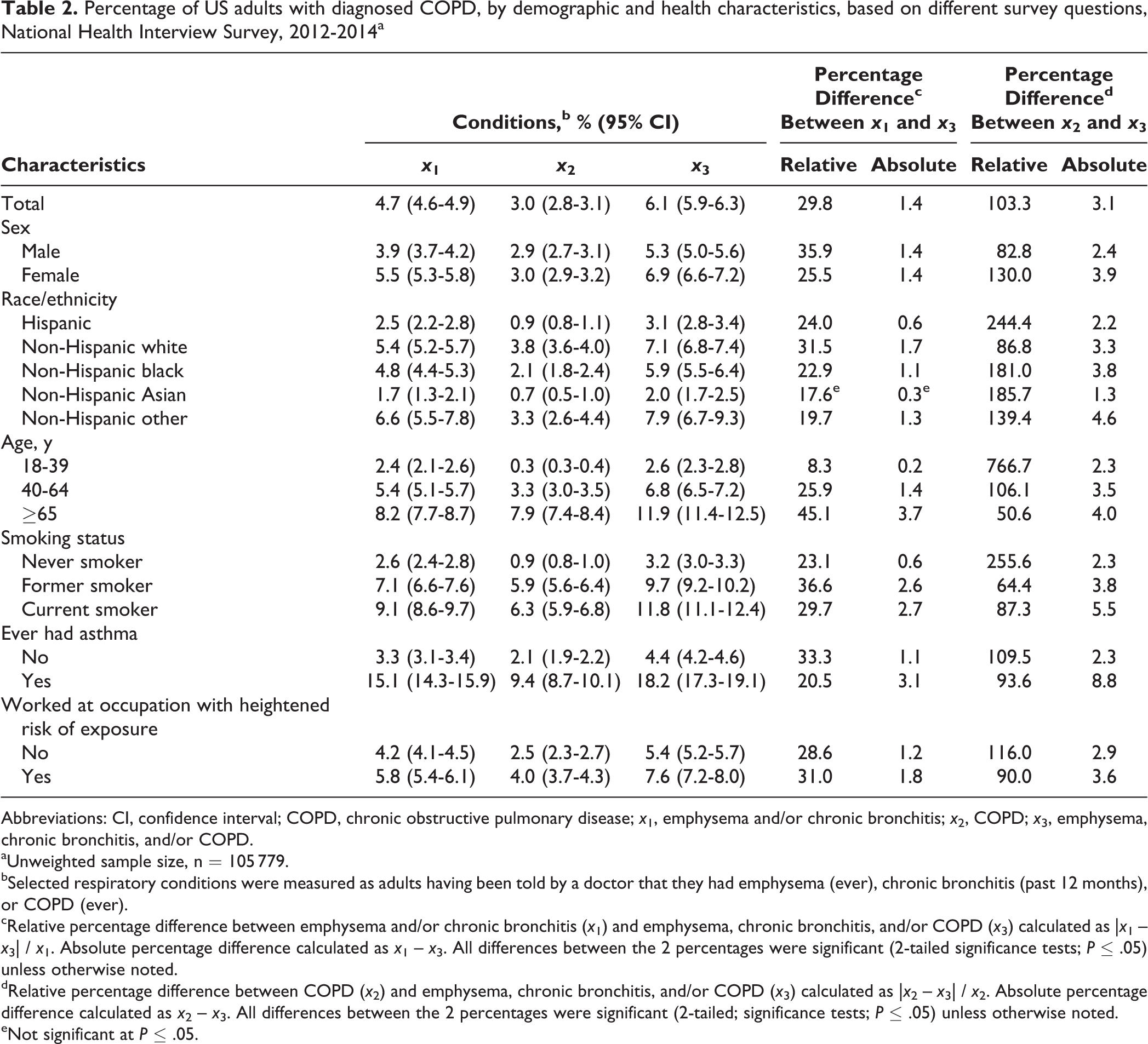
Abbreviations: CI, confidence interval; COPD, chronic obstructive pulmonary disease; x 1, emphysema and/or chronic bronchitis; x 2, COPD; x 3, emphysema, chronic bronchitis, and/or COPD.
aUnweighted sample size, n = 105 779.
bSelected respiratory conditions were measured as adults having been told by a doctor that they had emphysema (ever), chronic bronchitis (past 12 months), or COPD (ever).
cRelative percentage difference between emphysema and/or chronic bronchitis (x 1) and emphysema, chronic bronchitis, and/or COPD (x 3) calculated as |x 1 – x 3| / x 1. Absolute percentage difference calculated as x 1 – x 3. All differences between the 2 percentages were significant (2-tailed significance tests; P ≤ .05) unless otherwise noted.
dRelative percentage difference between COPD (x 2) and emphysema, chronic bronchitis, and/or COPD (x 3) calculated as |x 2 – x 3| / x 2. Absolute percentage difference calculated as x 2 – x 3. All differences between the 2 percentages were significant (2-tailed; significance tests; P ≤ .05) unless otherwise noted.
eNot significant at P ≤ .05.
Percentage distribution of selected diagnosed respiratory conditions, by demographic and health characteristics, among US adults with any of the 3 conditions, National Health Interview Survey, 2012-2014a
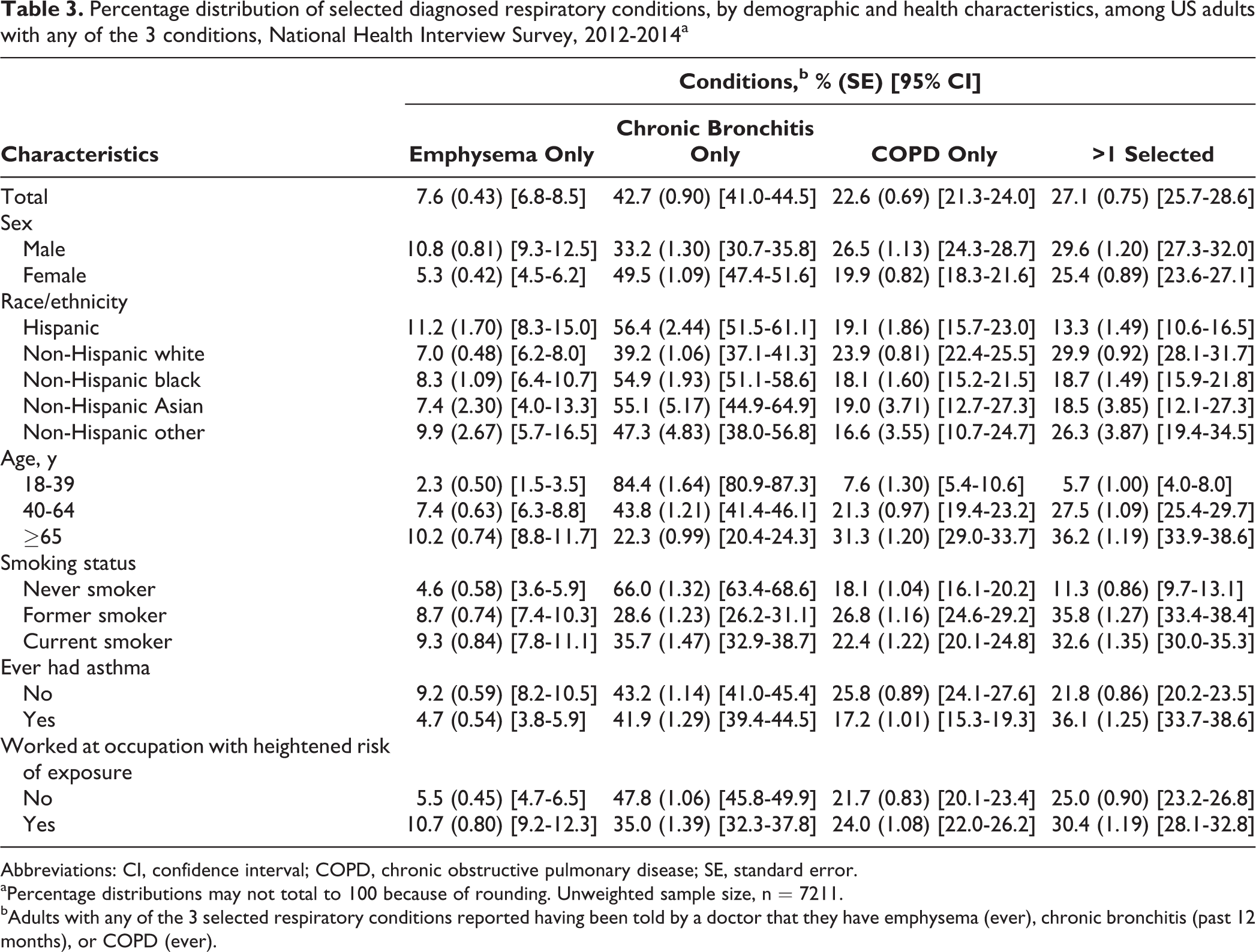
Abbreviations: CI, confidence interval; COPD, chronic obstructive pulmonary disease; SE, standard error.
aPercentage distributions may not total to 100 because of rounding. Unweighted sample size, n = 7211.
bAdults with any of the 3 selected respiratory conditions reported having been told by a doctor that they have emphysema (ever), chronic bronchitis (past 12 months), or COPD (ever).
Results
During 2012-2014, 1.6% of US adults had ever been diagnosed with emphysema, 3.7% had been diagnosed with chronic bronchitis in the previous 12 months, and 3.0% had ever been diagnosed with COPD. The US adult population and adults with at least 1 of the 3 diagnoses differed slightly in demographic and health characteristics (Table 1).
Among US adults, the estimated prevalence of diagnosed COPD was 4.7% (95% confidence interval [CI], 4.6%-4.9%) for reported diagnoses of emphysema and/or chronic bronchitis, 3.0% (95% CI, 2.8%-3.1%) for reported diagnoses of COPD only, and 6.1% (95% CI, 5.9%-6.3%) for any of the 3 diagnoses (Table 2). The prevalence of diagnosed COPD was significantly higher when we used the measure accounting for all 3 diagnoses than when we used the other 2 approaches. This pattern was found to be significant for each subgroup, with 1 exception: non-Hispanic Asian adults had no significant difference in prevalence between the measure of diagnoses of emphysema and/or chronic bronchitis and the measure of diagnoses of emphysema, chronic bronchitis, and/or COPD.
Absolute and relative differences in percentages show the magnitude of the impact of using different measures of diagnosed COPD prevalence for each subgroup. For subgroups in which reporting a COPD diagnosis was more prevalent, using a measure of emphysema and/or chronic bronchitis diagnoses yielded substantially lower estimates than using the measure accounting for all 3 diagnoses. These subgroups included adults who were non-Hispanic white (5.4% vs 7.1%; relative percentage difference, 31.5%), aged ≥65 (8.2% vs 11.9%; relative percentage difference, 45.1%), and former smokers (7.1% vs 9.7%; relative percentage difference, 36.6%) or current smokers (9.1% vs 11.8%; relative percentage difference, 29.7%). For subgroups in which reporting emphysema and/or chronic bronchitis diagnoses was more common than reporting COPD, using a measure of only COPD diagnosis yielded substantially lower estimates than using the measure accounting for all 3 diagnoses. This difference was particularly large among adults who were Hispanic (0.9% vs 3.1%; relative percentage difference, 244.4%), aged 18-39 (0.3% vs 2.6%; relative percentage difference, 766.7%), and never smokers (0.9% vs 3.2%; relative percentage difference, 255.6%), indicating that a COPD diagnosis accounted for only a small portion of the estimated prevalence. Most adults reporting any of the 3 diagnoses in these subgroups reported emphysema and/or chronic bronchitis but not COPD.
This finding raised the question of why a disproportionate number of adults in these subgroups appeared in the measure of diagnosed emphysema and/or chronic bronchitis but not in the measure of diagnosed COPD only. To investigate this question, we examined the percentage distribution of reporting emphysema, chronic bronchitis, COPD, and >1 of these conditions (Table 3). When we examined emphysema and chronic bronchitis diagnoses separately, we found for some subgroups that the prevalence of diagnosed COPD using the traditional measure (ie, having emphysema and/or chronic bronchitis) was driven primarily by a chronic bronchitis diagnosis. For example, 66.0% of adults with any of the 3 conditions who never smoked reported only a chronic bronchitis diagnosis but not emphysema or COPD, compared with 28.6% of former smokers and 35.7% of current smokers. Likewise, 84.4% of adults aged 18-39 with any of the 3 conditions reported chronic bronchitis diagnoses only, compared with 43.8% of adults aged 40-64 and 22.3% of adults aged ≥65. Only 5.7% of adults aged 18-39 had >1 diagnosis. Other subgroups with a comparatively higher proportion reporting only a chronic bronchitis diagnosis included Hispanic, non-Hispanic black, and non-Hispanic Asian adults and adults who had no heightened risk of occupational exposure. Even among all adults, it was more common for those with any respiratory diagnoses to report a diagnosis of only chronic bronchitis (42.7%) than to report only emphysema (7.6%), only COPD (22.6%), or >1 diagnosis (27.1%).
Thus, in estimating diagnosed COPD with a measure of emphysema and/or chronic bronchitis diagnosis or a measure accounting for all 3 diagnoses, the prevalence rate among certain subgroups may often be accounted for by reports of having only chronic bronchitis.
Discussion
We showed that national COPD prevalence estimates are affected by different measurement approaches: we estimated a significantly higher prevalence of diagnosed COPD by using a measure accounting for all 3 diagnoses (ie, emphysema, chronic bronchitis, and/or COPD) than by using a measure accounting for diagnosed COPD alone or by using a measure accounting for only emphysema and/or chronic bronchitis. The 6.1% prevalence estimated by combining NHIS data on all 3 diagnoses was nearly identical to the 6.3% estimate reported by the 2011 Behavioral Risk Factor Surveillance System (BRFSS). 8 The BRFSS asks about all 3 respiratory diagnoses in a single question: “Has a doctor, nurse, or other health professional ever told you that you have chronic obstructive pulmonary disease or COPD, emphysema, or chronic bronchitis?” 18 The BRFSS estimate is the only other published national estimate comparable to the NHIS estimate. We also showed that prevalence estimates for subgroups are affected in different ways by combining all 3 reported diagnoses. For example, adding a question about a COPD diagnosis changed the prevalence estimate very little for adults who were Hispanic, were aged 18-39, and had never smoked, because these adults typically respond no to this question. Our study indicates that the definition of COPD used in surveillance could have a greater impact on some subgroups than on others.
We estimated a higher percentage of adults with diagnosed COPD by using a measure of emphysema and/or chronic bronchitis diagnoses (4.7%) than by using a measure of COPD diagnosis only (3.0%). This pattern persisted for all subgroups. Although COPD encompasses both emphysema and chronic bronchitis and is often defined as such in national surveys, 1,2,8 it also includes less common respiratory conditions. 4 Therefore, it would be expected that asking about COPD would yield higher prevalence rates than asking about emphysema and/or chronic bronchitis only. Instead, the reverse pattern was found: higher prevalence rates resulted when we used the traditional approach (asking about emphysema and/or chronic bronchitis) than when we used a measure asking only about COPD. One explanation for this difference might be the terminology (eg, COPD vs emphysema) used by physicians when communicating with patients. Nelson and Hamilton 19 found that physicians and patients provided different responses on both name and nature of diagnosis when asked separately after a physician visit. This difference in terminology may be particularly likely for COPD, given evidence of limited health literacy among COPD patients 20 –22 and US adults in general. 23 Differences in terminology used by physicians when communicating with patients could influence how patients respond to self-report survey questions and ultimately could influence rates of COPD prevalence.
Another factor that could play a role in differing estimates resulting from different questions—particularly in which adults have reported emphysema and/or chronic bronchitis diagnoses but not COPD diagnoses—is confusion about acute bronchitis and chronic bronchitis. Respondents might answer affirmatively to a question about chronic bronchitis when they might instead have acute bronchitis that occurs periodically, unaware that the 2 conditions are different. A cognitive testing study provided support for this notion and suggested that surveys ask questions that distinguish between the 2 types of bronchitis. 24 Confusion about the 2 types of bronchitis might explain the surprisingly high prevalence rates of chronic bronchitis among younger adults and those who have never smoked. In previous years of the NHIS, 3% to 4% of children were reported to have a chronic bronchitis diagnosis, which further supports the hypothesis that recurrent episodes of acute bronchitis are reported as chronic bronchitis. 25
Lower prevalence estimates generated by using a measure of only COPD diagnosis may also have occurred because public awareness of COPD has historically been low. 13 Public awareness may be changing. The International COPD Coalition, which works to improve COPD awareness, conducted a survey and found that awareness improved since 2001. The coalition noted that in the United States, mass communication—including direct-to-consumer advertising of COPD products and education about COPD by foundations and other organizations—has improved awareness. 13
Differences in prevalence estimates resulting from the use of different questions raise the issue of how to accurately determine the prevalence of diagnosed COPD through current NHIS questions. Currently, no mechanism is in place for cross-validating patient-reported data with clinical tests. Research based on 2007-2010 National Health and Nutrition Examination Survey (NHANES) data included both patient-reported responses and bronchodilator spirometry data 26 and might have the potential for cross-validation. Unfortunately, bronchodilator spirometry data were collected in the NHANES from 2007 to 2012, when survey questions asked if participants had ever been diagnosed with emphysema and if participants had currently or ever been diagnosed with chronic bronchitis but not COPD. A question asking about COPD was not added to the NHANES until 2013-2014, when bronchodilator spirometry data were no longer collected. Regardless, research based on 2007-2010 NHANES data found that among US adults aged 40-79 who were eligible for spirometry testing, the prevalence of COPD based on self-reported diagnoses of only emphysema and/or chronic bronchitis was 5.2%. 26 This estimate was much lower than the prevalence determined by bronchodilator spirometry data, which ranged from 10.2% to 20.9% (depending on whether pre- vs postbronchodilator test results were used and which diagnostic criterion was used [fixed ratio vs lower limit of normal]). 26 These findings 26 do not reveal which combination of survey items is best for estimating the prevalence of diagnosed COPD but do add to evidence of the overall underestimation of COPD based on self-reported data rather than clinical data. Because no gold standard for clinical data on COPD exists, 27 this evidence of underestimation remained regardless of which test results and diagnostic criterion were used. 26
Practice Implications
Findings from this study allow for several recommendations on measuring diagnosed COPD prevalence based on self-reported data in US health surveys, such as the NHIS. First, using a question that asks respondents only about COPD diagnosis does not appear to be sufficient and results in a significantly lower COPD prevalence than does using questions asking about emphysema, chronic bronchitis, and COPD in combination. We recommend that a survey question asking respondents about COPD diagnosis only should not alone be used to estimate COPD prevalence. At the same time, combining questions about emphysema and/or chronic bronchitis diagnoses does not appear to be sufficient and results in significantly lower COPD prevalence than does using questions that combine all 3 (emphysema, chronic bronchitis, and COPD diagnoses). Therefore, the best option for measuring diagnosed COPD prevalence with national health survey data such as the NHIS might be to combine a question asking about COPD with questions asking about emphysema and chronic bronchitis. Furthermore, because of concerns about misreporting chronic bronchitis, particularly among younger adults, researchers might wish to consider limiting prevalence estimates to adults aged ≥40.
Further research could be conducted to better understand why differences in estimates exist. Future research should include investigating issues about cognition and understanding of COPD-related terminology (eg, acute vs chronic bronchitis; emphysema vs COPD) as well as other issues not directly addressed in this article, such as the reference period used in a survey question (eg, ever diagnosed vs diagnosed in past 12 months) and context effects (eg, the location of questions and order in which they appear). Ideally, such an investigation would include objective clinical measures such as bronchodilator spirometry (eg, the design of the BOLD [Burden of Obstructive Lung Disease] Initiative 28 ). Such an investigation might help to answer questions about why certain subgroups have disproportionately higher estimates of COPD than others. The high proportion of adults included in COPD estimates because they reported only a chronic bronchitis diagnosis was unexpected and might indicate an error in measurement. Thus, use of this survey question in measures of COPD prevalence warrants attention. All of these issues were beyond the scope of this study but could be investigated in future research to help develop more valid estimates of COPD prevalence based on self- or patient-reported data.
Prevalence rates from patient-reported diagnosis data provide critical information for evaluating public health programs aimed at respiratory health and monitoring national health objectives related to COPD. However, as shown in this study, prevalence rates can differ significantly depending on the question that is used. Understanding why these differences exist requires additional methodological research, but possible reasons revolve around doctor-patient communication about respiratory diagnoses. Nevertheless, epidemiologists interested in US surveillance of COPD should pay attention to the questions used to define diagnosed COPD and recognize that they affect the prevalence rates being reported in the overall population and among subgroups. By considering these issues, perhaps a clearer and more accurate understanding of the burden of COPD in the United States can be obtained.
Footnotes
Acknowledgments
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the National Center for Health Statistics, the Centers for Disease Control and Prevention, or the US Department of Health and Human Services.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.