
Abstract
Healthy People 2020 (HP2020) aims to improve population health outcomes through several objectives, including health communication and health information technology. We used 7 administrations of the Health Information National Trends Survey to examine HP2020 goals toward access to the Internet through broadband and mobile devices (N = 34 080). We conducted descriptive analyses and obtained predicted marginals, also known as model-adjusted risks, to estimate the association between demographic characteristics and use of mobile devices. The HP2020 target (7.7% of the US population) for accessing the Internet through a cellular network was surpassed in 2014 (59.7%), but the HP2020 target (83.2%) for broadband access fell short (63.8%). Sex and age were associated with accessing the Internet through a cellular network throughout the years (Wald F test, P <.05). The increase in the percentage of people accessing the Internet through mobile devices presents an opportunity for technology-based health interventions that should be explored.
Keywords
Healthy People 2020 (HP2020) outlines goals for the nation’s health for the year 2020 and includes a variety of health behaviors. 1 In recognition of the increasing importance of the Internet and mobile devices as a way to access health information, HP2020 also includes objectives for broadband (ie, high-speed transmission) access to the Internet and the use of mobile devices. The HP2020 goals are that 83.2% of the entire US population should have broadband access to the Internet and that 7.7% of the entire US population should be using mobile devices to access the Internet. 2,3 Monitoring the methods that people use to access online information is of continued interest to national public health planners.
The National Cancer Institute’s Health Information National Trends Survey (HINTS) tracks the public’s access to and use of information on cancer and health. 4 HINTS is a data source for tracking and assessing progress toward Healthy People objectives related to health communication and health information technology, and the data are often used to set the target goals for Healthy People objectives. Three authors of the present study used HINTS data to track HP2020 progress in access to the Internet. 5 Similarly, the objective of this study was to use data from HINTS to measure progress toward the HP2020 goals for broadband access to the Internet and use of mobile devices.
Methods
We integrated data from 7 administrations of HINTS: a publicly available, probability-based, cross-sectional survey of the US adult, civilian, noninstitutionalized population. Data were collected periodically from 2003 through 2014 (HINTS 1 to HINTS 4, cycle 4) by using varying sampling designs and modes of administration (eg, random-digit dialing, postal questionnaires), resulting in a nationally representative sample of 34 080 respondents across the 7 administrations (Table 1). HINTS methodology is documented elsewhere. 6 HINTS items include content on health communication, perceptions of health- and cancer-related information, and use of health information technologies. Sample sizes, response rates, and modes of administration are detailed elsewhere. 4 Because this study was a secondary data analysis of a publicly available data set, it was considered exempt from institutional review board approval.
Details of 7 administrations (N = 34 080 respondents) of the HINTS, 2003-2014a
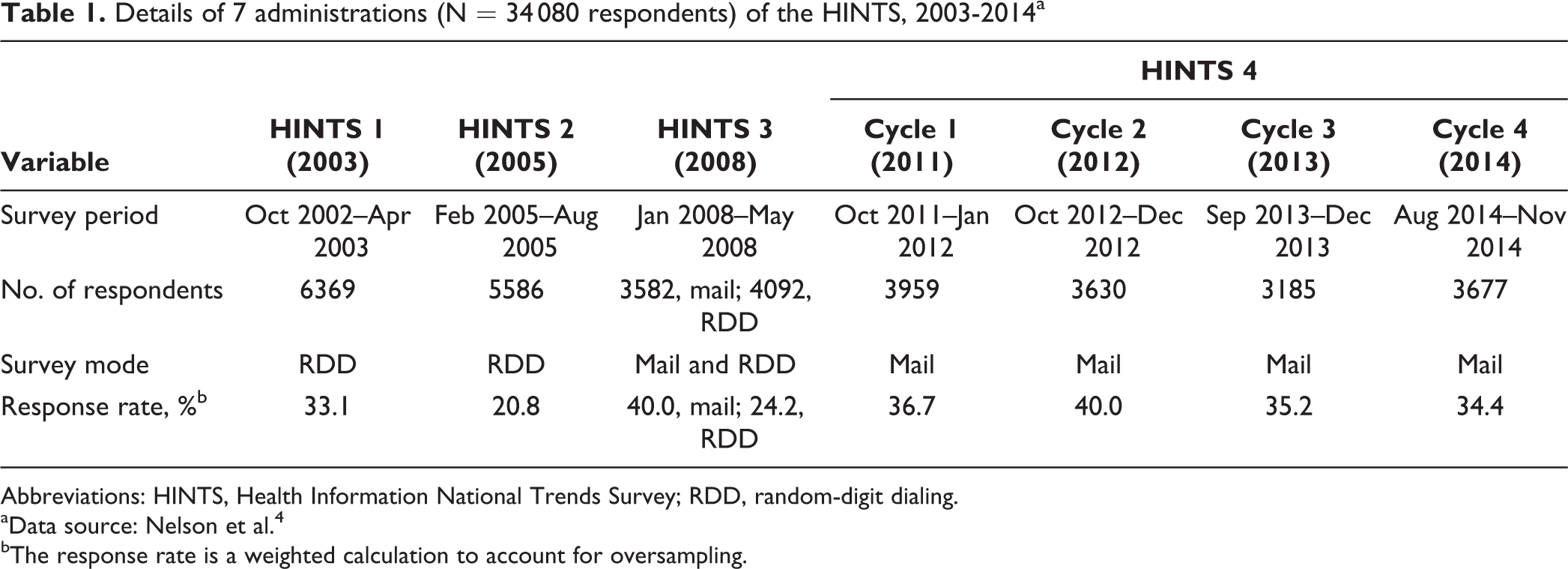
Abbreviations: HINTS, Health Information National Trends Survey; RDD, random-digit dialing.
aData source: Nelson et al. 4
bThe response rate is a weighted calculation to account for oversampling.
Measures and Statistical Analysis
We used the following item to assess the HP2020 goals for broadband access: “When you use the Internet, do you access it through…broadband such as DSL [digital subscriber line], cable, or FiOS [fiber optic service]?” (The wording was slightly different in HINTS 1 to HINTS 3 than in HINTS 4, cycles 1-4.) In addition, for mobile devices we assessed 2 items: (1) “In the last 12 months, have you used the Internet for any of the following reasons? Downloaded health-related information to a mobile device, such as an MP3 player, cell phone, tablet computer, or electronic book device?” (in HINTS 3 and HINTS 4, cycles 1 and 3) and (2) “When you use the Internet, do you access it through…a cellular network (ie, telephone, 3G/4G)?” (in HINTS 3 but worded differently and in HINTS 4, cycles 1-4).
We conducted descriptive analyses for all items. Because the baseline in 2008 for accessing the Internet through a cellular network was low (6.7%), we explored potential differences in access among various demographic characteristics, such as sex, age, race/ethnicity, education, and income. 3 We conducted logistic regression analyses with predicted marginals, also known as model-adjusted risks, to estimate the association between demographic characteristics (sex, age, race/ethnicity, education, and income) and accessing the Internet through a cellular network (“When you use the Internet, do you access it through…a cellular network?”). We included an interaction term between each demographic variable and survey year in the models to assess for differential change over time by each demographic characteristic. We conducted all analyses using SAS-callable SUDAAN (version 11.0) 7 to incorporate the sampling, replicate weights, and account for the complex sampling design.
Results
The weighted sample characteristics for each survey administration and cycle varied to some degree but in general were similar to the population estimates of the US Census. Most HINTS respondents were women, aged 18 to 34 years, and non-Hispanic white; had some college education; and had an annual household income of at least $75 000. Broadband access increased by about 43 percentage points from 2003 (32.7%; 95% confidence interval [CI], 30.9%-34.4%) to 2008 (75.8%; 95% CI, 72.7%-78.7%) but declined from 2011 (75.6%; 95% CI, 72.7%-78.3%) to 2014 (63.8%; 95% CI, 60.8%-66.8%). Internet access via cellular network increased from 2008 (6.7%; 95% CI, 5.4%-8.2%) to 2014 (59.7%; 95% CI, 56.8%-62.6%; Figure).
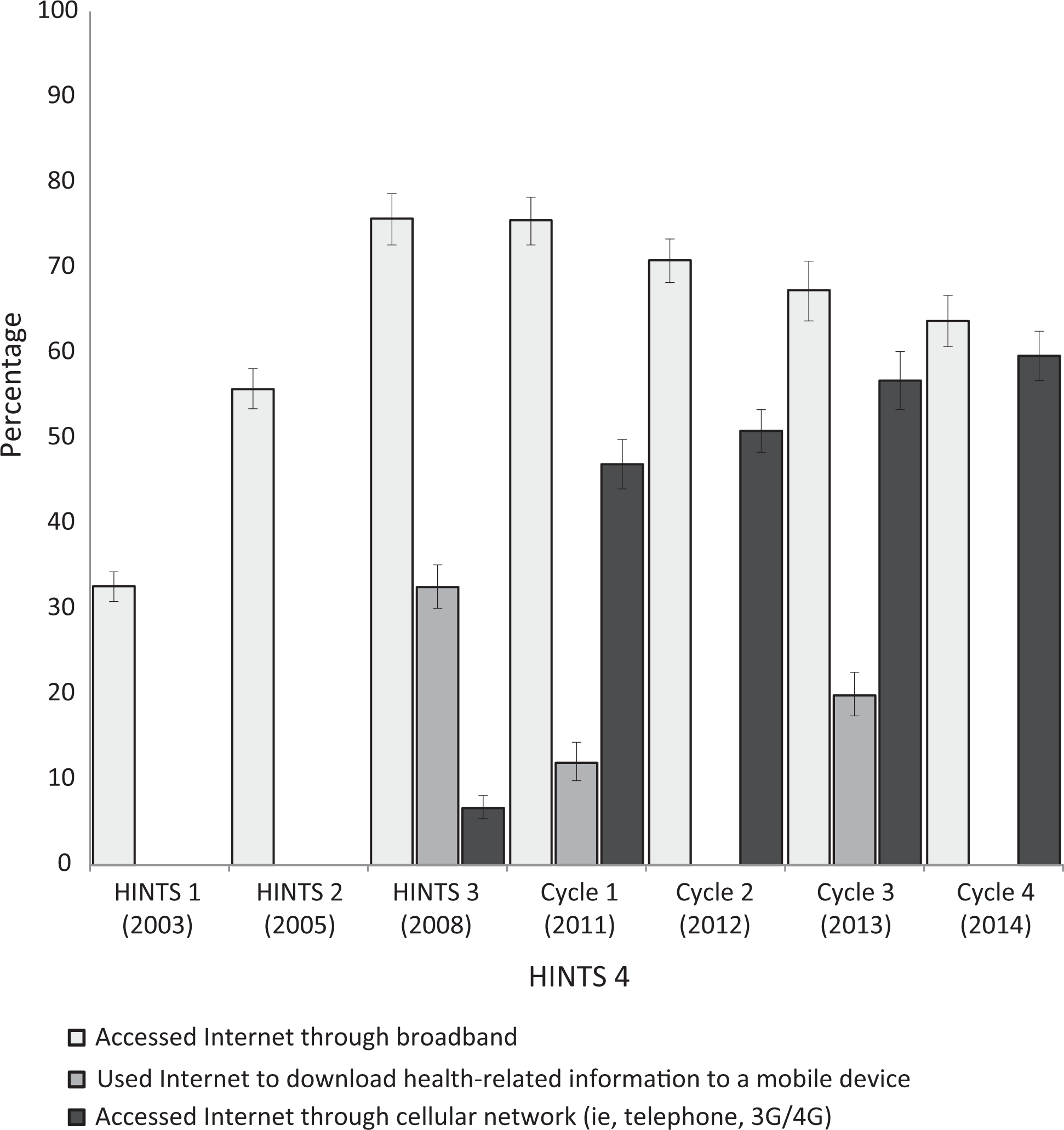
Percentage of the US adult population with access to the Internet via broadband and mobile devices, Health Information National Trends Survey (HINTS), 2003-2014. Survey question on using the Internet to download health-related information to a mobile device not asked in 2003, 2005, 2012, or 2014. Survey question on accessing the Internet through a cellular network not asked in 2003 or 2005. Error bars indicate 95% confidence intervals.
Among respondents accessing the Internet through a cellular network, the interaction between demographic characteristics and survey year was significant only for sex and age (Table 2). Women (62.3%) were more likely to access the Internet through a cellular network than men (60.4%) in 2014. Younger adults (aged 18-34) were more likely to access the Internet through a cellular network than adults aged ≥75 throughout the years, with an average separation of about 60 percentage points. The largest increases in accessing the Internet through a cellular network during 2011 to 2014 were among those aged 35 to 49 (from 46.8% in 2011 to 69.7% in 2014) and 50 to 64 (from 32.2% in 2011 to 46.3% in 2014). Overall, Hispanic and non-Hispanic African American people as compared with non-Hispanic white people, as well as respondents who had some college education as compared with those who had less than a college education, were more likely to access the Internet through a cellular network (percentages varied by year). Respondents with an annual household income ≥$75 000 were more likely to access the Internet through a cellular network than those in lower-income households during the study period (Table 2).
Predicted marginalsa for US adults accessing the Internet through a cellular network,b by demographic characteristics and survey year, HINTS, 2008-2014c
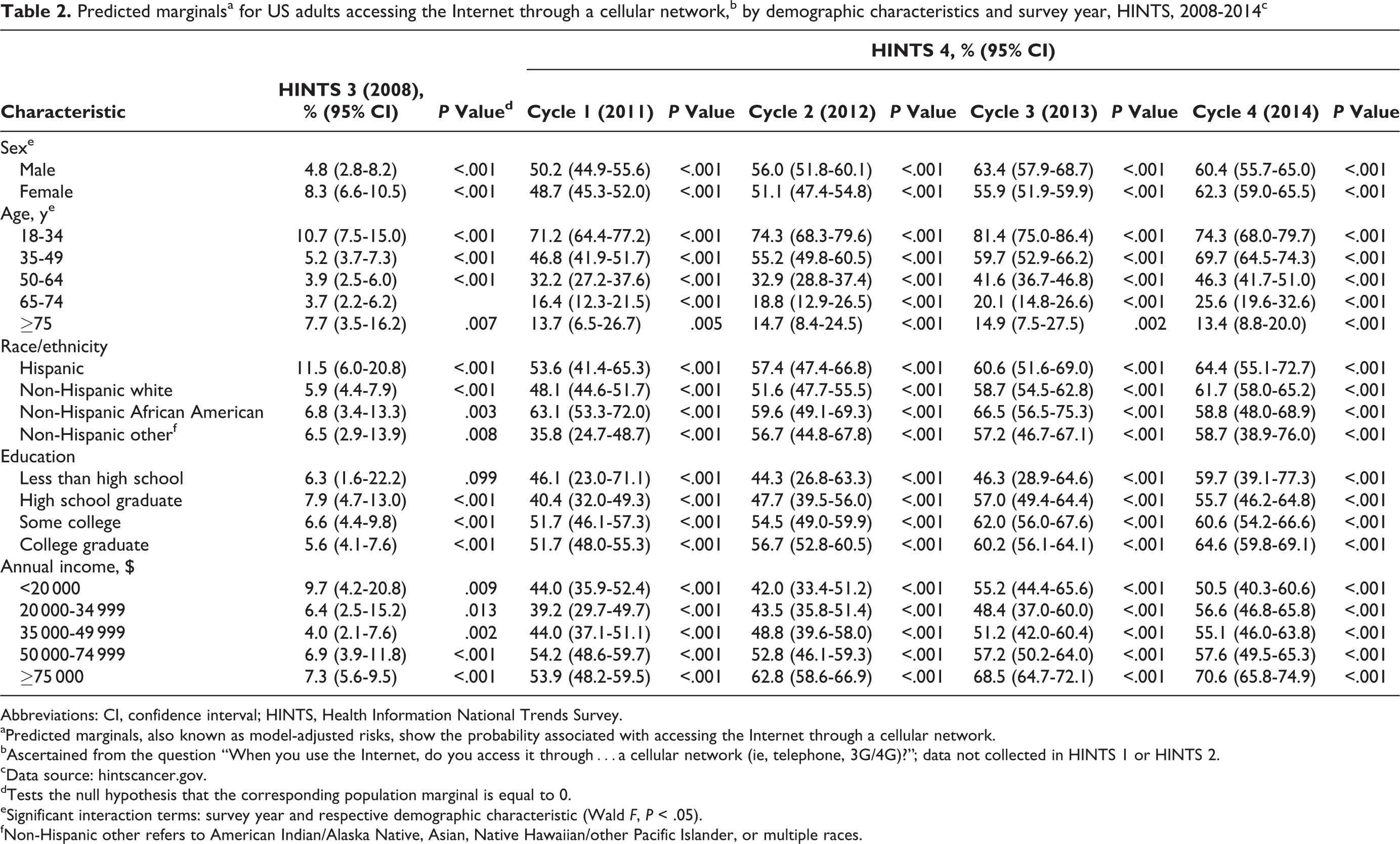
Abbreviations: CI, confidence interval; HINTS, Health Information National Trends Survey.
aPredicted marginals, also known as model-adjusted risks, show the probability associated with accessing the Internet through a cellular network.
bAscertained from the question “When you use the Internet, do you access it through…a cellular network (ie, telephone, 3G/4G)?”; data not collected in HINTS 1 or HINTS 2.
cData source: hintscancer.gov.
dTests the null hypothesis that the corresponding population marginal is equal to 0.
eSignificant interaction terms: survey year and respective demographic characteristic (Wald F, P < .05).
fNon-Hispanic other refers to American Indian/Alaska Native, Asian, Native Hawaiian/other Pacific Islander, or multiple races.
Discussion
Our study found that the percentage of respondents who had broadband Internet access declined from 75.8% in 2008 to 63.8% in 2014 and that those who reported accessing the Internet through a cellular network increased during the same period from 6.7% to 59.7%. People may be opting to use a cellular network via mobile devices rather than broadband to access the Internet.
The increasing percentage of people with access to the Internet via mobile devices presents a unique opportunity for health information technology–based interventions, as evidenced by the myriad mHealth applications and patient portals being made available to the public. 5,8 Such technologies offer new channels for patient activation and engagement, such as secure messaging between patients and providers and access to one’s electronic health records. 9,10 These tools also open up channels of communication and access to information for demographic groups that may face geographic barriers to direct health care services. Additionally, because most people carry their mobile devices with them throughout the day, immediate and timely communication among patients, providers, and caregivers is now possible. A better understanding of how people access the Internet and the disparities in Internet access among demographic groups would allow those designing mHealth applications and interventions to determine how to best communicate health information to certain segments of the public and create more opportunities for patient engagement.
Results from this study indicate that differences in Internet access via mobile devices remain across age groups, education, and income levels. This finding speaks to a “digital divide” among certain groups in Internet access—namely, that those who are older or are socioeconomically disadvantaged have less access than those who are younger or are socioeconomically advantaged. This divide has also been observed by the Office of the National Coordinator for Health Information Technology and other independent investigations. 11 -14 Thus, although health information technology communication channels present new opportunities for health-oriented interventions, investigators will need to understand the differences in access and usage when designing such interventions. Beyond questions of access, differences in health and digital literacy may persist independently of the closing gap in Internet access. 15,16 Several studies have noted that privacy and security issues, as well as willingness to use mobile technology for health purposes, are important considerations for health information technology–based interventions. 17,18 Strategies to monitor perceptions about these issues over time would help inform practice and policy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.