
Abstract
Objective:
The primary objective of this study was to estimate the percentage of individuals possibly eligible for lung cancer screening that report having discussed screening with a health care provider. The secondary objective was to investigate the associated factors of having patient–provider lung cancer screening discussion.
Methods:
Data from the Health Information National Trends Survey 2017 were used (n = 3217). Lung cancer screening eligibility was based on the criteria utilized by the Centers for Medicare and Medicaid Services. Gender, race, educational attainment, health insurance coverage, and usual source of health care were covariates. Current or former smokers ages 55–77 (n = 706) were considered potentially eligible for lung cancer screening (dependent variable).
Results:
Only 12.24% of individuals potentially eligible for lung cancer screening report prior discussion regarding lung cancer screening with a health care provider. Being eligible for lung cancer screening based on Centers for Medicare and Medicaid Services eligibility criteria was positively associated with the odds of a patient–provider lung cancer screening discussion (odds ratio = 3.95, 95% confidence interval = 2.48–6.30). Unlike gender, race, education, or insurance coverage, a usual source of health care was positively associated with a patient–provider screening discussion (odds ratio = 2.48, 95% confidence interval = 1.31–4.70).
Conclusion:
Individuals potentially eligible for lung cancer screening are more likely to have screening discussions with a health care provider. Having a usual source of health care may increase the odds of such a discussion, while patients are not discriminated based on race, gender, education, and insurance coverage. However, the relatively low rate (12.24%) of reported patient–provider lung cancer screening discussion indicates that significant barriers still remain.
Keywords
Introduction
Lung cancer is the leading cause of cancer-related deaths for both genders in the United States. In total, 234,030 new cases of lung cancer were expected to be diagnosed and 154,050 lung cancer–related deaths were expected to occur in the United States in 2018. Lung cancer is the leading cause of cancer-related death in the United States and worldwide. 1 Unfortunately, in contrast to breast cancer, a malignancy with both high screening rates and 5-year survival, most lung cancer patients have historically been diagnosed at later stages of disease, leading to a low overall 5-year relative survival rate of only 17% for men and 24% for women. 2
The National Lung Screening Trial (NLST) that included more than 50,000 participants showed a roughly 20% decrease in lung cancer deaths in individuals participating in annual low-dose computed tomography (LDCT) screening after 8 years of follow-up. 3 These robust data were further supported by a combination of evidence from smaller trials4,5 and input from several prominent organizations, including the American Cancer Society, the American College of Radiology, and the American College of Chest Physicians. Based on all of these data, the US Preventive Services Task Force (USPSTF) issued recommendations for lung cancer screening (LCS) in defined high-risk populations using LDCT imaging.6–8 Despite small variations in the recommended range of ages to screen (USPSTF, 55–80 years old, and American Cancer Society, 55–74 years old), there was a general consensus in the recommendation that health care providers should discuss LCS with individuals who (1) had a 30-pack year smoking history, (2) currently smoke, or (3) have quit smoking within the past 15 years. The Centers for Medicare and Medicaid Services (CMS) approved paid coverage of LDCT for LCS in these high-risk patients between the ages of 55 and 77 years in February 2015. 9
Shared decision making has been shown to be critical in the effectiveness of any large-scale cancer screening program. 8 In addition, shared decision making has been mandated as a requirement for reimbursement by the CMS. 9 Although there exist resources (including online materials) that provide patients with information regarding LCS, it has been documented in established cancer screening programs that patient–provider communication plays a central role in cancer screening adherence. 10 As LCS becomes increasingly available nationally, a clear understanding of the factors that affect the discussion of LCS between a patient and a health care provider is necessary. This understanding could ultimately increase patient enrollment and participation in this relatively newly established screening program. A recently published report on patient–provider discussion about LCS shows that racial disparities may affect having LCS discussions with providers as patients age. 11
This study sought to determine factors that may be associated with a discussion of LCS between patients and health care providers. In addition, this study looked to assess whether individuals who potentially meet CMS eligibility criteria for LCS (based on age and smoking history) exhibited increased odds of discussing LCS with their providers and the frequency at which such discussions are reported in this population. Finally, this study sought to elucidate the association between race, gender, education level, having a usual health care provider, and health insurance coverage and LCS discussions.
Materials and methods
Design and setting
This work is a secondary data analysis of a cross-sectional study from the Health Information National Trends Survey (HINTS-5), 2017. HINTS is a nationally representative survey that has been periodically administered by the National Cancer Institute (NCI) in the United States since 2003. HINTS is used to set national policies in the field of cancer. It also generates hundreds of research studies using various aspects of this questionnaire. 12 The goal of HINTS is to provide a comprehensive understanding regarding American adults’ access to, and use of, cancer and health-related information.13,14 The HINTS-5, Cycle 1, was conducted between January and May 2017. The HINTS questionnaire is available at: https://hints.cancer.gov/docs/Instruments/HINTS_FDA_English_Annotated_Survey.pdf
Ethical considerations
All participants provided written informed consent. The Westat’s Institutional Review Board (IRB) approved the HINTS-5 study protocol (Westat’s Federalwide Assurance (FWA) no. FWA00005551, Westat’s IRB no. 00000695, project OMB no. 0920-0589). The NIH Office of Human Subjects exempted HINTS from IRB review.
Sampling
The target population of HINTS is non-institutionalized American adults (18 years or older) who live in the United States. HINTS used a two-step sampling design. The first step was a stratified sample of addresses that were derived from all US residential addresses. In the second step, one adult from each household was selected to answer questions. The Marketing Systems Group (MSG) was used to prepare the list of addresses.13–16
Surveys
The HINTS surveys were mailed to the participants. To encourage participation, monetary incentive was included in the mailings. Two toll-free telephone numbers (one for English calls and one for Spanish calls) were provided to respondents. The overall response rate was 32.4%.13–15
Study variables
Evaluation of the HINTS dataset was limited to individuals’ reported age, gender, race, socioeconomic status (SES; education), smoking status, usual source of health care, insurance coverage, and discussion of LCS with a health care provider. Using the below definitions, these values were subsequently used to generate study variables used for analysis.
Independent variables
Potential LCS eligibility
A dichotomous variable (0 not eligible, 1 potentially eligible) was chosen for this study. Potential eligibility is defined as ages between 55 and 77 with a history of smoking. (Age range was derived from CMS reimbursement criteria. A description of smoking history is a requirement of CMS). However, specifics of pack years or time from quitting in former smokers are not recorded in the HINTS dataset.
Demographic factors
Age (range: 18–101) was a continuous measure. Gender was a dichotomous variable (0 female, 1 male). Race was a dichotomous variable (0 Whites, 1 non-Whites).
Education
A five-level ordinal scale was used to measure education level: (1) less than high school, (2) high school graduate, (3) attended college, (4) Bachelor’s degree, and (5) post-baccalaureate degree. Education was then operationalized as a continuous measure, with a potential range from 1 to 5, with a higher score reflecting increased educational attainment.
Ever smoker and current smoker
Ever or current smoking status was measured using the following two items: (1) “Have you smoked at least 100 cigarettes in your entire life?” and (2) “How often do you now smoke cigarettes?” Responses to the first item were yes/no. Responses to the second item were (1) Everyday, (2) Some days, and (3) Not at all. An ever smoker was defined as a positive response to the first question. Current smoker was defined as positive response to the first question and a response of “1” or “2” to the second question (i.e. individuals who have smoked at least 100 cigarettes in their life and at the time of the survey smoked cigarettes every day or some days).
Usual health care provider
Availability of health insurance was measured using the following insurance types: (1) insurance purchased from insurance companies, (2) Medicare (for people 65 and older, or people with disabilities), (3) Medicaid, Medical Assistance, or other government assistance plans, (4) TRICARE and any other military health care, (5) Veterans Affairs, (6) Indian Health Services, and (7) any other health coverage plan. Based upon a positive response to any of these questions, insurance was operationalized as a dichotomous variable (0 without insurance, 1 with insurance).
Dependent variable
A single item was used to measure the reported patient–provider LCS discussion. The item read “In the past year, have you talked with your doctor about having a test to check for lung cancer?” Responses included yes and no.
Statistical analysis
To accommodate the complex sampling design of the HINTS study, we used Stata version 13.0 (Stata Corp., College Station, TX, USA) for data analysis. Standard errors (SE) were re-estimated using the Taylor series linearization technique. As a result of adjusting weights, our rates and inferences are representative to the US general population. For descriptive analysis, we used mean (SE) and proportions (relative frequencies). For sample size calculation, as both our independent variable and dependent variables were binary, we calculated the sample size to compare two proportions, using two-sided p value at 0.05, to test the following hypothesis: H0: pA – pB = 0. With a Type I error of 0.5 and a Type II error of 20%, a sample size of 2621 individuals gives us a power of 80% to detect a difference in the prevalence of LCS patient–provider discussion in those who meet (pB20%) and those who do not meet (pA18%) the CMS criteria for LCS. For bivariate analyses, we used the Spearman correlation test to explore the unadjusted correlations between the study variables in the pooled sample. We ran our bivariate in the pooled sample to determine whether the LCS eligibility correlates with demographic, SES, and LCS discussion. If we had run the correlations among participants who were eligible, we could not explore bivariate correlates of eligibility. For multivariate analysis, we used logistic regression models. From our regression models, we reported beta coefficient, Wald statistics, adjusted odds ratios (ORs), SEs, 95% confidence intervals (CIs), and p values. In our logistic regression model, potential LCS eligibility, gender, race, education, usual health care provider, and insurance were the independent variables. The frequency of patient-reported discussion regarding LCS with a health care provider served as the dependent variable. A second model was run for individuals with potential LCS eligibility to investigate which variables affect the odds of a patient–provider LCS discussion in the setting of potential eligibility.
Model 1 is among all HINTS participants and includes potential LCS eligibility as a variable. Model 2 is performed among those whose potential LCS eligibility variable has a value of “1—possibly eligible.” In this subset of the participants (limited to individuals age between 55 and 77 with positive ever smoker status), both age and current smoker are included as independent variables. Model 3 is among all HINTS participants and also includes age and current smoking status in addition to potential LCS eligibility as independent variables. Model 4 is similar to model 3, but without potential LCS eligibility as a variable.
Results
Descriptive statistics
Table 1 summarizes the descriptive statistics of the sample. Participants had an average age of 49 years. Gender distribution approximated national averages with 51% (n = 1642) females; 66% of the participants were White; 91% of the participants reported some form of insurance and 66% reported having a usual health care provider; 38% of participants were determined to be in the ever smoker category. Only 12.24% of the potentially eligible LCS individuals based on age and positive ever smoker status reported having discussed LCS with a health care provider (Table 1).
Descriptive statistics (n = 3217).
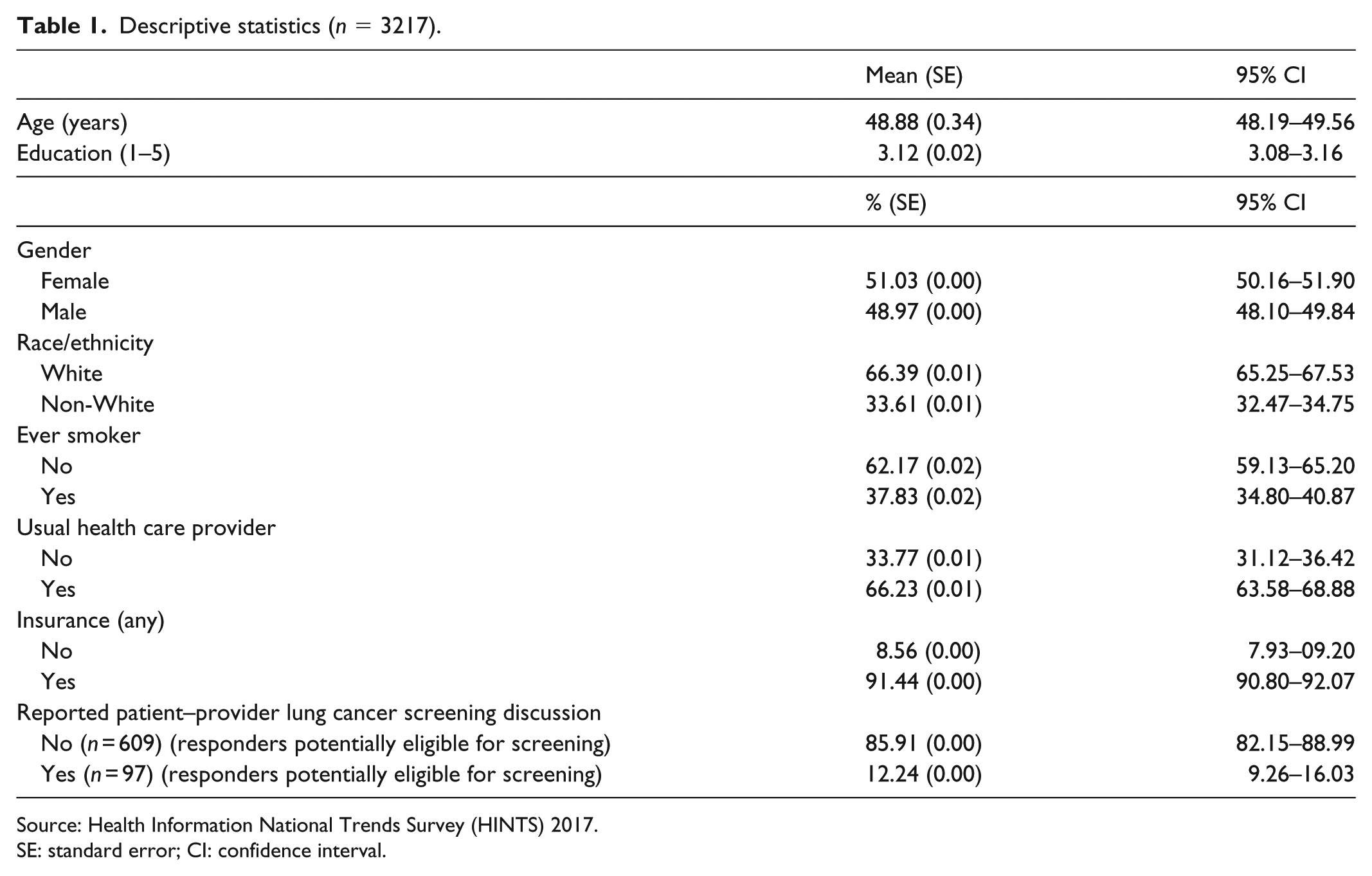
Source: Health Information National Trends Survey (HINTS) 2017.
SE: standard error; CI: confidence interval.
Bivariate analysis
Table 2 summarizes the correlations between study variables in the pooled sample. As shown in Table 2, potential LCS eligibility (r = 0.17), current smoker status (r = 0.17), ever smoker status (r = 0.18), having a usual health care provider (r = 0.06), male gender (r = 0.06), and age (r = 0.12) were positively correlated with the reported patient–provider LCS discussion. Education was negatively correlated with the reported patient–provider LCS discussion (r = –0.09). Race and insurance did not correlate with the reported patient–provider LCS discussion.
Correlation matrix (n = 3217).

Source: Health Information National Trends Survey (HINTS) 2017.
p < 0.05.
Multivariate analysis
Table 3 shows the summary of logistic regression models with demographic, social, and behavioral factors associated with receiving an LCS message in the sample. Potential LCS eligibility (OR = 3.95, 95% CI = 2.48–6.30) and having a usual health care provider (OR = 2.48, 95% CI = 1.31–4.70) showed a positive association with the reported patient–provider LCS discussion. A second model (model 2) limited to the subset of individuals with potential LCS eligibility in which current smoker status (OR = 2.73, 95% CI = 1.42–5.27) and age (OR = 1.06, 95% CI = 1.00–1.11) showed a positive association with patient–provider LCS discussion. Two additional models were generated (models 3 and 4) to confirm findings (Supplementary Table).
Summary of logistic regressions.

Source: Health Information National Trends Survey (HINTS) 2017.
SE: standard error; OR: odds ratio; CI: confidence interval.
Outcome: Who is discussing lung cancer screening with health care providers in the United States? Model 1 is among all HINTS 2017 participants and includes potential lung cancer screening eligibility as an independent variable. Model 2 is performed using only the subset of individuals who are potentially eligible for lung cancer screening and also includes age and current smoker as independent variables.
Discussion
This study demonstrated that individuals potentially meeting the LCS eligibility criteria are more likely to have discussed screening with a health care provider compared to individuals not meeting the LCS eligibility criteria. Furthermore, the incidence of the reported patient–provider LCS discussion was not influenced by patients’ gender, race, education, or insurance coverage. However, we found that having a usual health care provider increases the chance of having discussed LCS with a provider, independent of potential eligibility. In high-risk individuals (those potentially eligible for LCS), advanced age and current smoking status increased the odds of having discussed screening with a provider. Although this does not strictly follow LCS recommendation guidelines, it perhaps reflects a more individualized approach given potential increased risk of lung cancer in the setting of continued tobacco use and increased age.
Despite several guidelines recommending annual LCS using LDCT in high-risk individuals, the reported LCS participation rates have remained low. This is in spite of the CMS-approved coverage of LDCT screening for high-risk individuals. Based on a recent American Cancer Society study, there were an estimated 6.8 million current and former smokers eligible for LCS in 2015. Only 262,700 individuals (3.9%) received LCS in the same year. 17 These findings and our own analysis showing that only 12.24% of participants potentially eligible for screening discussed LCS with a health care provider reinforce the slow adoption of screening. However, our analysis also demonstrated that individuals between 55 and 77 years old with history of smoking (referred to as potential LCS eligibility in the results above) are involved in patient–provider discussion regarding LCS at a higher rate. This suggests that the screening guidelines have at a minimum triggered some discussions regarding LCS with the appropriate patient population. Overall, there clearly remains room for improvement, potentially with barriers to widespread adoption yet to be elucidated. Our results should be compared to an older report that found the prevalence of patient–provider discussion about LCS at 17% in 2012 and 10% in 2014. 18 There are minor differences in our inclusion criteria compared to these studies in which patients 55–80 years old were included based on USPSTF recommendation for LCS in 2013. By comparing our results, we can conclude that, in spite of the CMS-approved coverage of LDCT screening in 2015, the patient–provider discussion prevalence for LCS is still very suboptimal.
Based on our findings, both potentially eligible individuals as well as those maintaining a usual health care provider are more likely to report prior discussions of LCS, regardless of race or attained education level. Using data from more widely available cancer screening programs, it has been shown that cancer screening participation is associated with multiple factors such as race, gender, and SES. In particular, individuals with higher education, parental status, and life-course SES have been shown to be positively associated with breast and cervical cancer screening. 19 SES indicators such as education attainment of the patients were likewise found to be positively associated with colon cancer screening participation in the Canadian Community Health Survey, 2011–2012. 20 Such population-based assessments have yet to be comprehensively performed on the LCS target population; however, our data suggest that education level did not significantly affect the odds of patient–provider discussion regarding screening. The correlation between eligible individuals having discussed LCS recommendations and ultimate successful participation in a screening program has yet to be elucidated and is beyond the scope of this study.
Gender inequality in some cancer screening has been reported. Women are less likely to be screened for colorectal cancer in the United States.21,22 In a study conducted in central Italy, women showed a lower, although not significant, participation in colon cancer screening with colonoscopy. 23 Although lung cancer rate has declined in males in the past three decades and the incidence rate has increased in women, lung cancer is still more common in men than women. 24 This raises the potential for disparate screening rates similar to colon cancer. However, our analysis suggests that men and women receive comparable rates of patient–provider discussion regarding LCS, although the rate of screening participation following such discussions was not evaluated. In a recently published systematic review, researchers found over-representation of male participants in LCS programs. 25
Physician recommendation for mammograms has been determined to be a major motivator for patients’ compliance to breast cancer screening. 26 Such recommendations can be potentially affected by race and have been found to occur less commonly in Black women. 17 Awareness of tests for colorectal cancer screening is also lower among African Americans than Whites. 27 Black women are also less likely than White women to be aware of and use breast cancer screening tests (despite higher rates of compliance in those participating in screening). 28 Although neither awareness nor use of LCS was assessed, our analysis demonstrates that race does not affect the odds of patient–provider LCS discussion. In a recently published study assessing the effect of age on the LCS patient–provider discussion rate, researchers reported that Blacks receive fewer messages regarding LCS as a result of aging. 11 This demonstrates that although there is no gender difference in the LCS patient–provider discussion rate, Blacks, unlike Whites, do not receive continued LCS messages from their health care providers as they get older.
It is reported that the lack of health care insurance is associated with the significantly decreased use of recommended screening for breast, colorectal, and cervical cancers. 29 Although health insurance is one of the main enablers for health care access, 30 our results showed no difference in the rate of patient–provider discussion regarding LCS based on insurance status. Although the lack of health insurance coverage may be a significant barrier to obtaining a screening CT due to an increase of the out-of-pocket expense, assessment of the effect of insurance status on LCS participation was beyond the scope of our analysis.
Usual source of care, as defined by having a single health care provider seen most often, was positively associated with patient–provider LCS discussion, independent of potential eligibility criteria, insurance, and SES. Analogous findings have been found in established screening programs, with women with no regular source of care. These women have significantly less breast cancer screening awareness compared to women who have a regular source of care such as doctor’s office, hospital outpatient, or public health clinic. 28 It has also been shown that a greater number of office visits in any setting are associated with a greater likelihood of undergoing mammography. 31 Given our findings and results of prior studies with respect to other large-scale screening programs, it may be inferred that established patient–provider relationships prove advantageous in promoting preventive health measures such as cancer screening.
The current findings have several implications for clinical practice and public health programs promoting LCS participation. Although our data suggest that the appropriate populations are being targeted to some extent for LCS (without clear evident bias with respect to demographic factors), the low rate (12.24%) of reported patient–provider discussion in those potentially eligible for LCS indicates that significant barriers may still exist stifling widespread adoption/availability of screening for eligible individuals. The results may guide health policies that aim to expand LCS participation or further promote research to elucidate factors limiting participation. An active approach to encouraging rapid adoption of LCS programs is of particular importance given that lung cancer remains the leading cause of cancer death in both men and women in America, 1 with screening having demonstrated potential to increase survival and reduce costs. 3 As with any screening program, patient education and early targeted discussion of the risks and benefits of screening in susceptible populations are important and recommended.9,32 Although our data are reassuring in that no definite bias with regard to race, gender, and education was identified in the occurrence of patient–provider screening discussions, individuals without a usual health care provider appear less likely to be targeted despite representing a large portion of the evaluated population (33.77%).
Limitations
Our study has a number of limitations, some of which have been briefly discussed above. Most significantly, this study focused on LCS patient–provider discussions without determination of ultimate LCS participation. We also do not know whether the patient or the provider initiated the discussion. Furthermore, limits of the HINTS dataset allowed for the evaluation of individuals potentially eligible for LCS without the ability to assess for details of tobacco use (such as pack years and time since quitting in former smokers) necessary to definitively establish screening eligibility by CMS guidelines or USPSTF criteria, rather than definite, indication for LCS. However, the HINTS dataset has been used for the investigation of high-risk lung cancer patients.11,33,34 Furthermore, the required shared decision-making visit between the health care provider and patient, as defined by CMS, is an encounter in which benefits and harms of screening (including the possibility of over-diagnosis, false-positive findings, and total radiation exposure) are shared and discussed prior to patients’ decision to participate. 18 This study is limited in this regard as the precise breadth and details of information discussed between patients and health care providers were not evaluated in HINTS, with data reflecting only whether a patient recalled speaking with their physician regarding “a test to check for lung cancer.” Like all survey studies, our study might suffer from recall bias. Therefore, this study provides preliminary report and requires further investigation.
Conclusion
In conclusion, our analysis shows that only 12.24% of patients potentially eligible to receive LCS report having discussed LCS with their health care. Appropriately, individuals potentially meeting the LCS eligibility criteria are more likely to report such a discussion. Furthermore, the incidence of the reported patient–provider LCS discussion was not influenced by patients’ gender, race, education, or insurance coverage. This is an indicator of the lack of bias of the providers in providing such messages to the right (high-risk) individuals. Overall, this suggests a preventive health benefit of an established patient–provider relationship; having a usual health care provider is positively associated with LCS discussions. Although these findings suggest that recommendations for LCS have at a minimum triggered some provider discussion regarding screening with the appropriate population, the low rate of such patient–provider interactions in those potentially eligible for screening indicates that significant barriers may still exist stifling widespread adoption/availability of screening. More research is necessary to evaluate the potential disparities of race, gender, and SES with respect to the frequency of ultimately proceeding with LCS. This work could further elucidate factors that contribute to low participation rates. Ultimately, a concerted effort by health care providers, public health organizations, and governing bodies will likely be required to promote rapid adoption and increased availability of LCS programs to attain maximal benefit.
Supplemental Material
Supplementary – Supplemental material for Lung cancer screening patient–provider discussion: Where do we stand and what are the associated factors?
Supplemental material, Supplementary for Lung cancer screening patient–provider discussion: Where do we stand and what are the associated factors? by Hamid Chalian, Pegah Khoshpouri, Arya M Iranmanesh, Joseph G Mammarappallil and Shervin Assari in SAGE Open Medicine
Footnotes
Acknowledgements
The authors would like to thank the HINTS team which provided the publicly available data.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The Westat’s Institutional Review Board (IRB) approved the HINTS-5 study protocol (Westat’s Federalwide Assurance (FWA) no. FWA00005551). The NIH Office of Human Subjects exempted the HINT from IRB review.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from all subjects before the study.
Supplemental material
Supplemental material for this article is available online.
Trial registration
This study was registered under Westat’s IRB no. 00000695 and the project OMB no. 0920-0589.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.