
Abstract
Objective:
We determined cause-specific mortality prevalence and risks of Gulf War deployed and nondeployed veterans to determine if deployed veterans were at greater risk than nondeployed veterans for death overall or because of certain diseases or conditions up to 13 years after conflict subsided.
Methods:
Follow-up began when the veteran left the Gulf War theater or May 1, 1991, and ended on the date of death or December 31, 2004. We studied 621 901 veterans who served in the 1990-1991 Persian Gulf War and 746 247 veterans who served but were not deployed during the Gulf War. We used Cox proportional hazard models to calculate rate ratios adjusted for age at entry to follow-up, length of follow-up, race, sex, branch of service, and military unit. We compared the mortality of (1) Gulf War veterans with non–Gulf War veterans and (2) Gulf War army veterans potentially exposed to nerve agents at Khamisiyah in March 1991 with those not exposed. We compared standardized mortality ratios of deployed and nondeployed Gulf War veterans with the US population.
Results:
Male Gulf War veterans had a lower risk of mortality than male non–Gulf War veterans (adjusted rate ratio [aRR] = 0.97; 95% confidence interval [CI], 0.95-0.99), and female Gulf War veterans had a higher risk of mortality than female non–Gulf War veterans (aRR = 1.15; 95% CI, 1.03-1.28). Khamisiyah-exposed Gulf War army veterans had >3 times the risk of mortality from cirrhosis of the liver than nonexposed army Gulf War veterans (aRR = 3.73; 95% CI, 1.64-8.48). Compared with the US population, female Gulf War veterans had a 60% higher risk of suicide and male Gulf War veterans had a lower risk of suicide (standardized mortality ratio = 0.84; 95% CI, 0.80-0.88).
Conclusion:
The vital status and mortality risk of Gulf War and non–Gulf War veterans should continue to be investigated.
Between August 1990 and July 1991, approximately 700 000 US troops were deployed to the Persian Gulf. Potentially harmful exposures during the Gulf War included oil well fire smoke, chemical and biological warfare compounds, multiple vaccinations, depleted uranium, pesticides, and physical and psychological stressors. 1 –3 Concern persists about the possible adverse health effects of service during the Persian Gulf War. Studies show greater illness among Gulf War veterans compared with non–Gulf War veterans, including more self-reported medical and psychiatric conditions and poorer self-perceptions of general health. 4 –7 Gulf War veterans have more psychological illnesses, including posttraumatic stress disorder, and are at greater risk for chronic multisymptom illness than nondeployed veterans. 6 –13 Many symptoms reported by Gulf War veterans—such as back pain, joint pain, headaches, and fatigue—have not been attributable to a diagnosable disease. 5
Historically, Gulf War and non–Gulf War veterans have had lower overall mortality rates than the US population. 14 However, Gulf War veterans have had a greater risk of death from accidents, including motor vehicle accidents, than non–Gulf War veterans. 14 –17 The risk of death from motor vehicle accidents was greatest within 1 year after leaving the Gulf War theater but decreased after 7 years. 14
Concerns remain about the long-term health effects of potential exposure to harmful chemicals during the Gulf War. The nerve agents sarin and cyclosarin may have been released when US forces detonated a weapons cache at Khamisiyah, Iraq, from March 10 through March 13, 1991. A greater risk of brain cancer mortality among army Gulf War veterans who were exposed at Khamisiyah as compared with those not exposed was reported at 7 and 13 years after the war. 18,19 Other studies found associations between exposure at Khamisiyah and cognitive dysfunction, central nervous system pathology, immunosuppression, and decreased neurobehavioral functioning. 20 –27 However, clinical examinations of Gulf War veterans did not find a difference in the prevalence of distal symmetric polyneuropathy between those exposed and not exposed at Khamisiyah. 28 A health survey of Gulf War veterans found no adverse health effects among army veterans exposed at Khamisiyah. 29 A study conducted to determine if Khamisiyah exposure could explain the increased risk of motor vehicle crash deaths among Gulf War veterans showed no increase in risk of motor vehicle crash deaths between Khamisiyah-exposed and nonexposed veterans. 30 Another study found no differences in hospitalizations or self-reported medical conditions 9 years after the war. 31
Researchers, veterans, and clinicians are concerned about potential health effects resulting from soldiers’ exposure to Kuwaiti oil well fires during the Gulf War. Several studies reported an association between acute respiratory conditions and self-reported exposure to oil well fire smoke. 32,33 A survey of Australian Gulf War veterans found a greater frequency of self-reported lung conditions, including asthma, among those exposed to oil well fire smoke, although no evidence for ventilatory abnormalities was found after spirometric testing. 33 One study found an association between asthma and self-reported exposure to oil well fire smoke among US Gulf War veterans with high levels of exposure. 34 Another study found no pulmonary abnormalities among Gulf War veterans compared with non–Gulf War veterans 10 years after the war. 35 Other research found no increase in postwar hospitalizations among Gulf War veterans exposed to oil well fire smoke. 36
This study extends the follow-up period to 13 years (1991-2004) and compares cause-specific mortality risk among Gulf War veterans, non–Gulf War veterans, and the general US population.
Methods
The study cohort included 621 901 Gulf War veterans and 746 247 non–Gulf War veterans. To be eligible for the cohort, Gulf War veterans must have served in the Persian Gulf between August 1, 1990, and March 1, 1991—the period of armed conflict. Troops that arrived in the Persian Gulf after March 1, 1991, were excluded from the cohort. We selected veterans in the non–Gulf War group from a stratified random sample of military personnel, including reserve and National Guard members, who were in the military at the time of the Gulf War but were not deployed to the Persian Gulf. The US Department of Defense’s Defense Manpower Data Center supplied data on demographic and military characteristics for the study cohort, including race, date of birth, marital status at entry to follow-up, sex, military rank, branch of service, and unit component (ie, active duty, reserve, National Guard). This study was reviewed and approved by the Washington DC VA Medical Center Institutional Review Board.
For Gulf War veterans, the follow-up period began on the date that the veteran left the theater alive; for non–Gulf War veterans, the follow-up period began on May 1, 1991. Follow-up ended on the date of death or on December 31, 2004, whichever was earlier. We determined vital status by using the US Department of Veterans Affairs database, Beneficiary Identification and Records Locator Subsystem, in combination with the Social Security Administration Death Master File. The Beneficiary Identification and Records Locator Subsystem contains records on veterans who are eligible for death benefits and other benefits and identifies deceased veterans who have not yet been reported in the Social Security Administration file. We obtained cause-of-death data from either a death certificate located in the veteran’s claim folder or from the National Death Index Plus. Since 1997, the National Center for Health Statistics has provided cause-of-death codes by underlying cause using the International Classification of Diseases. A nosologist blinded to deployment status coded any death certificate obtained from claim folders using the International Classification of Diseases, Ninth Revision (ICD-9). 37
We used the 2000 plume model developed jointly by the Department of Defense and the Central Intelligence Agency to determine exposure at Khamisiyah. 38 In our study cohort, 98 406 army veterans who were considered potentially exposed to nerve agents were categorized as having been exposed for 1 day or ≥2 days.
The Department of Defense provided data on oil well fire smoke exposure, which are based on air and soil samples gathered during the Gulf War when the fires were burning. 39 For this study, veterans who were exposed to at least 0.26 mg of total suspended particulate per cubic meter of air for at least 1 day were considered exposed. Based on this criterion, 123 478 army veterans in this study cohort were considered exposed. Approximately 13% of army Gulf War veterans were exposed to nerve agents at Khamisiyah and to oil well fire smoke.
We calculated person-years at risk of dying and compared the relative frequency of overall and specific causes of death between Gulf War veterans and non–Gulf War veterans as well as between Khamisiyah-exposed and nonexposed army Gulf War veterans. We used crude death rates to calculate unadjusted rate ratios. We calculated adjusted rate ratios (aRRs) using Cox proportional hazard models, which included the following covariates: age at entry to follow-up, length of follow-up, race (white/nonwhite), sex, service branch, and type of military unit. We conducted analyses collectively as well as by sex. The cause-specific categories of mortality and their ICD-9 codes included disease-related causes (001-799), infectious and parasitic disease (001-139), all cancers (140-208), circulatory system (390-459), respiratory system (460-519), digestive system (520-579), all external causes (E800-E999), all accidents (E800-E929), motor vehicle accidents (E810-E825), suicide (E950-E959), and homicide (E960-E969). Analyses of Khamisiyah-exposed and nonexposed army veterans also controlled for oil well fire smoke exposure and included ICD-9 codes for lung cancer (162), chronic obstructive pulmonary disease (490-492, 494, 496), and cirrhosis of the liver (571).
We calculated standardized mortality ratios (SMRs) to compare observed deaths among veterans with expected deaths based on the US population using the National Institute for Occupational Safety and Health Life Table Analysis System. 40 We assessed significance using 95% confidence intervals (CIs). We analyzed data using SAS version 9.4. 41
Results
Compared with non–Gulf War veterans, Gulf War veterans were more likely to be male (93.0% vs 86.7%), to be younger (mean age in 1991: 28 vs 30 years), and to have served in active component units (83.3% vs 70.2%). Gulf War veterans and non–Gulf War veterans were similar in race (most were white), marital status (most were married), and branch of service (most were in the army; Table 1).
Demographic and military characteristics of US Gulf War veterans deployed between August 1, 1990, and March 1, 1991, and nondeployed veterans who served in the military during the same time period but did not deploy to the Persian Gulfa
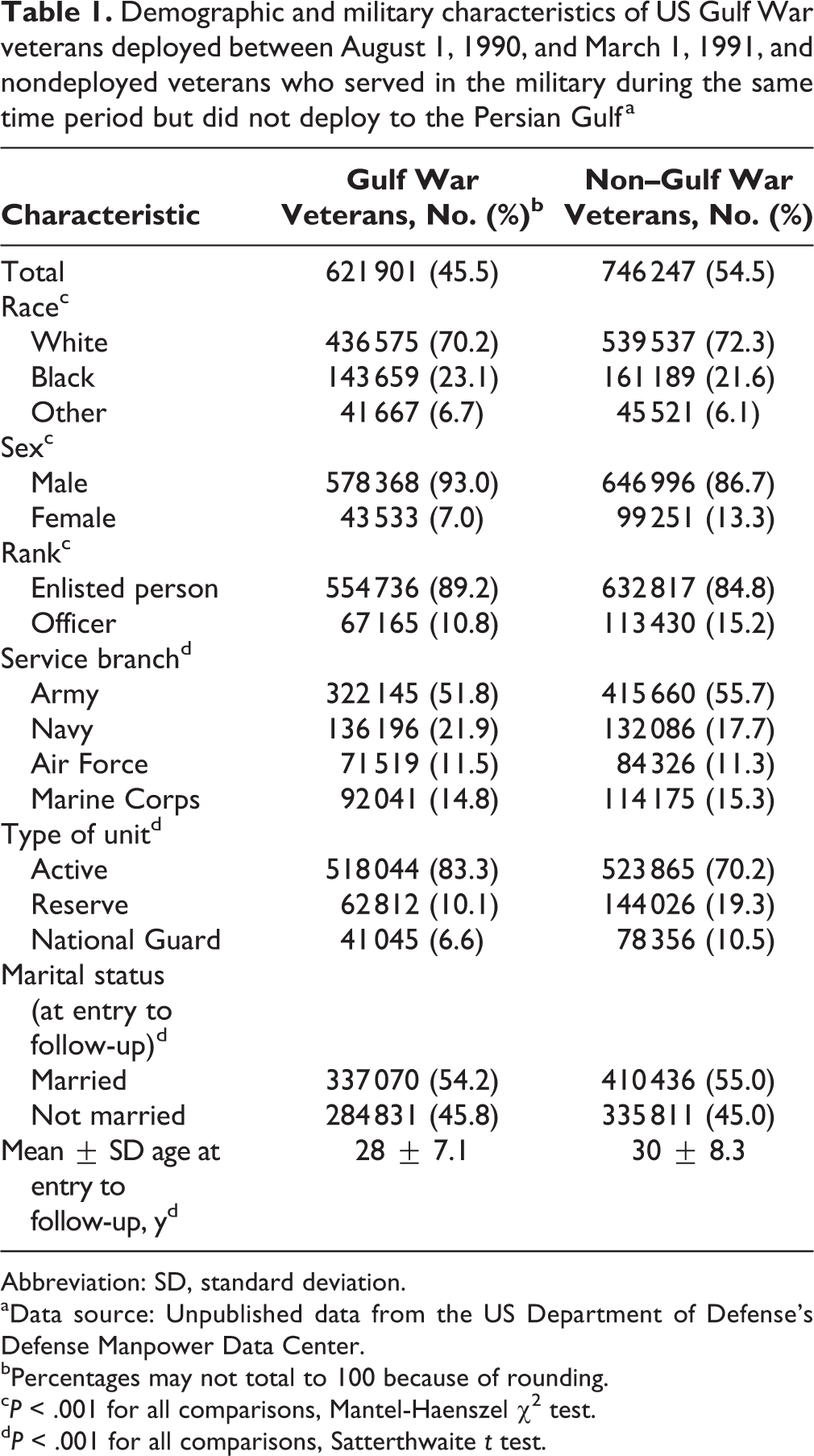
Abbreviation: SD, standard deviation.
aData source: Unpublished data from the US Department of Defense’s Defense Manpower Data Center.
bPercentages may not total to 100 because of rounding.
c P < .001 for all comparisons, Mantel-Haenszel χ2 test.
d P < .001 for all comparisons, Satterthwaite t test.
From the beginning of follow-up through December 31, 2004, 10 869 of 621 901 (1.7%) Gulf War veterans died (rate = 12.8 per 10 000 person-years), and 14 716 of 746 247 (2.0%) non–Gulf War veterans died (rate = 14.6 per 10 000 person-years; Table 2). Data on cause of death were missing for 770 of 10 869 (7.1%) deceased Gulf War veterans and for 1090 of 14 716 (7.4%) deceased non–Gulf War veterans. Gulf War veterans had a cumulative total of 8 466 469 person-years at risk, with an average length of follow-up of 13.6 years. Non–Gulf War veterans had a cumulative total of 10 018 690 person-years at risk, with an average length of follow-up of 13.6 years.
Mortality rates and adjusted rate ratios of US Gulf War veterans deployed between August 1, 1990, and March 1, 1991, and nondeployed veterans who served in the military during the same period but did not deploy, by cause of death, 1991-2004a
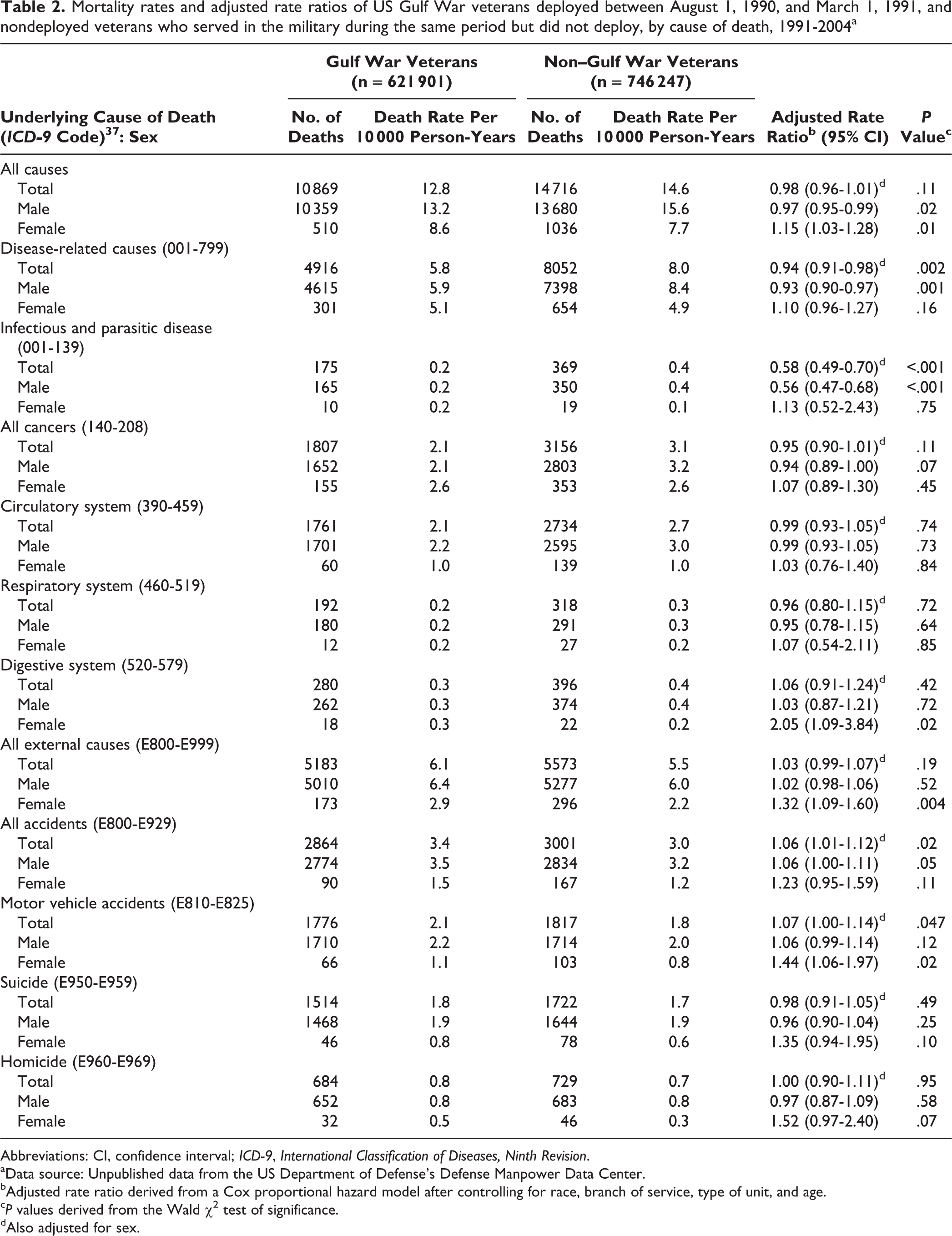
Abbreviations: CI, confidence interval; ICD-9, International Classification of Diseases, Ninth Revision.
aData source: Unpublished data from the US Department of Defense’s Defense Manpower Data Center.
bAdjusted rate ratio derived from a Cox proportional hazard model after controlling for race, branch of service, type of unit, and age.
c P values derived from the Wald χ2 test of significance.
dAlso adjusted for sex.
Compared with male non–Gulf War veterans, male Gulf War veterans had a lower risk of all-cause mortality (aRR = 0.97; 95% CI, 0.95-0.99), disease-related causes (aRR = 0.93; 95% CI, 0.90-0.97), and death from infectious and parasitic disease (aRR = 0.56; 95% CI, 0.47-0.68) but a slightly higher risk of death from all accidents (aRR = 1.06; 95% CI, 1.01-1.12; Table 2).
Compared with female non–Gulf War veterans, female Gulf War veterans had a higher risk of all-cause mortality (aRR = 1.15; 95% CI, 1.03-1.28), a higher risk of death from diseases of the digestive system (aRR = 2.05; 95% CI, 1.09-3.84), and a higher risk of death from external causes (aRR = 1.32; 95% CI, 1.09-1.60); 83% of these externally caused deaths were from motor vehicle accidents (aRR = 1.44; 95% CI, 1.06-1.97), suicide (aRR = 1.35; 95% CI, 0.94-1.95), or homicide (aRR = 1.52; 95% CI, 0.97-2.40). Overall, we found no significant differences between Gulf War veterans and non–Gulf War veterans for deaths from cancer or diseases of the circulatory or respiratory systems (Table 2).
Compared with nonexposed army Gulf War veterans, army Gulf War veterans potentially exposed to nerve agents at Khamisiyah for ≥2 days had a higher risk of mortality from cirrhosis of the liver when controlling for oil well fire smoke exposure (aRR = 3.73; 95% CI, 1.64-8.48). Mortality caused by chronic obstructive pulmonary disease among exposed and nonexposed army Gulf War veterans was similar. Likewise, mortality outcomes of army Gulf War veterans who were exposed to oil well fire smoke (controlling for Khamisiyah exposure) were not significantly different from those of nonexposed army Gulf War veterans (Table 3).
Mortality risks and adjusted rate ratios for deaths among US Army Gulf War veterans who were and were not potentially exposed to nerve gas at Khamisiyah, Iraq, in 1991, by length of exposure, 1991-2004a
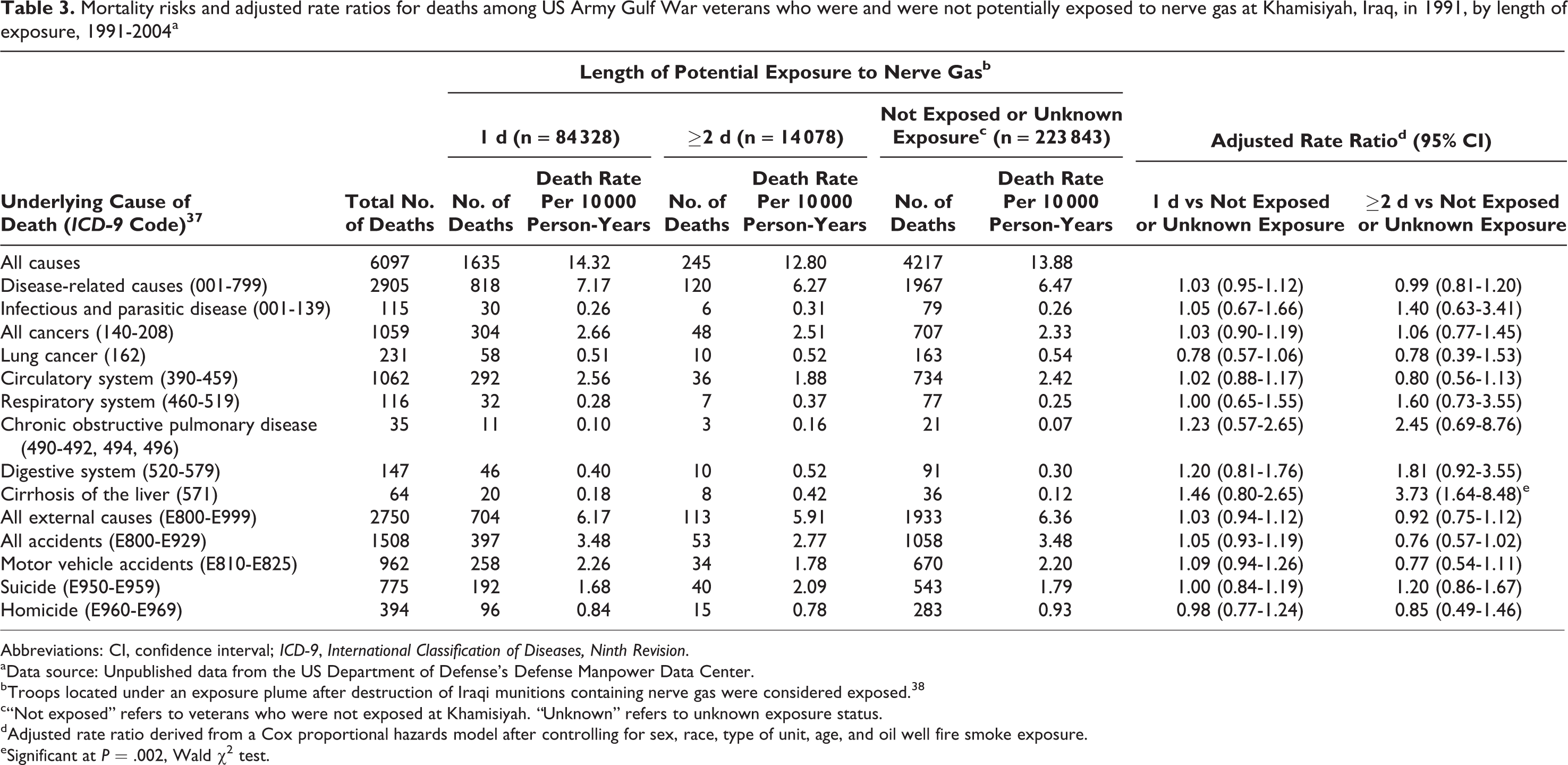
Abbreviations: CI, confidence interval; ICD-9, International Classification of Diseases, Ninth Revision.
aData source: Unpublished data from the US Department of Defense’s Defense Manpower Data Center.
bTroops located under an exposure plume after destruction of Iraqi munitions containing nerve gas were considered exposed. 38
c“Not exposed” refers to veterans who were not exposed at Khamisiyah. “Unknown” refers to unknown exposure status.
dAdjusted rate ratio derived from a Cox proportional hazards model after controlling for sex, race, type of unit, age, and oil well fire smoke exposure.
eSignificant at P = .002, Wald χ2 test.
Compared with the US population, both Gulf War and non–Gulf War veterans had significantly lower-than-expected all-cause and disease-related mortality rates. Female Gulf War veterans had a significantly higher risk of suicide (SMR = 1.60; 95% CI, 1.17-2.13) than females in the US population overall. Female non–Gulf War veterans also had a greater, although not significant, risk of suicide than females in the US population (SMR = 1.14; 95% CI, 0.90-1.43; Table 4).
Standard mortality ratios of US Gulf War veterans deployed between August 1, 1990, and March 1, 1991, and nondeployed veterans who served in the military during the same period compared with the US population, by cause of death, 1991-2004a
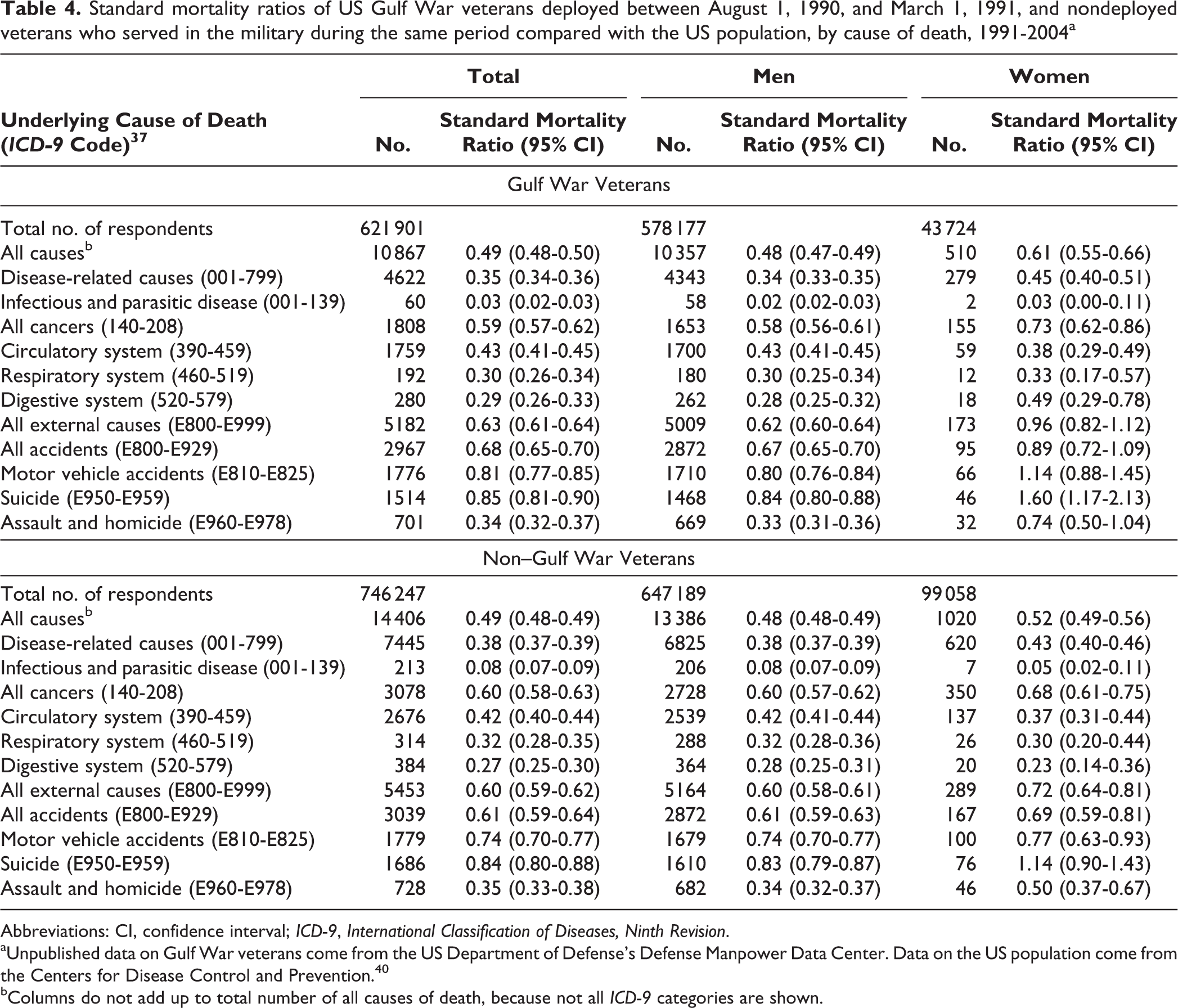
Abbreviations: CI, confidence interval; ICD-9, International Classification of Diseases, Ninth Revision.
aUnpublished data on Gulf War veterans come from the US Department of Defense’s Defense Manpower Data Center. Data on the US population come from the Centers for Disease Control and Prevention. 40
bColumns do not add up to total number of all causes of death, because not all ICD-9 categories are shown.
Discussion
The temporal trends in this cohort have been generally stable since the 7-year follow-up. 14 All Gulf War veterans continued to have a higher mortality risk for external causes and accidents than non–Gulf War veterans. Male Gulf War veterans continued to have a higher risk of mortality from all accidents as compared with male non–Gulf War veterans, although the risk decreased with increasing length of follow-up. The higher risk of mortality from motor vehicle accidents among male Gulf War veterans was no longer significant, but the risk of mortality from motor vehicle accidents among female Gulf War veterans compared with female non–Gulf War veterans was still significant. Postdeployment mortality of Gulf War veterans in the United States was also consistent with postdeployment mortality of Gulf War veterans in the United Kingdom for the first 13 years after the war. 42
Study results for female Gulf War veterans differed from those of their male Gulf War counterparts. Female Gulf War veterans had a higher risk of death from all causes when compared with female non–Gulf War veterans. This greater risk of all-cause mortality among female Gulf War veterans was mainly a result of their higher risk of mortality from external causes, of which motor vehicle accidents, suicide, and homicide constituted 83% of the total.
Female Gulf War veterans had a 32% higher risk of mortality from external causes than female non–Gulf War veterans. Although the risk decreased since the 7-year follow-up period, female Gulf War veterans continued to have a significantly higher risk of motor vehicle accident mortality than female non–Gulf War veterans at the 2004 follow-up period. Compared with females in the US population, female Gulf War veterans had a higher risk of death by suicide.
Using mortality rate as an indicator for overall health, both groups of veterans in this cohort were healthier than the US population. This finding is consistent with other studies that found a healthy soldier effect. 16,43 –46 Younger veterans are generally healthier than their age-matched civilian counterparts because of requirements for initial health screenings upon entry into the military, physical fitness during active duty, and access to medical care.
Because of increased interest in the health effects of exposures among veterans, we analyzed some additional causes of death among exposed army veterans. Veterans who were potentially exposed to nerve agents at Khamisiyah for ≥2 days had a significantly higher risk of death from cirrhosis of the liver. Other research on veterans exposed at Khamisiyah did not explain this finding. The most common causes of cirrhosis are infection with hepatitis B or hepatitis C and alcohol abuse; less common causes are bile duct disorders, hereditary diseases, medications, nonalcoholic fatty liver disease, and nonalcoholic steatohepatitis. 47 Of the few studies that compared the overall health and diseases of Khamisiyah-exposed and nonexposed Gulf War veterans, none found any difference between the 2 groups. 29,31 What was missing from the research on Gulf War veterans exposed at Khamisiyah were a description and comparison of health behaviors, such as alcohol abuse and drug use, which are common causes of cirrhosis. Further research into an explanation for this finding is warranted.
Chronic obstructive pulmonary disease is a leading cause of morbidity in the US population. 48 Although smoking is a major risk factor for chronic obstructive pulmonary disease, research shows a relationship between chronic obstructive pulmonary disease and exposure to noxious particles. 49 We hypothesized that Gulf War veterans who were exposed to environmental stressors would have a higher risk of death from chronic obstructive pulmonary disease than those without exposures; however, our results did not support this hypothesis. A limitation is that we were unable to control for smoking status in our analyses.
Strengths and Limitations
This study had several strengths. The sample of approximately 1.3 million veterans included all veterans deployed to the Gulf War, as well as about half of those who were in the military at the time of the Gulf War but were not deployed, which resulted in reduced sampling error. 50 Additionally, the large sample size allowed for substantial statistical power to detect small increased risks of mortality. 17
This study also had several limitations. One is the possibility that nondeployed Gulf War veterans may have been less healthy than deployed Gulf War veterans at the time of deployment. However, this possibility was addressed in a previous follow-up study, which indicated that a potential selection bias would be transient and limited. 14 Data on race, a variable used as a covariate in the model, were also limited in this historical Gulf War cohort. More extensive data on race/ethnicity might have altered the aRRs for some mortality outcomes. Finally, data on other health-related risk factors (eg, smoking) that may have contributed to certain causes of death were not available for this study cohort; therefore, we did not control for them in analyses.
Conclusion
In general, mortality patterns remained unchanged among all Gulf War veterans compared with non–Gulf War veterans. However, male Gulf War veterans no longer had a greater risk of motor vehicle accident mortality than male non–Gulf War veterans at the 13-year follow-up. Additionally, the mortality rate ratio for motor vehicle accident deaths among female Gulf War veterans compared with female non–Gulf War veterans also decreased at the 13-year follow-up as compared with the 7-year follow-up, although the ratio was still significant. Female Gulf War veterans had a significantly higher overall mortality risk than female non–Gulf War veterans, and this increased risk was mainly from external causes. Compared with the US population, female Gulf War veterans had a significantly higher risk of suicide.
We recommend that the vital status and mortality causes of cohorts of Gulf War and non–Gulf War veterans be periodically updated over time, including comparisons between these 2 groups and with the US population, to help understand any long-term effects of deployment and military service in general.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was based on work supported by merit review funding (GWRA-019-04 S) awarded by the US Department of Veterans Affairs, Office of Research and Development.