
Abstract
Having attenuated visualization has been proposed to confer vulnerability to hoarding, although some studies have found no differences in visualizing between individuals who hoard and controls. To clarify this, we investigated the presence and severity of hoarding symptoms and beliefs in a specialist sample of aphantasics (those without imagery) and hyperphantasics (those with extremely vivid imagery), compared to mid-range/typical visualizers, while controlling for confounds (i.e., age and depression levels). Bayesian analysis revealed stronger evidence favouring a lack of difference in hoarding symptoms between aphantasics (n = 58) and case-matched typical visualizers, although we found moderately strong evidence to suggest aphantasics were more inclined to report using objects as memory aids; a hoarding specific coping strategy. We also found moderately strong evidence to suggest hyperphantasics (n = 23) had lower hoarding symptoms compared to case-matched typical visualizers and were less likely to live in cluttered homes, whereas evidence was weaker/inconclusive regarding differences in hoarding beliefs. Overall, findings suggest attenuated visualization does not necessarily predispose hoarding, but enhanced visualizing capacities may protect against hoarding symptom development.
Introduction
Hoarding disorder (HD) is a complex and difficult to treat neuropsychiatric syndrome, characterised by urges to excessively acquire and save items, resulting in the accumulation of clutter that compromises living areas in the home and limits their intended use (American Psychiatric Association, 2022). The condition tends to onset in adolescence and worsens with age (Dozier et al., 2016; Grisham et al., 2006), affecting approximately 2.5% of the working population (Postlethwaite et al., 2019). Although highly comorbid with other psychopathology, such as depression (Vieira et al., 2022), hoarding negatively impacts an individual’s functioning independent of comorbid psychopathology, and is associated with low quality of life and high levels of impairment (Nutley et al., 2022). This includes elevated risk of death from fires and hazards within the home, financial problems, threats of eviction, and high rates of conflict with neighbours and cohabiting family members (Ong et al., 2015; Tolin et al., 2008). At the societal level, hygiene and safety concerns associated with severe hoarding cases pose public health risks, often necessitating expensive clean ups by city councils (Neave et al., 2017).
Given the profound impact of hoarding on the afflicted individual, their families, and society at large, great interest lies in the identification of individual difference factors that may confer vulnerability to hoarding problems (Raines et al., 2016). The most popular account of these can be found in Frost and Hartl’s (1996) cognitive-behavioural model of hoarding, expanded by Steketee & Frost (2003, 2006). In this model, hoarding is thought to arise from a combination of distal diatheses, such as genetic predispositions, information processing deficits (e.g., memory issues, attentional problems, dysexecutive symptoms), early aversive experiences (i.e., trauma and emotional deprivation) and personality traits (i.e., perfectionism, indecisiveness). These distal factors are theorised to lead to the development of certain beliefs and coping strategies, such as using objects as memory aids or relying on possessions as sources of comfort and security (Steketee et al., 2003), resulting in maladaptive reinforcements cycles that maintain hoarding problems more proximally (i.e., positive emotion when acquiring/saving and distress when discarding).
While most components of the cognitive-behavioural hoarding model have a strong evidence base (Grisham & Barlow, 2005), it has been criticised for neglecting some prominent clinical features of the disorder (e.g., attachment difficulties), leading to revised and updated conceptualisations (e.g., see Mathes et al., 2020). Moreover, cognitive behavioural therapy (CBT) for hoarding, which is based on this model, only results in clinically significant symptom reduction in approximately a third of cases (David et al., 2022), and many individuals refuse therapy or discontinue prematurely (Steketee et al., 2010). Tolin and colleagues (2015) thus describe CBT for hoarding as a “work in progress” and suggest that treatment could be improved by targeting vulnerability factors that may exacerbate hoarding difficulties. This clarion call has led to the development of a number of alternative and adjunctive treatments for hoarding targeting these potential factors (e.g., emotion regulation difficulties; Grisham et al., 2022).
Emerging research suggests disruptions in mental imagery may be one important but understudied clinical feature of hoarding problems and a possible future intervention target (e.g., Stewart et al., 2020; Sabel et al., 2025). Mental images are sensory-perceptual experiences that occur without direct afferent input (i.e., “Seeing with the mind’s eye”; Kosslyn et al., 2001, p. 635); including constructs such as dreams, memories and imagery-based simulations of future events. Mental images can be both voluntarily evoked (e.g., when fantasizing or daydreaming) and involuntarily triggered (e.g., experienced as a brief flash), and may exist across sensory modalities (i.e., auditory experiences, haptic sensations), although visual images are the most discussed in the literature and tend to be the most vivid (Pearson & Westbrook, 2015; Schifferstein, 2009).
The ability to visualize (i.e., deliberately generate, maintain and transform visual images) is a trait-like tendency (Pounder et al., 2021), that has been found to vary on a spectrum in the population from people whose voluntary visual imagery is entirely absent to those whose visual imagery vividness rivals perceptual experience (Pearson, 2019; Zeman, 2024). These visual imagery vividness extremes have been coined aphantasia and hyperphantasia respectively (Zeman et al., 2015, 2020), are rare in the population (4-5% for aphantasia and 3% for hyperphantasia; Dance et al., 2022; Zeman, 2024), and have a number of psychological and behavioural correlates. For example, individuals with aphantasia are more likely to attract diagnoses of autism spectrum disorder (Milton et al., 2021), and have difficulties with facial recognition (Takahashi et al., 2023), whereas hyperphantasic individuals are more likely to work in traditionally ‘creative’ industries (Zeman et al., 2020), have increased rates of synaesthesia (Barnett & Newell, 2008), and may be more prone to psychopathology that has imagery as a clinical feature (i.e. post-traumatic stress disorder; Cavedon-Taylor, 2022; Keogh et al., 2023).
Although individual differences in visualization ability, such as aphantasia and hyperphantasia, are usually assessed through self-report measures (i.e., via the Vividness of Visual Imagery Questionnaire; VVIQ; Marks, 1973), these introspective methods have been validated against objective indices of imagery vividness and strength, including binocular rivalry paradigms (Keogh & Pearson, 2018, 2024), skin conductance measures (Wicken et al., 2021), and the pupillary light index (Kay et al., 2022). Individual differences in the ability to visualize appear to be closely related to the size of the visual cortex (Bergmann et al., 2016), its resting state activity (Keogh et al., 2020), and its functional capacity and wiring (Chang et al., 2025), but may also depend upon prefrontal, temporal and parietal brain regions, as well as parts of the default mode network (Fulford et al., 2018). Importantly, visualization abilities are thought to be largely congenitally determined (i.e., present from birth; Pounder et al., 2021), although can also be impacted by events throughout the lifespan (e.g., acquired via traumatic brain injury or stroke; Knowles et al., 2021).
Similar to other forms of psychopathology (e.g., Brewin et al., 2010), individuals who hoard appear to experience intrusive images in daily life that cause distress and disruptions in functioning (Oaie et al., 2024; Sabel et al., 2025; Stewart et al., 2020), including images that may interfere with discarding (Stewart et al., 2020). However, recent work by Sabel and colleagues (2025) suggests that in addition to a heightened susceptibility to negative involuntary imagery, individuals who hoard may also have challenges with intentional visualization. In their investigation, they found that hoarding symptoms were associated with a lower ability to deliberately generate vivid visual images, whereas no significant associations emerged between hoarding and the capacity to generate imagery in other sensory modalities (i.e., audition, touch, smell etc). Although the association was small in size, it occurred across two measures of visualizing (i.e., the VVIQ (Marks, 1973) and the Plymouth Sensory Imagery Questionnaire – Visualizing subscale (PSIQ - Visual; Andrade et al., 2014)). Moreover, visualizing ability negatively predicted hoarding symptoms even when holding constant other psychological symptoms associated with mental imagery abnormalities (i.e., post-traumatic stress, obsessive compulsive disorder symptoms and depression). Furthermore, the authors found that the tendency to use objects as memory aids partially mediated the association between reduced visualizing abilities and increased hoarding symptoms, suggesting that difficulties bringing visual images to mind may make individuals more prone to accumulating objects as cues to facilitate the retrieval of memories. The authors suggest that individuals who hoard may be more prone to aphantasia, with visualizing difficulties potentially forming part of the information processing diatheses conferring vulnerability to hoarding problems (Frost & Hartl, 1996). They also propose that visualization difficulties may represent a possible future intervention target to improve treatment outcomes in hoarding, for example, via imagery training interventions (Rhodes et al., 2024).
However, before this can be firmly established, more research is needed to replicate these preliminary associations and resolve several limitations with the method and design of Sabel et al. (2025). Firstly, two studies prior to Sabel and colleagues (2025) found no significant differences between individuals with elevated hoarding tendencies and controls in visual imagery use tendency or the ability to conjure visual imagery with vividness and strength (Stewart et al., 2020; Yap & Grisham, 2020), so more research is needed to reconcile these differences across the literature. Secondly, Sabel and colleagues examined the association between hoarding and imagery in an undergraduate convenience sample, so it is unclear whether results will generalize to clinical HD samples or participants who have formally been identified as aphantasic and hyperphantasic. Thirdly, although Sabel and colleagues (2025) included several control measures, such as depressive symptoms, they failed to control for other confounds, such as age – which has been associated with both attenuated imagery vividness (Gulyás et al., 2022) and worsened hoarding symptoms (Dozier et al., 2016). Finally, the authors only examined the association between visualizing abilities and global indices of hoarding symptom severity, so it is unclear what facet of hoarding symptoms visualizing difficulties may underscore the most (i.e., difficulty discarding, excessive acquiring or clutter), or whether visualizing difficulties may also give rise to other associated hoarding beliefs and coping strategies.
In the present study, we therefore aimed to partially address these limitations by exploring the presence and severity of hoarding tendencies, and associated beliefs and coping strategies, within a specialist sample of aphantasic and hyperphantasic individuals recruited from an existing participant pool of individuals with extreme visualizing abilities, compiled by imagery experts (See https://www.futuremindslab.com/). To permit normative comparisons while accounting for extraneous variables, we compared these groups to a community sample of typical/mid-range visualizers and controlled for age and depression levels. Given that the ability to conjure visual imagery appears to be largely congenitally determined (i.e., present from birth; Pounder et al., 2022), and because Sabel et al. (2025) reasoned that visualizing difficulties may be part of the information processing deficits conferring vulnerability to hoarding problems, we hypothesised that aphantasic individuals would therefore endorse more severe hoarding symptoms and beliefs compared to ‘typical/mid-range’ visualizers, whereas hyperphantasic individuals would endorse fewer hoarding symptoms and beliefs than typical/mid-range visualizers.
Method
Participants
One hundred and forty-three self-identified aphantasic and hyperphantasic individuals from a specialist pool of participants with extreme imagery abilities were recruited into the study through the Future Minds lab (https://www.futuremindslab.com/). This database consists of participants who contacted the Lab with self-suspected aphantasia or hyperphantasia and expressed a willingness to participate in research and treatment opportunities. Participants from this sample who had missing data (n = 17), failed more than one of three attention and validity checks recommended by Agley et al. (2022) embedded throughout the survey (n = 2), or exhibited patterns of responding that were extreme and non-sensical (i.e., providing an impossible age, n = 1) were subsequently excluded from analysis. We also excluded participants from this sample who returned VVIQ scores that fell outside the cut-off values for aphantasia (VVIQ scores >23, n = 10) and hyperphantasia (VVIQ scores <75, n = 8), recommended by Milton et al. (2021) and Zeman et al. (2020). This left a remaining sample of 105 participants (aphantasics: n = 97, hyperphantasics: n = 9).
We then recruited a community control sample of 357 participants with typical/mid-range visualizing ability abilities from the r/SampleSize forum on Reddit. Reddit is a social media and news aggregation website where users can browse and post content anonymously on different forums or ‘subreddits’. One subreddit, known as r/SampleSize is a dedicated community of over 165’000 registered members worldwide who are interested in participating in research opportunities voluntarily. Several studies have provided insight into the characteristics of the r/SampleSize participant pool, including greater demographic diversity in terms of age, education level and gender representation compared to traditionally used samples, as well as increased internal motivation to participate in research opportunities and a greater need for cognition (Jamnik & Lane, 2017; Luong & Lomanowska, 2022). Several well-known psychological phenomena have been successfully replicated using r/SampleSize participants, including findings on psychological well-being and the fundamental attribution error (Jamnik & Lane, 2017; Luong & Butler, 2023).
Participants from this sample who had missing data (n = 108), failed more than one of three attention and validity checks recommended by Agley et al. (2022) embedded throughout the survey (n = 6) or exhibited patterns of extreme and non-sensical responding (n = 1) were subsequently excluded from analysis. Participants with valid data from this sample who also provided VVIQ scores indicating an aphantasic (VVIQ < 23, n = 14) or hyperphantasic profile (VVIQ > 75, n = 14) were also removed from the control group and placed into the aphantasic and hyperphantasic groups, respectively. This left a remaining sample of 214 community control participants with ‘typical/mid-range’ visualizing abilities, 111 aphantasics, and 23 hyperphantasic participants for comparative analysis.
Materials
Procedure
All procedures were reviewed and approved by the University of New South Wales human research ethics committee (HREAP-C file no. 3784), which applies research ethics principles in accordance with the World Medical Association Declaration of Helsinki. Following ethics approval, interested participants signed up for the study by responding to a recruitment advertisement that was either emailed from the distribution list of participants with mental imagery vividness extremes or posted multiple times on the r/SampleSize subreddit between January and June 2024. The research was advertised as a study investigating the association between acquiring and saving behaviours and experiences with imagery, and interested participants were guided to click on a hyperlink embedded within this advertisement to access the survey hosted on the Qualtrics platform (https://www.qualtrics.com/). Participants initially provided written informed consent and then completed the demographics items and other study measures. To minimize the impact of order effects and fatigue, the presentation of the questionnaires was randomised across participants. Following completion, participants were shown the debriefing statement and given the first author’s contact details for follow up questions. No renumeration was provided, and the study took approximately 30 minutes to complete.
Results
Descriptive Statistics
Means, Standard Deviations and Demographic Characteristics for the Three Study Groups
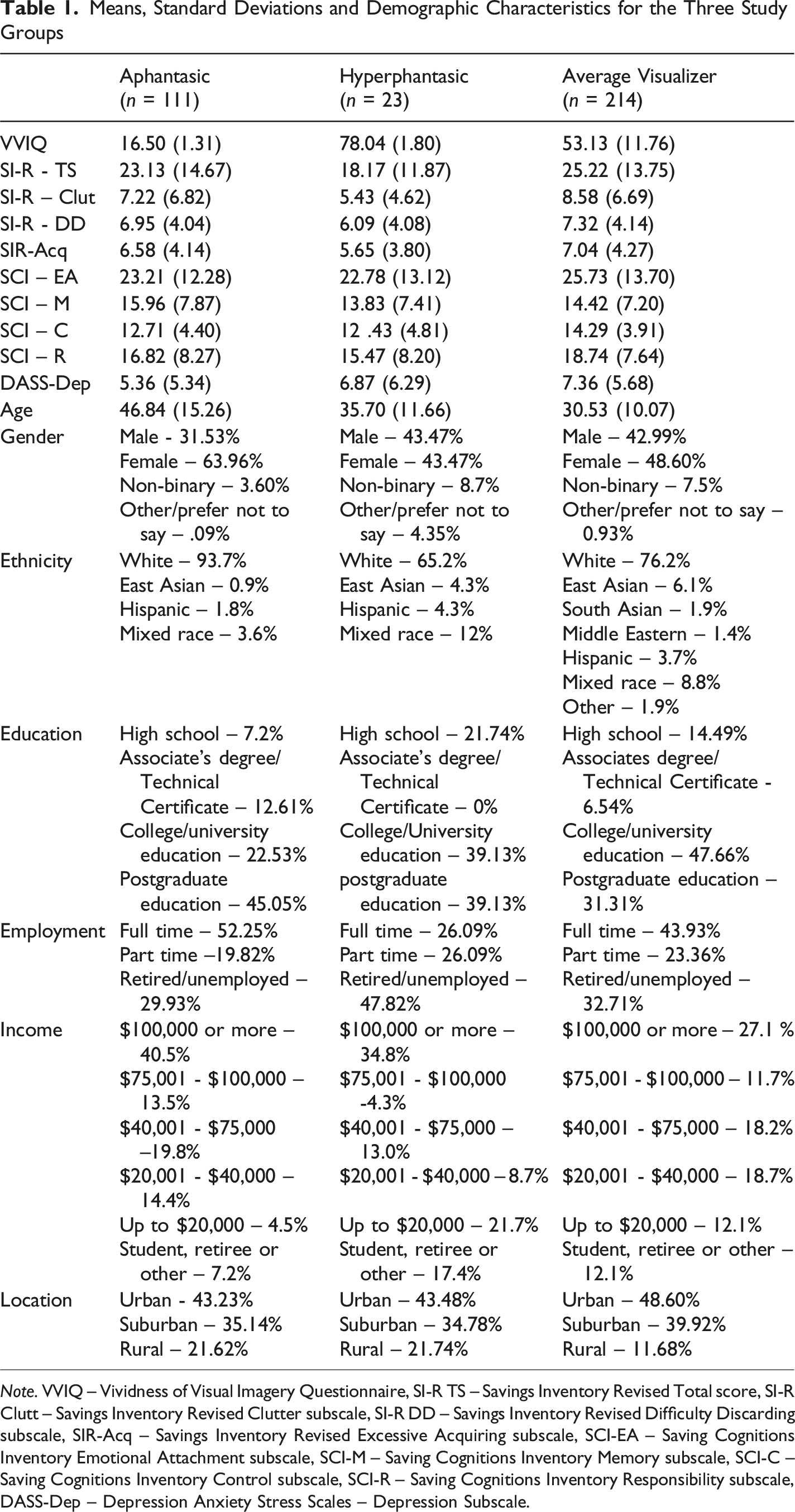
Note. VVIQ – Vividness of Visual Imagery Questionnaire, SI-R TS – Savings Inventory Revised Total score, SI-R Clutt – Savings Inventory Revised Clutter subscale, SI-R DD – Savings Inventory Revised Difficulty Discarding subscale, SIR-Acq – Savings Inventory Revised Excessive Acquiring subscale, SCI-EA – Saving Cognitions Inventory Emotional Attachment subscale, SCI-M – Saving Cognitions Inventory Memory subscale, SCI-C – Saving Cognitions Inventory Control subscale, SCI-R – Saving Cognitions Inventory Responsibility subscale, DASS-Dep – Depression Anxiety Stress Scales – Depression Subscale.
The mean scores of the aphantasic, hyperphantasic and average visualizer samples on the SI-R were also notable compared to population norms. While the average visualizer and aphantasic samples had mean scores on the SI-R of 25.22 (SD 13.75) and 23.13 (SD 14.67), respectively, that resembled norms for non-hoarding clinical (x̅ = 24; Frost et al., 2004) and community control participants (x̅ = 23; Frost et al., 2004), our hyperphantasic sample had somewhat lower SI-R mean scores of 18.17 (SD 11.87).
Case Control Matching
Aphantasics
Initially, there were significant differences between the aphantasic and average visualizer groups in age, Welch’s t (df = 161.00) = −10.17, p < .001, and depression scores, Welch’s t (df = 235.17) = 3.12, p = .001. As increasing age and depression levels are known to attenuate imagery vividness (Gulyás et al., 2022; Holmes et al., 2016) and worsen hoarding symptoms (Dozier et al., 2016; Frost et al., 2015), age and depression matched groups were created using the python FUZZY case-control matching extension for SPSS v.29. Using this procedure, we randomly drew cases from the aphantasic and average visualizer groups that were matched in age and depressive symptoms. Matched tolerance was set at 1 for both variables, and participants were sampled without replacement.
This procedure resulted in 58 matches. As expected, the matched aphantasic group (n = 58) had significantly lower VVIQ scores (M = 16.50, SD = 1.34) than the matched typical visualizer group (n = 58, M = 53.70, SD = 10.77), Welch’s t (df = 58.76) = 26.10, p < .001. Importantly however, there was no significant difference in age between the matched aphantasic group (M = 37.10, SD = 11.38) and the matched typical visualizer group (M = 37.00, SD = 11.39), t (df = 114) = −.05, p = .48, and no significant difference in depression scores (aphantasic M = 5.62, SD = 5.14; typical visualizer M = 5.48, SD = 4.95), t (df = 114) = −.15, p = .44. After case control matching, there were also no significant differences between groups in the distributions of any of the other demographic variables, such as gender, χ2 (df = 3) = 7.16, p = .07, ethnicity, χ2 (df = 7) = 7.49, p = .38, education level, χ2 (df = 7) = 9.91, p = .19, income, χ2 (df = 5) = 4.85, p = .43, employment status χ2 (df = 12) = 18.40, p = .10, or location χ2 (df = 2) = 1.62, p = .45.
Hyperphantasics
Initially, we also found significant differences in age between the hyperphantasic and typical visualizer groups, Welch’s t (df = 25.65) = −2.05, p = .01, but no significant differences in depression scores, Welch’s t (df = 26.01) = .36, p = .36. Using the same python FUZZY case-control matching procedure, we therefore created aged-matched groups by randomly drawing cases from the hyperphantasic and typical visualizer groups. Matched tolerance was set at 1 and participants were sampled without replacement.
This procedure resulted in matches for the entire hyperphantasic sample. As expected, the matched hyperphantasic group (n = 23) had significantly higher VVIQ scores (M = 78.04, SD = 1.79) than the matched typical visualizer group (n = 23, M = 53.74, SD = 11.50), Welch’s t (df = 23.07) = −10.01, p < .001. Importantly however, there was no significant difference in age between the matched hyperphantasic group (M = 35.74, SD = 11.73) and the matched typical visualizer group (M = 35.70, SD = 11.66), t (df = 44) = .01, p = .50. After case control matching, there were also no significant differences between groups in depression scores, t (df = 44) = −.21, p = .42, or the distributions of any of the other demographic variables, such as gender, χ2 (df = 4) = 3.92, p = .42, ethnicity, χ2 (df = 5) = 8.32, p = .14, employment status, χ2 (df = 9) = 4.47, p = .88, income, χ2 (df = 5) = 5.29, p = .38, education levels, χ2 (df = 7) = 7.34, p = .40, or location, χ2 (df = 2) = 0.00, p = 1.00.
Inferential Statistics
We then conducted Bayesian one-sided independent samples t-tests in JASP (JASP team, 2023) to test the directional hypotheses that aphantasics would exhibit more severe hoarding symptoms and beliefs than typical visualizers, and that hyperphantasic individuals would exhibit less severe hoarding symptoms and beliefs than typical visualizers. We chose Bayesian over frequentist methods as our primary analytic method, given that Bayesian inference tends to be more sensitive and robust when sample size is small (Georgiou, 2024; McNeish, 2016) and to compare the strength of evidence for different between-group comparisons under both the alternative and null hypotheses. However, to satisfy conventional reporting norms, as well as further cross-validate our results, we also report supplementary frequentist independent samples t-tests.
As previous research has suggested imagery ability and hoarding tendencies may share a small-to-moderate negative association (d ≈ 0.35–0.45; Sabel et al., 2025), but two previous studies have found no differences in visualizing between individuals with elevated HD tendencies and controls (Stewart et al., 2020; Yap & Grisham, 2020), we set a conservative informed normal prior mean centred at 0, with the standard deviation set at 0.5. To increase confidence in the study findings (i.e., to ensure that our results are not unduly influenced by the prior), we then conducted sensitivity analysis by varying the standard deviation around the informed normal prior (i.e., SD = 0.2, 0.5, 1.0). Across all tests, bayes factors and posterior estimates were stable (i.e., tests that supported the alternative hypothesis under one prior also supported it under all other variations and vice versa), suggesting robustness to variations in prior assumptions. As per convention, Bayes factors were interpreted according to common threshold values, where <1 = “No evidence”, 1–3 = “Weak/inconclusive evidence”, 3–10 = “Moderate evidence”, 10–30 = “Strong evidence”, 30–100 = “Very strong evidence”, and >100 = “Extreme evidence” (Jeffreys, 1961; Kass & Raftery, 1995).
Differences Between Aphantasic and Average Visualizer Groups
Mean and Standard Deviation Scores Between the Matched Aphantasia and Typical Visualizer Groups and the Matched Hyerphantasia and Typical Visualizer Groups
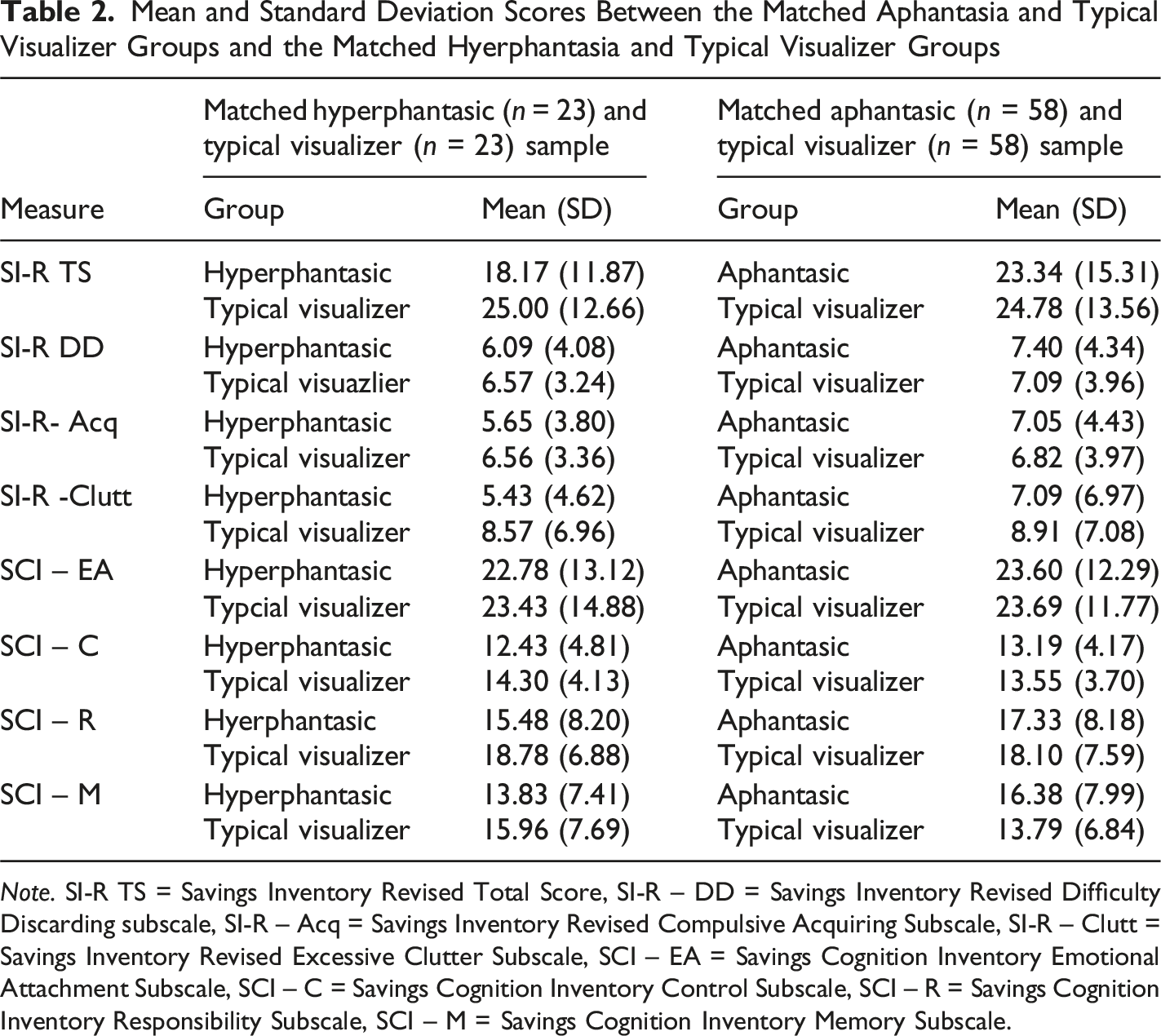
Note. SI-R TS = Savings Inventory Revised Total Score, SI-R – DD = Savings Inventory Revised Difficulty Discarding subscale, SI-R – Acq = Savings Inventory Revised Compulsive Acquiring Subscale, SI-R – Clutt = Savings Inventory Revised Excessive Clutter Subscale, SCI – EA = Savings Cognition Inventory Emotional Attachment Subscale, SCI – C = Savings Cognition Inventory Control Subscale, SCI – R = Savings Cognition Inventory Responsibility Subscale, SCI – M = Savings Cognition Inventory Memory Subscale.
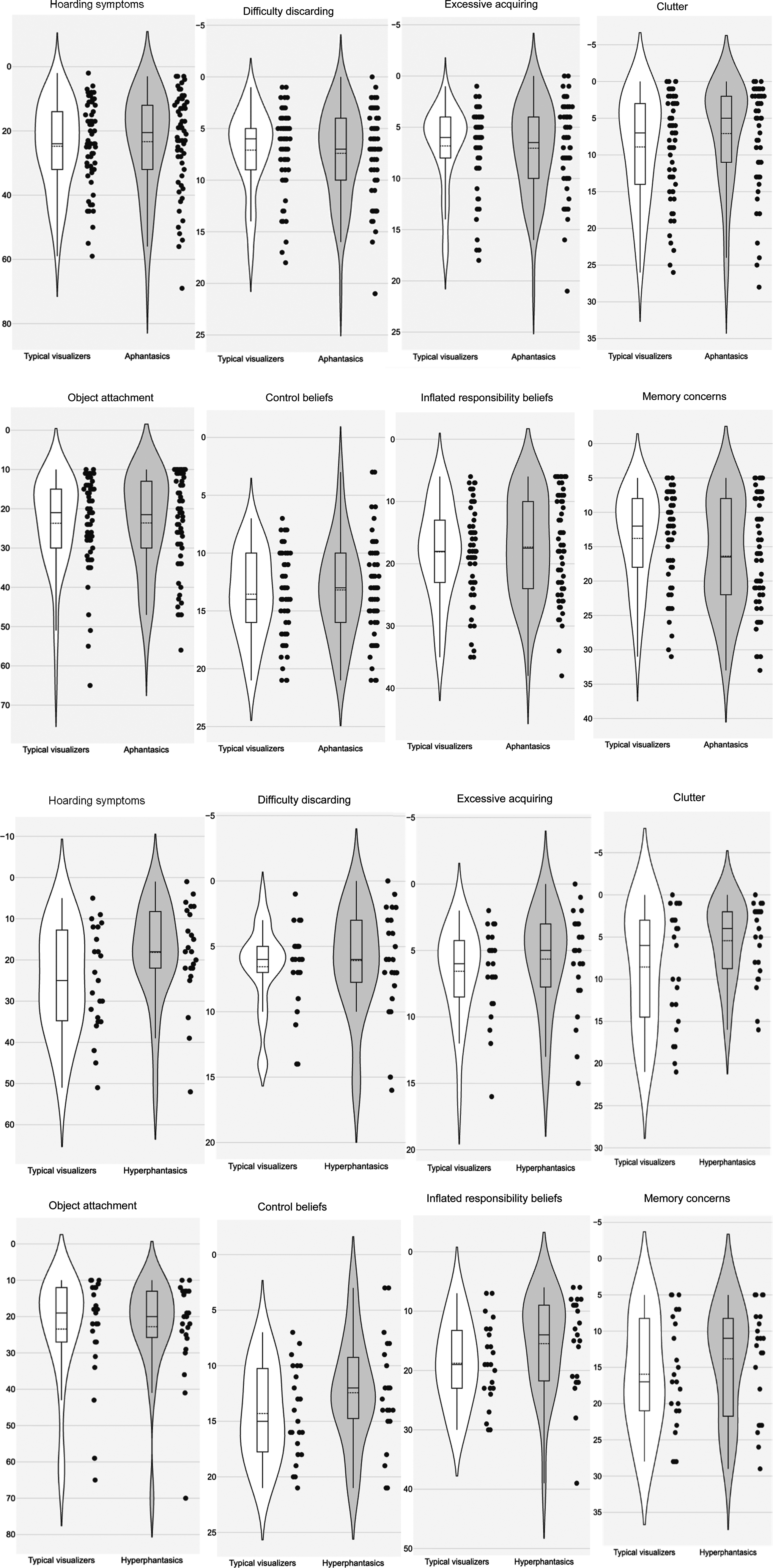
Violin plots of hoarding symptoms and associated belief domains.
Contrary to predictions, there was also moderately strong evidence from our Bayesian tests to suggest aphantasics and case matched typical visualizers did not differ in their control beliefs towards objects (BF01 = 4.01, δ = 0.09, 95% CI [0.004, 0.338]), and inflated sense of responsibility towards items (BF10 = 4.10, δ = 0.09, 95% CI [0.004, 0.335]), whereas evidence was weaker/inconclusive, yet still favouring a lack of difference between groups for object attachment (BF01 = 2.96, δ = 0.12, 95% CI [0.005, 0.386]). However, consistent with predictions, we found moderately strong evidence to suggest aphantasics had greater object-memory concerns than their case-matched typical visualizing counterparts (BF10 = 3.08, δ = 0.32, 95% CI [0.040, 0.652]). Overall, this pattern suggests that while aphantasics appear no more likely than typical visualizers to demonstrate a sense of attachment to, control over, and inflated sense of responsibility towards their possessions, they appear to be more likely to rely on objects as memory aids. This conclusion was mirrored in the pattern of frequentist tests, suggesting a lack of significant differences between groups for participants’ object attachment t (df = 114) = −0.04, p = .52, d = −.007, control beliefs t (df = 114) = −0.50, p = .69, d = 0.19, and sense of responsibility towards items, t (df = 114) = −0.53, p = .70, d = .019 but a significant group difference for object-memory-concerns, t (df = 114) = 1.87, p = .03, d = .35.
Differences Between Hyperphantasic and Average Visualizer Groups
Table 2 depicts the means and standard deviation scores for the hyperphantasic and case matched typical visualizer groups on hoarding symptom and belief measures, whereas Figure 1 depicts the distribution and density of scores across groups. Consistent with predictions, we found moderately strong evidence to suggest that hyperphantasic individuals had less severe hoarding symptoms (BF10 = 3.47, δ = −0.43, 95% CI [−0.922, −0.047]) and clutter problems (BF10 = 3.07, δ = −0.41, 95% CI [−0.903, −0.042]) than their case matched typical visualizing counterparts, whereas evidence was weaker/inconclusive regarding excessive acquiring (BF10 = 1.04, δ = −0.26, 95% CI [−0.717, −0.016]). There was no evidence for any differences in difficulty discarding, with weak/inconclusive evidence favouring a lack of difference between groups (BF01 = 1.41, δ = −0.21, 95% CI [−0.641, −0.011]). Overall, these results suggest hyperphantasic individuals may be less likely to exhibit hoarding symptoms than typical visualizers, especially clutter problems. This pattern of findings was largely mirrored in the frequentist tests, which suggested hyperphantasics had significantly lower hoarding symptoms, t (df = 44) = -1.89, p = 0.03, d = −.556, and clutter levels, t (df = 44) = −1.80, p = 0.04, d = −.53 than typical visualizers, whereas no significant differences emerged between groups in their symptoms of excessive acquiring, t (df = 44) = −.86, p = .20, d = −.26, and difficulty discarding t (df = 44) = -0.44, p = .33, d = −.13.
There was some weak/inconclusive evidence suggesting that hyperphantasics may endorse lower beliefs about control (BF10 = 1.88, δ = −0.35, 95% CI [−0.824, 0.−0.028]), responsibility (BF10 = 2.04, δ = −0.36, 95% CI [−0.838, −0.030]), and memory (BF10 = 1.14, δ = −0.28, 95% CI [−0.734, −0.017]) than their case matched typical visualizing counterparts, however, there was no evidence for any difference between groups in object attachment, with some weak/inconclusive evidence favouring a lack of difference between groups (BF01 = 1.76, δ = −0.19, 95% CI [−0.594, −0.009). Overall, results provide only limited support for the prediction that hyperphantasics would endorse fewer hoarding-related beliefs than case-matched typical visualizers. Corresponding frequentist frequentists tests revealed no significant differences between groups for object attachment, t (df = 44) = −0.16, p = .44, d = −.05, control beliefs, t (df = 44) = -1.41, p = .08, d = −.42, responsibility towards items t (df = 44) = −1.48, p = .07, d = −.44, and memory concerns t (df = 44) = −0.96, p = .17, d = −.28.
Discussion
This study aimed to determine whether visualizing difficulties confer vulnerability to hoarding problems by investigating the presence and severity of hoarding symptoms in a sample of participants with extreme visualizing abilities, compared to mid-range/typical visualizers. Contrary to predictions, we found moderately strong evidence to suggest aphantasic individuals (i.e., those without imagery) did not differ in their mean level of hoarding symptoms compared to case-matched typical/mid-range visualizers, although aphantasics were more inclined to use objects as visual cues to facilitate recall, a hoarding-specific coping strategy (Hartl et al., 2004; Steketee et al., 2003). Consistent with hypotheses, however, we found moderately strong evidence to suggest that hyperphantasic individuals (i.e., those with extremely vivid imagery) had less severe hoarding symptoms than case matched typical/mid-range visualizers, and were less likely to live in cluttered homes, whereas evidence was inconclusive regarding the reduced endorsement of hoarding-related beliefs in this group. This interesting pattern of results sheds some clarity on the conflicting findings found in the previous literature (Sabel et al., 2025; Stewart et al., 2020; Yap & Grisham, 2019), and may have important implications regarding the relevance of imagery-based conceptualisations and treatments of hoarding problems.
Aphantasics
Contrary to predictions, we found no evidence to suggest any differences between aphantasics and age and depression matched typical/mid-range visualizers in global hoarding symptom severity, or the subscale scores of excessive acquiring, difficulty discarding or clutter. Aphantasics also showed mean levels of hoarding symptoms that approximated population norms. This result is not in keeping with the proposition of Sabel et al. (2025), and suggests that having a visualizing deficit (i.e., being aphantasic) does not necessarily make an individual more prone to hoarding. Although we cannot rule out that hoarding may still be associated with reduced visualization abilities when examined dimensionally in large-scale, correlational studies, our results would suggest that such difficulties may be subtle or not clinically meaningful, especially when considered in light of prior research showing that individuals with elevated hoarding tendencies tend to have, on average, visualization abilities that approximate community controls (Stewart et al., 2020; Yap & Grisham, 2019). On reflection, this result is perhaps unsurprising given that individuals who hoard report elevations in negative intrusive imagery at the group level (e.g., Stewart et al., 2020), implying that most suffers must have at least some capacity to experience imagery.
Nevertheless, consistent with predictions, we found moderately strong evidence to suggest that aphantasic individuals were more inclined than controls to endorse using objects as memory aids; a hoarding specific coping strategy (Hartl et al., 2004; Steketee et al., 2003). This result accords with a broader literature suggesting aphantasics report autobiographical memory deficits (Dawes et al., 2020; Greenberg & Knowlton, 2014; Zeman et al., 2015) and reduced memory confidence (Wittmann & Şatırer, 2022), but only partially aligns with the findings of Sabel and colleagues (2025), who found that the tendency to rely on objects as cues to facilitate autobiographical memory-retrieval mediated the link between reduced visualizing ability and increased hoarding symptoms. Our results suggest that while aphantasic individuals may be more prone to relying on objects as cues to facilitate the retrieval of memories, this tendency does not appear to make them more prone to hoarding symptoms, although longitudinal studies should be conducted to verify this conclusion as we measured this association cross sectionally.
Hyperphantasics
As hypothesised, however, we found moderately strong evidence to suggest hyperphantasic individuals exhibited lower hoarding symptoms compared their typical visualizing counterparts and were less likely to endorse symptoms of excessive clutter. Clutter is the hallmark feature of hoarding (Nix & Dozier, 2023), and one of the main sources of quality of life and functional impairment in the disorder, resulting in conflict with cohabiting family members, illnesses due to unsanitary conditions, and disruption in the ability to perform activities of daily living, such as cooking, sleeping, toileting and leisure activities (Ayers et al., 2012). These findings were therefore very encouraging, and appear to nuance the correlational finding of Sabel et al. (2025). That is, individuals with lower visualizing abilities do not appear necessarily more likely to hoard, rather, it is individuals with stronger visualizing abilities that appear less likely to. Moreover, it contradicts the prevailing notion that individuals who are hyperphantasic might be more prone to psychopathology, because many disorders have imagery as a clinical feature (e.g., post-traumatic stress disorder, maladaptive daydreaming etc; Cavedon-Taylor, 2022; Pearson et al., 2015). Our findings suggest, at least when it comes to hoarding, that hyperphantasia might promote psychological health.
One potential explanation for this finding can be found by considering the influence of volitional mental imagery on wider cognitive and executive processes thought to underscore successful activities in daily living. Mental imagery is considered to be an important cognitive tool that has a profound influence on daily tasks, such as planning, navigating, remembering and decision making (Pearson et al., 2015). For example, the ability to intentionally conjure prospective images of a future event allows that event to be pre-experienced and consequences of different choice alternatives to be “tried out”; underscoring effective planning and decision making (Zaleskiewicz et al., 2023). Similarly, successfully navigating through and locating objects within one’s environment relies on the purposeful retrieval of previously encoded perceptual information in the form of visuo-spatial images, as well as constructing image-based mental representations of that environment (Bocchi et al., 2017). The ability to set goals, remember information, make effective decisions and execute plans - skills considered to be instrumental for the ability to sort, organise and effectively discard possessions, and thereby maintain a clean home environment (Frost & Hartl, 1996) - may therefore be heightened in hyperphantasic individuals, insofar as these processes partially rely on imagery. In turn, this may protect hyperphantasic individuals against the development of hoarding symptoms, particularly environmental clutter, which is the hoarding symptom domain considered to be most strongly influenced by executive functioning deficits (Frost & Hartl, 1996).
We also found some weak/anecdotal evidence to suggest hyperphantasic individuals may be less prone to excessive acquiring and less likely to endorse some hoarding-related beliefs and coping strategies (i.e., the need to exert excessive control over one’s possessions, feeling excessively responsible for items, relying on objects as memory-aids). However, due to the low strength of evidence, and corresponding pattern of non-significant frequentist tests, we are unable to draw any meaningful conclusions from these findings. Further research in larger, well-powered samples will be required to verify whether these results reflect true differences or merely represent artifacts of random variability or measurement error.
Clinical Implications
The results of this study may have clinical implications regarding the relevance of imagery-based conceptualisations and treatments for hoarding problems. In their original article, Sabel et al. (2025) tentatively suggested that difficulties visualizing may form part of the information processing deficits conferring vulnerability to hoarding problems, sitting alongside other impairments, such as memory, attentional and dysexecutive problems specified in Frost and Hartl’s (1996) Cognitive-Behavioural model. The authors go on to propose that treatments designed to remediate visualizing deficits (e.g., Functional Imagery Training; Rhodes et al., 2024), or coping approaches, that emphasise accepting and managing difficulties bringing images to mind, such as memories of important past events, may therefore hold relevance for hoarding problems. However, the results of the current study do not necessarily support such a proposition, as aphantasics were no more likely than typical visualizers to exhibit hoarding symptoms and showed mean levels of hoarding symptoms that approximated population norms. When considered in conjunction with research showing that individuals with elevated hoarding tendencies on average exhibit no differences in visualization abilities compared to community controls (Stewart et al., 2020; Yap & Grisham, 2019), such findings suggest there may be no need to remediate visualizing deficits in individuals who hoard or help them cope with such difficulties.
Instead, as hyperphantasics demonstrated fewer hoarding symptoms relative to typical visualizers in this study, findings tentatively suggest (pending replication and extension) that techniques designed to enhance imagining capacities beyond an individual’s baseline by making imagery richer, more vivid and specific, as well as encouraging more routine use of imagery in daily life, could yield beneficial down-stream effects on hoarding symptoms. For example, future experimental work may seek to test whether increasing the vividness and accessibility of memories that individuals fear forgetting by discarding through techniques such as memory-specificity training (Barry et al., 2021) leads to greater discarding ease, or whether electrically decreasing visual cortex excitability using transcranial direct current stimulation – a method that appears to increase mental imagery strength-leads to any temporary or sustained reductions in hoarding symptoms (Pearson, 2020). It would also be interesting to see whether increasing the vividness, strength and control of imagery ability makes individuals who hoard more, or less vulnerable to visual intrusions; a known clinical feature of hoarding problems (Stewart et al., 2020). However, these directions for future experimental and translational research are presented very tentatively, recognising that more studies should be conducted beforehand to confirm the link between hoarding and imagery, and elucidate their hypothesised mechanisms of association.
The results of this study may also hold relevance for practitioners using imagery-based techniques with hoarding clients. If visualizing difficulties were found to confer vulnerability to hoarding, techniques that rely on imagery, such as imaginal exposure (Koerner & Fracalanza, 2012) and imagery rescripting (Morina et al., 2017) could arguably be contraindicated for this population, as there is evidence suggesting individuals who are aphantasic benefit less from these treatments and find them unhelpful (Mawtus et al., 2024). However, as aphantasics were found to be no more likely than typical visualizers to show hoarding symptoms, and previous research has found that, on average, individuals who hoard show visualization abilities that approximate community norms (Stewart et al., 2020; Yap & Grisham, 2019), imagery-based treatments should be continued to be trialled for hoarding, with emerging preclinical evidence suggesting they may hold promise in this population (Fracalanza et al., 2024; Sabel et al., 2024). Nevertheless, we would advise practitioners to assess individuals’ visualizing abilities prior to using imagery techniques for hoarding, as we predict this ability may moderate the effectiveness of the intervention, and there is some evidence supporting this contention (Sabel et al., 2024).
Limitations and Future Research Directions
The findings of this study should be considered in light of several limitations. Firstly, we relied on introspective, self-report measures to assess participants’ visualizing abilities and hoarding symptoms. Although this is a standard research practice in both the hoarding and imagery fields (Blomkvist & Marks, 2023; Kellman-McFarlane et al., 2019), and the measures we employed are considered industry standard (Pearson, 2020; Sarvestani et al., 2025), this raises the possibility that the pattern of associations in this study may reflect common method variance. Future studies would therefore benefit from the inclusion of more objective measures. For example, the pupillary light response (Kay et al., 2022) or the binocular rivalry paradigm (Keogh & Pearson, 2018, 2024), could be used to cross-validate participants’ self-reported VVIQ scores and provide further verification of their group membership (i.e., as aphantasics). Similarly, pictorial clutter assessments (e.g., the Clutter Image Rating Scale; Frost et al., 2008) could be used to corroborate the presence and severity of clinically disabling clutter in participants’ homes. Alternative methods to self-report, such as descriptive experience sampling, should also be explored in future research with hoarding samples to further understand their experiences with mental events, such as imagery (McKelvie, 2021).
Secondly, although we rigorously screened the data to ensure valid data, future studies may benefit from assessment methods that permit more accurate differential diagnosis. For example, structured clinical interviews could be used in future research to ascertain the prevalence of clinically significant/diagnostic hoarding cases across groups. Without the use of a structured clinical interview, we are unfortunately unable to certify that hoarding behaviours resulting from the presence of other psychopathology, such as eating disorders (Novara et al., 2016), dementia (Hwang et al., 1998) and psychosis (Machado et al., 2019) are not muddying our severity estimates. We also did not assess whether participants’ visualizing abilities were congenital or acquired. For example, there are reports of individuals who previously had imagery but subsequently lost this ability via head injury or stroke (Knowles et al., 2021), which may have more widespread effects on cognition, unrelated to aphantasia.
Future researchers may also seek to improve upon our sampling and recruitment procedures. For example, despite our best efforts, we were only able to recruit a small number of hyperphantasics into the study, relative to our aphantasic and typical-visualizer groups, which may have limited the likelihood of detecting strong evidence for between-groups effects for this group. Although hyperphantasia and aphantasia are rare in the population (Wright et al., 2024) with most studies investigating these phenomena relying on small samples (e.g., between 15–25 per group; Kay et al., 2022; Keogh & Pearson, 2018; Milton et al., 2021), and we employed a host of ‘best practices’ given our small sample size this group (e.g., Bayesian inference with conservative priors, rigorous data-screening, case-control matching to reduce error variance etc), future research should endeavour to replicate our work, recruiting a larger sample of hyperphantasics. Future research may also consider recruiting a large general population sample where participants with imagery extremes are enlisted naturally, rather than via an aphantasia/hyperphantasia contact list, to eliminate the possibility of recruitment bias and demand characteristics. It is possible that participants in our research responded differently knowing the study was related to the fact that they identified as aphantasic or hyperphantasic (e.g., see Allbutt et al., 2011).
Finally, competing explanations for our findings should be tested in future experimental work. Although our case and control groups were matched on key confounds of interest (i.e., age and depression) and all demographic characteristics – making it more certain that variations in imagery ability were driving any differences in hoarding symptoms observed between groups, it is possible that unmeasured third variables provide a better account of the study findings. For instance, hyperphantasics may have lower levels of alexithymia (i.e., limited emotional awareness), which may reduce hoarding risk independently of imagery ability (Monzel et al., 2024; Pozza et al., 2015). Visualizing may also be reduced in autism spectrum disorder (King et al., 2024), and individuals who hoard show higher levels of autistic traits (Pertusa et al., 2012), which may provide a better explanation of the nexus between hoarding and imagery than our proposed mechanisms (i.e., elevations in hoarding beliefs, such as object memory concerns). Using a case-control design with cross-sectional measurements taken at a single time point also limits causal conclusions or inferences about temporal order. To overcome these drawbacks, future studies may therefore seek to test competing explanatory accounts, conduct experimental manipulations between hoarding and imagery, and/or employ longitudinal designs.
Concluding Remarks
Despite these limitations, the present research demonstrates that individuals with aphantasia do not appear to be at increased risk of hoarding symptoms, compared to their same aged, and equally depressed typical visualizing peers, although they may be prone to using objects as visual cues to facilitate recall; a hoarding specific coping strategy. Conversely, hyperphantasic individuals appear to be less susceptible to developing HD symptoms compared to same-aged typical visualizers and less likely to live in cluttered homes. This intriguing pattern of results appears to partially harmonize the conflicting findings found in previous research (e.g., Sabel et al., 2025; Stewart et al., 2020; Yap & Grisham, 2019) and suggest, pending replication and extension, techniques designed to make imagery stronger and more vivid, beyond an individual’s baseline could yield downstream positive effects on HD symptoms. Moreover, our findings suggest techniques that require the use of an imagery modality, such as imagery rescripting (Morina et al., 2017), and imaginal exposure (Koerner & Fracalanza, 2012) will likely not be contraindicated for most HD sufferers, and should continue to be researched (Fracalanza et al., 2024; Sabel et al., 2024).
Footnotes
Ethical Considerations
All procedures were reviewed and approved by the University of New South Wales human research ethics committee (HREAP-C file no. 3784). The protocol was carried out in accordance with the provisions of the World Medical Association Declaration of Helsinki.
Consent to Participate
All participants provided written informed consent prior to participation.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by an Australian Government Research Training Program Scholarship (RTP) awarded to Isaac Sabel by the University of New South Wales (UNSW).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The code and data supporting the findings of this study are openly available on the Open Science Framework at https://doi.org/10.17605/OSF.IO/T6YKA, ![]() .
.