
Abstract
Impaired Perceived Health (PH) is frequently encountered in Somatic Symptom Disorder (SSD). Health Anxiety (HA) and Psychological Attribution (PA) of symptoms are influential factors in the conversion of poor PH into Somatic Complaints (SC). This study explores the mediating roles of HA and PA in the relationship between PH and SC in SSD while controlling for family history of chronic disease and various demographic factors such as gender, age, education level, income level, and marital status. To better reflect the current DSM-5 SSD diagnosis, participants were recruited from seven different clinics across five health institutions in three major provinces of Turkey (Istanbul, Ankara, and Mersin), rather than only from psychiatric clinics. The cross-sectional study included a total of 314 SSD outpatients: 212 women (67.5%) and 102 men (32.5%), with ages ranging from 18 to 84 years (M = 39; SD = 14). The Whiteley Index and Symptom Interpretation Questionnaire, along with a semi-structured form questioning PH, SC, and demographics, were administered to all participants under the supervision of clinicians. Additionally, the Clinician Assessment Form was used as evidence of whether the patients had SSD or not. To check the indirect effect of PH on SC through HA and PA, mediation model 4 (parallel mediation) of the SPSS PROCESS macro was used. There was a significant total indirect effect of PH through HA and PA, b = −.12% CI [−.09,−.18], from which an indirect effect of PH on SC through HA was b = −.08, CI [−.05,−.12], and through PA it equaled b = −.04, CI [−.02,−.07]. The indirect to total effect ratio was .49.
Keywords
Introduction
According to the DSM-5 (APA, 2013), individuals diagnosed with Somatic Symptom Disorder (SSD) experience distressing somatic symptoms, accompanied by cognitive-affective and behavioral symptoms, typically lasting for six months or more. The prevalence of SSD in general practice is reported to be 7.7%, and its burden on the healthcare system is emphasized (Lehmann et al., 2022; Sirri et al., 2017). The diagnosis of SSD does not negate the possibility of the existence of medical illness variables. This marks a significant shift from older somatoform disorder diagnoses, which stipulated that physical symptoms could not be explained by a general medical condition. The DSM-5’s emphasis on the cognitive, affective, and behavioral experiences of individuals with SSD regarding their symptoms underscores the importance of considering the health and illness perceptions of this group. In this sense, many studies in the literature highlight Perceived Health (PH) related concepts such as body scanning, illness denial, and self-concept of bodily weakness, which have an impact on the prognosis of SSD (Klaus et al., 2015; Wollburg et al., 2013). Even in cardiovascular diseases or cancer with transparent medical sources, the weak correlation between objectively determined anatomical or functional abnormalities and the severity of somatic symptoms reveals how important PH is (Kohlmann et al., 2013; Kop et al., 2019). Individuals with SSD often report a high number of Somatic Complaints (SC) and poor PH, which can negatively impact their quality of life and functioning (Stanton & Campbell, 2014). However, the underlying mechanisms contributing to this relationship are not fully understood. PH and the number of SC in individuals with SSD are complexly intertwined with psychological factors such as Health Anxiety (HA) and Psychological Attribution (PA).
The existing literature suggests that HA and PA of somatic symptoms play a significant role in the experience and progression of SSD (Kirmayer et al., 2006; Wollburg et al., 2013). One of the valuable studies has shown that individuals with high HA are more likely to experience increased somatic symptoms, which in turn leads to poorer PH and health-related quality of life. This relationship persists even when accounting for depressive symptoms, indicating that HA is a critical factor in the experience of somatic symptoms and PH (Murphy et al., 2017). Furthermore, individuals with SSD who perceive their health as poor are more likely to experience heightened HA, which can lead to an increased focus on bodily sensations and a tendency to catastrophize about the potential medical causes of their symptoms (Deary et al., 2007; Kirmayer et al., 2006). Individuals with SSD often exhibit a heightened focus on bodily sensations, a tendency to misinterpret them as signs of serious illness, and a preoccupation with their health that can lead to excessive healthcare utilization and disability (Stanton & Campbell, 2014).
Additionally, the tendency to attribute physical symptoms to psychological factors, such as stress or emotional distress, may further contribute to a diminished sense of overall health and well-being in those with SSD (Guidi et al., 2013). These cognitive-affective and behavioral patterns can contribute to the amplification and persistence of somatic symptoms as individuals become increasingly focused on and anxious about their PH issues, leading to a vicious cycle of increased symptom reporting (Ballas & Staab, 2003). By examining these potential mediating mechanisms, the current study aims to elucidate the psychological processes that underlie the link between PH and SC in this clinical population. To more accurately reflect the current DSM-5 SSD diagnosis, participants were recruited from seven different clinics within five health institutions in three major provinces of Turkey (Istanbul, Ankara, and Mersin), rather than solely those applying to psychiatric clinics.
Furthermore, to determine whether the participants had SSD, the opinions of 10 clinicians working in these clinics and assisting with the case collection phase of the study were consulted.
Drawing from this body of work, the current study proposes that the association between PH and SC may be explained in part by individuals’ tendencies to experience health-related anxiety and attribute their physical symptoms to psychological factors.
While various studies in the literature examine the relationships among the variables relevant to the current study, no research has explicitly focused on the mediating roles of HA and PA in the relationship between PH and SC in the SSD outpatient sample. It would be beneficial to present additional evidence elucidating the underlying mechanisms connecting PH and SC. In this context, the study’s hypotheses are as follows: H1: A significant relationship exists between perceived health, somatic complaints, health anxiety, and psychological attribution. H2: Health anxiety and psychological attribution have a mediating role in the relationship between perceived health and somatic complaints, while controlling for family history of chronic disease and various demographic variables such as gender, age, education level, income level, and marital status.
Methods
Participants
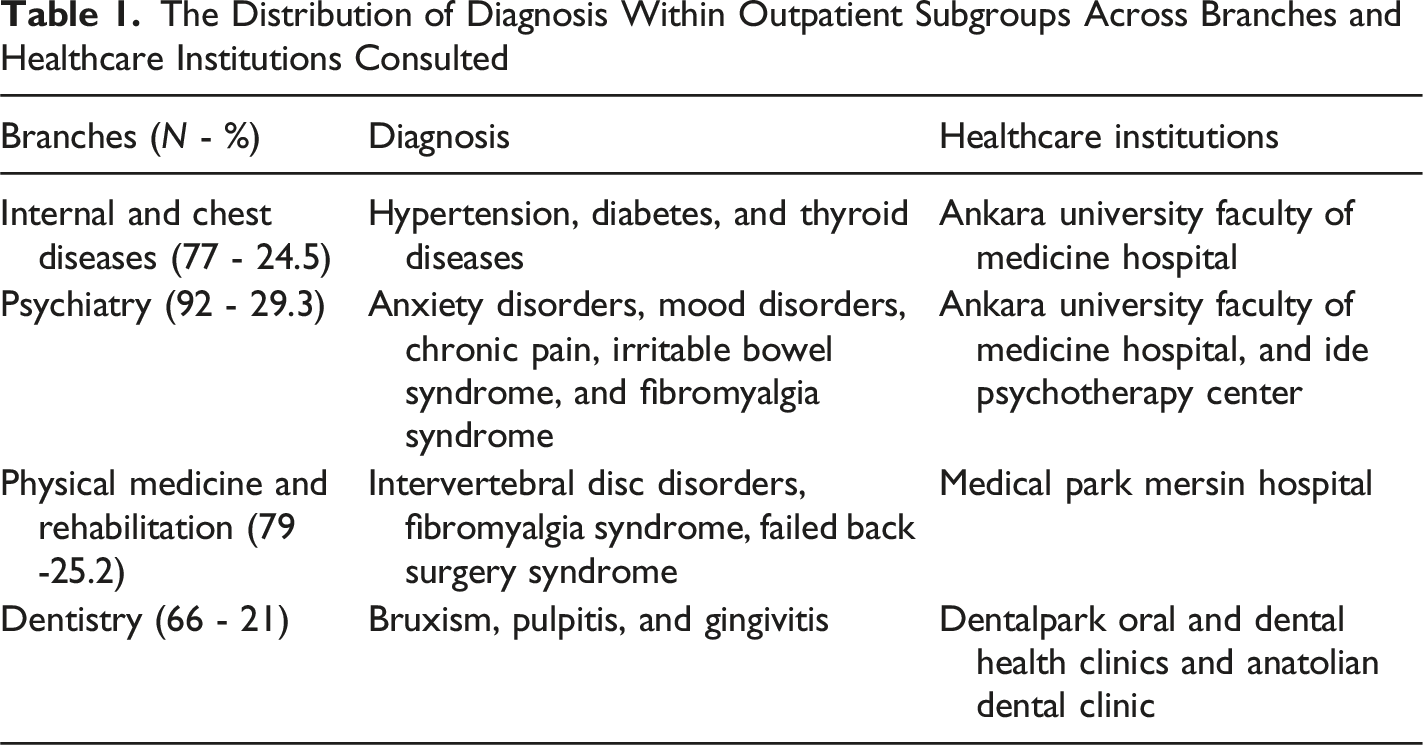
The participants of this study were 314 SSD outpatients attending the Departments of Internal Diseases, Chest Diseases, and Mental Health and Diseases at Ankara University Faculty of Medicine Hospital, the Department of Physical Medicine and Rehabilitation at Medical Park Mersin Hospital, Dental Park Oral and Dental Health Clinics, Anatolian Dental Clinic, and Ide Psychotherapy Center. To prevent confusing effects on the generalization of the results, the participants were recruited from three metropolitan cities reflecting the similar socio-cultural structures of Turkey.
The Distribution of Diagnosis Within Outpatient Subgroups Across Branches and Healthcare Institutions Consulted
Measures
The Whiteley Index (WI-7)
The Whiteley Index, developed by Fink et al. (1999) by revising the scale created by Pilowsky (1967) to measure HA, is a seven-item dichotomous (yes/no) scale. The internal consistency, Cronbach’s alpha value of the scale, whose Turkish adaptation was carried out by Güleç et al. (2013), was found to be .78 in the validity and reliability study and .69 in the current study.
Symptom Interpretation Questionnaire (SIQ)
Developed as a self-assessment scale by Robbins and Kirmayer (1991), the SIQ consists of items to evaluate individuals’ attributions about their symptoms. The scale includes 42 items, comprising 13 situations involving common physical symptoms and four statements directed at the participants for each situation. Participants are asked to score the sentences containing psychologized, somatized, and normalized references regarding the causes of the conditions on a four-point scale and to indicate whether these situations occur for them on a binary scale of yes/no. In the validity and reliability study of the scale, conducted faithfully to the original by Güleç and Sayar (2005), Cronbach’s alpha and item-total score correlation values were .82 and .28-.57 for the psychologized subscale, .76 and .17-.50 for the somatized subscale, .82 for the normalized subscale, and .27-.61.
Semi-Structured Form
The researcher created it to assess PH and SC along with demographic and control variables (gender, education level, income level, age, marital status, and family history of chronic disease). Patients rated their current physical and mental health over the past month using a 5-point Likert scale (0 = severely impaired, 4 = not at all impaired) for the PH variable in this form. The PH variable consists of the sum of these patients’ evaluations. Additionally, the number of SC that the patients taken from this form have experienced so intensely that they needed to consult a doctor in the last month constitutes the SC variable.
Clinician Assessment Form
The researcher created this form to obtain the opinions of 10 clinicians in 1 min who supported the case collection phase regarding the patients they referred to the study. In this form, clinicians were asked brief questions about whether the relationship they established with the symptoms of the patients they referred included the extremity in the DSM-5 SSD diagnosis, and patients with SSD were selected accordingly.
Statistical Analysis
Characteristics of the Sample
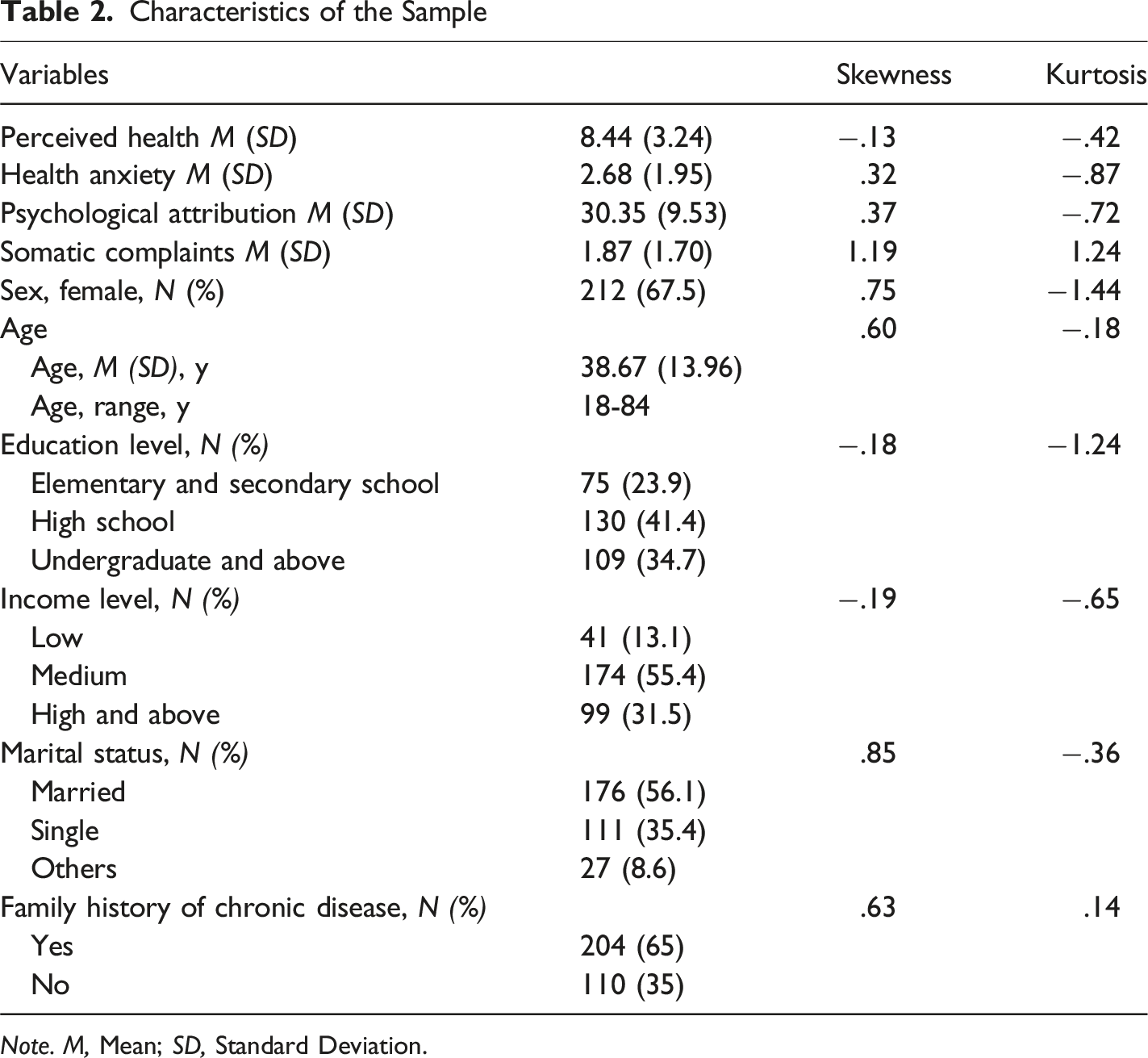
Note. M, Mean; SD, Standard Deviation.
Correlations Between Variables
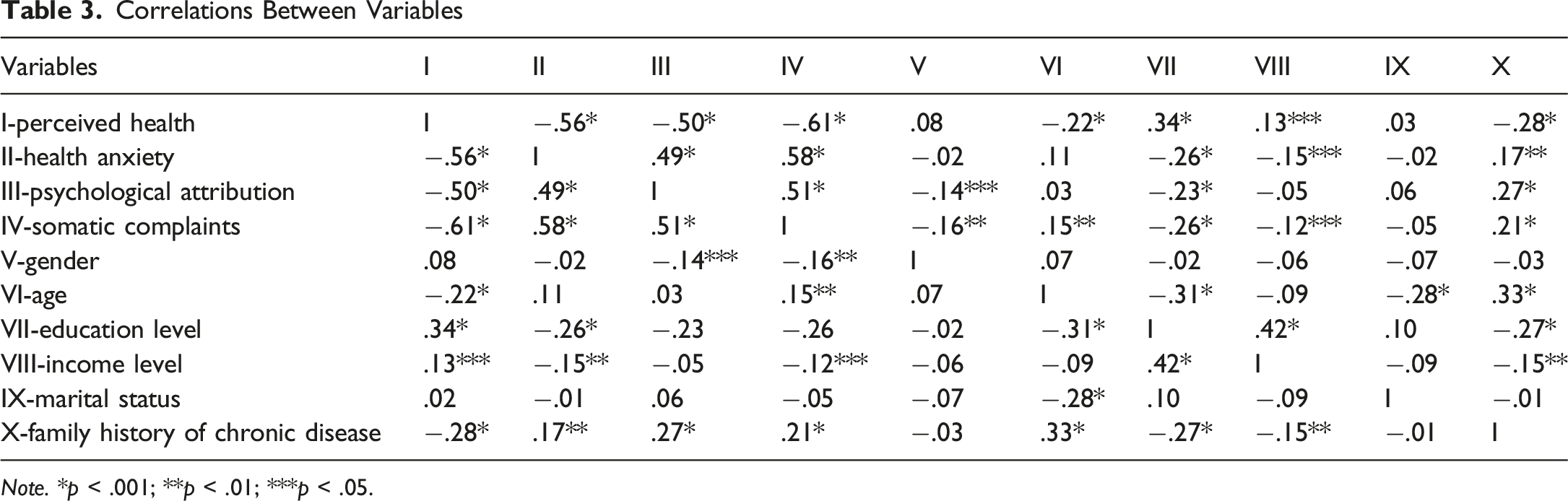
Note. *p < .001; **p < .01; ***p < .05.
To assess the multicollinearity required for regression analysis, variance inflation factors and tolerance values for each variable were evaluated. The VIF for the variables was 1.62, and the tolerance was .62, indicating no multicollinearity issues. The mediating roles of HA and PA in the relationship between PH and SC were examined using the Regression-Based Bootstrapping Technique. A total of 5,000 bootstrap samples were used, and the predictions were assessed within a 95% confidence interval that was bias-free and reflected corrected results. The mediation model was structured according to Model 4, showing the Parallel Multiple Mediator Model, which involved one independent variable, one dependent variable, and two mediators (Coutts & Hayes, 2023). The significance of the effects was tested by ensuring that the 95% confidence interval did not include zero, utilizing the bootstrap technique.
Results
Sample Characteristics
Since 36 out of 350 outpatients participating in the study had missing data, the analyses were conducted with 314 outpatients, comprising 212 women (67.5%) and 102 men (32.5%), aged between 18 and 84 years (M = 38.67 years, SD = 13.96). Considering the kurtosis and skewness values, the data in the study show a normal distribution (Tabachnick & Fidell, 2019). Table 2 provides details about the sample characteristics.
Pearson Analysis
Table 3 shows the correlation analysis results for the relationships among variables within the context of the research’s first hypothesis.
In Table 3, which presents the highly significant correlation (p < .001) among the four main variables in the study, it is evident that as PH increases, HA, PA, and SC scores decrease, as expected. Additionally, this table shows correlations among family history of chronic disease, gender, age, education level, income level, and marital status variables, which are included as control variables in the mediation analysis, both among themselves and with the four primary variables. Mediation analysis was conducted after identifying significant correlations among the variables.
Mediation Analysis Results
Main Effects on PH, HA, PA, SC and Control Variables
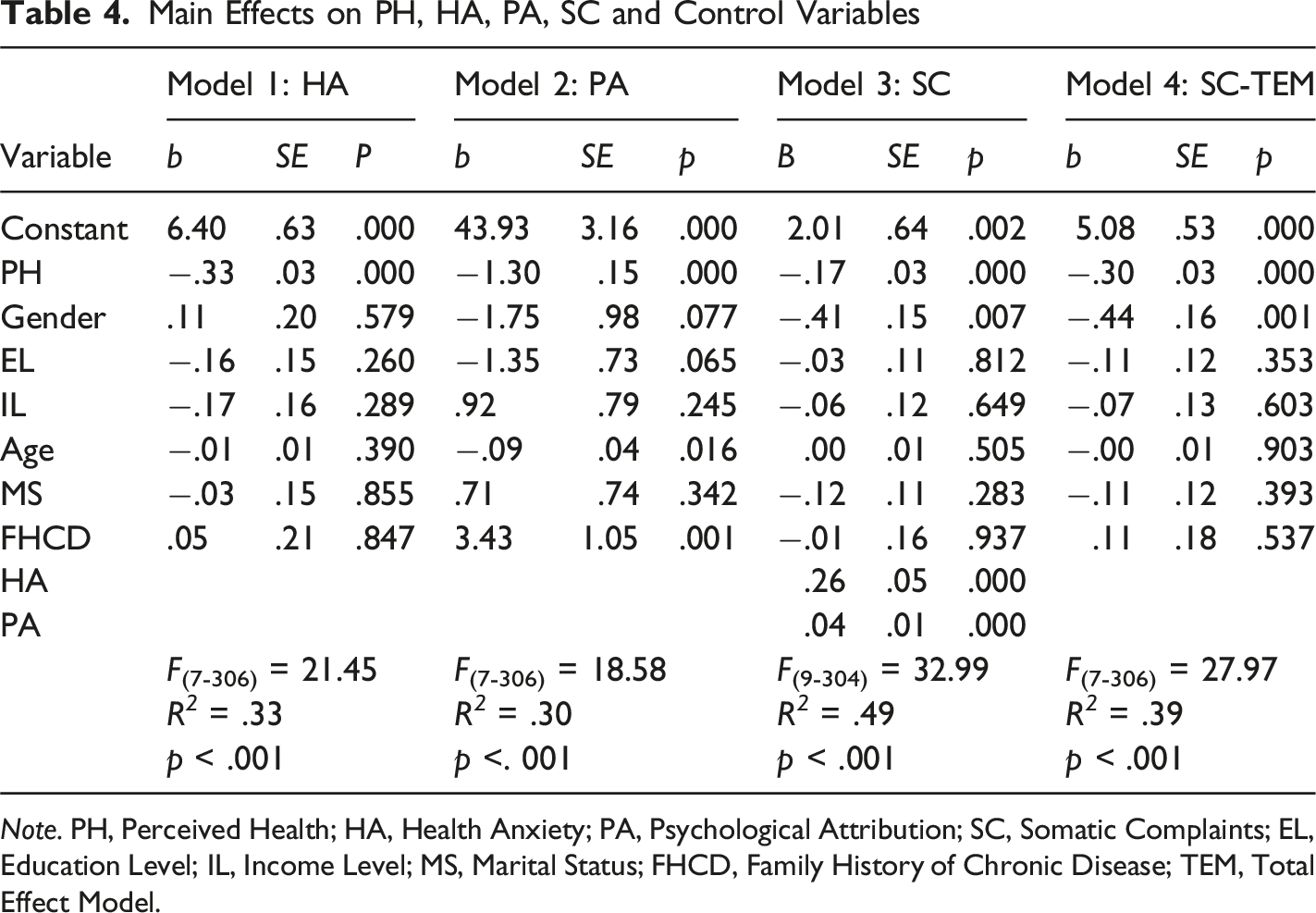
Note. PH, Perceived Health; HA, Health Anxiety; PA, Psychological Attribution; SC, Somatic Complaints; EL, Education Level; IL, Income Level; MS, Marital Status; FHCD, Family History of Chronic Disease; TEM, Total Effect Model.
Unstandardized Coefficients and 95% Bootstrap Confidence Intervals
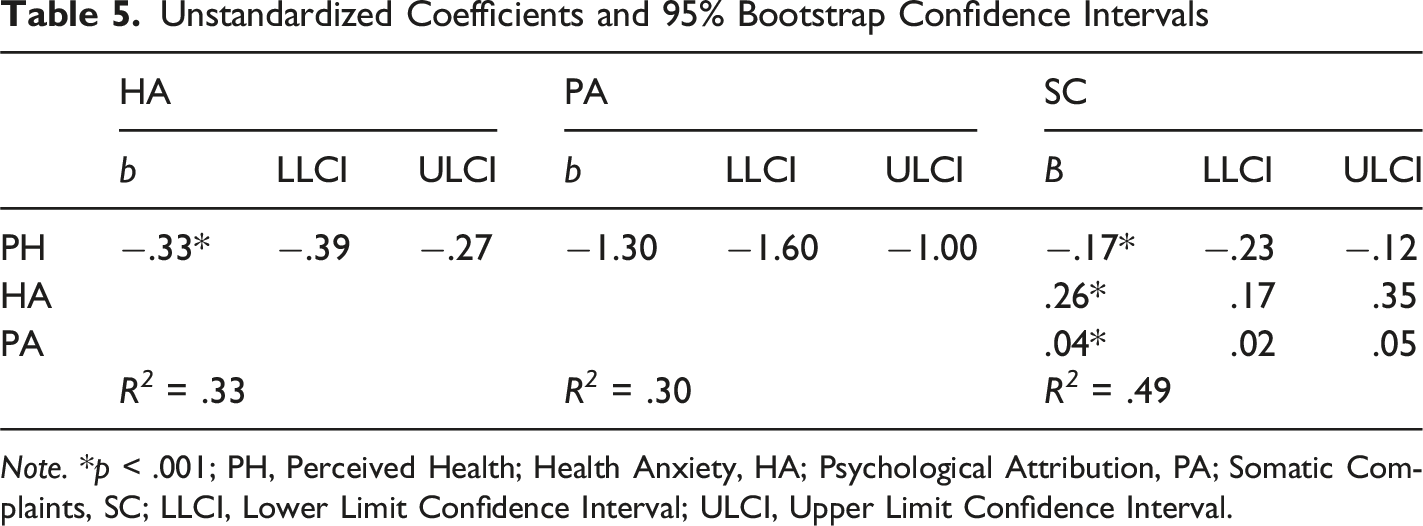
Note. *p < .001; PH, Perceived Health; Health Anxiety, HA; Psychological Attribution, PA; Somatic Complaints, SC; LLCI, Lower Limit Confidence Interval; ULCI, Upper Limit Confidence Interval.
The model developed under the second hypothesis of the research, concerning the mediating roles of HA and PA in the impact of PH on SC while controlling for family history of chronic disease and various demographic factors such as gender, age, education level, income level, and marital status., is illustrated in Figure 1. Perceived Health Predicts Somatic Complaints Through Health Anxiety and Psychological Attribution [R
2
= .49, F(9-304) = 32.99, p < .001]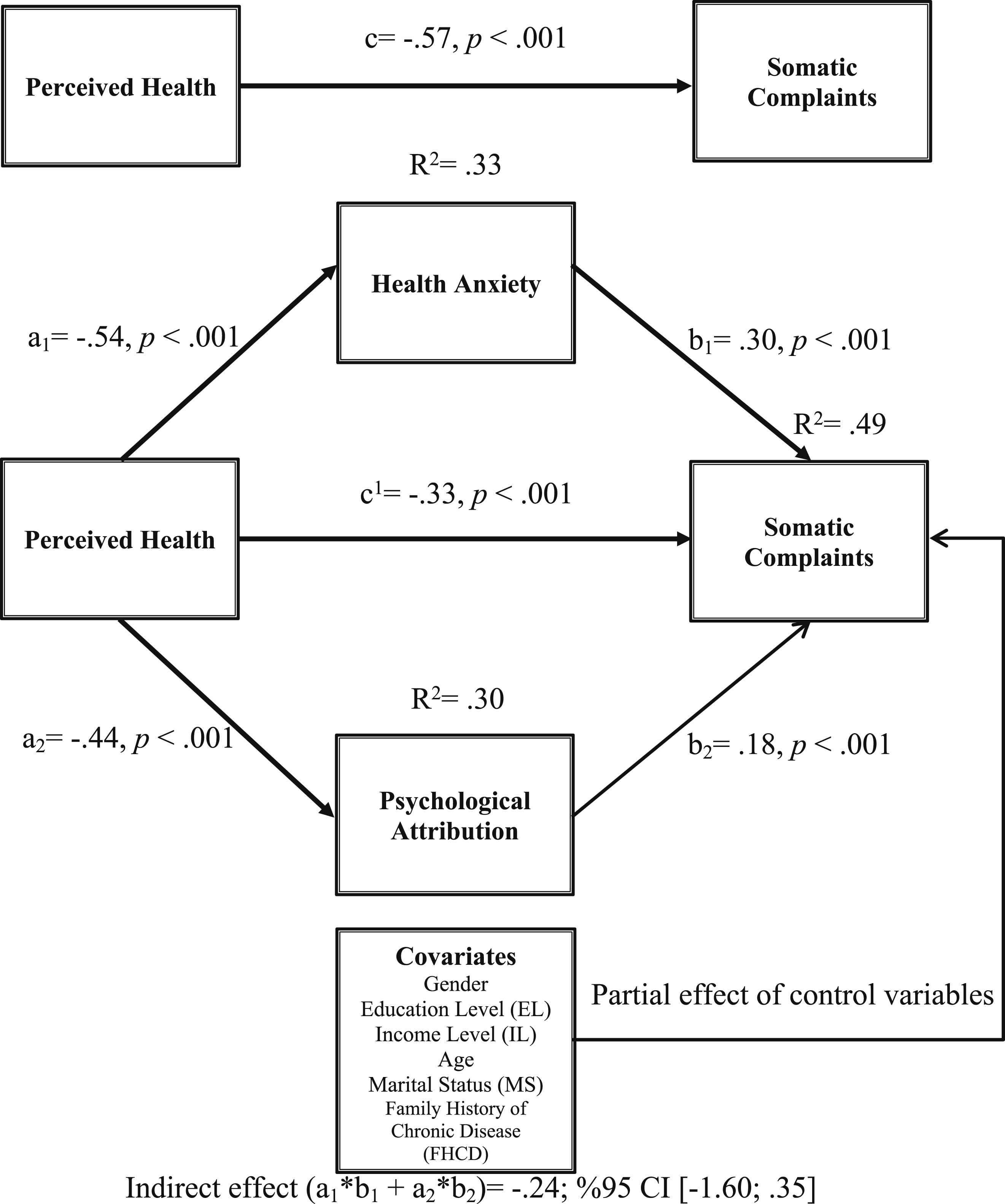
Direct and Indirect Effects of Perceived Health on Somatic Complaints
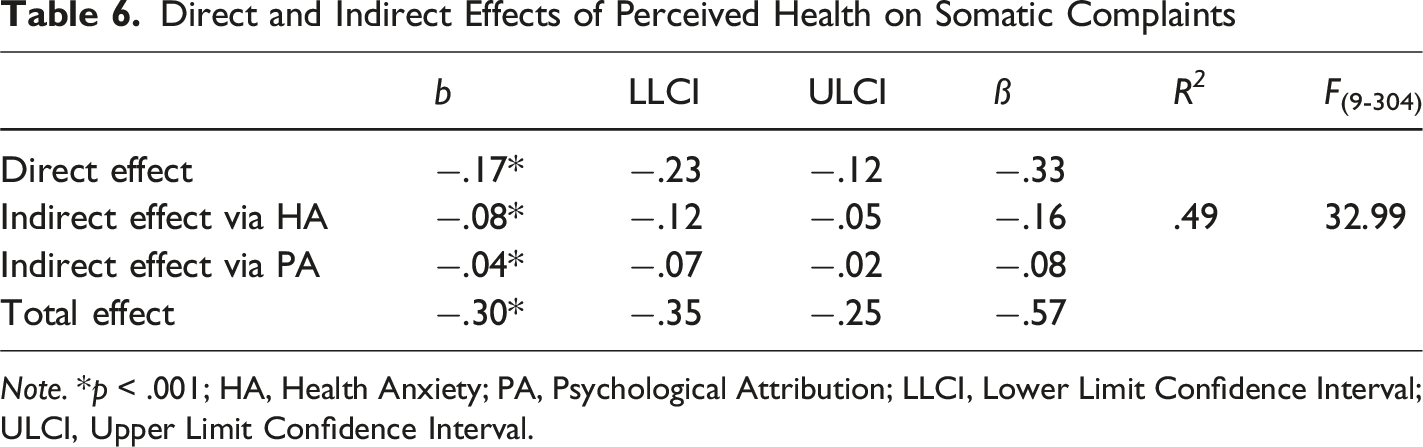
Note. *p < .001; HA, Health Anxiety; PA, Psychological Attribution; LLCI, Lower Limit Confidence Interval; ULCI, Upper Limit Confidence Interval.
In Table 6, It can be said that the total effect of PH on SC is −.30. This total effect occurs through the partial mediation of HA and PA [F (3-310) = 32.99, p < .001]. PH, HA, and PA accounted for 49% of the variance in SC. It was concluded that the mediating role of HA and PA in the effect of PH on SC is significant, and these confidence intervals do not include any zero (0) points. (Bootstrap Coefficient = −.24, 95% CI [−.12; −.02]). When examining whether the indirect effects are statistically different, it was observed that HA does not have a significantly higher indirect effect than PA (b = −.08, 95% CI [−.09; .02]). Additionally, approximately 27% of PH’s total effect on SC is from HA (−.08/−.30), and about 13.5% is from PA (−.04/−.30). Considering both variables, 40.5% of the total effect is due to indirect influence.
Discussion
This study examined how Health Anxiety (HA) and Psychological Attribution (PA) mediate the relationship between Perceived Health (PH) and Somatic Complaints (SC), while controlling for family history of chronic disease and various demographic factors such as gender, age, education level, income level, and marital status among individuals with Somatic Symptom Disorder (SSD). The results showed that PH had a significant negative relationship with HA and PA, and these variables, in turn, had a positive relationship with SC. PH was found to have a direct negative effect on SC, and this effect decreased but remained significant when HA and PA were included as mediators, indicating a partial mediation effect (Hayes & Preacher, 2014). Specifically, individuals with poorer PH may be more likely to experience SC if they also exhibit high levels of HA and attribute their symptoms to psychological causes (Mayerl et al., 2017; Wiedermann & Von Eye, 2015).
The results align with previous research highlighting the importance of cognitive and affective factors in the experience of somatic symptoms (Smakowski et al., 2024). Individuals with SSD often exhibit heightened attention to bodily sensations and a tendency to interpret these sensations as signs of illness (Stanton & Campbell, 2014). This heightened attention and interpretation bias, which are core components of HA, can contribute to increased anxiety and worry about health, further exacerbating SC (Deary et al., 2007). Moreover, longitudinal analyses reveal that fluctuations in PH predict subsequent changes in health-related anxiety, which in turn forecast increases in somatic symptom burden over time (Csibi et al., 2023; Joustra et al., 2018). Similarly, PA, which involves attributing bodily symptoms to psychological causes, can also intensify the experience of somatic distress and contribute to a cycle of symptom amplification (Douzenis & Seretis, 2013). Psychological attribution of bodily sensations to mental origins further intensifies perceived distress and functional impairment, as the co-occurrence of health anxiety and somatic symptom burden has been linked to heightened psychological distress (Rask et al., 2024). Consequently, attributing symptoms to psychological origins may sustain safety-seeking illness behaviors, thereby perpetuating the mediating role of health anxiety identified between functional somatic symptoms and maladaptive illness behavior (Ma et al., 2019).
The study’s findings contribute to a growing body of literature emphasizing the complex interplay between physical and psychological factors in SSD. The significant indirect effects of HA and PA suggest that interventions targeting these psychological processes may be beneficial in reducing somatic complaints and improving overall well-being in individuals with SSD. Cognitive-behavioral therapy, for example, has shown promise in addressing HA and PA and may thus be a valuable treatment approach for SSD (Axelsson & Hedman-Lagerlöf, 2023; Creed, 2011). Targeting these maladaptive attributional beliefs through cognitive-behavioral interventions may attenuate the reinforcing cycle of health-anxiety-driven symptom amplification (Ma et al., 2019; Rachor & Penney, 2020).
In addition to these, although various studies in the literature examine the relationships among the variables relevant to the current study, no research has explicitly focused on the mediating roles of HA and PA in the relationship between PH and SC in the SSD outpatient sample. Therefore, it will be helpful to include literature findings on the main effects between variables in this section.
Accordingly, in Model 2, the effects of PH and age on PA were negative (b = −1.30, p < .001; b = −.09, p < .05, respectively), while the effect of Family History of Chronic Disease (FHCD) on PA was positive (b = 3.43, p < .01). Recent revisions of DSM-5 and ICD-11 highlight that PH, age, and FHCD critically influence PA in SSD, a condition marked by persistent somatic distress and maladaptive cognitive-affective processes (Smakowski et al., 2024). Consistent with evidence that illness representations influence subjective distress, lower self-rated health predicted more negative psychological attributions. At the same time, a positive FHCD was linked to stronger maladaptive attribution of symptoms (Rometsch et al., 2023). These findings underscore the complex interplay of patient-reported health perceptions and genetic predispositions in shaping the cognitive and emotional responses to somatic symptoms (Smakowski et al., 2024). Specifically, individuals with lower self-rated health are prone to develop more maladaptive psychological attributions, suggesting a significant role of subjective illness representations in the etiology of SSD (Axelsson et al., 2020). Furthermore, a family history of chronic disease may intensify these maladaptive attributions, potentially due to learned illness behaviors or heightened health anxiety within the family unit (Nazzal et al., 2021). This highlights the importance of assessing these factors to develop targeted interventions that address both individual illness perceptions and familial health contexts in managing SSD (Mander et al., 2017; Martin & Piehler, 2020).
Additionally, these results concur with prior evidence that younger age is associated with elevated health anxiety, thereby fostering more adverse psychological attributions of somatic experiences (Csibi et al., 2023). This phenomenon is particularly salient in the context of functional somatic symptoms, where younger individuals tend to catastrophically interpret bodily sensations, leading to heightened health anxiety and inappropriate illness behaviors (Ma et al., 2019). This susceptibility in younger populations suggests a potential developmental vulnerability, especially given the observed positive association between health anxiety and self-reported unspecific somatic complaints in preadolescence and adolescence (Rask et al., 2024). Additionally, older adults tend to exhibit less severe clinical presentations of anxiety compared to younger individuals, although it is possible they may underreport symptoms (Guineau et al., 2023). This potential underreporting may stem from a variety of factors, including ageism within healthcare, a prioritization of somatic comorbidities, or a greater inclination among older adults to normalize anxiety symptoms, unlike younger populations who may exhibit increased self-monitoring of their health status, potentially influenced by contemporary trends, which could contribute to heightened health worries (Hendriks et al., 2024).
Looking at Model 3, the effects of the independent variable PH and the control variable gender on SC were negative (b = −.17, p < .001; b = −.41, p < .01, respectively), while the effects of mediating variables HA and PA on SC were positive (b = .26, p < .001; b = .04, p < .001, respectively). Additionally, in Model 4, it is shown that the effects of the independent variable PH and the control variable gender on the total effect of the SC are negative (b = −.30, p < .001; b = −.44, p < .01, respectively). Since the literature on the primary variables has already been discussed, it is appropriate to present the literature related to gender, one of the control variables, among these findings. The findings indicate that perceived health and gender are significant determinants of somatic complaints within a SSD population, suggesting that interventions targeting health perceptions and gender-specific factors may be beneficial for this cohort (Heseltine-Carp et al., 2023; Scheffers et al., 2018). Furthermore, the observed negative association with male gender aligns with previous research indicating that males often report less subjective distress, which could imply a protective factor against somatic complaints (Rometsch et al., 2023). This aligns with findings suggesting that female gender is associated with higher rates of SSD (Nazzal et al., 2021). This gender disparity in prevalence may be influenced by various factors, including differences in how symptoms are reported and culturally influenced coping mechanisms (Lunov, 2024; Nazzal et al., 2021).
The study’s other strengths include recruiting participants from diverse clinical settings, reflecting the heterogeneity of SSD presentations, and aligning with DSM-5 diagnostic criteria (Herzog et al., 2015). To better reflect the current DSM-5 SSD diagnosis, participants were recruited from seven different clinics across five health institutions rather than only from psychiatric clinics (Rief & Martin, 2014). The multicenter recruitment across internal, chest, psychiatry, and dental clinics mirrors the diverse sampling strategies employed in prior SSD validation studies, which have been shown to enhance the generalizability of findings across varied clinical settings (Martinelli et al., 2025). Such heterogeneous sampling enhances the external validity of the findings and permits examination of DSM-5 SSD criteria across distinct clinical contexts (Xiong et al., 2017).
Another advantage of this study’s generalizability lies in the procedure followed by the doctors who directed the participants to the research. To determine whether the participants had SSD, the opinions of 10 clinicians working in these clinics and assisting with the case collection phase of the study were consulted. The opinions of the doctors regarding whether the patient they referred has SSD have been obtained through the “Clinician Assessment Form”. In this form, clinicians were asked brief questions about whether the relationship they established with the symptoms of the patients they referred included the extremity in the DSM-5 SSD diagnosis, and patients with SSD were selected accordingly. Trained clinicians used a standardized form to ensure inter-rater reliability and diagnostic consistency (Röhricht et al., 2019). Clinicians received standardized training and ongoing supervision to ensure fidelity to the DSM-5’s perspective on SSDs, as demonstrated in comparable multicenter SSD studies (Hijne et al., 2022).
Finally, another point to consider regarding the study’s generalizability is that the participants were recruited from three metropolitan cities in Turkey, which have similar socioeconomic and cultural structures. Since somatic presentations are influenced by culture and often occur alongside depressive and anxiety symptoms, recruiting patients from three metropolitan cities in Turkey that share similar socioeconomic backgrounds helps ensure representation of the familiar sociocultural environment affecting how symptoms are expressed (Bagayogo et al., 2013). Somatic manifestations frequently co-occur with depressive and anxiety disorders. They are shaped by culturally specific idioms of distress, underscoring the need to examine these patterns within Turkey’s urban sociocultural context (Salmon et al., 2022). Given that cultural norms in Turkey often discourage overt emotional expression, individuals may prefer to express psychological distress through bodily complaints, a pattern consistent with cross-cultural findings on somatization (Tang et al., 2025). Indeed, prior research demonstrates that levels of somatization vary across cultures, reflecting different social and cultural contexts that influence symptom expression (Barbati et al., 2022). This culturally mediated focus on somatic symptoms has been documented in non-Western populations, where physical symptom reporting often exceeds affective reporting (El-Ammari et al., 2023). In line with observations from Chinese cohorts, where somatic expression was more common than emotional distress, Turkish patients often articulate distress somatically rather than affectively (Xiong et al., 2017). Supporting evidence from Arabic-speaking refugee outpatients, who report moderate somatic symptoms alongside psychological distress, further confirms the dominance of bodily expressions of distress across different cultures (Kim et al., 2021; Lindheimer et al., 2020). Additionally, mental health stigma that discourages acknowledgment of psychological issues may increase somatic symptom reporting in Turkish urban populations, reflecting the culturally mediated pathways described by Kirmayer and Ryder (Lindheimer et al., 2020). As a result, internalized stigma may be an essential predictor of somatic symptom severity in these groups (Lindheimer et al., 2020). Empirical evidence also shows that individuals with depressive disorders are more likely to present with somatic symptoms, highlighting the close connection between these conditions (Tang et al., 2025). These data emphasize the importance of using the variables of PH and SC in this study, both because cultural and culturally-based perceptual factors can influence them, and of using the variables of HA and PA because somatic symptoms often co-occur with depression and anxiety symptoms.
Limitations and Future Directions
The current study has several limitations that should be considered when interpreting the findings. The cross-sectional design of the current study restricts the ability to establish causal relationships among the variables. This limitation is inherent in cross-sectional research, as it captures a snapshot in time and does not allow for the examination of temporal precedence or the dynamic nature of the constructs. Future longitudinal studies are necessary to understand better the causal pathways and the longitudinal interplay between PH, HA, PA, and SC. Longitudinal designs would enable researchers to trace the directionality of these relationships and elucidate how changes in one variable may precede and influence changes in the others over time. This would provide more robust evidence regarding the temporal and causal links between the key constructs, leading to a more comprehensive understanding of the complex mechanisms underlying the associations among PH, HA, PA, and SC.
Second, the study relied on self-report measures, which may be subject to biases and may not capture the full complexity of the constructs. Future research should consider incorporating objective measures, such as physiological indicators of health and well-being, to provide a more comprehensive assessment.
Furthermore, while providing valuable insights, this study’s correlational methodology may be inadequate for drawing conclusive findings regarding the causal linkages between the variables; instead, an experimental design that manipulates the key factors may be more appropriate to establish stronger causal inferences.
The present study was conducted within a specific cultural context, which may limit the generalizability of the findings to other populations and settings. Further research is needed to explore how cultural, demographic, and contextual factors may influence the relationships between PH, HA, PA, and SC. Examining these factors could provide valuable insights into the complex interplay between physical and mental health and help inform more tailored and effective interventions for addressing SC across diverse populations.
Conclusion
In conclusion, the current study presents findings for the partially mediating roles of HA and PA in the relationship between PH and SC among individuals with Somatic Symptom Disorder (SSD). These findings were reached while controlling for family history of chronic disease and various demographic factors such as gender, age, education level, income level, and marital status. The results indicate that considering both physical and psychological factors might be beneficial when assessing and managing somatic complaints; it also suggests the importance of a more holistic, biopsychosocial approach to healthcare. Future research may be necessary to elucidate the complex interplay between these constructs further and to explore potential moderating and contextual factors that might influence these relationships. Additionally, longitudinal investigations and incorporating both subjective and objective measures could provide a more comprehensive understanding of the dynamic nature of the associations between PH, HA, PA, and SC, potentially leading to more tailored and effective interventions for addressing these issues across diverse populations.
Footnotes
Acknowledgments
The author would like to sincerely thank the clinicians and their assistants who kindly gave their time to guide outpatients in this study. The author would also like to thank the participants who contributed to this research.
Ethical Considerations
The Social and Human Sciences Research and Publication Ethics Board at Istanbul Medeniyet University reviewed and approved the study involving human participants under ethical permission IMU-3516-48 on January 29, 2018.
Consent to Participate
All patients/participants participated in the research voluntarily and anonymously. Informed consent was obtained from all participants for inclusion in the study. Their data are stored in coded materials and databases without personal data. The author has a policy in place to manage and keep data secure.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Datasets presented in this article are available from the corresponding author upon reasonable request