
Abstract
Functional somatic disorders (FSD) result from a complex interplay of biological, psychological, and social factors, the combination of which varies between individuals. Professional and academic communities recommend an integrative, biopsychosocial, and personalized approach in order to achieve early diagnosis, an appropriate understanding of predisposing, triggering, and maintaining factors, and effective treatment. In order to obtain an integrative understanding, constructing a case formulation is suggested to be an important skill for clinicians treating patients with complex health conditions—such as FSD. However, in daily practice, many clinicians are struggling to conceptualize and then implement the biopsychosocial approach into their work with children and their families. This sustains the risk of a fragmented understanding of the child’s symptoms and functioning, and consequently fragmentation of health care. As members of a multidisciplinary team of professionals who treat children and adolescents with complex FSD, we here describe and share our experience of a clinical conversational tool—the biopsychosocial board—that we use to promote communication and to achieve an integrative understanding of the patient’s symptoms. We highlight the clinician’s ability to facilitate and co-construct a biopsychosocial case formulation together with the patient and family because this in the next turn will function as a roadmap to effective and personalized treatment. Used in such a way, we find that our conversation tool has the potential to be an innovative and useful tool for broad diagnostic assessment and identification of effective treatment options tailored to the individual child.
Keywords
Functional somatic disorders (FSD) is an overarching term to include a broad array of symptoms of physical discomfort, irregular function, and motor and sensory disturbances (Kozlowska et al., 2020). Examples can be disorders of long-lasting pain, fatigue, dizziness, irregular bowel functioning, nausea, convulsions, gait distortions, paralysis, and loss of vision. Although medical assessment cannot reveal an identifiable disease process, the symptoms reflect disturbances in neurophysiological regulation (Agorastos and Chrousos, 2021; Kozlowska et al., 2020). Some patients develop anxiety and depressive symptoms, and experience severe functional and social disability (Campo, 2012; Garralda and Rask, 2015). Between 4% and 10% of children and adolescents in the general population experience functional symptoms to such an extent that they need treatment (Garralda and Rask, 2015). Children with FSD have an increased risk of functional somatic symptoms, anxiety, and depression later in adolescence and adulthood (Bohman et al., 2012; Campo, 2012; Horst et al., 2014).
It is well recognized that FSD are related to negative life events and trauma, and involves a variety of biological, psychological, and social factors in complex interplay (Agorastos et al., 2019; Kozlowska et al., 2020; You et al., 2019). Although the exact pathogenic mechanisms are still unclear, we now have sound research-based knowledge supporting FSD to reflect disturbances in the neurophysiological regulation of the stress regulation system of the body (Agorastos and Chrousos, 2021; Chrousos, 2009; Kozlowska et al., 2020). Through evolution, living organisms have developed a cohesive and finely regulated internal physiological environment (homeostasis) that controls all vital processes and protects the organism against disease, injury, and external danger. A number of different biopsychosocial factors—stressors—can lead to stress, which in this context is defined as a physiological condition where homeostasis is disrupted or threatened to become so (Chrousos, 2009). Changes in homeostasis trigger carefully regulated physiological processes (stress responses) and change in behavior to minimize deviations and maintain a stable internal milieu. These body stress responses are necessary for normal functioning and survival, and are in many situations desirable—for example, when exercising physical or mental activity, or playing (Agorastos and Chrousos, 2021). However, when a stressor exceeds the natural regulatory capacity of the organism, maladaptive stress responses may occur reflected in a variety of somatic symptoms and a feeling of disease (Agorastos and Chrousos, 2021; Kozlowska et al., 2020).
A number of different biopsychosocial stressors in complex interplay with the body systems contribute to both symptom development and maintenance. Conditions related to stressor (type and timing) combined with individual vulnerability factors such as personality, social skills cognitive skills, and health make the individual more or less vulnerable. Genes, gender, previous life experiences, and epigenetic mechanisms are factors that affect the individual’s vulnerability to stress and stress management (Agorastos et al., 2019; Stavrou et al., 2017). A big traumatic event and/or the cumulative effect of more common negative life events during the child’s vulnerable developmental periods (fetal life, early childhood, and puberty) may lead to adverse effects on brain structures and functions, and the stress regulation system of the body (Agorastos et al., 2019; Diez et al., 2020; Felitti et al., 1998; You et al., 2019). This complex interplay of biopsychosocial factors early in life is known to play an important role in the etiology of functional somatic symptoms and disorders later in adolescence and adulthood (Agorastos et al., 2019; Diez et al., 2020; Pervanidou and Chrousos, 2018).
A biopsychosocial understanding and approach
Recognized professional and academic communities recommend that FSD must be understood in the light of the biopsychosocial model of illness, and emphasize an integrative, biopsychosocial approach to achieve an appropriate understanding and effective treatment of the individual child (Garralda and Rask, 2015; Gjems and Helgeland, 2018; Kozlowska et al., 2021; Liossi and Howard, 2016). Since children are different when it comes to genes, previous experiences, health, personality, cognitive skills, coping strategies, and current life situation, there are individual differences in terms of which factors that predispose, trigger, and maintain their symptoms (Garralda and Rask, 2015; Liossi and Howard, 2016). Similarly, there will be differences in which factors that affect symptom experience and illness behaviors (Institute of Medicine, 1987). Thus, in order to succeed in treatment, a holistic understanding of the individual child and its symptoms is of crucial importance because it guides the way to personalized—often interdisciplinary and multimodal—treatment (Kozlowska et al., 2020; Liossi and Howard, 2016).
Despite recommendations, however, the traditional and reductionist biomedical model of illness still prevails in many clinical settings, and many clinicians lack sufficient knowledge about the complex, multifactorial etiology of FSD (Kozlowska et al., 2021; Liossi and Howard, 2016; Malas et al., 2017). This outdated illness model rests on the premise that only objective findings provide a valid basis for correct knowledge about the body. This has created a sharp distinction between physical, demonstrable disease on one side, and mental, not-demonstrable illness on the other. Within this paradigm, FSD are perceived as non-specific, medically unexplained, and psychologically conditioned (Kozlowska et al., 2021; Liossi and Howard, 2016; Malas et al., 2017). However, many patients with FSD do not meet the criteria for a psychiatric diagnosis and are therefore dismissed from further follow-up in mental health services (Kozlowska et al., 2021). Thus, the patients do not find proper care neither in medical nor in mental health services. Unfortunately, many patients with FSD feel misunderstood, distrusted, and rejected in the clinical encounter with health care professionals in both medical and mental health care (Chew-Graham et al., 2017; Epstein et al., 2006; Kozlowska et al., 2021). This inhibits fruitful communication and development of a therapeutic relationship, which is an important cornerstone in all treatment (Epstein et al., 2006; Kozlowska et al., 2020; Street et al., 2009).
The culture of the biomedical paradigm seems to be tenacious and self-sustaining as it continues to permeate the knowledge and the attitudes of the clinicians, the patients, the families, and the general population, and influences the organization of the health care systems (Album et al., 2017; Kozlowska et al., 2021; Perez et al., 2021). Consequently, patients with FSD often are referred back and forth between their GP and various specialists who tend to categorize their symptoms as either disease-related or psychological, without anyone taking responsibility for obtaining a comprehensive understanding of the child’s symptoms (Gjems and Helgeland, 2018; Kozlowska et al., 2021; Malas et al., 2017). The fragmented understanding increases the risk of multiple unnecessary assessments and failed treatment (Kozlowska et al., 2021; Liossi and Howard, 2016; Malas et al., 2017). For the child and the parents, this contributes to concern, frustration, and increased consumption of health care services in the hope of receiving explanation and effective treatment (Gjems and Helgeland, 2018; Malas et al., 2017). This is unfortunate as we know that early diagnosis and treatment improves prognosis and counteracts a long-term course of FSD (Bonvanie et al., 2017). In a broader perspective, this fragmentation of health care has major societal consequences in the form of increased financial costs (Groenewald and Palermo, 2015; Liossi and Howard, 2016). Notably, the World Health Organization highlights fragmentation of health care as one of five major shortcomings of today’s healthcare services (World Health Organization, 2008).
A case formulation—A good step on the road
In order to maintain an integrative and biopsychosocial understanding, constructing a case formulation is suggested to be an important skill for clinicians treating patients with complex health conditions—such as FSD (Fayed et al., 2020; Johnstone et al., 2011; Liossi and Howard, 2016; Winters et al., 2007). Accordingly, development of case formulation abilities has now been implemented in teaching programs for clinicians (Ross et al., 2016). A case formulation is an integrative synthesis of the child’s medical history, developmental history, family history, life situation, and other relevant information from the child, caregivers, and teachers, and includes hypotheses about predisposing, triggering, maintaining, and protective factors (Fayed et al., 2020; Henderson and Martin, 2014; Johnstone et al., 2011). In children with FSD, it pays particular attention to the child’s adverse experiences and the cumulative effect of these experiences, which can be conceptualized as accumulative stress (Johnstone et al., 2011; Kozlowska et al., 2020; Liossi and Howard, 2016). Existing literature recommend that a case formulation should be collaboratively co-constructed with the young patients and their caregivers (Henderson and Martin, 2014; Johnstone et al., 2011; Liossi and Howard, 2016; Winters et al., 2007). As part of this process, the patient, parents, and clinician jointly exchange and discuss information, and explore symptoms and possible connections between symptoms and current and previous life experiences of the child and family. The emerging factors are integrated into a rich, coherent, and meaningful narrative that provides an overview of the child’s history, and produces hypotheses about predisposing, triggering, maintaining, and protective factors (Fayed et al., 2020; Henderson and Martin, 2014; Johnstone et al., 2011). Such a comprehensive understanding is, thus, a synergistic synthesis that includes the clinician’s expertise and professional knowledge, the child’s experiences, and values and preferences of the child and family (Johnstone et al., 2011). Importantly, a good formulation guides the way to a multidimensional treatment plan tailored to the individual child. However, putting theory into practice seems to be difficult. Repeatedly, in our daily clinical work, we meet clinicians who struggle to co-construct an integrative case formulation—despite thorough knowledge about the patient. Instead, they end up with a fragmented and incomplete understanding of the patient. This falls short of the holistic shared understanding that the patient, family, and clinician need. An unfortunate consequence is that many clinicians fail to deliver effective treatment strategies tailored to the individual child.
The biopsychosocial board—A conversation tool
The biopsychosocial board.
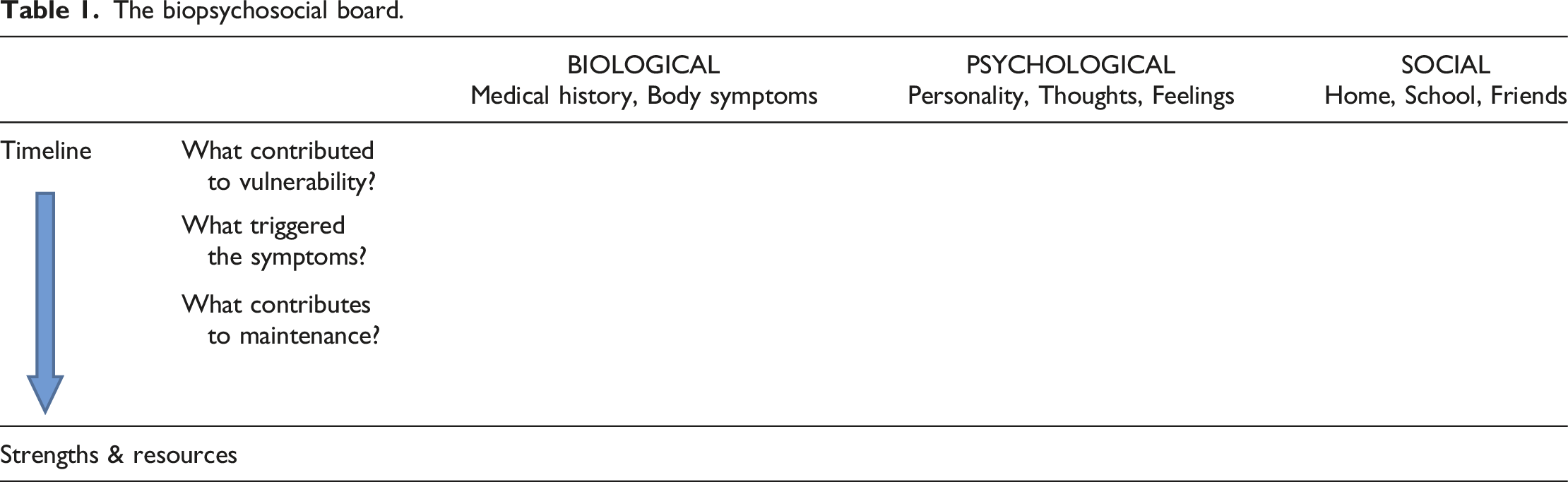
However, the board is more than just being a tool for sorting information and providing an overview. The innovative feature of the board—as we see it—is that it is an aid to promote communication and a shared, comprehensive understanding when used as a conversation tool in the clinical encounter with the patient and family. This is achieved through respectful conversation, collaboration, and joint attention aimed at filling out the board together. The therapeutic relationship that develops through this contributes to mutual trust, acceptance of the child’s symptoms and opens a broader exploration and understanding of the child’s symptoms. Used as a conversation tool, the board is of particular importance when it comes to engaging and committing the family in the collaborative process of co-constructing the case formulation of the individual child.
Engaging the family
In order to engage a family in filling out the board, it is important to start where the family is. How do they understand the child’s symptoms? Many families are more on the “biological side” of the board. For example, when a family report that a mild infection or injury triggered the child’s symptoms, this will be a natural starting point. Some families may explain a child`s symptoms by defects in the child`s immune system. This factor also belongs on the board. However, when a thorough medical assessment has not revealed anything wrong with the immune system, the family usually agree on writing a question mark behind their hypothesis. The next step can be placing, for example, the child’s long-lasting pain and sleep problems on the board, since we easily can agree on these well-known maintenance factors (Kozlowska et al., 2020). In a tempo adjusted to the family, we introduce psychosocial factors from the story they already have reported, but not included in their understanding, as potential candidates for the board. For example, a recent relocation of living, a death of a grandparent, and unaddressed family conflicts may be included, when captured by the team. Using the family`s own words, for example, “nanny” instead of grandmother, can help the family to recognize the board as “their” board. Over time, as the therapeutic relationship grows stronger, the child and the parents typically become ready to let go of some of their assumptions, and are willing to include other important factors.
In particular challenging and difficult situations, when the family disapproves or does not recognize highly relevant triggering and perpetuating factors, we experience that this conversational tool gives a particularly unique therapeutic opportunity. With the clinician’s suggestions and questions written down on the board, it represents an externalizing technique that reduces conflicts and opens for active family reflections and change processes. Disagreements within the family or between family members and clinicians can be acknowledged by writing the disputed factors or hypotheses followed by question marks or in brackets. A disputed hypothesis written on the board can also be a “silent” reminder, when the discussion of the hypothesis is put on hold for a while. A controversial hypothesis can also be erased from the board—if necessary—and later revisited when more appropriate in the conversation.
To our experience, the identification of the primary factors of critical importance becomes evident during the therapeutic process of using the board as a conversation tool. There is no shortcut in this process of distillation. The dynamics of the board assist to disclose possible factors of relevance. Thorough discussion or obtaining new information when considered necessary help to evaluate the relevancy of a certain factor. For example, when parents and teachers at first claim that bullying has been handled and therefore is part of the child`s previous history, we seldom dismiss bullying as a possible maintenance factor right away. When carefully and respectfully explored, we often experience that some children reveal ongoing subtle bullying, which needs to be addressed in order to succeed with treatment. Unfortunately, many clinicians and families jump too fast to conclusions regarding which factors to include or not in the case formulation. This can have serious consequences. Missing an important maintenance factor can make an otherwise reasonable treatment program fail.
The importance of sharing
We experience that the process of shared information and deliberation is particularly important. It brings forth new perspectives and opens for insight into not immediately available information necessary to gain a nuanced, comprehensive, and meaningful understanding of the patient’s symptoms. Interestingly, the existent research reports that a process of sharing information and reflecting together prepares the ground for well-informed choices, patient autonomy, and self-determination (Epstein, 2013; Windle et al., 2019). That the patient and family experience the treatment offered corresponding to their values and preferences has also been shown to have a positive effect on treatment adherence and outcomes (Windle et al., 2019). Furthermore, for the patient and family, an understanding of the child’s symptoms and situation can help reduce worries and stimulate good coping and treatment compliance (Kozlowska et al., 2020; Street et al., 2009; Winters et al., 2007). Below is the case study of Ann 14 years. Table 2 shows the corresponding completed board. Ann was a 14 years old girl in Secondary school living with both parents and her younger brother. She was referred to our multidisciplinary team—consisting of a pediatrician, a child and adolescent psychiatrist, a psychologist, and a physiotherapist—at our hospital for an integrative assessment of widespread pain and fatigue. When Ann and her parents met the team, they presented the following narrative: In the wake of a mild head injury 1 year ago, Ann gradually developed a mixed symptom picture with widespread pain, fatigue, dizziness, concentration problems, and sleep problems. Her functional and social disability was comprehensive. She had been out of school since the injury, had no contact with friends, and did not go to soccer practice. Until the accident, Ann had been a good, conscientious, and hardworking student. She had spent time with her friends and had been a passionate soccer player. During the last year, Ann had visited several doctors and she had been through many tests. However, the doctors did not find anything wrong and could not give her an explanation. The family felt rejected and mistrusted by the doctors, and feared that the doctors had overseen a rare disease or dangerous sequelae. Ann’s completed board. (*) Numbers in superscript help the reader to follow the timeline in Ann’s narrative.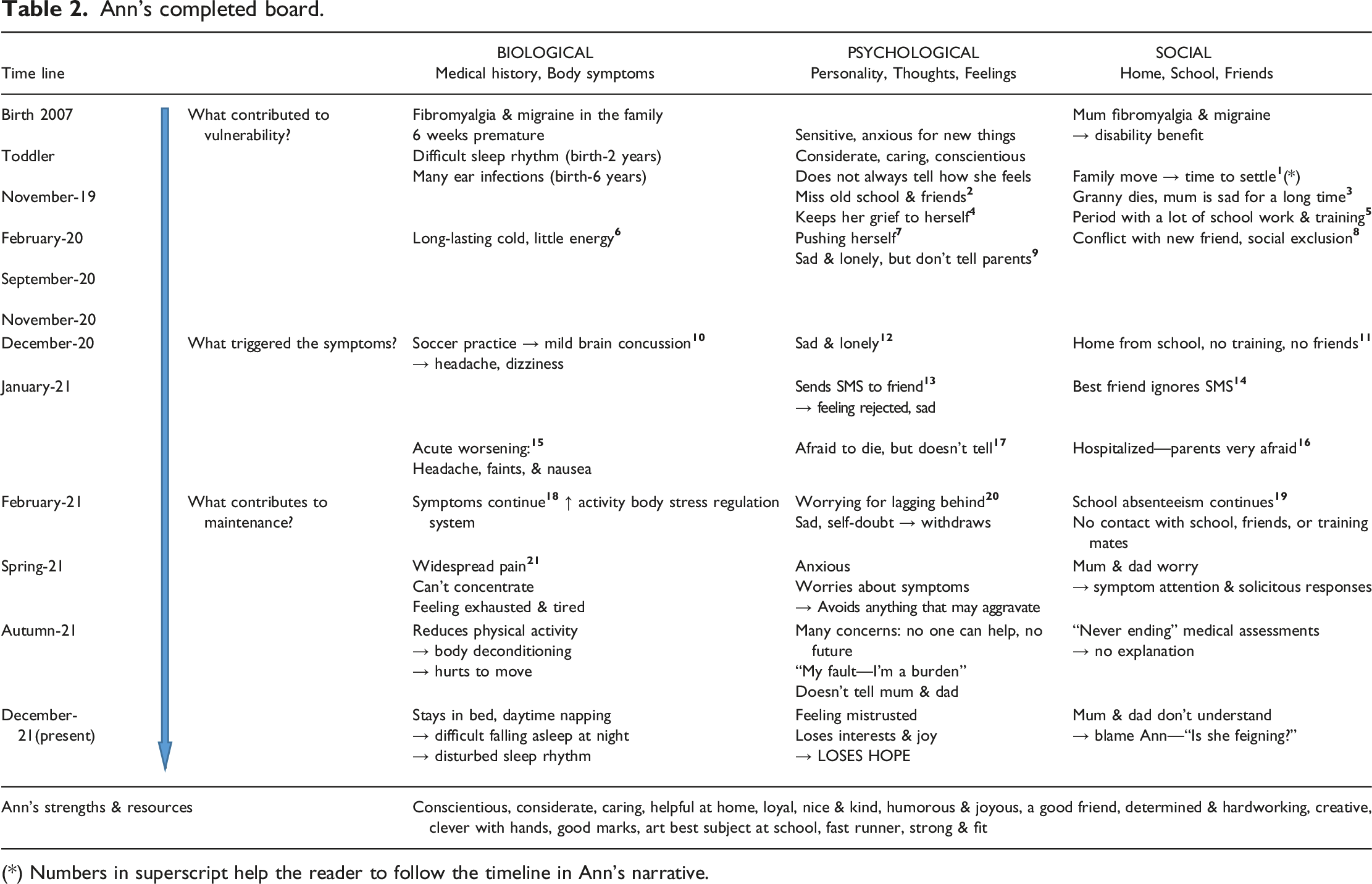
In our first meeting, we introduced Ann and her parents to the board and the biopsychosocial illness model. During the following days, we jointly explored Ann’s present situation—at home, at school, and among friends—in light of her medical history, developmental history, vulnerability factors, and previous experiences. She also underwent a professional assessment by each member of the team. Her parents participated in separate parental conversations. As Ann’s story unfolded, the team shared customized information about how the stress regulation system of the body plays an important role in the pathophysiology of FSD, and how the cumulative effect of life strain can lead to FSD.
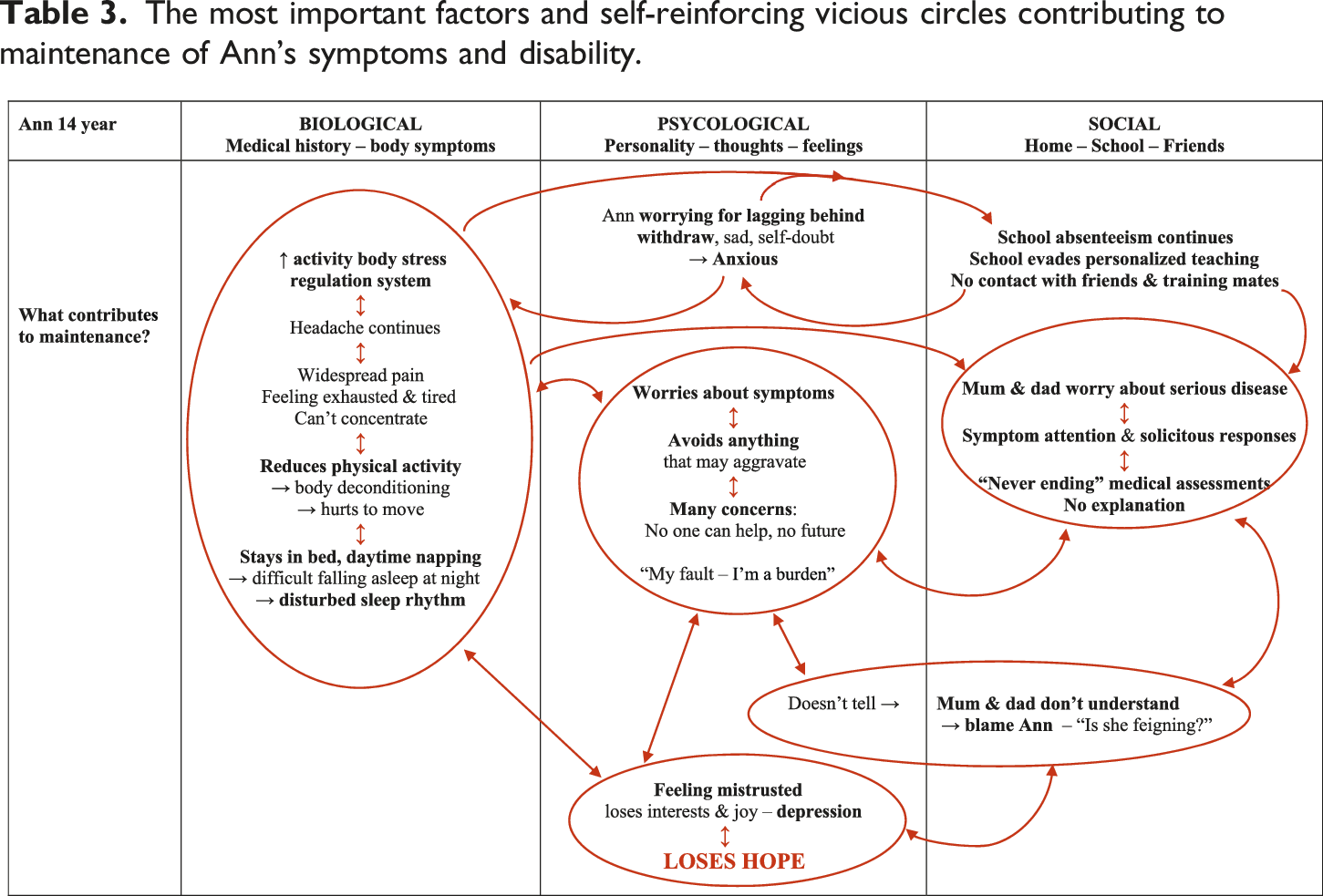
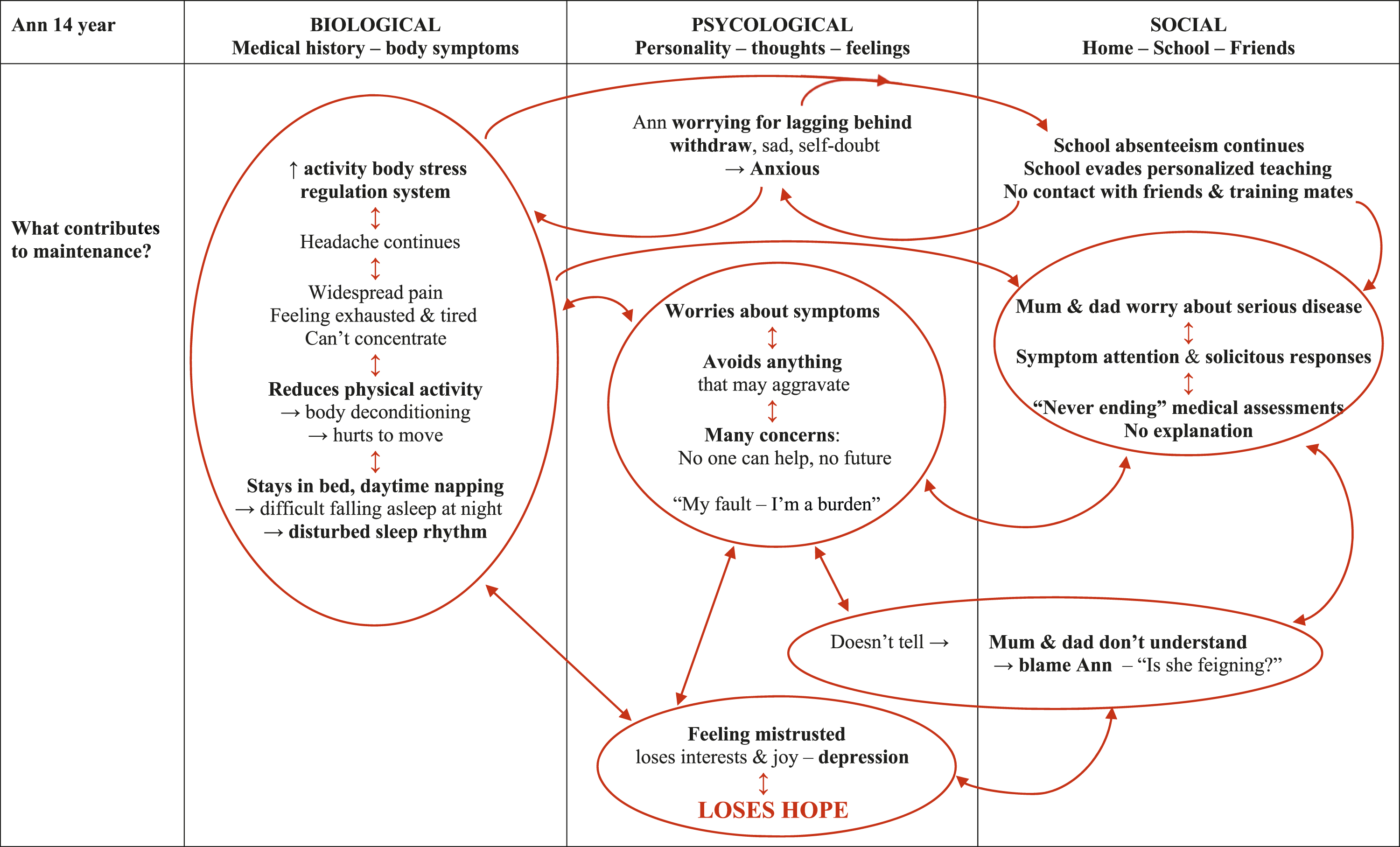
The most important factors and self-reinforcing vicious circles contributing to maintenance of Ann’s symptoms and disability.
A guide to personalized treatment
A completed and meaningful board contributes to shared insight into what the child needs—both at the individual and the system level (family, school, friends, and so on). Notwithstanding, two children with a rather similar symptom picture—for example, long-lasting, disabling abdominal pain, fatigue, and concentration problems—may need quite different treatment. A completed board visualizes the links between the individual understanding of the particular child and the corresponding treatment options. The central turning point is the joint identification and recognition of all relevant factors that contribute to maintenance of the child’s symptoms and illness behavior. Maintenance factors commonly include a unique combination of several factors. Examples can be lack of explanation, not being believed, unfortunate symptom attention, other illnesses or functional disability in the child or the parents, difficult family relationships, parents being overinvolved in their child, undiscovered learning difficulties, social anxiety, bullying, enduring school absenteeism, and so on (Elliott et al., 2020; Logan et al., 2012; Palermo et al., 2014; Walker et al., 2006). A key to good and effective treatment is to identify—jointly and systematically—the most prominent ongoing vicious circles, and next, agree on strategies for breaking them. Importantly, the intervention strategies must facilitate coping opportunities based on the resources of the child and family (Kozlowska et al., 2020, 2021). Table 3 shows the most important maintenance factors and self-reinforcing vicious circles in Ann`s history.
Hence, with this conversational tool, we enhance the likelihood of developing a personalized, multidimensional, and effective treatment plan where multiple targets for treatment can be addressed simultaneously—as needed with FSD. This is in contrast to the outdated and insufficient biomedical approach investigating one single symptom at a time: When no “cause” is identified as target for treatment, there is a return to start all over again. Unfortunately, there are countless examples of patients with FSD undergoing new, unnecessary, and potentially harmful examinations in a never-ending medical assessment—adding to the perpetuating and detrimenting vicious circles (Geist et al., 2008).
Therapeutic orientation and frameworks
In our experience, the board can be a beneficial supplement to all clinicians meeting children with FSD in their practice. Success requires that assessment and treatment targets and engages all system levels of relevance for the child’s symptoms, well-being, and functioning. Systems thinking—the holistic understanding of the child`s functioning within its different environments thinking in terms of relationships, interactions, and patterns—is therefore of crucial importance (Capra and Luisi, 2014; Kozlowska et al., 2020). Beyond this, our conversation tool is not bound to a specific therapeutic orientation, for example, cognitive behavioral therapy or systemic family therapy, or a certain method. However, for a particular child and family, systemic family therapy, or cognitive behavioral therapy, may be a pertinent and prominent part of the treatment program when in accordance with their case formulation.
Progress in scientific research within the fields of neurobiology, stress, and attachment over the last decades has brought up new knowledge that provide the biopsychosocial model with substance (Kozlowska et al., 2020). In parallel, we have evolved our conversation tool. Today, contemporary research and current models and practices inform our use of the board. In particular, our practice fits well with “The Stress-System Model for Functional Somatic Symptoms” as referred to throughout this article (Kozlowska et al., 2020). Naturally, our practice also harmonizes other relevant contemporary models and frameworks, for example, Van der Kolk’s trauma-informed model and the Power Threat Meaning (PMT) Framework (Johnstone and Boyle, 2018; Van der Kolk, 2015).
The biopsychosocial model for functional somatic disorders—applied in the clinic
In our work with children and adolescents with severe and complex FSD, we work in a multidisciplinary team within the framework of the biopsychosocial model (Engel, 1980). Informed by progress in scientific research over the last decades, we have experienced that this model becomes meaningful and clinically applicable when brought into focus using a structured, targeted, and patient-centered process—a conversation tool—integrated into clinical practice in the encounter with the individual patient and family. Used in this interactive way, we find that the board—in line with international recommendations for holistic care—has the potential to be an innovative and useful tool for broad diagnostic assessment and identification of effective treatment options tailored to the individual child and family (World Health Organization, 2008).
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.