
Abstract
Harm reduction services are empirically based strategies aimed at counteracting drug overdoses and other drug-related harms. Despite the various harms associated with heroin use as well as other drug use, the accessibility of these services varies across the United States. In this study, we explored the role honor norms might contribute to reduced support for harm reduction programs in the United States. We conducted a web-based survey of a sample of adults living in the United States (N = 376) that assessed honor norms, controllability beliefs about heroin use disorder, and support for harm reduction programs. Overall, we found higher levels of honor endorsement to be linked with lower support for harm reduction programs. Additionally, controllability beliefs explained the honor-support link for most of the harm reduction programs. Our findings suggest that acquiring public support and enacting policies for these types of services may be difficult in regions of the United States permeated with honor culture.
Introduction
In 2021, approximately 1 million people in the United States had a substance use disorder involving heroin (Substance Abuse and Mental Health Services Administration, 2022). Regular and long-term heroin use is related to a multitude of adverse outcomes. Some of these harms can be physical, such as dependence and withdrawal (Kreek et al., 2012; Swami et al., 2025), neuropsychological impairments (Ghosh et al., 2023), blood-borne and bacterial infections (associated with unsterile injection use; Lavender & McCarron, 2013), and overdose (Arteaga & Barone, 2021; Cook, 2022; Kiyatkin, 2024; White & Irvine, 1999), whereas occupational issues, financial problems, criminal setbacks, interpersonal issues, and stigmatization exemplify some of the social, psychological, and economic consequences of heroin use (Ahern et al., 2007; Moses et al., 2018). It should be noted that the following outcomes can be a consequence of other forms of drug use, and heroin is just one type of substance the United States has been combatting for the past few decades (Blanco & Volkow, 2019; Centers for Disease Control and Prevention [CDC], 2024b; Favrod-Coune & Broers, 2010).
Public health efforts have continued to search for ways to minimize the harms related to drug use, including heroin use. One such effort includes the establishment of harm reduction programs. While classifications of harm reduction vary (Vearrier, 2019), broadly defined, harm reduction refers to a variety of programs and services aimed at minimizing the negative health, social, and economic outcomes associated with substance use (e.g., overdose, illness, criminal setbacks). Some oppose government policies promoting these services, often with claims that the public should not be funding such approaches, or that individuals should have been able to prevent their substance use disorder in the first place (e.g., Sharp et al., 2020). Considering that opposition creates a barrier for funding that can help to save lives from illness and overdose (Barry et al., 2014; Barry & McGinty, 2014), it is important to investigate which specific factors might contribute to a lack of support. The current study uses theories of causal attributions, self-reliance research, and cultural frameworks to understand who may oppose these programs and why. More specifically, the study explores if norms found in the United States culture of honor, which often center around self-reliance, might contribute to negative attitudes toward harm reduction programs.
Role of Harm Reduction
In the context of substance use, the philosophy of harm reduction gained considerable traction around the 1980s in regions like the Netherlands and the United Kingdom (Burring, 1991; O’Hare, 2007). Since then, it has expanded globally as a public health model for addressing issues surrounding drug use. In contrast to many abstinence-based models and programs, the prevention or reduction of drug use is not necessarily a core component of harm reduction programs; rather, such programs seek to prevent harms at an individual’s current stage of consumption (Marlatt, 1996). Some examples of these services include syringe service programs where individuals can access sterile equipment for the consumption of drugs to avoid needle sharing, overdose prevention centers where individuals can safely inject under medical supervision, heroin maintenance which provides prescription heroin to individuals who are unresponsive to other forms of opioid agonist treatment, the decriminalization of heroin which diminishes the legal consequences for the possession of heroin, legal drug content testing sites where individuals can check drug content for dangerous mix-ins, the distribution and education of the overdose reversal medication naloxone to those most likely to witness an overdose, and Good Samaritan laws that provide immunity from criminal charges to bystanders who seek medical services for an individual experiencing an overdose (CDC, 2018; Ellis et al., 2024). Within the United States, the federal government outlines principles and provides grant funds for harm reduction services (United States Office of National Drug Control Strategy, 2022); however, policy enactment for these services are mostly regulated at the state and local levels (Lieberman et al., 2024). Despite existing evidence supporting the efficacy of these services at reducing drug-related harms (Jakubowski et al., 2018; Peiper et al., 2019; Potier et al., 2014; Rando et al., 2015; Strang et al., 2015; Wheeler et al., 2012), as well as saving taxpayer dollars on long-term chronic substance use issues (e.g., Wilson et al., 2015), disparities exist between programs in relation to their accessibility across the nation.
One relatively accessible harm reduction service is the distribution of naloxone. As of 2023, two naloxone products have been FDA-approved and are available over the counter, and all 50 states, the District of Columbia (D.C.), and Puerto Rico allow an individual (to some extent) to access the medication without a prescription. Additionally, 37 states and Washington D.C. provide a bystander who administers the medication to an individual experiencing an overdose immunity against criminal and civil charges (Legislative Analysis and Public Policy Association, 2023). Alternatively, overdose prevention centers remain one of the most restricted services in the United States. For example, currently, the city of New York contains two functioning sites, and Rhode Island is the only state in the United States that has authorized this strategy, opening its first sanctioned site in 2024 (City of New York, 2021; Project Weber/RENEW, 2024; Providence City Council, 2024; State of Rhode Island Department of Health, 2024). Other harm reduction services are moderately accessible; however, some states impose legislation that limits their functionality. For example, some states fail to exempt syringe service program participants from drug paraphernalia laws in their legislation. This permits participants within such states to be charged for the possession of syringes of drug residue (Prescription Drug Abuse Policy System, 2021). Good Samaritan laws and drug checking are also examples of services affected by similar processes (Davis, 2024; Prescription Drug Abuse Policy System, 2023).
Public opinion on harm reduction has the potential to reinforce policy enactment- especially in regions where drug use is seen as a salient issue (Bromley-Trujillo & Poe, 2018; Burstein, 2003; Lax & Phillips, 2012). This can be seen with Oregon’s Ballot Measure 110 which permitted state voters to vote directly for or against a drug law reform. Measure 110 made two major revisions to previous drug law by decriminalizing the possession of illegal drugs and redirecting criminal enforcement costs for drug possession to fund treatment and recovery programs for drug use. After approximately 58% of voters indicated their approval for the law in November of 2020, the law later came into effect February 1, 2021 (Lantz & Nieubuurt, 2020). Such opportunities further emphasize the importance public opinion has on policy adoption.
Although this is just one example indicating public support impacting policy for a harm reduction program, research reveals that public opinion on harm reduction within the United States varies greatly. Some studies reveal general support for these services (Hanson et al., 2024; Kulesza et al., 2015) while others indicate an overall lack of support (McGinty et al., 2018). Considering the varied results across the empirical work (Jakubowski et al., 2018; Peiper et al., 2019; Potier et al., 2014; Rando et al., 2015; Strang et al., 2015; Wheeler et al., 2012), these inconsistent findings suggest there may be important barriers at play that are impacting public support. In fact, many researchers have taken steps attempting to identify such barriers. Factors identified as predicting lower support for harm reduction policies include demographic factors, like political conservatism, higher religiosity, older age, and being male (Andraka-Cristou et al., 2022; McGinty et al., 2018; Sylvester et al., 2022). Importantly, stigma surrounding opioid use disorder (OUD) is also found to be a predictor. OUD stigma is related to the belief that an individual deserves to be punished for their disorder (Hanson et al., 2024; Kulesza et al., 2015; McGinty et al., 2018). It should be noted that OUD stigma can be explained clearly by Weiner et al.’s Attribution Theory (1988), which proposes that helping behavior can be influenced by an individual’s assumption about the cause and controllability of a condition. Various studies within the mental health literature indicate that individuals with a substance use disorder, compared to other health conditions, are seen as being more responsible for their condition. Consequently, individuals are less willing to help an individual using drugs (Corrigan et al., 2000, 2003, 2009). A recent study found similar outcomes, in that many participants believed individuals developed an OUD because they “lacked self-control” (Taylor et al., 2021). While the following studies address OUD holistically and do not explicitly distinguish between the different types of opioids (e.g., opiates, prescription opioids, synthetic opioids, semi-synthetic opioids) some evidence indicates that the following process may be even more pronounced for illegally obtained opioids like heroin (Weeks & Strenstrom, 2020).
Self-Reliance and Controllability Beliefs
Weiner et al.’s (1988) attribution model places great importance on controllability beliefs (i.e., a person should be able to control their substance use) in influencing support for various policies. Related work has found that these controllability beliefs may find their roots in people’s own beliefs about self-reliance. In other words, if individuals believe that they themselves should be self-reliant, they may project this belief onto stigmatized identities. It is already known that individuals higher in self-reliance beliefs tend to be more judgmental of their own mental wellbeing (Choo & Marzsalek, 2019), often avoiding services due to beliefs about self-reliance (Choi et al., 2024), and that they hold higher levels of stigma due to beliefs on the “immutability” of mental illnesses (Hantzi et al., 2019). Self-reliance beliefs are also linked with higher levels of mental illness stigma (Keller & Owens, 2022), with qualitative work suggesting that this link is due to beliefs about controllability of mental illness. For example, in a qualitative study on first responder views of people who use drugs (PWUD), Ezell et al. (2021) found that many respondents believed PWUD can control the situation by “picking yourself by the bootstraps.” One respondent even noted, “I just don’t see how life would ever be that bad. To me, it’s just simple; quit doing drugs, clean up your act, get a job,” suggesting a belief that individuals should be able to fix their condition with a few “easy” steps. In Trang et al. (2021), respondents experiencing drug use noted that many of their peers and family had simply told them to fix the problem themselves; one respondent commented, “My siblings said I needed to look after myself, to save myself, that no one could save me and that each person had her own life… Of course, I know this, but sometimes [I feel sad]… They have their family, and I have no one.” Unfortunately, these public attitudes become internalized in PWUD, which can subsequently increase the likelihood of overdose (e.g., Sibley et al., 2024). Overall, controllability beliefs and self-reliance contribute to the high levels of stigma toward PWUD (Sumnall et al., 2021). Collectively, this suggests that individuals who place stronger emphasis on self-reliance might be less likely to support harm reduction programs due to beliefs they have about PWUD.
Culture of Honor, Self-Reliance, and Stigma
The associations among norms of self-reliance, perceptions of substance use disorder, and support for harm reduction programs are likely to be prominent in cultures of honor. Within such cultures, the defense and maintenance of one’s reputation is of utmost importance (Brown, 2016; Nisbett & Cohen, 1996; Uskul & Cross, 2020). While it should be noted that honor cultures are found in various regions around the world (e.g., the Middle East, the Mediterranean), the United States culture of honor are predominately located in southern and western states which is largely due to the migration patterns of Scots-Irish settlers within the nation during the 18th and 19th centuries (Brown, 2016; Fischer, 1989; Lopez et al., 2024). Cultures of honor arise in socioecologies characterized by lawlessness or insecurity (Uskul & Cross, 2020) and, consequently, individuals (particularly men) are responsible for defending themselves against social threats. Further, the norms governing how honor is conferred and maintained are highly gendered. For example, men are prescribed to be strong, brave, and to have an intolerance for disrespect which is a vital component to honor cultures since it serves as a deterrence for exploitation (Cohen & Nisbett, 1994; Fischer, 1989). Although not traditionally viewed to be defenders of the family, it is equally as important for women in cultures of honor to uphold reputations of sexual purity and fidelity given that survival of the family is interdependent, and that one’s disreputable behavior can compromise protection by tarnishing the family’s honor (Mosquera, 2011; Rodriguez Mosquera, 2016; Vandello & Cohen, 2003). Importantly, researchers have often examined the extent to which individuals endorse these honor-related norms and values (henceforth, honor endorsement) in predicting many important outcomes. Because the endorsement of honor norms is akin to one’s belief in the cultural ideology of honor, it is unsurprising that men and women endorse honor-related gender norms and general honor concerns to a similar extent (Bock et al., 2024; Guerra et al., 2013).
Much of the early literature examining cultures honor highlights honor endorsers’ heightened sensitivity to reputational threats and portrays the emphasis on self-reliance as manifesting through violent reputation defense (Uskul et al., 2019) however, recent evidence suggests a broader application of self-reliance outside of violence and aggression. For example, evidence indicates honor endorsers are more likely to associate mental health help-seeking with a sign of weakness (Brown et al., 2014). Consequently, honor endorsers are less willing to seek professional mental health services (Foster et al., 2021), contributing to higher rates of suicide in these regions (Bock et al., 2023; Lopez et al., 2024; Osterman & Brown, 2011; Roberts et al., 2019). Recent work has shown that honor endorsers even avoid expressing their emotions to be seen as more self-reliant and able to self-regulate (Foster et al., 2022). Furthermore, results from a study examining honor values, self-reliance, and adherence to governmental COVID-19 protocol (e.g., wearing face masks, getting vaccinated, and practicing social distancing; CDC, 2024a) indicated that many honor endorsers avoided adhering to government protocol because they felt they should handle the pandemic themselves instead of relying on government recommendations (Wang et al., 2021). The relationship found by Wang and colleagues suggests that honor endorsers believe that an individual is either capable of choosing what actions to take to protect oneself or capable of dealing with the potential ramifications of inaction without the need for government intervention. These findings, alongside the frequent indication of self-reliance as a core tenet of honor norms (Brown & Osterman, 2012), imply self-reliance beliefs feeding into negative attitudes toward certain harm reduction programs.
Present Research
Based on Weiner et al.’s (1988) attribution theory and other supporting research, we know that controllability beliefs about drug use can influence helping behavior (Corrigan et al., 2000, 2003, 2009). Additionally, we know that self-reliance is a key feature for coping with problems or situations that are deemed controllable by the individual (Sniderman & Brody, 1977). Therefore, we have reason to believe that when an individual views drug use as controllable, they are more likely to see PWUD, such as those using heroin, as responsible for coping with their condition and less likely to support government interventions, such as harm reduction programs. Furthermore, because honor endorsement is associated with beliefs about the importance of self-reliance (Foster & Bock, 2024a; Roberts et al., 2019; Wang et al., 2021), we propose that they may be less likely to support harm reduction programs. In the present study, we examined the relationships among honor endorsement, controllability beliefs about substance use disorder involving heroin, and support for various harm reduction programs. While there are other forms of opioid use which are certainly worth discussing, this current study focuses on heroin use as this type of substance use has been identified as the downstream outcome emerging from prescription opioid use which has created the modern “opioid crisis” (Cicero et al., 2014). With this in mind, we hypothesized that individuals scoring higher in honor endorsement would exhibit lower support for harm reduction programs (Hypothesis 1). Moreover, we hypothesized that the link between honor endorsement and harm reduction program support would be explained by higher controllability beliefs about heroin use (Hypothesis 2). We also sought to explore if these pathways varied between men and women, considering the mixed findings regarding gender differences in honor outcomes found in prior work (e.g., Ceylan-Batur et al., 2023; Novin et al., 2015).
Method
Participants
Participants were 373 individuals (184 identified as male, 181 identified as female, 7 identified as nonbinary, 1 cell was missing) collected via Prolific, an online data collection platform. Participants were approximately 38 years of age (M = 38.47, SD = 13.03; Range 18–76) and predominately white, non-LatinX (75.6%)—the remainder of the participants identified as African American (7.5%), Asian (7.2%), LatinX/Hispanic (5.9%), Middle Eastern (0.8%) or “Other” (2.9%). Over one third of participants (37.1%) reported knowing someone who either has an opiate addiction or had died/overdosed from opiates. The study received IRB approval from [anonymized for review] (IRB Approval # = Foster & Bock, 2024a). Data are available upon reasonable request from the first author.
Measures
Honor Endorsement
To assess endorsement of honor norms, we administered three commonly used scales. These included the 16-item Honor Ideology for Manhood Scale (HIM; Barnes et al., 2012; α = .95; M = 3.19, SD = 1.39) which encapsulates the endorsement of the masculine facet of honor by assessing support for retributive aggression upon receiving a reputation threat (e.g., “A man has the right to act with physical aggression toward another man who insults his mother”) and the desirable characteristics that comprise a “real man” (e.g., “A real man doesn’t let other people push him around”); the 12-item Honor Ideology for Womanhood Scale (HIW; Barnes et al., 2014; α = .94; M = 3.91, SD = 1.49) which assesses the feminine facet of honor by capturing concerns regarding sexual purity and loyalty to one’s spouse and family (e.g., “A respectable woman never wants to be known as sexually permissive”, “A respectable woman knows that what she does reflects on her family name”); and the 9-item Honor Concern scale (HC; IJzerman et al., 2007; α = .88; M = 3.82, SD = 1.23) which assesses general endorsement of honor norms (e.g., “I think that honor is one of the most important things that I have as a human being”). Participants responded to each item using a scale from 1 (Strongly Disagree) to 7 (Strongly Agree). Consistent with prior work (e.g., Barnes et al., 2014; Bock et al., 2024; Foster et al., 2024b), we sought to validate the use of a latent honor factor by conducting a factor analysis using principal axis factoring as the extraction method with the three honor scales as indicators. A single dominant factor emerged (eigenvalue = 2.21) explaining 63.23% of the variability in the honor scales. Scores were saved using the regression method and the subsequent honor factor scores served as the honor measure for bivariate statistics. As the honor factor scores are essentially standardized values, factor scores have a mean of 0 and standard deviation of 1, with units being represented in standard deviations. 1
Controllability Beliefs
Two items were used to assess beliefs about the controllability of heroin use (“People who use heroin made a decision to become addicted to heroin” and “People have complete control over whether or not they become addicted to heroin”; α = .80). Participants responded to each item using a scale from 1 (Strongly Disagree) to 7 (Strongly Agree). These scores were averaged to create a single controllability beliefs score.
Harm Reduction Program Support
Participants indicated their support for harm reduction programs after receiving the following prompt:
Many people have different ideas about how we should deal with opioid/heroin addiction issues in this country. One set of ideas come from harm-reduction techniques, intended to play a role in preventing drug-related deaths by offering access to healthcare, social services, and treatment. To what extent would you support the following policies regarding harm reduction for opiates/heroin?
Using a scale from 1 (little to no support) to 7 (strong support), participants responded to prompts for needle and syringe distribution to those who use drugs (to avoid needle-sharing), sites where individuals can safely inject under medical supervision, heroin maintenance (prescription of heroin to those who do not do well with other treatments), decriminalization of heroin (e.g., possessing small amounts does not cause jail/prison time), legal drug content testing (e.g., sites where to check drug content for dangerous mix-ins before using), and Good Samaritan laws (e.g., no criminal prosecution for assisting someone who needs emergency medical help during an opioid overdose). They also received a prompt for Narcan:
One other aspect of dealing with heroin use is the use of NARCAN/naloxone, a drug which is nasally administered by paramedics/medical technicians to reverse the effects of opiate drug overdose. To what extent would you support programs for the administering of NARCAN/naloxone to individuals who have overdosed?
The items did share considerable overlap (α = .89) but were treated as distinct outcomes in the main analyses.
Covariates
As covariates, we used participants’ age, participants’ sex (0 = female, 1 = male), and knowing someone with an opiate addiction (0 = no, 1 = yes). We also collected political affiliation on a scale from 1 (extremely liberal) to 7 (extremely conservative) given well-known links between conservatism and both opioid use stigma and decreased support for governmental social programs (Reynolds et al., 2022; Skitka & Tetlock, 1993).
Results
Descriptive and Bivariate Statistics
Bivariate Correlations and Descriptive Statistics for Variables of Interest
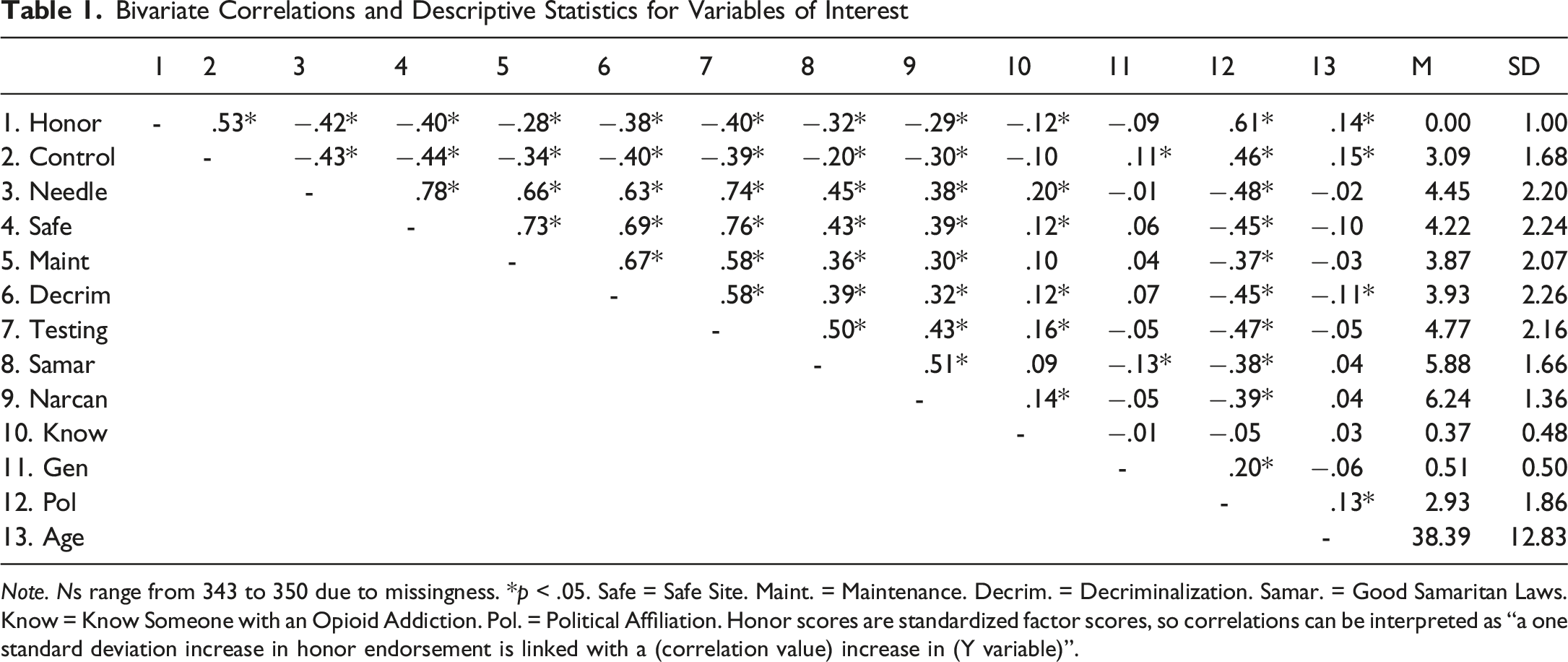
Note. Ns range from 343 to 350 due to missingness. *p < .05. Safe = Safe Site. Maint. = Maintenance. Decrim. = Decriminalization. Samar. = Good Samaritan Laws. Know = Know Someone with an Opioid Addiction. Pol. = Political Affiliation. Honor scores are standardized factor scores, so correlations can be interpreted as “a one standard deviation increase in honor endorsement is linked with a (correlation value) increase in (Y variable)”.
A measurement model was estimated in MPlus, which showed good fit to the data [ꭓ2 (23) = 53.64, p < .05, CFI = .987, TLI = .945, RMSEA = .062 [.040, .083], SRMR = .020]. The model was then run to test for significance of the indirect effects from latent honor to each of the outcomes through controllability beliefs. Standardized estimates showed significant effects for the needle sharing outcome (Mediated Effect—ME = −.09, 95% CI [-0.14, −0.03]), the safe site outcome (ME = −.11, 95% CI [−0.17, −0.05]), the drug maintenance outcome (ME = −.09, 95% CI [−0.15, −0.03]), the decriminalization outcome (ME = −.08, 95% CI [−0.14, −0.03]), the drug testing program outcome (ME = −.07, 95% CI [−0.12, −0.01], p = .016), and the Narcan outcome (ME = −.07, 95% CI [−0.13, −0.01]). The effect for Good Samaritan laws was not significant (ME = .02, 95% CI [−0.04, 0.08]).
Next, indirect effects were tested using the MODEL CONSTRAINT function in MPlus. This approach constrains indirect effects to be equal across male and female subgroups
2
, in this case, and a significant Wald test would indicate the indirect effects are significantly different from each other. No significant differences emerged for the needle sharing indirect effect (Wald = 1.59, p = .207), the safe site indirect effect (Wald = 0.01, p = .923), the drug maintenance indirect effect (Wald = 0.89, p = .346), the decriminalization indirect effect (Wald = 1.39, p = .238), or the drug testing indirect effect (Wald = 0.001, p = .984). The nonsignificant Good Samaritan indirect effect was nonsignificant across both groups as well (Wald = 2.03, p = .154). There was a significant difference for the Narcan outcome (Wald = 6.01, p = .014), such that the indirect effect was significant for females in the sample (ME = −.23, p = .005), but not for males (ME = .05, p = .518). The final model can be found in Figure 1.
3
Final Model Testing Indirect Effects From Latent Honor to HRP Support Outcomes Through Controllability Beliefs.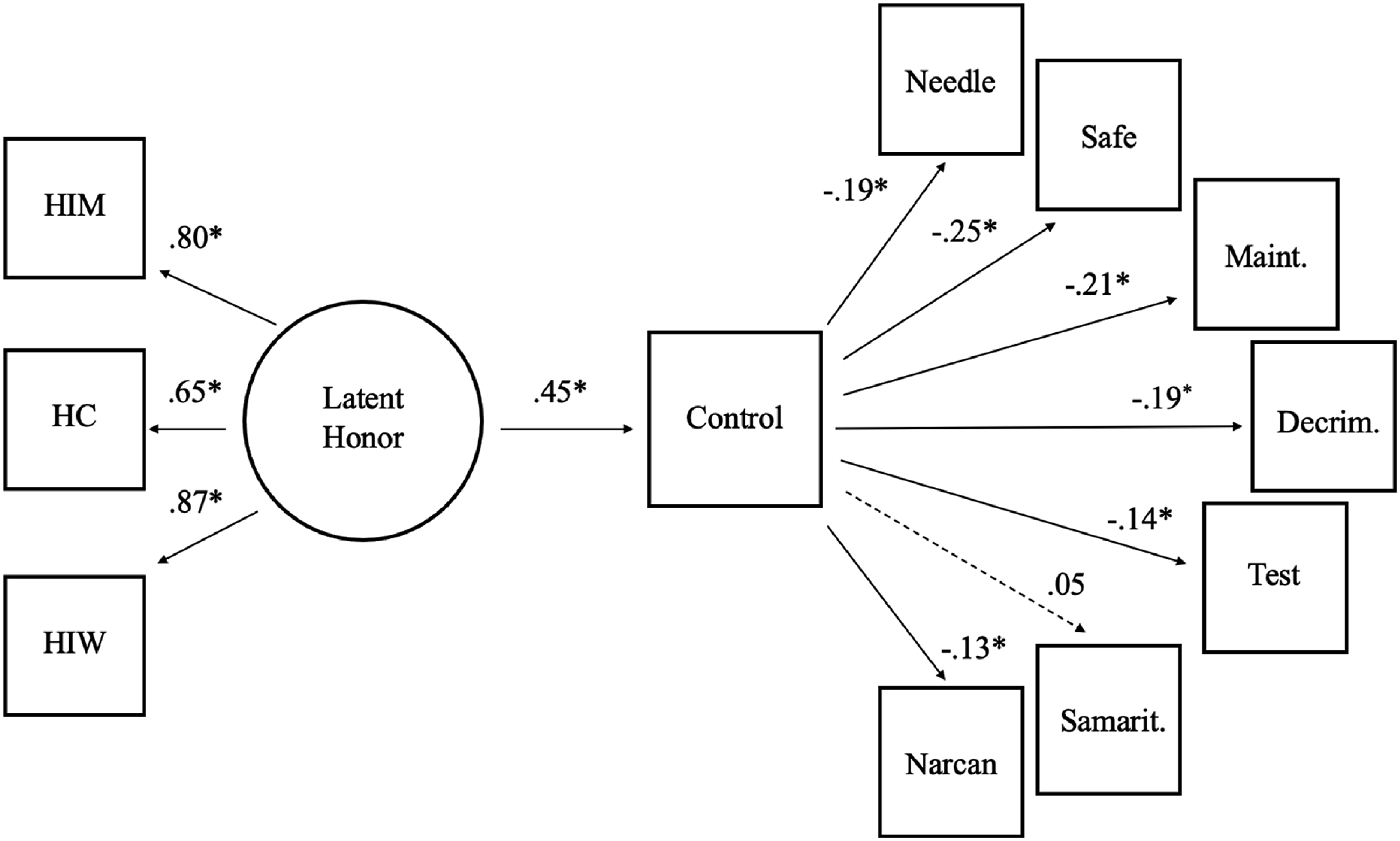
Discussion
The current study, to our knowledge, is the first to examine the relationship between honor endorsement and support for harm reduction programs within the United States. Supporting our first hypothesis, we found higher levels of honor endorsement to be negatively associated with support for harm reduction programs. Although further research is required in this area, this finding can be of importance to policy makers and harm reduction advocates. As previously noted, public opinion has the potential to shape election outcomes and policy enactment (Burstein, 2003), and assuming indicated attitudes of heroin use and harm reduction would accurately translate into voting behavior and monetary support, our findings suggest that acquiring public funding and establishing policies or electing officials that endorse these services may be especially difficult in honor-oriented regions of the United States (i.e., southern and western regions; Lopez et al., 2024). Within these regions, lack of support for harm reduction programs can be especially injurious to PWUD due to other economic, physical, and social conditions that can further inflate drug-related harms. For example, although regions where honor values are highly endorsed are not limited to rural areas, in general, they tend to share overlapping characteristics with rurality such as limited access to healthcare resources (e.g., Barnes et al., 2012; Crowder & Kemmelmeier, 2014), and higher levels of economic precariousness (Lopez et al., 2024; Nisbett & Cohen, 1996) which shape the risk-environment for opioid-related harms (Thomas et al., 2020). Without access to proper treatment or preemptive measures like harm reduction, drug use has the potential to be prolonged, thus exacerbating the risk for drug-related harms within these regions (Rigg et al., 2018). Future research should extend investigation into the regional level by comparing harm reduction program accessibility and drug-related mortalities within honor states to those of non-honor states.
In support of our second hypothesis, we found that significant indirect effects from the endorsement of honor norms through heroin controllability beliefs to lower support for the following services: syringe service programs, overdose prevention centers, heroin maintenance, decriminalization of heroin, drug-testing programs, and naloxone distribution programs. Not only does our data suggest that those strongly endorsing honor norms are likely projecting self-reliance beliefs onto people who use heroin which is consequently inhibiting their support for programs aiding these individuals, but it may also indicate their disposition for self-stigmatization in the context of heroin use. In other words, those strongly endorsing honor values who are experiencing substance use may be more reticent to seeking out harm reduction programs, and perhaps treatment programs in general, based on their personal beliefs that heroin use is controllable. Such a mindset that could subsequentially result in this population experiencing heightened rates of heroin-related mortality. The following proposition is plausible considering similar process occurs in relation to mental health help-seeking (Bock et al., 2023; Brown et al., 2014; Foster et al., 2021), and future research should take steps to delineate this relationship at both the state and individual levels. Additionally, our findings may be of importance for the design of future interventions as previous research indicates message framing can impact people’s perceptions of harm reduction (Bachhuber et al., 2015; McGinty et al., 2023; Sumnall et al., 2023). Perhaps designing these programs in a way that targets controllability beliefs about substance use disorders, and heroin use specifically, would be efficacious at increasing support for these services. For this study, we proposed a link would be found between honor endorsement and controllability beliefs based on the conception that a relationship exists between views on self-reliance and controllability beliefs about a condition (Cook & Brownstein 2019; Sniderman & Brody, 1977; Wang et al., 2021); however, to our knowledge, this relationship has not been directly examined in honor culture research up to this point. Future research should investigate the extent to which this relationship exists as it may provide further insight into approaches for intervention implementation.
Interestingly, we found that individuals exhibiting greater levels of honor endorsement who viewed substance use involving heroin as controllable were not less likely to support Good Samaritan laws compared to their counterparts. This finding aligns with other harm reduction research that indicates these services to be highly supported relative to other strategies (Andraka-Christou et al., 2022). This disparity could result from these services potentially being seen as directly benefiting bystanders who provide help during an overdose rather than the person experiencing an overdose, thus shifting the focus of the policy away from a stigmatized identity like PWUD (Olsen & Sharfstein, 2014).
When testing for moderation of the indirect effect pathways by participant sex, most interaction effects remained nonsignificant. We did, however, find a significant difference between males and females for the Narcan outcome in our study. In this case, higher levels of honor endorsement predicted lower support for this service through controllability beliefs for women; however, this effect did not emerge for males in our sample. This is of particular interest for a few reasons. First, it suggests that there may be gender-specific concerns which are reflected in support for Narcan policies. Considering that substance use is often viewed as a “male” disorder (e.g., Uziel-Miller & Dresner, 2002), it is possible that men were more likely to have a sense of connection or empathy when thinking of individuals who were overdosing and in need of Narcan. Of course, it is also possible that this was merely a statistical artifact. Overall, it is an intriguing finding which must be explored in future work on support for Narcan programs.
Limitations
This current study is not without limitations, and its results should be interpreted with caution. First, the generalizability of our findings is limited given that our participants were recruited using an online data collection platform. Other sample characteristics, such that the sample consisted only of United States residents and that much of our sample identified as politically liberal, further limits interpretation. The former characteristic may be especially vital when attempting to generalize findings among cultures of honor as cultural differences in self-reliance values may impact findings among honor endorsers in other regions of the world (Guerra et al., 2013; Sev’er & Yurdakul, 2001; Wang et al., 2021). Although we did statistically control for political affiliation in the current analysis, one might consider that, because conservatism is linked with lower support for government funded programs like HRPs, finding effects in a relatively liberal sample strengthens the current findings even more. Regardless, one might consider exploring these effects in heavily conservative samples, at least for a comparison to the effects in this sample.
In addition to these limitations, future research should account for other demographic characteristics (e.g., education level, socio-economic status, marital status, etc.) of the sample that may influence our findings—online convenience samples are somewhat limited in demographic diversity, although Prolific tends to perform relatively well in terms of data quality (Douglas et al., 2023). Community samples and non-convenience approaches would be helpful when replicating the existing work. Second, data were collected on a self-report basis. There is the potential that indicated values do not actually reflect how an individual truly feels towards a topic. Third, although we attempted to focus on controllability beliefs surrounding heroin for this study, the brief use of other terms in our survey, such as “opioid” and “opiate”, may have shifted participants’ thoughts away from this specific substance. Caution should be taken when attempting to apply these results only to heroin use, and future iterations of this study should avoid interchanging terms to minimize conflation. Fourth, any implications of this study are under the impression that indicated attitudes towards heroin use and harm reduction services would translate via voting behavior and public funding (e.g., individuals indicating a decreased support for harm reduction, when presented the opportunity, would vote against policy or government officials endorsing these services as well as refuse to fund these services); however, we cannot be certain this is always the case, and future work should extend these findings into applied policy areas.
Conclusion
The role of this study was to identify the role honor plays in harm reduction program support. We based our investigation on prior research suggesting a relation between self-reliance and controllability beliefs about health conditions. Results indicated that greater levels of honor endorsement were related to lower policy support, and this relationship could be explained by believing OUD involving heroin to be a controllable condition. Despite a few limitations, our study further adds to both the harm reduction and honor culture literature. Investigating the impact controllability belief interventions may have on support for harm reduction, especially in states where honor culture is prevalent, is recommended as a necessary future direction.
Footnotes
Ethical Considerations
The current study received ethical approval via the main author’s IRB at Penn State University, United States of America (IRB # STUDY00022668).
Consent to Participate
As this project was indicated for exempt review by the IRB, all participants completed an implied consent document per APA ethical guidelines.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.