
Abstract
Opioid-related overdose deaths have risen sharply in rural areas of the United States during the past decade. Intranasal naloxone (IN) can reverse the effects of opioid overdose if given promptly. However, access to IN is often hampered by cost, availability, and stigma. Dispensing IN in vending machines (VMs) offers a means of addressing these barriers and increasing the availability of this form of overdose prevention for the general public in rural communities. From September 2022 to December 2024, the University of Vermont Center on Rural Addiction undertook a descriptive exploratory multi-site intranasal naloxone vending machine (INVM) implementation project, partnering with five organizations in underserved rural areas throughout northern New England. In this report, we describe our stepwise approach to site selection, machine design and installation, community relations, and data collection and monitoring that we developed to facilitate program implementation. Monthly total IN doses dispensed per machine typically peaked in the first month after installation (mean 131; range 44–226) and subsequently averaged 47 (range 10–98) doses per month, with 19.3% of doses dispensed on weekends, and 49.5% occurring outside of business hours. Concerns voiced by rural community members in response to the anticipated placement of a VM were addressed by engagement with stakeholders and communication of facts about IN. Overall, these results suggest that VM-based naloxone distribution is feasible in rural communities and holds substantial potential for addressing opioid-related harm in these hard-hit areas.
Keywords
Introduction
Harm reduction is an effective, evidence-based set of practical strategies and ideas aimed at reducing the harms associated with drug use, employed without judgment, stigma, or discrimination (Denning & Little, 2017; Marlatt et al., 2011; Substance Abuse and Mental Health Services Administration, 2023). This is distinct from but complementary to treatment, and entails using strategies to minimize negative consequences of drug use, while neither requiring nor discouraging abstinence (Denning & Little, 2017; Marlatt et al., 2011; Substance Abuse and Mental Health Services Administration, 2023). A core tenet of harm reduction is to design interventions and policies that address specific individual and community needs, in order to “meet them where they are” (Marlatt et al., 2011). For practical impact, this includes ensuring that overdose prevention resources are offered in physical locations where people can access them, during times when people are available to receive them, and with minimal barriers to utilization.
Naloxone is a µ-opioid receptor antagonist used to reverse the effects of opioid overdose, such as respiratory depression (Saari et al., 2024). Intranasal naloxone (IN) HCl is designed to be absorbed through the nasal mucous membranes for rapid receptor site access (Foldes et al., 1969), and can be administered by laypeople. The U.S. Food and Drug Administration approved IN by prescription in November 2015, and then approved over-the-counter availability in March, 2023, thereby making opioid overdose reversal medication more accessible for community use (Food and Drug Administration, 2024).
Vending machines (VMs) have recently gained traction in the United States for distributing overdose prevention supplies, including IN (Allen et al., 2022; Arendt, 2023; Kerr et al., 2022; McDonald, 2009; Russell et al., 2023; Zhang et al., 2025). Intranasal naloxone vending machines (INVMs) differ from traditional VMs only in the product dispensed. Multiple studies have found that making IN available through a VM (INVM) can lessen health disparities among populations that are financially distressed or have fewer connections to social services (Allen et al., 2022; Arendt, 2023; Russell et al., 2023), may be associated with an increase in harm reduction service utilization (Kerr et al., 2022), and can translate to a decrease in opioid-involved overdose fatalities (Allen et al., 2022).
To date, the literature on INVMs has primarily focused on implementation in urban areas (Allen et al., 2022; Arendt, 2023; Kerr et al., 2022; Russell et al., 2023; Stewart et al., 2023). However, there is a pressing need in the United States for rural overdose prevention efforts. From 1999 to 2019, the U.S. national overdose death rate increased by >400% (from 6.04 per 100,000 to 28.2 per 100,000 persons; Centers for Disease Control and Prevention, 2022; Hedegaard & Spencer, 2021). During that period, the overdose death rate increased faster in rural counties (average annual increases of 4%–20%) than in urban counties (3%–17%), largely attributable to synthetic and semi-synthetic opioids (Hedegaard et al., 2019; Parker et al., 2023). Despite the effects of the opioid epidemic on rural communities, disproportionate barriers exist for rural individuals in need of overdose prevention resources and substance use disorder (SUD) treatment. Rural barriers occur at multiple levels, including planning and funding (Parker et al., 2023); healthcare provider availability and capacity (MacDougal et al., 2024; MacDowell et al., 2010); public health surveillance efforts (Parker et al., 2023); stigma amongst providers, community members, and patients (Dunn et al., 2016); and public education and awareness (Franz et al., 2021). Placing INVMs at rural community sites represents an opportunity to extend potentially lifesaving overdose prevention resources in a low-barrier manner to underserved individuals, and connect them to additional education, treatment, and recovery services (Substance Abuse and Mental Health Services Administration, 2023).
The University of Vermont Center on Rural Addiction (UVM CORA) was established in 2019 by the Health Resources and Services Administration (HRSA), with a mission to identify, translate, and disseminate evidence-based treatment for opioid use disorder in rural communities in northern New England. Beginning in 2022, UVM CORA undertook a descriptive exploratory multi-site INVM implementation project in partnership with five rural organizations in northern New England. UVM CORA provided HRSA grant subaward funds to the selected organizations to purchase the INVMs, supplied each organization with enough IN to fill each machine twice, offered technical support throughout planning and implementation, and covered other related costs for the first 2 years. After this initial 2-year implementation period, organizations were expected to operate and maintain the machines independently. To our knowledge, there were no publicly accessible INVMs in these states prior to this effort. This article reports our stepwise approach to the placement and monitoring of these machines for rural use. Our goal was to assess feasibility of implementation at these diverse rural sites and determine if the INVMs could indeed be installed, used, and accepted by the community. In addition, we considered after-hours use of the INVM an indicator of success. The efforts described in this article were deemed not research by the institutional review board of the University of Vermont.
Methods
Project planning began in Fall 2022. We consulted existing literature (reviewed above) and aligned our approach with previous publications. We predicted that the circumstances of each environment would differ, and the process would involve close collaboration with each organization to meet the needs of their community. While maintaining flexibility, we structured our approach into four general phases: organization selection; machine design, installation, and upkeep; community relations; and data collection. We describe each of these below.
Organization Selection
To identify optimal rural organizations for INVM implementation, in February 2023 we announced the opportunity via the UVM CORA listserv, website, social media, and the Federal Office of Rural Health Policy weekly newsletter, seeking community organizations in rural northern New England interested in applying to receive a machine through partnership with UVM CORA. Eligibility criteria reflected our center’s mission, funder priorities, and University of Vermont’s requirements for subaward contracts: (a) non-profit organization licensed to conduct business, (b) located in a non-metropolitan county in northern New England that HRSA designates as rural (Rural Health Grants Eligibility Analyzer, 2024), (c) experienced with harm reduction principles and practices, (d) documentation of sustainable staffing and funding to support the continued independent operation of the machine beyond the period of UVM CORA support, and (e) commitment to sharing their INVM utilization data with UVM CORA. We asked interested organizations to complete an application that we developed to assess organization eligibility and characteristics (Russell et al., 2023) favorable to the implementation and continued operation of an INVM (see Table 1).
Considerations When Screening Candidate Sites for an INVM.
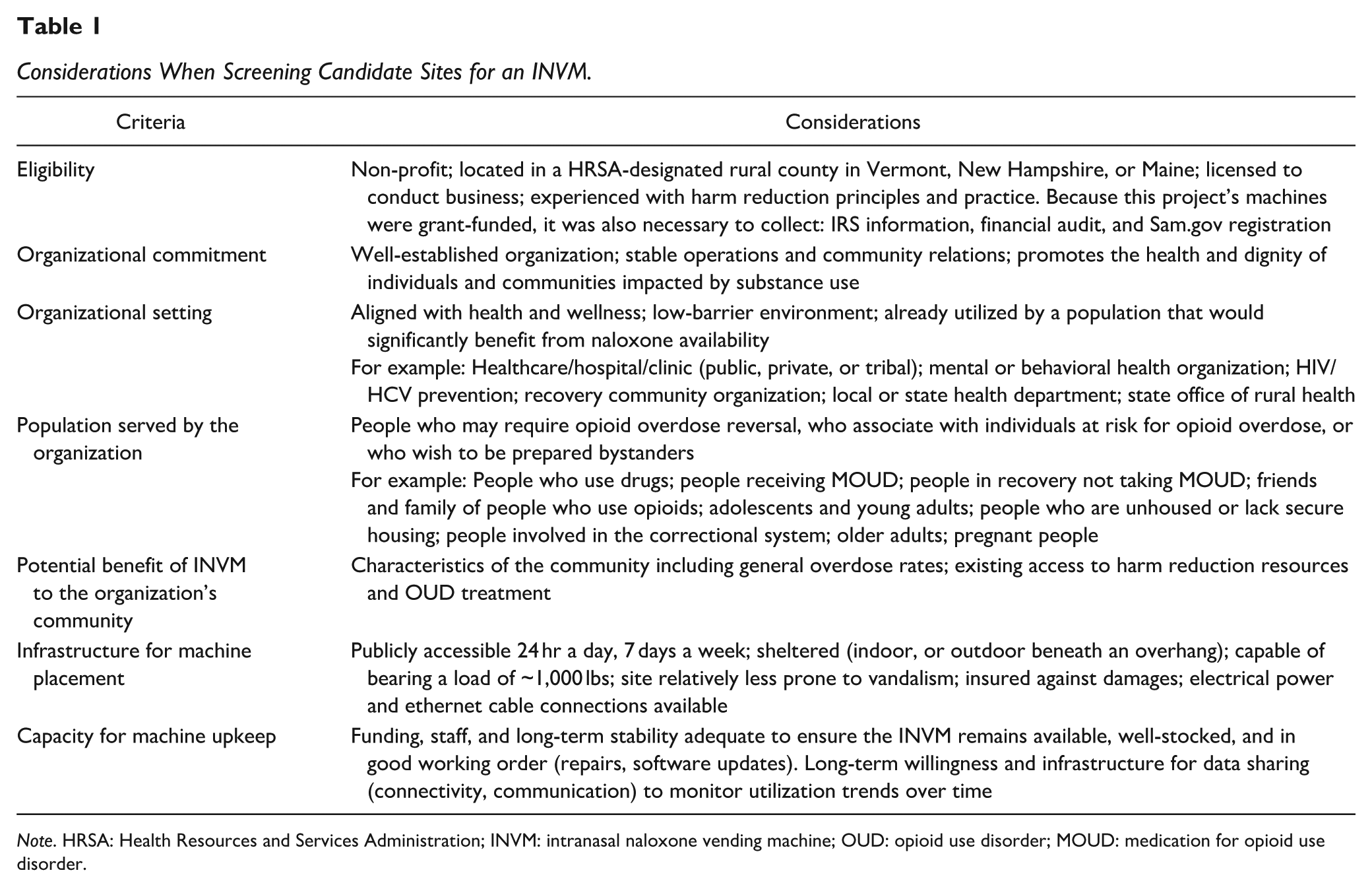
Note. HRSA: Health Resources and Services Administration; INVM: intranasal naloxone vending machine; OUD: opioid use disorder; MOUD: medication for opioid use disorder.
UVM CORA faculty and staff conducted videoconference interviews with applicants to confirm eligibility, further assess each rural organization’s interest in an INVM, how the machine might improve the care they provide to their rural clients and community, how the organization planned to communicate with rural community members and navigate any concerns, and logistics of installation and accessibility of the INVM to the community. In anticipation of community resistance to INVM that was identified in previous publications (Bessen et al., 2019; Stewart et al., 2023), our interview guide included questions about community support for overdose prevention efforts, existing approaches to naloxone distribution, and the value of a machine to the community.
Machine Design, Installation, and Upkeep
Following organization selection, each INVM was manufactured with custom specifications for its site, then installed when the machine and recipient organization were ready. After project planning in Fall 2022, the UVM CORA team selected VMs that could contain several hundred IN doses, maintain climate-controlled conditions within the dispenser, be reconfigured for supplies of different sizes if product dimensions were to change in the future, dispense products free of charge, display QR code links to additional resources and support, and electronically track and report utilization over time. Intelligent Dispensing Solutions (IDS, Des Moines, IA, USA) manufactured all five INVMs. The logo wrap and exact machine dimensions were customized for each rural organization. Machine capacities varied from 120 to 180 boxes (240–360 doses) of IN. Photographs of one of the installed machines can be seen in Supplemental Material. The manufacturing lead time from order placement to machine delivery was approximately 3 to 6 months, during which time the infrastructural considerations detailed in Table 1 were addressed. Installation was assisted by the manufacturer, who delivered the INVM and ensured proper placement and set-up. IN was ordered in bulk from Emergent BioSolutions (Rockville, MD, USA), packaged with two doses per dispensable box. Once the INVM was installed, each rural organization assumed responsibility for machine maintenance, repairs, software updates, and subsequent product restocking.
Community Relations
After rural organizations were selected, UVM CORA supported each organization’s efforts to prepare their community to be an INVM site, using an evidence-based approach to identify common concerns and effective methods and/or information to address them (Bessen et al., 2019; Islam et al., 2008; Stewart et al., 2023). Organizations were encouraged to proactively engage with their key local populations (e.g., partners, funders, law enforcement, first responders, individuals who use drugs and those who are in recovery, as well as their friends and family members), and with the community at large, to hear questions and concerns, provide information as needed, and build support prior to and following INVM arrival. Finally, UVM CORA supported public-facing events in each rural organization’s community involving public officials, community members, and the press to raise awareness about the presence, purpose, and benefits of having an INVM in the community.
Data Collection
Utilization data monitoring began immediately after each machine was installed, generally following the timeline shown in Figure 1. Each INVM was equipped with software that tracked descriptive data on machine utilization and tabulated the quantity of doses dispensed to generate monthly web-based reports allowing UVM CORA and the onsite rural organization to monitor utilization.
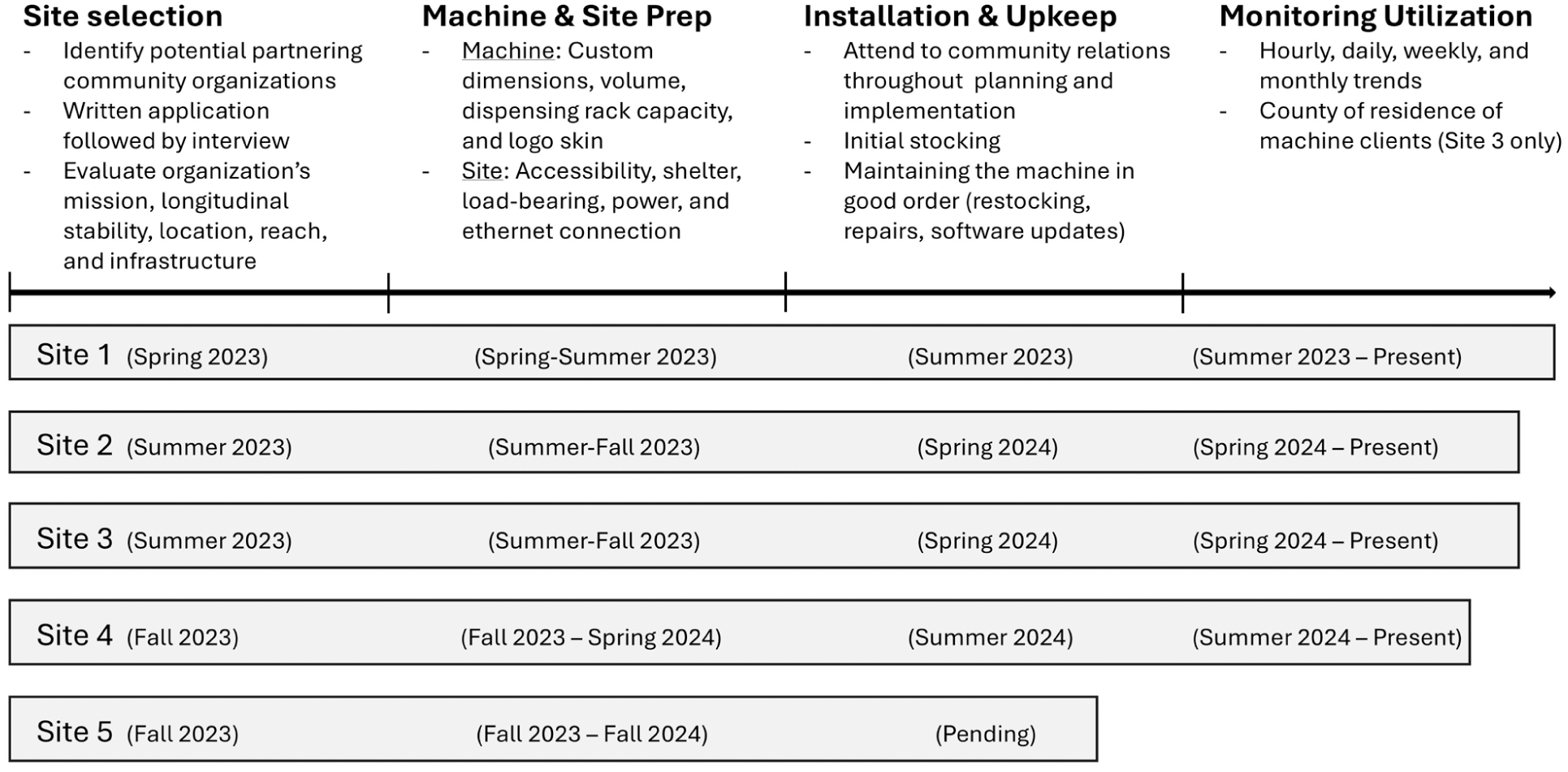
Process Overview for Intranasal Naloxone Vending Machine Implementation
In addition to the quantitative data generated by the VMs, the rural organizations have provided formative feedback throughout the entire project about their experiences with planning, installation, and data collection. The primary staff contact at each of the four sites also participated in a 30-min structured interview with two study authors [GR and SC] 30 days after machine placement. The 30-day follow-up interview encompassed questions about the rural organizations’ expectations versus actual experiences with the machine, community feedback surrounding INVM placement, any changes in the rate of utilization of their other in-person overdose prevention and/or treatment services since VM placement, and practical questions on machine functionality, restocking, and data monitoring. To synthesize this qualitative feedback, two study authors manually reviewed written communications and interview notes to identify patterns of experiences across organizations. While this was not research and the authors did not conduct formal thematic analysis, the authors met to discuss and compare their observations, reconcile discrepancies, and reach consensus.
Results
After reviewing all applications (24 total), we ruled out ineligible applications and selected 10 candidate organizations for virtual interviews with their Program or Site Directors and the individuals who submitted the application. Each interview was 60 min and was conducted by 3 to 5 faculty, staff, and program advisors from UVM CORA. The interviews were conducted in Fall 2022 and Winter of 2023 and covered questions related to the selection criteria. Interviewers separately rated each organization as to how well they met inclusion criteria. We identified the top ranked organizations, resolved ties through group discussion, and unanimously selected five organizations. Organizations included a primary care clinic (Site 1; county size = 26,060 residents), a family medicine clinic on a Native American reservation (Site 2; county size = 67,351), a health consortium (Site 3; county size = 93,146), a recovery center (Site 4; county size = 37,183), and a health justice organization (Site 5; county size = 56,526). INVM installation occurred in August 2023 (Site 1), March 2024 (Site 2), April 2024 (Site 3), and August 2024 (Site 4), with installation pending for Site 5 at the time of submission of this manuscript.
Machine Utilization
Utilization of each INVM through November 30, 2024, is detailed in Figures 2 and 3. Monthly total IN doses dispensed typically peaked in the first month following installation (mean of all sites = 131; range 44–226).Averaging across all months, doses dispensed per machine per month was 49.6 (range 29.3–70.5). With the first (outlier) month removed, average monthly doses dispensed across all sites was 47 (range 10–98). Our fourth machine has just 3 months of data. The percent change in doses dispensed by month over the first 3 months across all INVMs was −47.3 from month 1 to month 3.
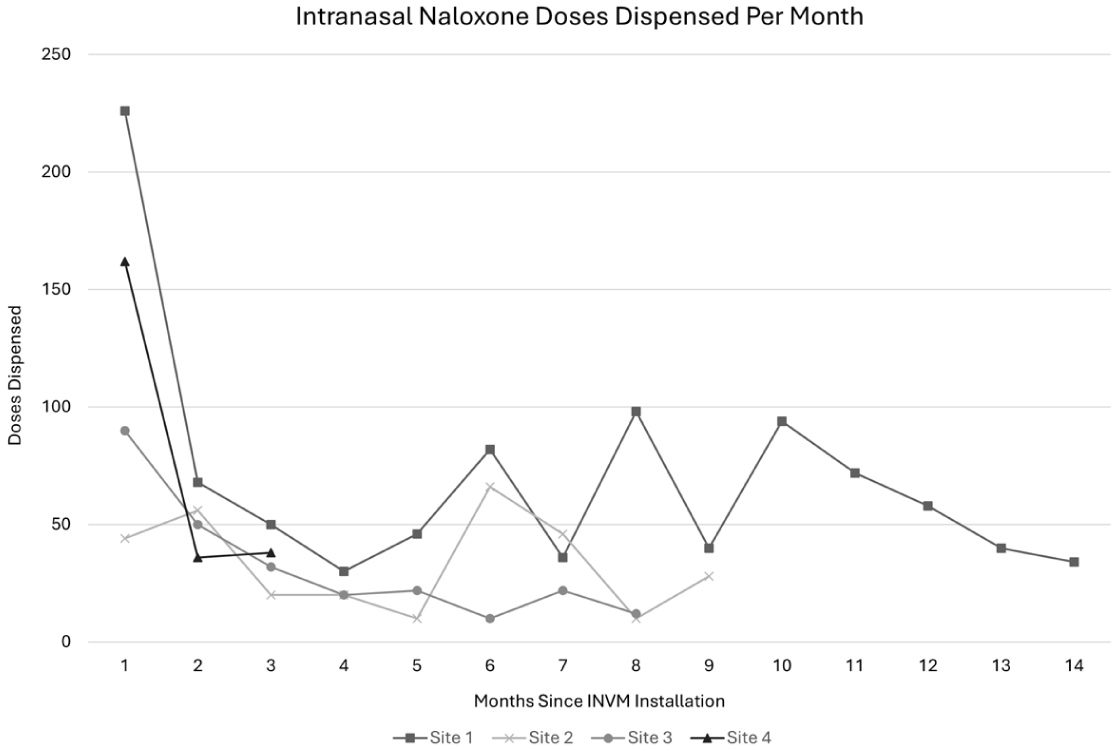
Intranasal Naloxone Doses Dispensed per Month From the Four Operational INVM Sites
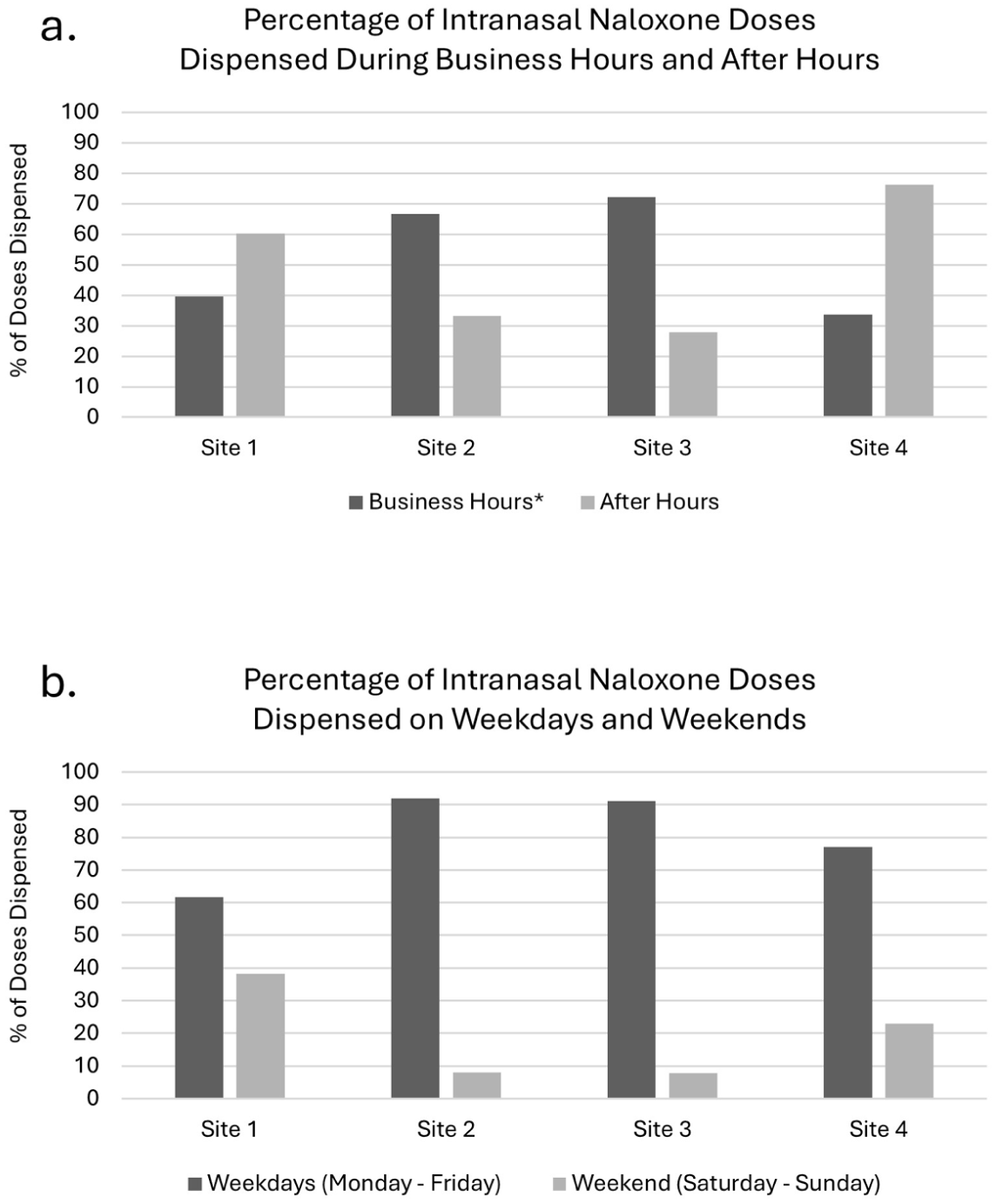
Intranasal Naloxone Dispensing Trends During Versus Outside of Business Hours
Figure 3a and b show the variability in daily and weekly dispensing patterns across the sites. INVM utilization outside of business hours (i.e., weekends plus overnights) accounted for between 27.9% and 76.3% of doses dispensed, depending on the site (Figure 3a). Combining data from all the sites, the average percent of doses that were dispensed off-hours was 49.5%. Weekend INVM utilization varied markedly between sites (range: 7.8%–38.3%; Figure 3b). Combining data from all the sites, approximately one-fifth (mean 19.3%) of doses were dispensed on weekends.
In addition, Site 3 collected data on the county and municipality of origin for individuals who accessed the VM via zip codes individuals voluntarily entered at the at the time of utilization. Those data indicated that 49% of dispensed IN doses were to residents of the town where the machine is located, 22% were dispensed to out-of-town residents of the same county, and the remaining 29% to individuals from one of five predominantly rural adjacent counties.
Community Relations
UVM CORA maintained contact with the point person at recipient organizations by email and videoconference as needed to address questions or concerns their staff may have received from rural community members regarding the anticipated arrival of the INVM in their community. Of the small number of concerns received, themes generally included (a) concern about allocation of resources to overdose prevention versus other, less stigmatized, public health problems; (b) concerns that an INVM may draw more people with SUD and potentially more crime to the area; but also (c) curiosity about the machine, its function and contents, and its potential positive versus negative impact on the community; and (d) desire to ensure the machine’s placement would balance accessibility, safety, and discreteness.
Themes arising from the organizations’ experiences with community relations indicated that to prevent and assuage community concerns it was helpful when organizations took a proactive approach to communication about IN, the effects of overdose prevention programs, and what the VM would and would not dispense. Providing education about IN was helpful, for example, explaining that naloxone itself has no abuse potential, can play a lifesaving role in opioid overdose reversal, does not require a prescription (Food and Drug Administration, 2024), can be safely administered by laypersons, and that provision of naloxone has not been shown to promote increased substance use (Bessen et al., 2019; Tse et al., 2022). For example, one organization encountered “a lot of negative comments online after the press release—concerns about the risk of children getting addicted, or about taxpayer money funding it. There’s a lot of misinformation about what [naloxone] can do. Putting out educational materials helps considerably.” Recipient organizations noted change over time in their communities’ attitudes. In the words of one recipient, “Now that [the INVM] is operational, the feedback has been overwhelmingly positive. Our [INVM] has set a precedent, such that other organizations are looking for their own funding to obtain a machine.”
With regard to overdose prevention more generally, organizations found that community concerns were eased by explaining that such programs or resources have not been shown to increase crime or public nuisance, but rather are related to significant reductions in opioid overdose morbidity and mortality, lessening of high-risk drug use behaviors, and increased referrals to addiction treatment and recovery programs (Day et al., 2016; Islam et al., 2008; Levengood et al., 2021; Stewart et al., 2023). One site stated “The local response has been positive, with the exception of one person. Our director met with him and talked through [the actual effects of harm reduction services], and he was reassured.” By the time each INVM became operational for public use, each organization reported overall community support and positive press coverage. As one site reported, “The town manager attended the ribbon cutting. . . Police are thrilled. Hospitals are supportive. Most organizations are giving [us] a lot of credit for bringing the machine to the community.”
Impact on In-Person Distribution of Risk Reduction Services
All four rural INVM organizations reported dispensing more IN through their VM than they have historically distributed through in-person interactions. Site 1 stated “We have never given out 97 boxes of naloxone in a month before, but the [INVM] exceeded that amount within our first month.” Site 2 reported being “surprised by the numbers. It was more than we’ve ever distributed [in person] in any month prior.” Site 3 stated that they had distributed an average of 70 IN doses per month during the 3-month period prior to INVM implementation, compared to 90 doses in the first month with the machine. Similarly, Site 4 reported distributing IN to “perhaps one person a month who came inside to request it” prior to arrival of the INVM, versus 44 doses dispensed during the machine’s first month in operation.
No site reported decreased in-person client volume or hearing that their services were being bypassed in favor of using the INVM. Several organizations reported that the machine appeared to increase awareness about their services and draw new clients to their program. For example, Site 4 described an encounter with a man who approached them for educational materials and a dose of IN to keep in his home because his partner takes prescription opioids for chronic pain. Site 3 reported that a school heard about their INVM and requested a training on overdose risks, harm reduction, and how to administer IN. Of note, Site 2 articulated a desire to balance their efforts toward raising awareness about their overdose prevention services against the desire to maintain a discrete site for individuals’ privacy, stating “We need to increase awareness about our offerings and let people know that [the INVM] is operational, but it’s a double-edged sword. We don’t want to frighten people away by making it too visible.”
Discussion
In this first rural-focused INVM implementation project, community utilization of the INVMs was high at each site, with over 500 IN doses dispensed during the first month after placement. Overall IN distribution rates (counting both INVM and traditional in-person methods) initially increased by orders of magnitude (up to 40-fold at Site 2), followed by a lower but steady average number of doses dispensed per month, while in-person client visits to the physical site remained the same or slightly increased, and requests from the broader community for additional overdose prevention education increased. Our findings are consistent with prior reports that VMs lower barriers to risk reduction access and may attract participants who would not otherwise access materials from fixed sites or pharmacies, or during traditional business hours (Kerr et al., 2022; Russell et al., 2023).
While each rural organization in our pilot encountered some expressions of concern from community members in advance of VM implementation, all found that concerns were readily addressed by proactive communication and information. This finding is consistent with prior reports noting the importance of establishing strong feedback loops between the organization where the VM was located, people who use overdose prevention resources, and the broader community (Islam et al., 2008; Russell et al., 2023).
While our program’s VMs only dispensed IN, other studies have investigated community acceptability of VMs that dispense other risk reduction items. In a study of community perspectives about harm reduction VMs in Philadelphia (Stewart et al., 2023), interviews with healthcare workers, businesses and faith-based organizations, and community advisory boards found universal support for dispensing IN; general acceptance for providing test strips, first aid equipment, and wound care supplies; but marked controversy over dispensing syringes and needles. Educational resources about SUD and materials helping people connect with services (e.g., crisis hotline, shelters, and treatment programs) were also viewed favorably, and likely to help the VM gain community acceptance (Stewart et al., 2023). By design, all the machines in our project dispensed IN only, and none offered syringes or needles.
While INVMs are not a comprehensive or stand-alone solution to the ongoing opioid overdose crisis, they may help rural communities provide affordable access to tangible overdose prevention resources via a low-stigma and low-barrier approach (Allen et al., 2022; Kerr et al., 2022; Russell et al., 2023; Stewart et al., 2023). INVMs can also gather local- or regional-level data on the demand for IN (and other overdose prevention resources, if the machine is also configured to dispense them), which may provide useful insights for community-specific planning. As our participating organizations found, VM implementation at rural sites may also create opportunities for robust discussions and potential new partnerships in rural communities.
Limitations to this project include its small sample size (four active sites), limited follow-up time for data collection (3–14 months to date, depending on the site), and the localized focus on rural northern New England. However, the quantitative utilization data and qualitative interview themes are congruent for all four sites, and our data are consistent with the existing literature on harm reduction VMs. As another limitation, the decision to maintain the full anonymity of people who use the INVMs means that we are unable to systematically collect information from the end-users of the IN obtained from the machines, precluding direct data on whether it has been administered in overdose situations. Future INVM installations might consider implementing an anonymous registration and survey process similar to that used in other studies (Allen et al., 2022; Arendt, 2023) to enable collection of end-user experiences.
Sustainability of the INVMs over time is an issue we addressed from the outset. One of our selection criteria was demonstrated sustainable infrastructure and finances to support the continued independent operation of the VM beyond the period of support by our center. We ascertained this criterion by asking the organizations to identify their current and past funding sources, current sources of IN, duration of operation in that community, ownership of their property, relationships to other community organizations, current staffing, and ability to designate one person as the VM monitor and liaison with our center. While these attributes can help an organization remain solvent, funding is always an issue and an organization’s flexibility to adapt to various unanticipated circumstances is a critical component of their success. In this case, the INVM provides a free product that the organization was already supplying. When the stock we provided is depleted, the organizations are aware they will need another source of IN. The organization also needs to plan for the costs of electricity and the monthly fee to the machine’s manufacturer. These costs are potentially prohibitive to some organizations and affordable to others. Future research could conduct longer-term follow-up evaluations with organizations to understand their challenges to sustainability.
Overall, INVMs may offer an important new low-barrier mechanism for dispensing IN and other lifesaving resources in rural communities hard-hit by the opioid epidemic. Our experience with planning, placing, and monitoring INVMs in rural communities supports the feasibility of this approach to increase rural access to naloxone, and can serve as a model for other potential sites seeking to implement their own. Future research on the experiences of machine users and the staff of the hosting organizations could answer questions about the perceived value of INVMs versus other sources of naloxone, the circumstances under which it was accessed (e.g., urgent vs. general need), or the effect of the machine on community member engagement with the organization (e.g., increase in requests for other supplies or accessing clinical services). Community-based research could examine whether acceptance of a broader scope of VM-based risk reduction resources increases over time after a rural community has grown accustomed to a naloxone-only VM. Studies with more rigorous prospective pre-post or randomized designs could quantify the impact not only on IN distribution but also on IN administration in the community, regional overdose deaths, or community acceptance of risk reduction more generally.
Supplemental Material
sj-jpg-1-prv-10.1177_26320770261434033 – Supplemental material for Distributing intranasal naloxone in rural communities: Implementation of a novel approach
Supplemental material, sj-jpg-1-prv-10.1177_26320770261434033 for Distributing intranasal naloxone in rural communities: Implementation of a novel approach by Gail L. Rose, Stephen Crosswhite, Kelly R. Peck, Sarah H. Heil and Stacey C. Sigmon in Journal of Prevention and Health Promotion
Supplemental Material
sj-jpg-2-prv-10.1177_26320770261434033 – Supplemental material for Distributing intranasal naloxone in rural communities: Implementation of a novel approach
Supplemental material, sj-jpg-2-prv-10.1177_26320770261434033 for Distributing intranasal naloxone in rural communities: Implementation of a novel approach by Gail L. Rose, Stephen Crosswhite, Kelly R. Peck, Sarah H. Heil and Stacey C. Sigmon in Journal of Prevention and Health Promotion
Footnotes
Acknowledgements
The authors acknowledge the assistance of Cassandra Beste in the acquisition and summary of relevant literature and Sarah Jacobs, MD, in writing and editing.
Ethical Considerations
The University of Vermont Institutional Review Board deemed this project not research and thus waived the requirement for approval of this project.
Consent to Participate
The University of Vermont Institutional Review Board deemed this project not research and thus waived the requirement to obtain informed consent.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health Human Services (HHS) as part of an award totaling $3.33 million per year with zero percentage financed with non-governmental sources. The contents are those of the authors and do not necessarily represent the official views of, nor an endorsement, by HRSA, HHS, or the U.S. Government. As the Rural Communities Opioid Response Program (RCORP) - Rural Center of Excellence (RCOE) on SUD Treatment, University of Vermont provides access to a wide range of resources on relevant topics. Inclusion in this paper does not imply endorsement of, or agreement with, the contents by The University of Vermont Center on Rural Addiction RCOE on SUD Treatment or the Health Resources and Services Administration.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data can be shared upon reasonable request from the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.