
Abstract
Intimate partner violence (IPV) is behavior in an intimate relationship that causes physical, psychological or sexual harm (World Health Organisation [WHO], 2012). IPV encompasses physical and sexual violence, psychological abuse (e.g., humiliation) and controlling behaviours (e.g., isolating) (WHO, 2012). Reportedly experienced by 2.4 million adults (5%) in England and Wales in 2021–2022 (Office for National Statistics [ONS], 2022a), IPV has profound negative effects on victim physical and mental health (Campbell, 2002), considerable social and economic costs (Home Office, 2019) and is a public health concern.
Often unreported, IPV is a concealed problem, and few reported cases are recorded as crimes (ONS, 2020). Official figures are, therefore, likely to be misleading. Several possible reasons are worth consideration: variation remains in public sense-making of IPV; IPV has been considered a private matter (Montalvo-Liendo, 2008); and physical abuse is often appraised as IPV, but non-physical abuse may be considered less abusive (Carlson & Worden, 2005; Minto et al., 2020). Indeed, many individuals in emotionally, economically or verbally abusive relationships reportedly did not consider this abuse (Cravens et al., 2015).
Common in media headlines, IPV discourses tend to blame victims (e.g., by describing perpetrators as ‘jilted lovers’, insinuating some if not all victim responsibility) (Lloyd & Ramon, 2016). This is concerning as helping agencies such as criminal justice and healthcare systems share contexts with these discourses. Indeed, victim-blaming tendencies reportedly exist among some healthcare professionals (Sprague et al., 2012). Police may be more likely to arrest perpetrators of physical abuse over other forms (Myhill, 2017), and arrests reportedly depend on victim gender (Fagerlund, 2021).
One important factor is perceived acceptability of IPV (Waltermaurer, 2012). IPV sense-making varies with context as individuals reportedly use ‘conditional logics’, or cite certain contextual factors (such as victim behaviour or whether the abuse is novel or repeated), to legitimise abuse (Lelaurain et al., 2018). This is significant as those who maintain that IPV is admissible are less likely as victims to report it and more likely to self-blame (Tran et al., 2016). Such contextual factors may include perpetrator substance use (Javaid, 2015), mental health difficulties (Varshney et al., 2016) and gender (Carlson & Worden, 2005).
Research suggests that IPV perpetrated by men is considered more justified in some contexts (e.g., if his partner neglects the children or goes out without telling him) than others (e.g., if his partner argues with him) (Hayes & Boyd, 2017), and abuse perpetrated by women is less likely to be appraised as IPV than abuse perpetrated by men (Carlson & Worden, 2005). This indicates an ambiguous relationship between IPV and gender. Factors relevant to IPV legitimisation may pertain to cisgender stereotypes (Scarduzio et al., 2016), while the context in gender nonbinary communities is more uncertain. Abuse is reportedly more common in gender nonbinary communities (Peitzmeier et al., 2020), but research is lacking regarding sense-making of IPV committed by gender nonbinary individuals.
Research highlights a relationship between post-traumatic stress disorder (PTSD) diagnoses and IPV perpetration (Shorey et al., 2021). Whether this is a conditional logic, however, is uncertain, although research suggests IPV appraisals may vary with this diagnosis as IPV was less recognised as such when the perpetrator had a diagnosis of PTSD and was a construction worker rather than a military veteran (Mackinnon et al., 2023). Further research is needed regarding perceived admissibility of IPV in this context.
Public sense-making of IPV is nuanced, something the UK government aimed to address via the Domestic Abuse Bill 2020 (Home Office, 2020a), which details a revised description of abuse to include coercive control, psychological and financial abuse. The bill hoped to improve public understanding, victim safeguarding and legal system responses. However, gaps exist in the literature regarding public sense-making of IPV and conditions that facilitate its justification. Victim-blaming narratives may be internalised by victims of IPV and their communities, and may affect disclosures, responses and management. Research is, therefore, necessary to explore public discourses of IPV.
Aims
The aim of this study was to explore how people make sense of IPV in the context of perpetrator diagnostic status (PTSD or no PTSD) and gender identity (female, male or nonbinary) by exploring IPV ratings and IPV discourses. The study differentiated between sex (based on anatomy and typically assigned at birth) and gender (a deep, self-defined internal sense of self, which may or may not correspond with sex) (Stonewall, 2023).
The study explored effects of perpetrator qualities only. Via the exploration of gender identity, it built upon research by Mackinnon et al. (2023), which investigated public IPV discourses regarding military background and PTSD diagnosis.
Owing to its preliminary nature, study hypotheses were broad and no predictions regarding direction of effect were made. Hypotheses were: (i) IPV ratings would vary with perpetrator diagnostic status and gender identity; and (ii) IPV discourses would vary with perpetrator diagnostic status and gender identity.
Method
Ethical Approval
The study received ethical approval from the University of Bath Psychology Research Ethics Panel (reference 21–257).
Design
A between-groups, mixed methods design was used. All participants completed quantitative measures and half completed a qualitative exercise. Independent variables were perpetrator diagnostic status (PTSD or no PTSD) and gender identity (female, male or nonbinary). Dependent variables were IPV ratings and IPV discourses.
Participants
A G*Power analysis indicated that, based on Cohen’s (1992) effect sizes and an alpha of .05, samples of 400 and 107 were needed for small and medium effect sizes, respectively. The study was, therefore, adequately powered to identify medium and small-medium effects. A small-medium effect size was the smallest effect to be considered meaningful in the absence of prior literature on which to base such calculations.
Demographic Data (N = 265).
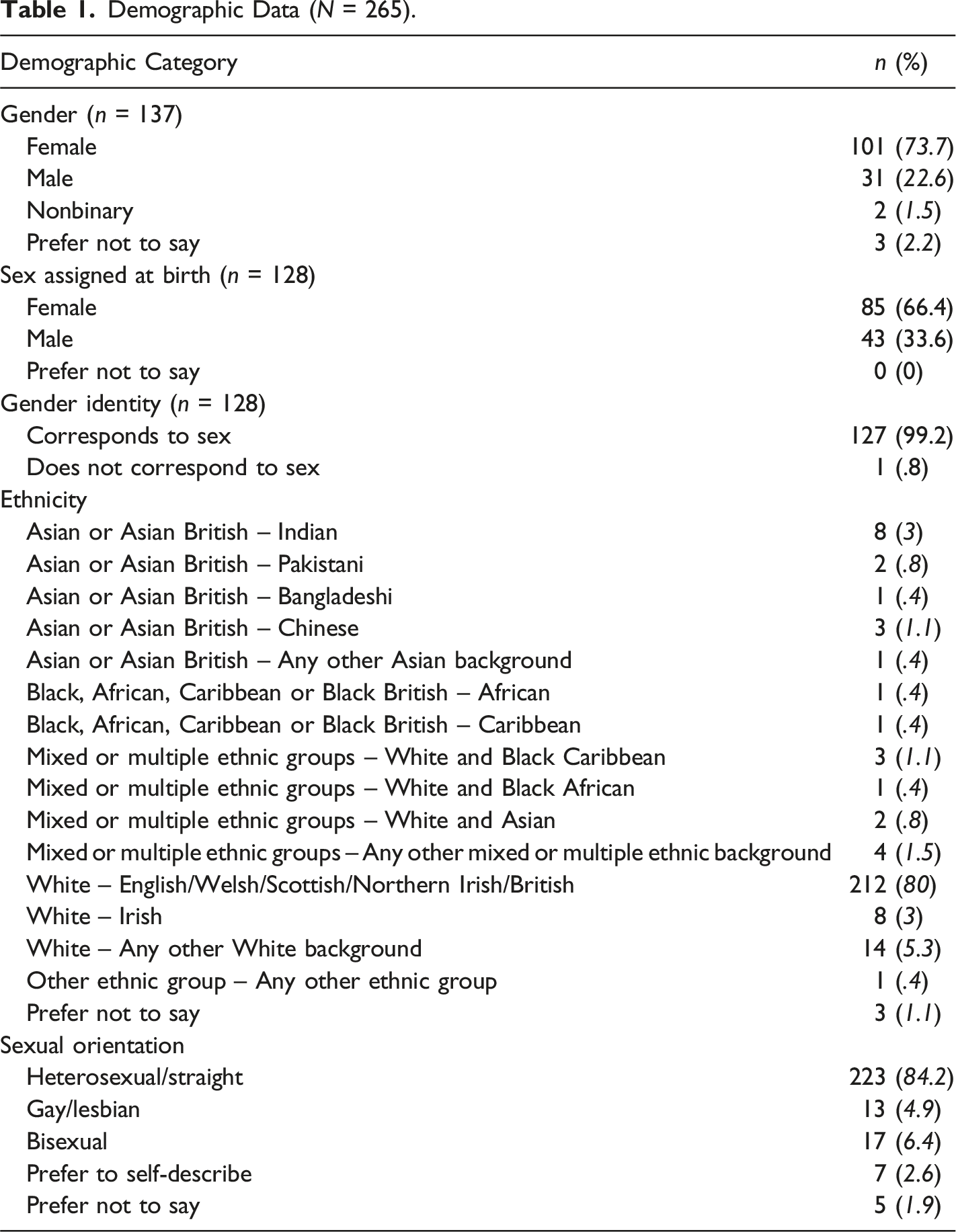
Age ranged from 18 to 90 years old (median = 31.24; IQR = 26.6) and was positively skewed. Eighty per cent (80%) were White British (vs. 74.4% of the population in England and Wales [ONS, 2022b]). Women were overrepresented (70.2%), and three participants identified as gender nonbinary (2.3%). Of those asked (n = 128), most said their gender identity corresponds to their sex assigned at birth (99.2% vs. 93.5% of the population in England and Wales [ONS, 2023a]). Sexual orientation was reasonably well matched (84.2% heterosexual vs. 89.4% of the population in England and Wales [ONS, 2023b]). Responses from participants who preferred to self-describe their sexual orientation (2.6%) were ‘queer’, ‘pansexual’ and/or ‘asexual’.
Participant Relevant Experience (N = 265).
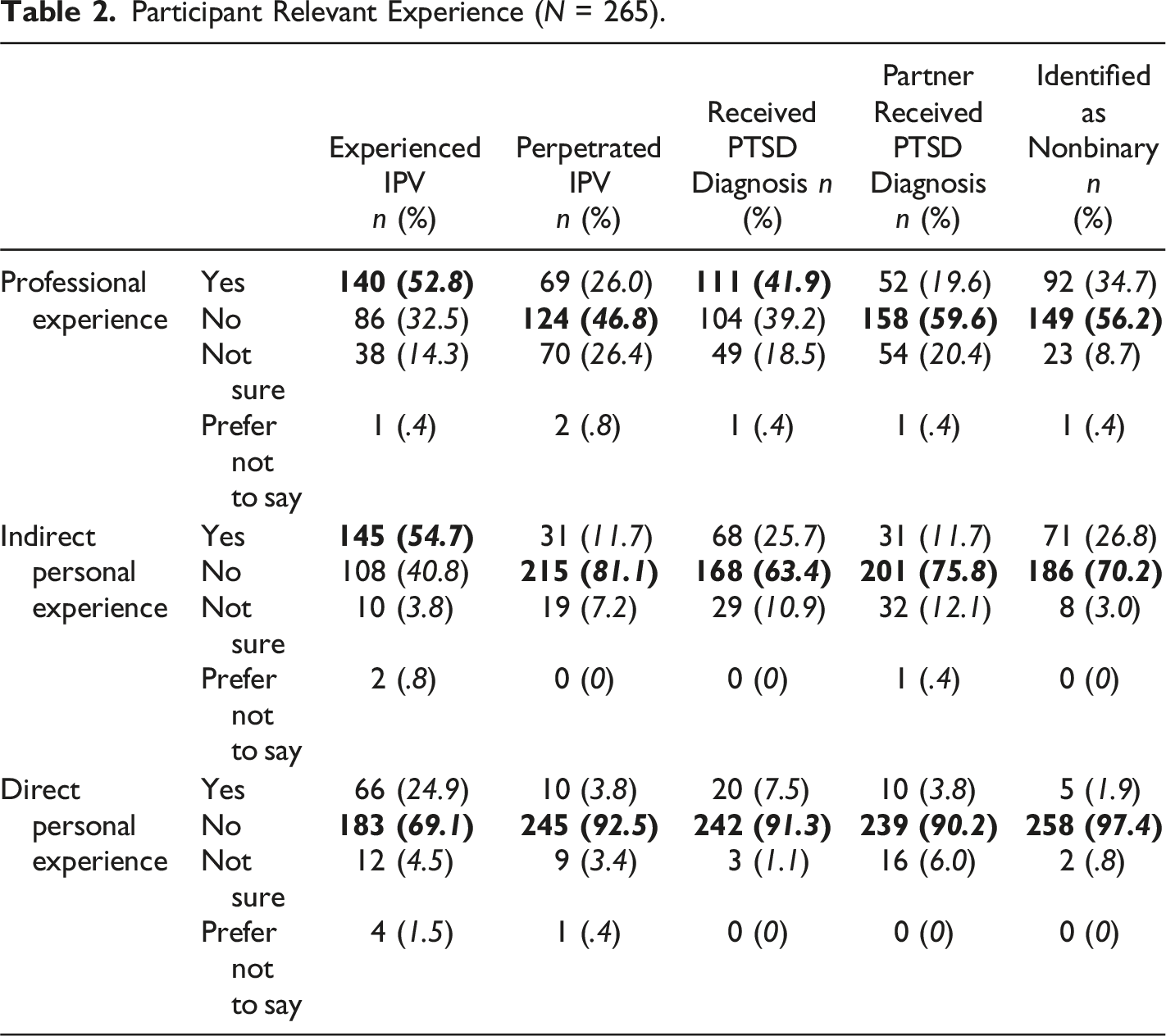
There were high rates of professional experience with IPV (52.8%) and PTSD diagnosis (41.9%) and indirect personal experience with IPV (54.7%). Rates of direct personal experience of IPV (24.9%) and PTSD diagnosis (7.5%) were elevated compared to UK prevalence rates for IPV (5%; ONS, 2022a) and PTSD diagnosis (3.88%; PTSD UK, 2022).
Materials
Story
A story depicting IPV between two partners was adapted from Mackinnon et al. (2023) (Appendix B). In the story, Alex hid a phone belonging to Frances (control) then hit a wall and threw the phone towards Frances (physical threats; aggression). Frances told a friend, Nicky, and asked for advice. Stories were identical across conditions bar perpetrator diagnostic status (PTSD or no PTSD) and perpetrator gender identity (female, male or nonbinary). Names were chosen to be gender neutral.
Measures
Study Measures.
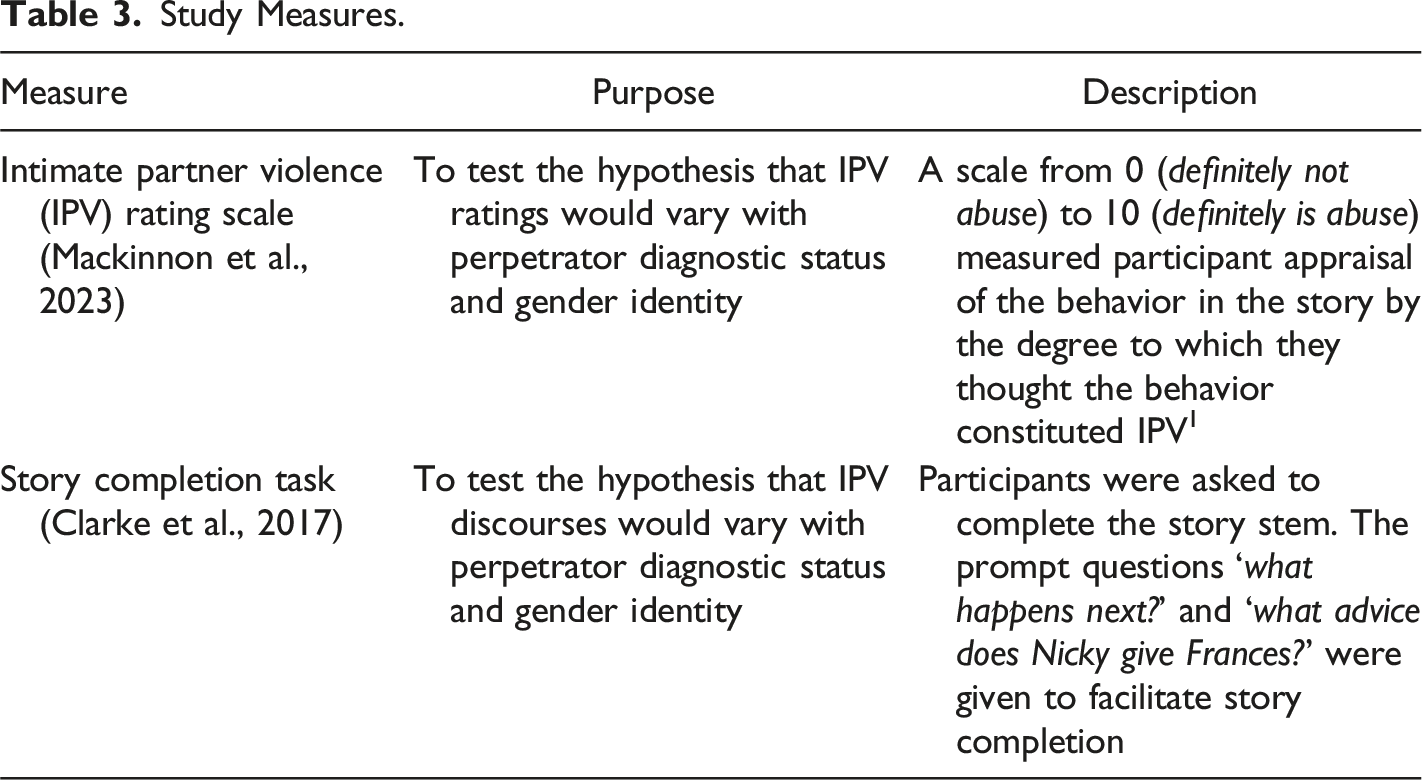
Suitable for various theoretical positions, SC was analysed within a contextualist framework, which acknowledges that realities are mediated by socio-cultural meanings and ‘truth conditions’ of knowledge claims vary with the contexts in which the claims are made (Pynn, 2016). As such, the stories generated by participants reflect wider discourses and narratives around IPV, PTSD and gender, and it is these discourses and narratives that provide the context within which individuals make sense of IPV. Prompt questions were chosen to enable theoretical consistency.
Procedure
The study was hosted online via Qualtrics. Participants were told the study aim was ‘how we make sense of personal relationships’ to reduce priming regarding IPV. Written informed consent and demographic information were collected. Participants were randomly assigned via Qualtrics function to one of six groups: (i) Female-PTSD; (ii) Female-No PTSD; (iii) Male-PTSD; (iv) Male-No PTSD; (v) Nonbinary-PTSD; (vi) Nonbinary-No PTSD. The relevant story was provided, and participants rated the extent to which they thought the behavior constituted IPV. Approximately half the participants were randomly allocated via Qualtrics function to the story completion exercise. Finally, participants were asked to specify their perception of the victim gender. A debrief with information of relevant support organisations was provided to all participants on study completion.
Data Analysis
Quantitative Data
Exploratory analysis using box plots identified three outliers each in Male-PTSD and Nonbinary-No PTSD, and significant negative skew in Nonbinary-No PTSD. As the study was preliminary, and the number of outliers and associated risk of bias low, all data including outliers were analysed, and the large sample size meant a normal distribution was not necessary (Field, 2013). A two-way ANOVA, therefore, measured main and interactive effects of perpetrator diagnostic status (PTSD or no PTSD) and gender identity (female, male or nonbinary) on IPV ratings. An ANCOVA measured effects of demographic and relevant experience variables on IPV ratings. Parameter estimates were based on 1000 bootstrapped samples to increase robustness (Field, 2013). Finally, whole sample victim gender check frequencies were calculated. As the study explored effects of perpetrator characteristics, the victim gender check was not an outcome measure but intended to capture broad narratives about who experiences IPV.
Qualitative Data
Approximately half the participants in each condition were randomly assigned to the story completion task (n = 130). Data were uploaded to NVivo and analysed using reflexive thematic analysis (RTA) (Braun & Clarke, 2019) to explore themes in public sense-making of IPV. Like story completion, RTA was used within a contextualist framework, and ‘reflexive’ acknowledges researcher subjectivity in theme identification.
The author familiarised themselves with the data then generated codes to capture meaning in the data. Codes were semantic and captured explicit meaning in the data (where codes were latent this is clearly noted). Inter-rater reliability checks of codes were not used as inter-rater reliability is grounded in a positivist framework that presupposes a reality in the data. Codes were collated into themes and both codes and themes were reflected upon and refined with the primary supervisor. Code frequency was explored to identify theme similarities and differences across conditions.
Results
Victim Gender Check
Participant perceptions of victim gender are shown in Figure 1. Nearly half the participants (n = 119; 44.9%) responded ‘female’. Remaining responses were ‘did not think about it’ (62; 23.4%), ‘not sure’ (45; 17%), ‘male’ (26; 9.8%), ‘nonbinary’ (six; 2.2%), ‘girl’ (three; 1.1%), ‘woman’ (two; 0.8%), ‘made no assumption’ (one; 0.4%) and ‘not important’ (one; 0.4%). Victim gender check responses (N = 265).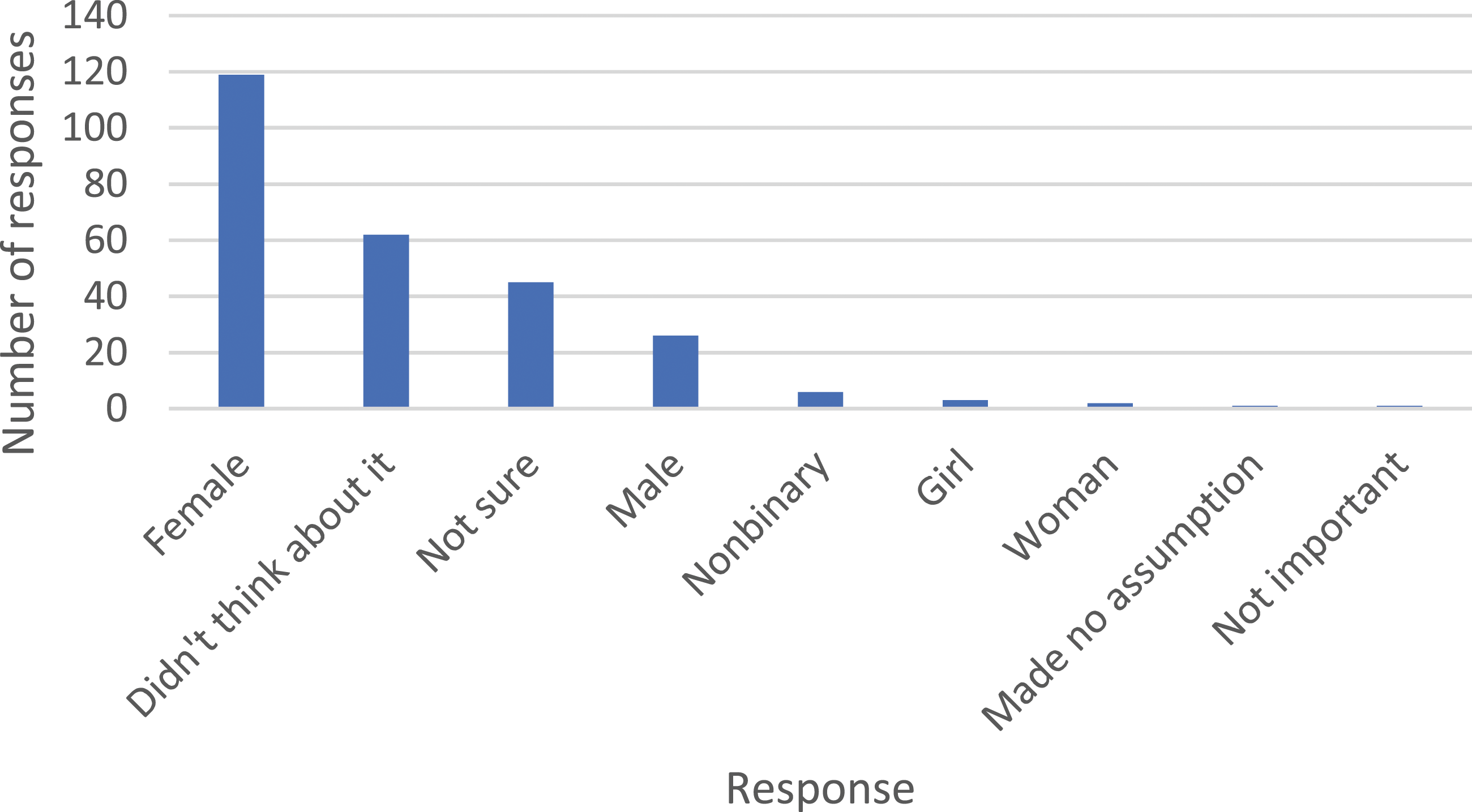
IPV Ratings
IPV Ratings (N = 265).
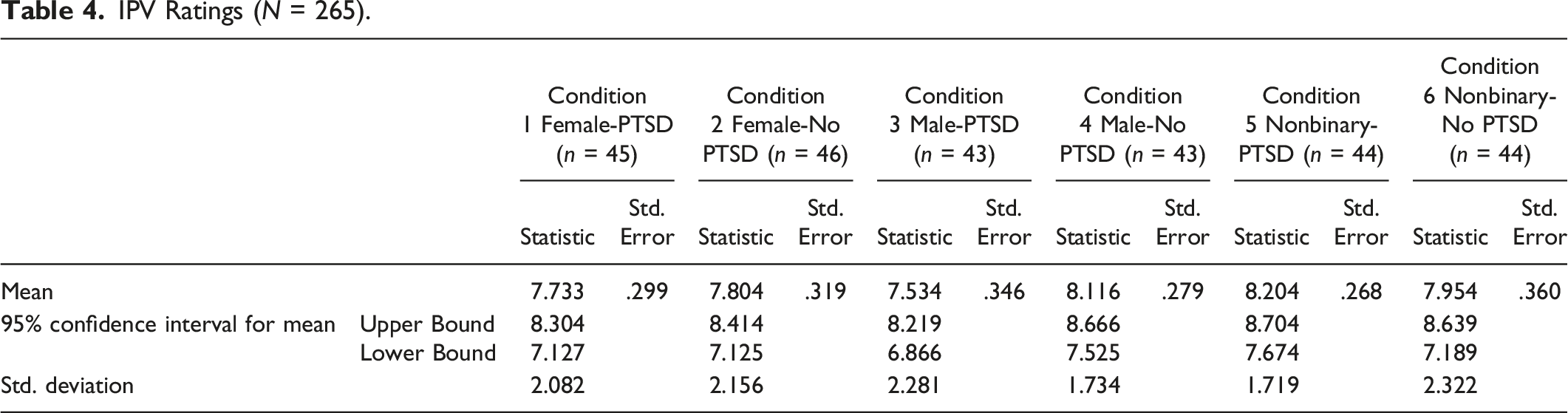
A two-way ANOVA found no significant interaction between diagnostic status and gender identity on IPV ratings (F [2, 259] = .896, p = .410, partial η2 = .007). There was no significant main effect of diagnostic status (F [1, 259] = .279, p = .598, partial η2 = .001) or gender identity (F [2, 259] = .569, p = .567, partial η2 = .004) on IPV ratings. The model fit was weak (r2 = .012), meaning most of the variance in IPV ratings is best explained by other factors.
Covariates
An ANCOVA found no significant effect of participant demographic or relevant experience variables on IPV ratings. Professional experience of experienced IPV (working in a professional capacity with someone who had experienced IPV) approached but did not reach significance (F [1, 258] = 3.621, p = .058, partial η2 = .014).
IPV Discourses
Data Extracts for ‘Characterise the Behavior’ (n = 130).
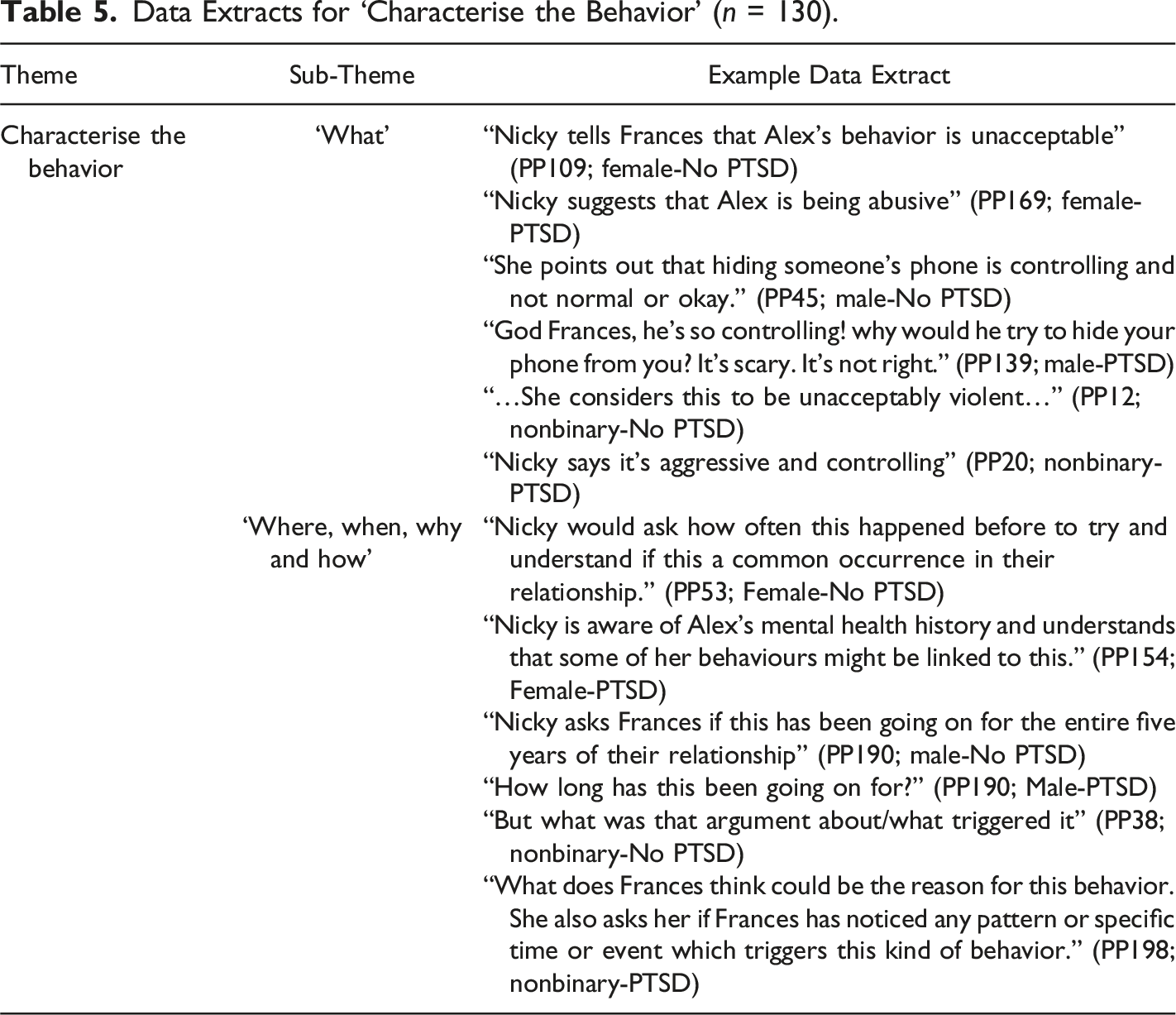
Characterise the Behavior
Participants consistently characterised Alex’s behavior. Responses included descriptors and language that considered its frequency, duration and cause. Two subthemes were identified: (i) ‘what’; and (ii) ‘where, when, why and how’ (Table 5). The behaviour was repeatedly described as aggressive, controlling, violent, abusive and unacceptable. ‘Abusive’ and ‘domestic violence’ were used more frequently in no PTSD than PTSD conditions regardless of gender identity, and most frequently in Nonbinary-PTSD. Responses across conditions linked the PTSD diagnosis to the behaviour but there was no theme regarding PTSD diagnosis as an excuse.
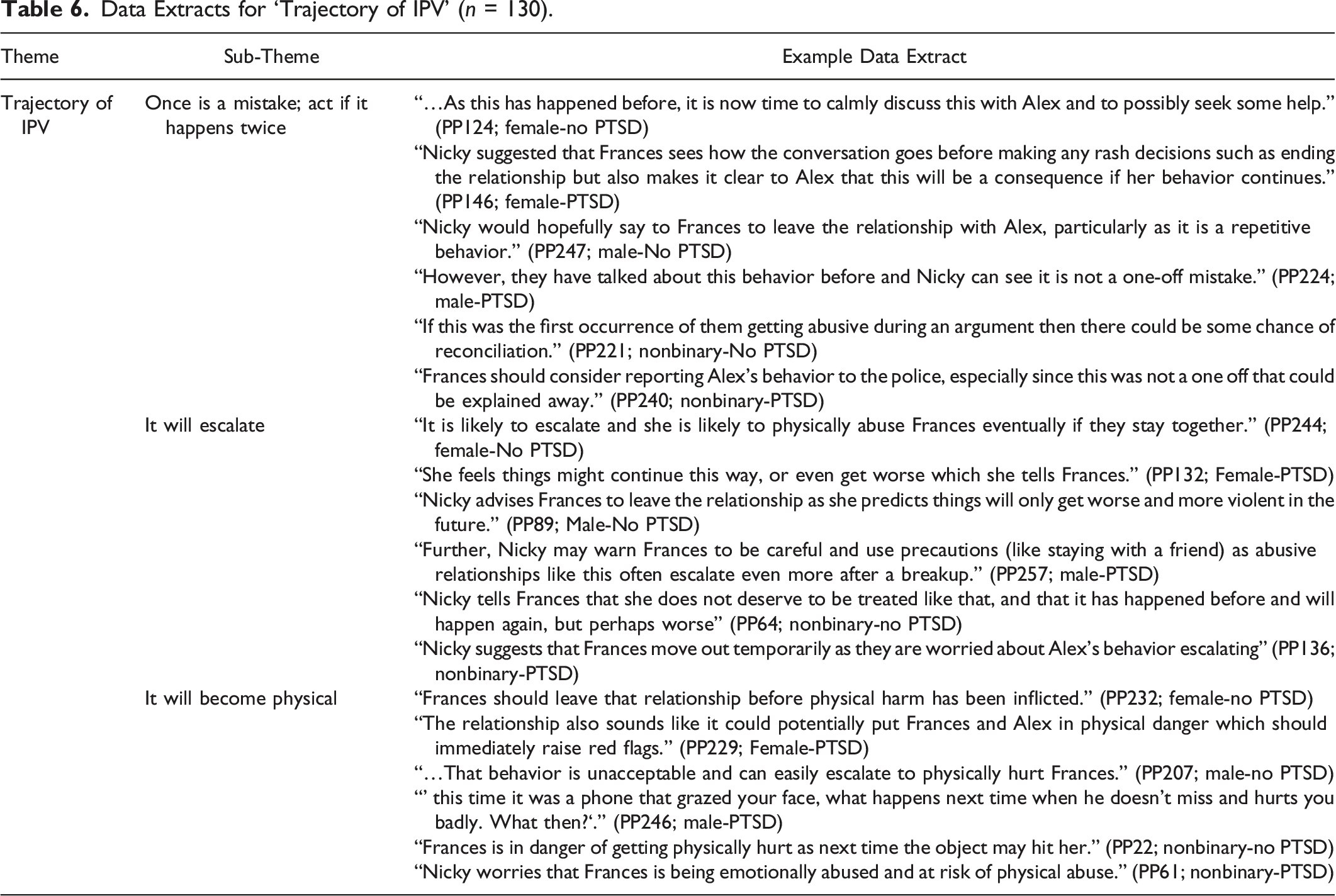
Trajectory of IPV
Data Extracts for ‘Trajectory of IPV’ (n = 130).
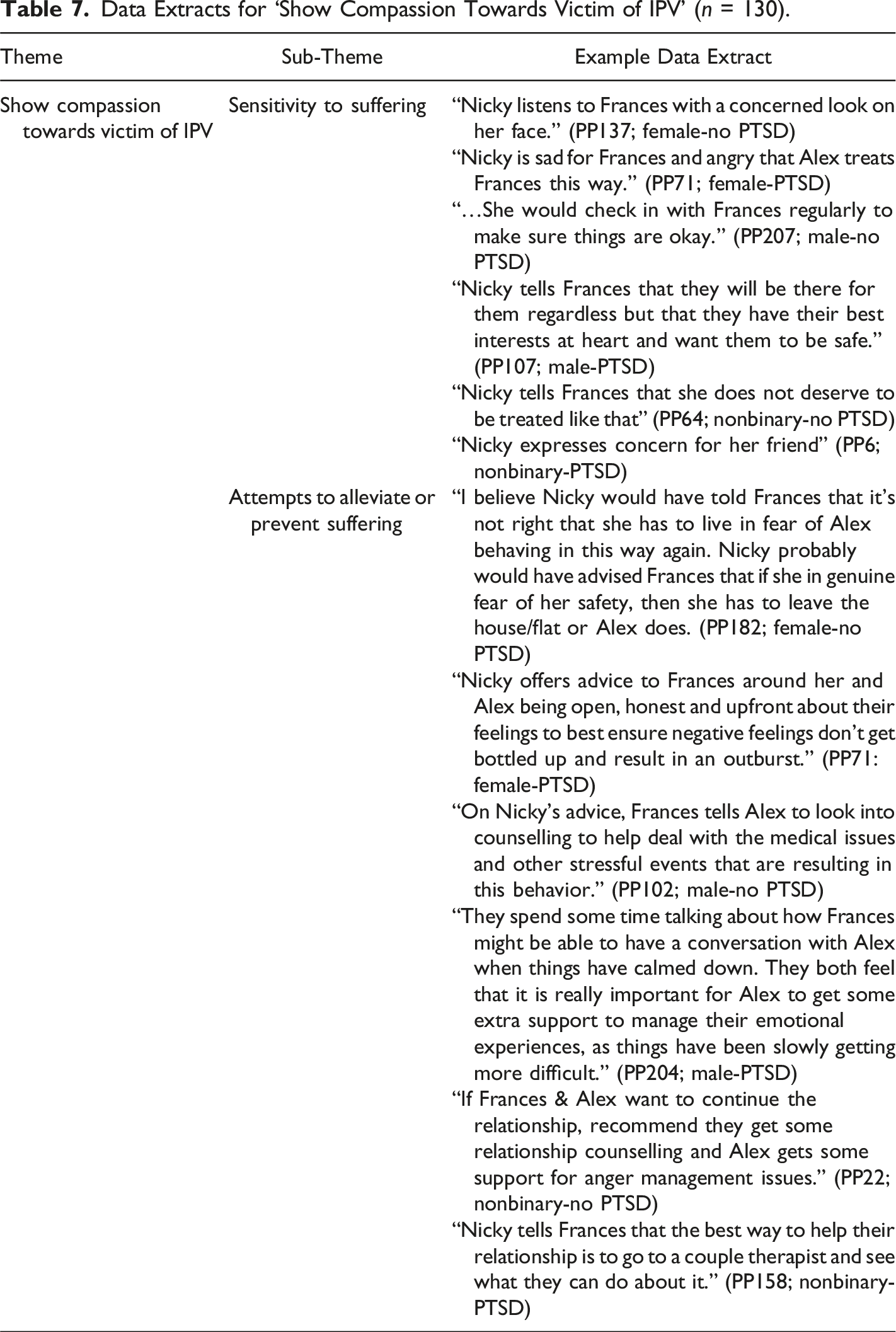
Show Compassion Towards Victim of IPV
Data Extracts for ‘Show Compassion Towards Victim of IPV’ (n = 130).
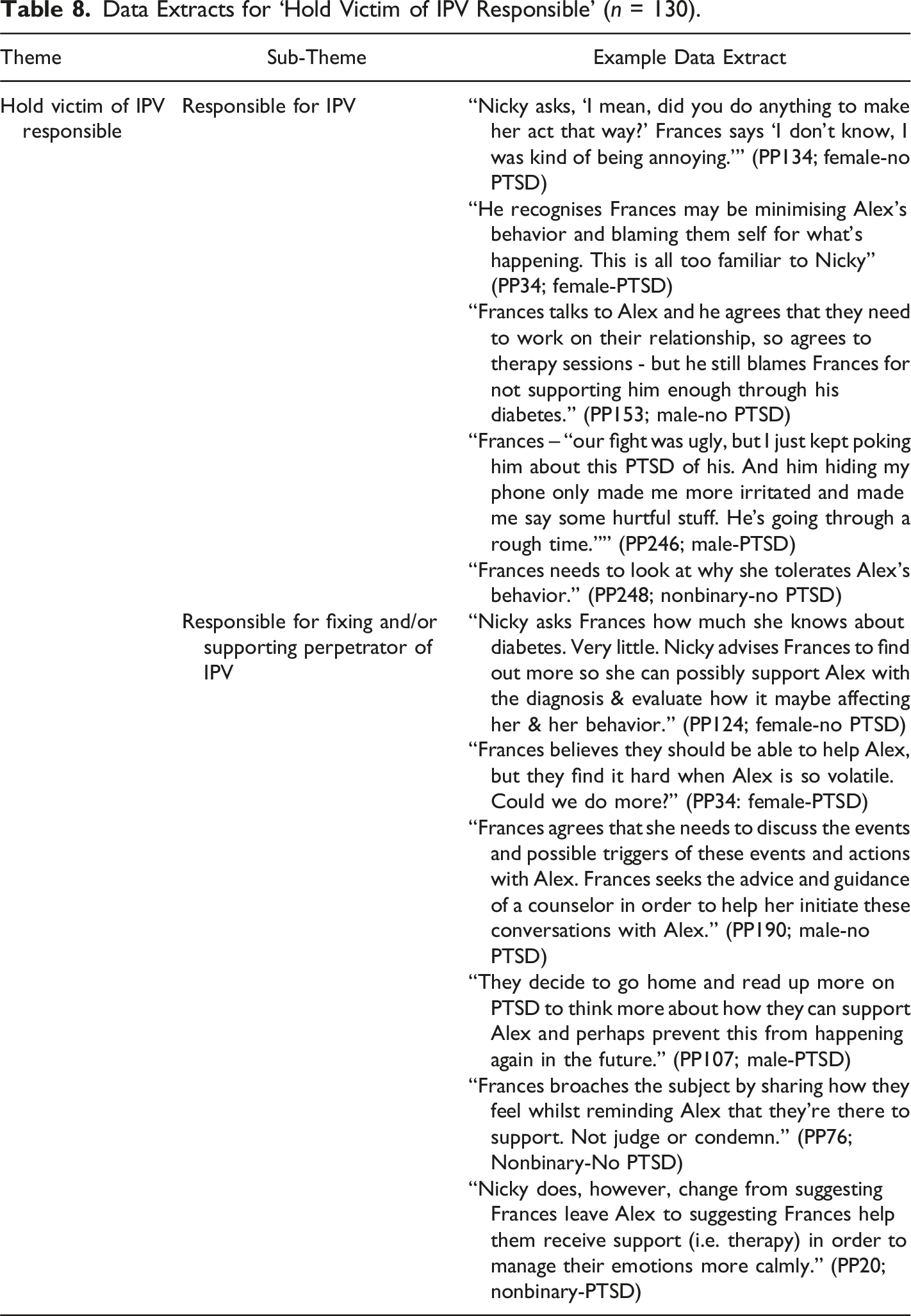
Hold Victim of IPV Responsible
Data Extracts for ‘Hold Victim of IPV Responsible’ (n = 130).
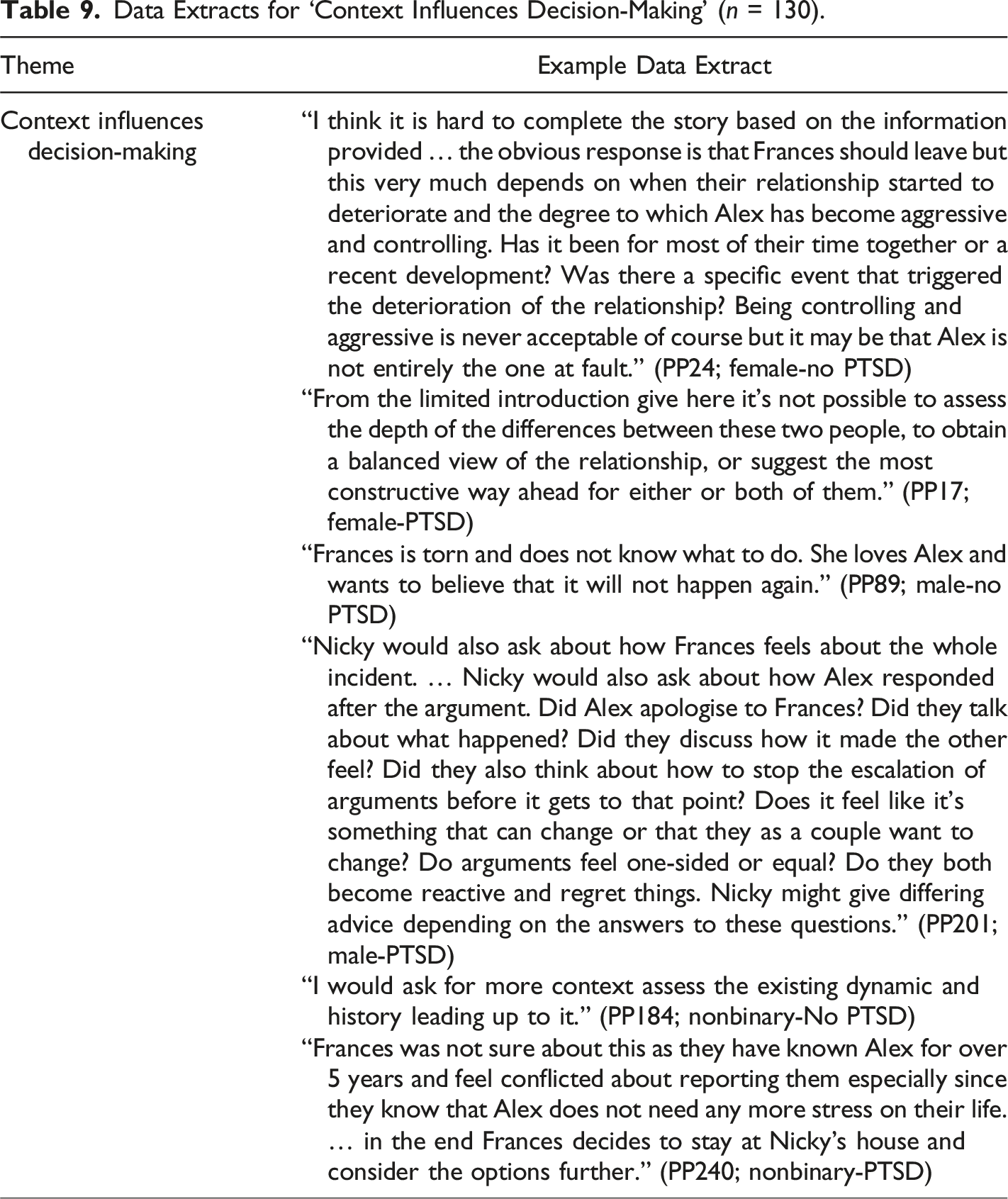
Context Influences Decision-Making
Data Extracts for ‘Context Influences Decision-Making’ (n = 130).
Discussion
The study explored how people make sense of IPV in the context of perpetrator diagnostic status (PTSD or no PTSD) and gender identity (female, male or nonbinary) by exploring IPV ratings and IPV discourses. Hypotheses were that IPV ratings and IPV discourses would vary with perpetrator diagnostic status and gender identity. IPV discourses were consistent across conditions, but discourse frequency varied by condition. IPV ratings did not vary between conditions.
Victim Gender Check
Approximately half the participants thought the victim was female versus 10% male and 2.2% nonbinary. This may suggest a narrative that IPV is more commonly experienced by women. Dominant discourses tend to position IPV victimisation as a woman’s experience (Morgan & Wells, 2016), which may influence public sense-making of IPV, and, therefore, participant responses. Some participants said the spelling of ‘Frances’ is specific to women, which may have influenced responses. There may also be a relationship between perpetrator gender and victim gender, where victim gender was assumed based on perpetrator gender and narratives regarding sexuality. As the current study only broadly investigated victim gender, future research could investigate this further.
IPV Ratings
IPV ratings did not vary with perpetrator diagnostic status or gender identity. Participants tended to appraise Alex’s behavior as abuse: responses were consistently negatively skewed, and all mean responses corresponded to ‘probably is abuse’. This is interesting when considered alongside the more nuanced responses in the story completion task, which may suggest different appraisal processes.
That neither perpetrator PTSD diagnostic status nor gender identity altered IPV ratings is interesting in the context of research suggesting that the public may use these contextual details as legitimising or excusing factors (Carlson & Worden, 2005; Lelaurain et al., 2018; Mackinnon et al., 2023). This may reflect growing public knowledge around IPV. Indeed, Women’s Aid and the National Domestic Violence Hotline have published resources regarding mental health diagnoses and IPV: both portray a clear message that the former does not excuse the latter. That such myth-challenging resources exist, however, suggests the appraisal process may be more ambiguous than the current findings imply. One may wonder what effect victim gender had on ratings, and whether specification of the gender would have affected these. Of course, it is also possible that participants appraised the behavior as abuse but still employed PTSD diagnostic status and/or gender identity as legitimising factors.
Neither personal nor professional participant IPV experience significantly affected ratings. This is inconsistent with previous findings that professional experience positively correlated with ratings (Carlson & Worden, 2005; Mackinnon et al., 2023). This may be due to the nature of the data overall as ratings were consistently weighted towards abuse.
IPV Discourses
It should first be noted that the author and supervisors’ positions are that the behavior in the story was IPV, which corroborates current definitions and perspectives in this field. This inherently influences theme identification and interpretation, and it is not possible to analyse the data without also acknowledging this influence.
Characterise the Behavior
Making sense of the behavior’s nature, details and course seemed necessary for participants to proceed. This aligns with theories that individuals name and categorise experiences according to previous knowledges and experiences (‘schemas’) to make sense of the world (McVee et al., 2005). Participants told a story about the behaviour and drew on this for clues to other related stories (e.g., what happens next, what to think or feel, how to respond).
Interestingly, participants more frequently described Alex’s behavior as ‘abusive’ or ‘domestic violence’ in no PTSD than PTSD diagnosis conditions. This suggests a specific discourse regarding PTSD and IPV: a PTSD diagnosis somehow alters what the behavior is and how it is described. It is a subtle difference as IPV ratings were consistent and there was no theme that a PTSD diagnosis excuses IPV, but language suggests that ‘abuse’ and ‘domestic violence’ feature less in public sense-making when there is a known PTSD diagnosis. This may be because the PTSD diagnosis, rather than the nature of the behavior, became the focus in these conditions. Nonetheless, this finding supports previous findings that the public may use a PTSD diagnosis as a mitigating factor for IPV (Mackinnon et al., 2023), which may or may not be conscious.
Trajectory of IPV
The discourse about how IPV unfolds over time organised advice for the immediate future and predictions about what might happen longer term. IPV escalation predictions were more frequent in no PTSD than PTSD diagnosis conditions. This may relate to the finding above: described less frequently as ‘abuse’ and ‘domestic violence’ in PTSD conditions, it would figure that IPV trajectory discourses are referenced less in this context. Other themes may also be relevant here: a greater focus on support in PTSD diagnosis conditions may have overpowered the escalation narrative. Perhaps participants assumed that, with professional support, both the PTSD and IPV would improve. Such an assumption might suggest an inextricable PTSD-IPV link in public sense-making, where IPV is perhaps thought to be symptomatic of a PTSD diagnosis.
There was concern that physical harm was likely (especially for the victim). The narratives that once is a mistake and ‘escalate’ means becomes physical may presuppose that, currently, it is not so bad. Indeed, participants gave conditional advice, offering remedies or solutions if the behavior persists. That physical abuse is necessarily ‘worse’ in public consciousness is a concern and supports previous findings that non-physical abuse is considered less abusive (Carlson & Worden, 2005; Cravens et al., 2015; Minto et al., 2020).
Show Compassion Towards Victim of IPV
Participants paradoxically showed compassion towards the victim and held the victim responsible. Sensitivity to suffering was expressed via worry and anger for the undeserving victim. Worry was greater in Male and Nonbinary-No PTSD conditions, and anger (towards Alex, on behalf of Frances and/or about the situation) was expressed only in Female conditions. Such variation suggests IPV sense-making depends on who perpetrated the IPV: by men and nonbinary individuals is seemingly anxiety-inducing, but by women is angering and unjust. Perhaps IPV perpetrated by women violates dominant discourses that victimisation, not perpetration, is a woman’s experience (Morgan & Wells, 2016). Violation of such strong narratives may also feel angering and unjust.
Attempts to alleviate or prevent suffering were expressed via recommendations and advice (e.g., leave the relationship, talk about it, seek therapy). This finding may pertain specifically to narratives about IPV disclosures and their responses (i.e., do something about abusive behavior) but may also be indicative of problem-solution narratives in general. For example, discourses may dictate that the ‘correct’ response to an identified problem is to offer a solution. This urge to solve others’ problems has been named the righting reflex and is thought to involve listener intolerance of uncertainty (Easton, 2021). This finding may also reflect growing awareness of IPV and its risks. Either way, it is reassuring given the IPV ratings: the underlying message is that it cannot or should not continue without intervention.
Hold Victim of IPV Responsible
Victim responsibility had two subthemes: responsible for the IPV itself and responsible for fixing or supporting the perpetrator. Victim responsibility for the IPV was indirectly suggested in Nonbinary-PTSD and expressed directly and consistently in all other conditions from all perspectives in the story: perpetrator, victim and outsider. As participant-generated stories reflect wider discourses and narratives regarding IPV, this finding suggests that victim-blaming IPV discourses (Lloyd & Ramon, 2016; Sprague et al., 2012; Waltermaurer, 2012) remain pervasive in public narratives.
Theorised to underpin victim-blaming, the just-world bias (JWB) refers to beliefs that people get what they deserve, so individuals blame victims to defend their worldview (Strömwall et al., 2012). Victim-blaming reportedly increases with JWB, particularly in women who are thought to defend against the idea of their own victimisation (Kristiansen & Giulietti, 1990; Strömwall et al., 2012). Gender norms may also intersect with victim responsibility: for example, being ‘a man’ by taking responsibility for a partner’s IPV (Entilli & Cipolletta, 2017), or being ‘submissive’ and meeting expectations of pervasive roles for women (Street & Dardis, 2018).
Responsibility for supporting the perpetrator was expressed more frequently in PTSD than no PTSD diagnosis conditions, and most frequently in Male-PTSD. This suggests that PTSD diagnoses, and especially men with PTSD diagnoses, alter discourses about helping responsibilities. Coupled with the victim gender check, these data may pertain to gender norms regarding help in general. Indeed, literature highlights pervasive gender roles regarding helping behavior as women are expected to provide caregiving or emotional support (Atkinson et al., 2023).
These data may also suggest that the burden of victim-blaming, and of helping responsibilities specifically when IPV is perpetrated by men with PTSD diagnoses, falls on women. Thought to be one of many social identities (e.g., gender identity, sexual orientation, race, class) that intersect to either marginalise and oppress or privilege individuals within social structures fraught with hierarchy and systemic oppression (e.g., sexism, cisgenderism) (McLeod et al., 2020), these data may reflect such subordination discourses regarding women. Caution must be exercised, however, given the earlier mentioned spelling of the name Frances, which may also have influenced these data.
Together with the compassion theme, this suggests a bind for IPV victims: they are suffering but are also both responsible for the IPV happening and, therefore, their suffering, and for providing a solution and support to the perpetrator.
Context Influences Decision-Making
Context influences decision-making was identified in both victim and outsider perspectives. In the outsider perspective, more contextual information was required before proceeding. Participants had many questions regarding the length of the relationship, the extent and duration of the behavior, how both partners feel, respond and cope with conflict and what each partner wants from the relationship. The opposite was true in the victim perspective, where they were unsure what to do and whether to take advice because of all they knew about the relationship and the perpetrator. This might make sense given the expressed worry, an emotion strongly associated with uncertainty (Freeston et al., 2020). Individuals may cope with uncertainty via over-engagement to obtain certainty (e.g., repeated questioning), under-engagement to disengage (e.g., procrastination) or ‘dither’ behaviours (e.g., inaction) that lead to uncertainty paralysis (Freeston et al., 2020). This may help explain the influence of context on decision-making in both perspectives.
Interestingly, this theme accompanied behavior characterisation, the IPV trajectory, victim responsibility and compassion towards the victim. Naming the IPV and referring to IPV discourses did not seem to enable satisfactory sense-making: despite these narratives, participants were unsure how, or reluctant, to proceed. Information seemed to strongly influence, even cloud, decision-making. Research reports similar findings. Thought to have implications for decision-making, individuals were repeatedly more likely to engage in ‘additive’ problem-solving (adding more components to a problem situation) than the advantageous subtraction of components (Adams et al., 2021).
Findings told a story about how people make sense of IPV. They tended to appraise it as abuse regardless of perpetrator diagnostic status or gender identity. They communicated narratives about behavior characterisation, an IPV trajectory, compassion towards the victim, victim responsibility and the influence of context on decision-making.
Limitations
Online data collection may have simultaneously facilitated and hindered accessibility. Although UK-wide participants were recruited, online collection privileges IT-literacy and internet accessibility. Second, women were overrepresented in the sample. Findings may not generalise to other gender identities. Third, story completion (SC) may privilege individuals with certain life experiences or education that enables experiences of storytelling and story-writing. SC may not have made sense without these experiences. SC also requires imagination and the ability to think creatively with minimal information and prompts, which may not be accessible for all. Fourth, participant perceptions of perpetrator gender were not checked. Inclusion of a manipulation check would improve finding robustness. Finally, asking participants whether the behavior was IPV may have produced framing effects and influenced ratings. One may wonder why a question is asked at all if it were not relevant in the first place.
Future Research
Further exploration that physical IPV is necessarily more damaging than other forms should be prioritised. As this suggests non-physical IPV is less serious or warrants less immediate action, research should explore the pervasiveness of this narrative and whether it also exists among helping services (e.g., healthcare, police and criminal justice systems).
Future research should also explore IPV discourses about victim gender. Figures suggest IPV disproportionately affects women and gender minority individuals (WHO, 2012). Indeed, victimisation has been positioned as a woman’s experience in public discourses (Morgan & Wells, 2016), which may influence public sense-making of IPV. Is it still IPV if the victim is not a woman? Exploration of victim gender identity effects may provide further insight into discourses about who experiences IPV. Research should also explore victim and perpetrator gender identities together. Research highlights the roles of heterosexism and gender role socialisation in IPV sense-making in both same-gender couples and couples in which the perpetrator is a woman and the victim a man (Brown, 2008). This would be helpful for policy makers and the justice system to understand as narratives may influence IPV disclosures and responses.
Discourses regarding IPV and PTSD diagnoses should also be explored. IPV was described less as abuse or domestic violence in the context of a PTSD diagnosis, suggesting a possible unconscious mitigating of IPV. Finally, it would be helpful to further explore experiences and discourses among men and gender nonbinary individuals.
Implications and Recommendations for Practice
Findings suggest further public information is needed regarding IPV and its different forms. Although ratings skewed towards abuse, escalation and physical harm narratives suggest public discourses may prioritise physical abuse. Given the UK Government definition was recently republished to include coercive control and financial abuse (Home Office, 2020a), it would be helpful to further publicise this to update public discourses.
Attention should also be paid to the narrative that context influences decision-making. In clinical practice this may look like awareness of risk or safeguarding issues, but uncertainty about how to proceed without first establishing further details, or because of the degree of detail already known. One would hope there are clear protocols to follow to protect safety that are less influenced by contextual factors. Further exploration, education and/or training may be useful in clinical practice. It may also be helpful to provide clinicians with training and/or resources to facilitate identification of IPV with clients and patients.
Finally, public information and professionals’ training is needed regarding help-seeking responsibilities in IPV. Findings suggest IPV victims are suffering but responsible for the IPV and the solution, and the burden of this responsibility may fall on women when IPV is perpetrated by men with PTSD diagnoses. Training for professionals may be helpful regarding the potential gender bias in helping responsibilities and the importance of supporting victims to help themselves rather than feel responsible for supporting perpetrators. Public information on accountability and help-seeking in IPV is also needed to update public discourses and free victims from the bind in which such discourses place them.
Conclusions
The study explored how people make sense of IPV by looking at IPV ratings and IPV discourses in the context of perpetrator PTSD diagnostic status and gender identity. IPV ratings did not vary with PTSD diagnostic status or gender identity. Frequency of IPV discourses identified in all conditions did vary. Discourses suggest that context influences decision-making even when IPV is named; a PTSD diagnosis reduces the likelihood that IPV is described as abuse or domestic violence; and escalation equates to physical harm and help is needed, but the responsibility falls on the victim. Public information campaigns are recommended to clarify the nature of IPV, who is responsible and who should seek help and how.
Supplemental Material
Supplemental Material - How Do People Make Sense of Intimate Partner Violence (IPV) in the Context of Perpetrator PTSD Diagnostic Status and Gender Identity?
Supplemental Material for How Do People Make Sense of Intimate Partner Violence (IPV) in the Context of Perpetrator PTSD Diagnostic Status and Gender Identity? by Ella Lonnen, Jessica Mackinnon, and Rachel Paskell in Psychological Reports
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
Note
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.