
Abstract
Intimate Partner Violence (IPV) represents a significant public and social health concern and may present particular complexities in military veteran relationships which are subject to unique stressors including separations, transition to civilian life and increased risk of Post-Traumatic Stress Disorder (PTSD). Public understanding is vital in terms of ensuring access to services and appropriate intervention. However, little is known about the public perception of IPV in this context. This study sought to assess how public recognition and discourse is affected by military veteran status and a diagnosis of PTSD. Community participants (N = 269) were randomly allocated to one of four conditions and presented with a story containing IPV in which the profession (military veteran/civilian worker) and diagnostic status (PTSD/No PTSD) were manipulated. All participants rated the extent to which they felt the story contained IPV; additionally, half (n = 123) took part in a story completion task designed to elicit qualitative data with regards to public discourse. The mean scores in all conditions were weighted towards IPV recognition. Results indicated a small interaction between job role and PTSD (F[1265] = 7.888, p < 0.01, partial n2 = 0.029) meaning that the public are more likely to recognise IPV when it is perpetrated by a military veteran than a civilian with PTSD. Diagnostic status made no difference to recognising abuse perpetrated by a military veteran. However, the fit of the model was weak (r2 = .040) meaning that the large majority of variance was due to factors not accounted for. Qualitative findings indicated that in a military population trauma may be assumed even where not indicated and the public appear less likely to consider current stressors or acknowledge that PTSD cannot justify abuse. Victims of IPV in military relationships may therefore be particularly vulnerable to discourses that prioritise the victim status of the perpetrator.
Introduction
The Ministry of Defence (2018) has identified the need for specialist strategies to address Intimate Partner Violence (IPV) within military communities. The extent to which rates of IPV are higher in the military is unclear (Kwan et al., 2020; MacManus et al., 2022; Rentz et al., 2006; Sparrow et al., 2018; Taft et al., 2011). However, there is strong evidence that where it does occur the risk of physical harm is greater (Aronson et al., 2014; Hoyt et al., 2014).
Military relationships may be subject to unique stressors such as long periods of separation, frequent relocation and financial dependency (Jones, 2012), which can continue to play out long after a person has retired from service (Burland & Lundquist, 2013; Sparrow, et al., 2017). As a necessity, military culture normalises the use of instrumental violence (Bradley, 2007), which may generalise across contexts (Jones, 2012; Lysova and Straus, 2019), with combat experience being a specific risk factor (Kwan et al., 2018). Hyper-masculine ideals may also foster abuse (Herrero et al., 2017; Taft, Watkins et al., 2011). A further complexity is the role of post-traumatic stress disorder (PTSD), which occurs at a higher rate in the military than in the general population, and at higher rates in veterans than serving personnel (NHS Digital, 2014; Stevelink et al., 2018).
The interplay between PTSD and IPV has significant implications for intervention. Mental distress may be particularly stigmatised in military culture, preventing people from accessing treatment (Aronson et al., 2014; Cornish et al., 2014; Greene-Shortridge et al., 2007; Silvestrini & Chen, 2022) but trauma symptoms, in turn, may limit the efficacy of IPV intervention (Taft, Wadswirth et al., 2011). Military personnel may be most likely to disclose psychological difficulties to family and friends (Stevelink et al., 2019); thus, the social network around a military couple can be vital in facilitating access to services (Aronson et al., 2014). As such, public understanding with regards to IPV and PTSD in this community demands attention.
Public understanding, that is to say the general, non-expert population’s understanding of IPV is well evidenced – with physical and sexual abuse particularly recognised as unacceptable (Carlson & Worden, 2005). Demographics such as age, gender, ethnicity, and experience of IPV may have some bearing on beliefs, although findings are inconsistent and risk stereotyping groups (Gracia & Tomás, 2014; Wagers et al., 2017; Worden & Carlson, 2005).
More convincing is the evidence that public understanding of IPV is mediated by contextual factors, such as the relationship between the perpetrator and victim, leading to what Lelaurain et al. (2018) term ‘conditional logics’ by which the public navigate ambivalence regarding abuse by citing factors which minimise or legitimise behaviour (Carlson & Worden, 2005; Sorenson & Thomas, 2009; Taylor & Sorenson, 2005; Worden & Carlson, 2005). Public discourse is also reproduced across health and social care settings by professionals who inevitably act from within their social context (Bradbury-Jones et al., 2014; Buck & Collins, 2007; Ramsey et al., 2012; Saletti-Cuesta et al., 2018).
Therefore, there are indicators that myths that legitimise abuse may remain latent if not overt in public and professional discourse (Lelaurain et al., 2018; Refuge, n.d.) with concerning implications for disclosure and access to support (Barnett, 2001; Bradbury-Jones et al., 2014). However, little is known about the way in which understanding of the specific issues facing military veteran couples intersects with wider public discourse. Conceivably, abuse may be reframed through the lens of trauma (Worden & Carlson, 2005); equally, ideas regarding military culture as aggressive (Taft, Watkins et al., 2011) may align with broader ideas about who perpetrates violence and why. The role of social discourses in personal and professional support is particularly pertinent given the role of civilian services who are required to support veterans but may lack understanding of the military context (Home Office, 2020). Research is therefore needed in order to inform campaigning and intervention with the veteran community.
Current Study
The current study aims to consider two key factors that may impact on IPV recognition and discourse in the general public; namely, (a) PTSD and no PTSD diagnosis, and (b) across military veteran and civilian status in a general sample. As a scoping study, no prediction as to direction of effect was possible. Instead, two broad hypotheses were made: 1. Public recognition of an incident as a form of IPV will be affected by: a. Whether the perpetrator is a military veteran or a civilian worker. b. Whether the perpetrator has a diagnosis or no diagnosis of PTSD. 2. Public discourse regarding an incident of IPV will be affected by: a. Whether the perpetrator is a military veteran or a civilian worker. b. Whether the perpetrator has a diagnosis or no diagnosis of PTSD.
The study also considered variance in recognition of IPV due to participant demographic factors and relevant experience in line with the wider literature (Carlson & Worden, 2005). However, given the mixed findings no hypotheses were made regarding presence or direction of an effect.
Method
Ethical Approval
The study received ethical approval from The University of Bath Psychology Department Research Ethics Panel (reference 19–282).
Design
The study employed a cross-sectional, between groups, mixed methods design. All participants completed a quantitative measure. In order to limit risk of saturation and in line with recommendations for the methodology used (Clarke et al., 2017) half were then randomly allocated to complete an additional qualitative task.
Participants
Adults aged 18 years and over, and currently residing in the UK were recruited via the University of Bath Department of Psychology study participation panel, on social media (Facebook and Twitter) and using snowball sampling (N = 269).
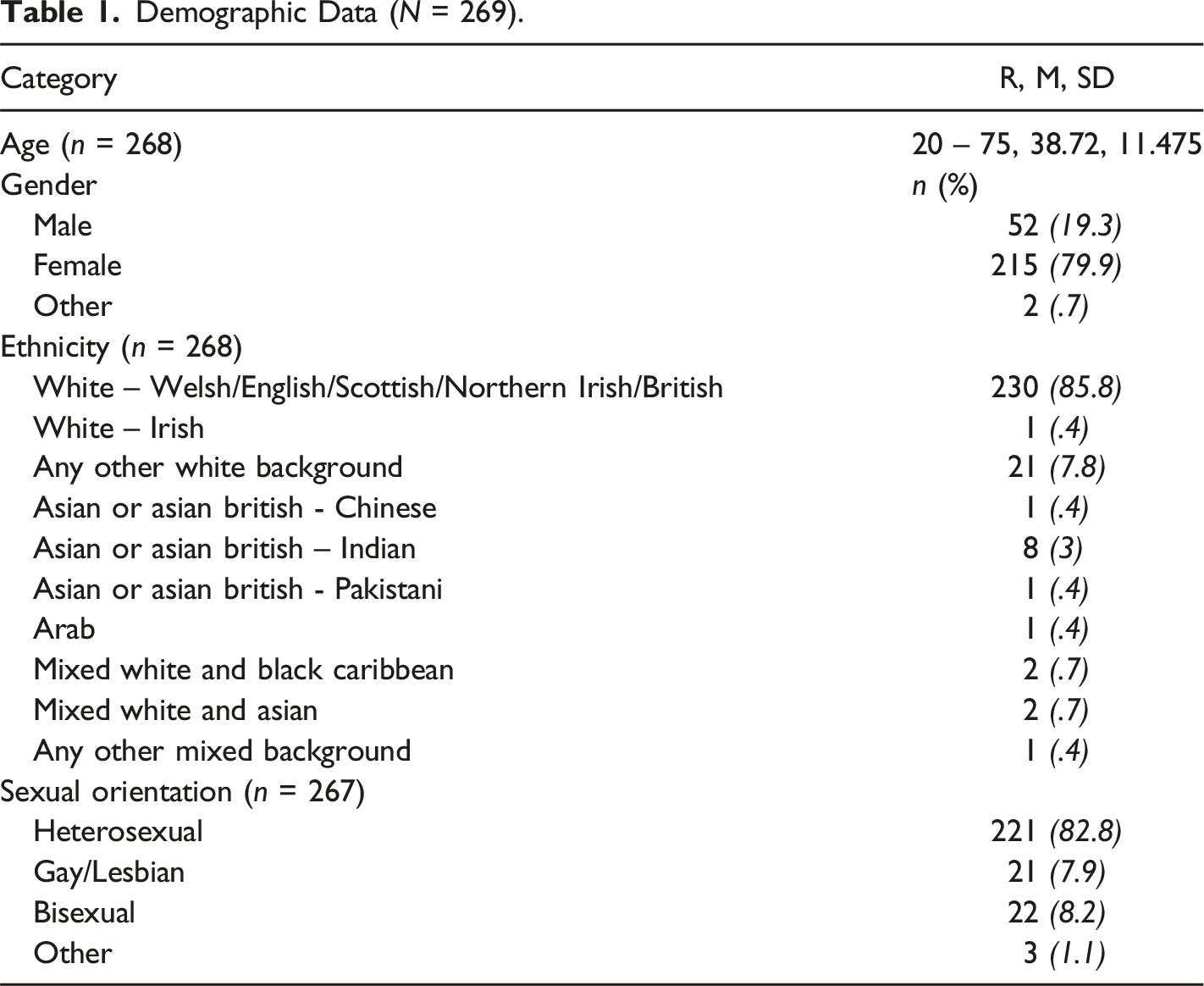
Demographic Data (N = 269).
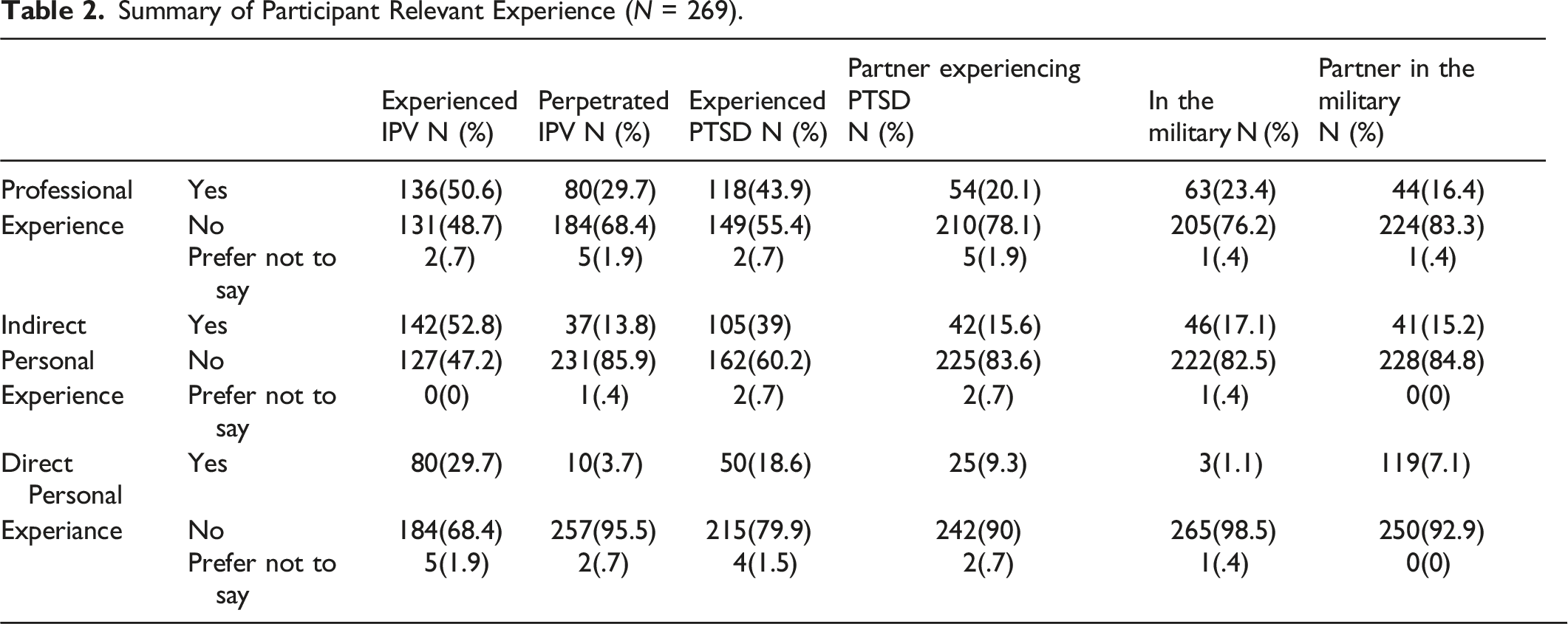
Summary of Participant Relevant Experience (N = 269).
Measures
A rating scale and a story completion task were designed for specific use in this study.
Intimate Partner Violence Rating Scale
Participants were asked to rate the extent to which they thought the behaviour described in the study story constituted IPV using a Likert scale of 0–10 (recorded to one decimal place) where 0 = definitely not abuse, 5 = not sure if abuse and 10 = definitely is abuse. This aimed to test the hypothesis that the status of a perpetrator as a military veteran experiencing PTSD would impact upon recognition of IPV.
Story Completion Task
This asked the participants to complete an unfinished story imagining that they were offering advice as a friend of the victim. This generated textual data for qualitative analysis focused on public discourses about military veteran status and diagnosis of PTSD in an incident of IPV.
Procedure
The study was hosted online by Qualtrics. Participants were recruited via a UK university research community participation panel, social media (Twitter and Facebook), and using snowballing. The study focus was described as ‘work, wellbeing and relationships’ in order to limit priming with regards to IPV content. An information page provided further limited details including a warning that participants would be requested to read an account of an argument in which a man becomes very angry, bearing in mind the potential to cause distress. Following informed consent, demographic information were collected. Participants were then randomly allocated to one of the four conditions: • Condition 1: Military Veteran, PTSD (COND1 MVet PTSD) • Condition 2: Military Veteran, No PTSD (COND2 MVet NPTSD) • Condition 3: Control (Construction Worker), PTSD (COND3 ConW PTSD) • Condition 4: Control (Construction Worker), No PTSD (COND4 ConW NPTSD)
Construction work was identified as the civilian role (control) with parallels in terms of being a male dominated industry with positions across social class and educational attainment.
In each condition all participants were first asked to read the study story. The story described a married heterosexual couple, Danny and Naomi, having an argument during which Danny, having hidden Naomi’s phone, then punched a wall and threw the phone in her direction. The story ended with Naomi describing the incident to her friend Steph and asking for advice. The story thus contained evidence of IPV, namely control (hiding the phone) and physical threats (punching the wall and throwing the phone). In each condition the story was identical except for the job role and diagnostic status of Danny, which were manipulated as previously outlined.
Half of the participants in each condition were next randomly allocated to the story completion task. Story completion is a novel method for generating qualitative data. It is well suited to between groups comparison as IVs can be manipulated within story prompts. It also provides a distancing effect allowing sensitive subjects to be more safely explored and potentially limiting desirability affects which can be a concern in the wider IPV literature (Clarke et al., 2017; Visschers et al., 2017). Participants were asked to complete the story as if they were Steph, responding to Naomi’s request for advice and were instructed to write at least 10 lines in order to generate rich data for qualitative exploration.
All participants were then requested to complete the IPV rating scale and relevant experience questionnaire. At every stage, an ‘exit study’ button was available, redirecting participants to a debrief page, that included details of relevant agencies, thereby ensuring that it was possible to access support without needing to complete the study. The debrief page was made available to all participants following study completion.
Data Analysis Plan
Quantitative data
Exploratory analysis identified outliers in Conditions 1 and 3, negative skew across all four conditions, and kurtosis in Condition 1. As such, assumptions of normal distribution were not met. However, given the mixed evidence as to the requirement of normal distribution when calculating an F-statistic (Field, 2018) and debate as to acceptable levels of skew and kurtosis (Bandalos, 2018; Morgan et al., 2000), a 2 X 2 ANOVA was employed to calculate main and interactive effects of Job Role (Military Veteran/Construction Worker) and Diagnostic status (PTSD/No PTSD) (independent variables) on IPV rating (dependent variable). In order to enhance robustness, parameter estimates were based on 1000 bootstrapped resamples (Field, 2018). Simple effects were then calculated using independent t-tests, bootstrapped at 1000.
A secondary analysis was completed in order to identify any significant impact of demographic or relevant experience variables on IPV rating. An ANCOVA (with parameter estimates bootstrapped at 1000) was performed with each variable entered into the model separately. Again, significant findings were followed up with a calculation of simple effects using independent t-tests bootstrapped at 1000.
Qualitative data
Data were uploaded to NVivo and analysed first using thematic analysis as outlined by Braun et al. (2015) in order to explore public discourse with regards to IPV and any impact of military veteran status and PTSD diagnosis. The first author immersed themselves in the data before identifying initial extracts across all four conditions relevant to the research question and labelling initial codes. Codes were then drawn together into themes and sub-themes. The data was next split according to condition and cross-referenced with the initial themes to check that meaning was adequately captured and no condition specific themes were missed. In line with Terry et al., (2017) the analysis was understood as inherently a process of construction meaning that secondary ratings would not necessarily add to the validity of findings. Instead the primary author participated in supervisions with the second author, reflecting upon data representation and relevance. Finally, frequency analysis of coding was completed in order to identify any differences between groups in terms of the prominence of themes.
Results
Results with regards to, first, the quantitative analysis of the IPV rating and, second, the qualitative analysis of the story completion task are presented below.
IPV Rating
Summary Statistics (N = 269).
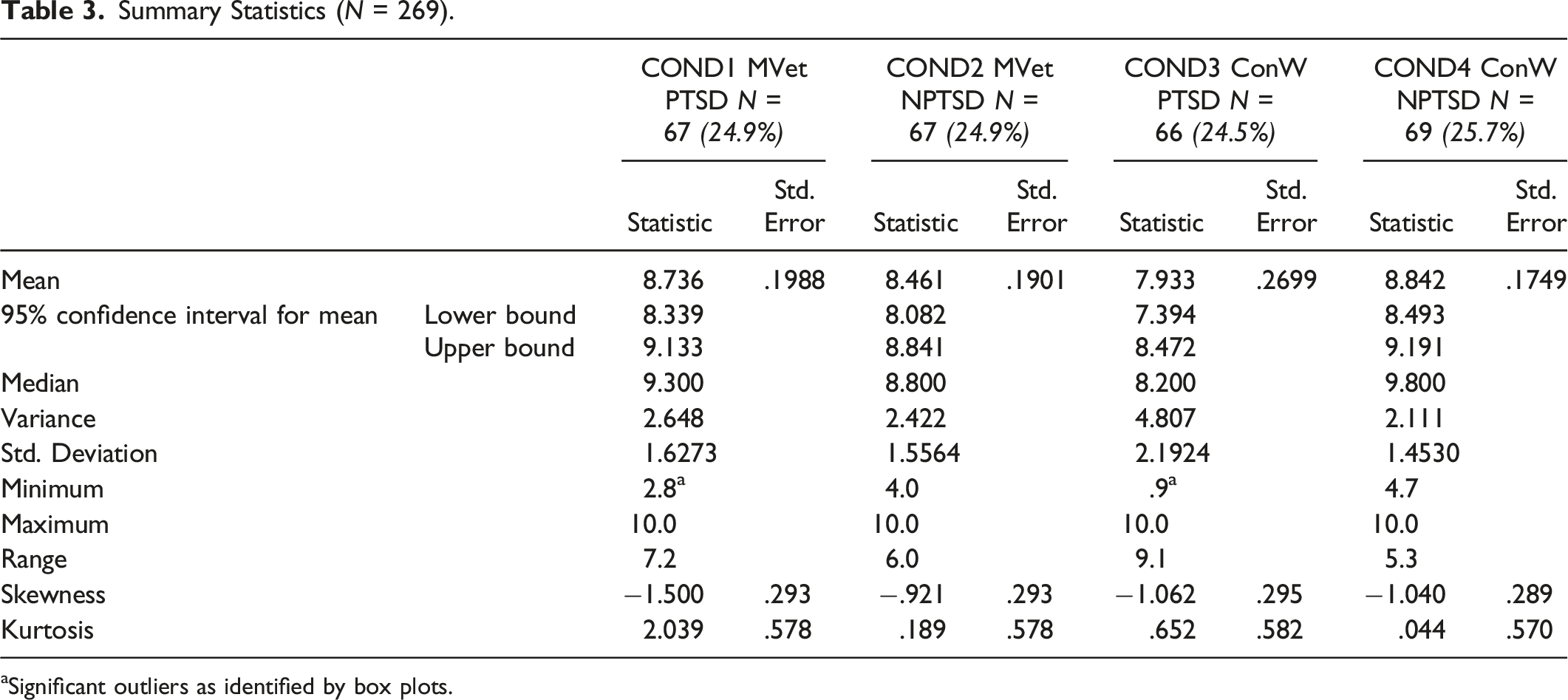
aSignificant outliers as identified by box plots.
Analysis of Main and Interactive Effects.
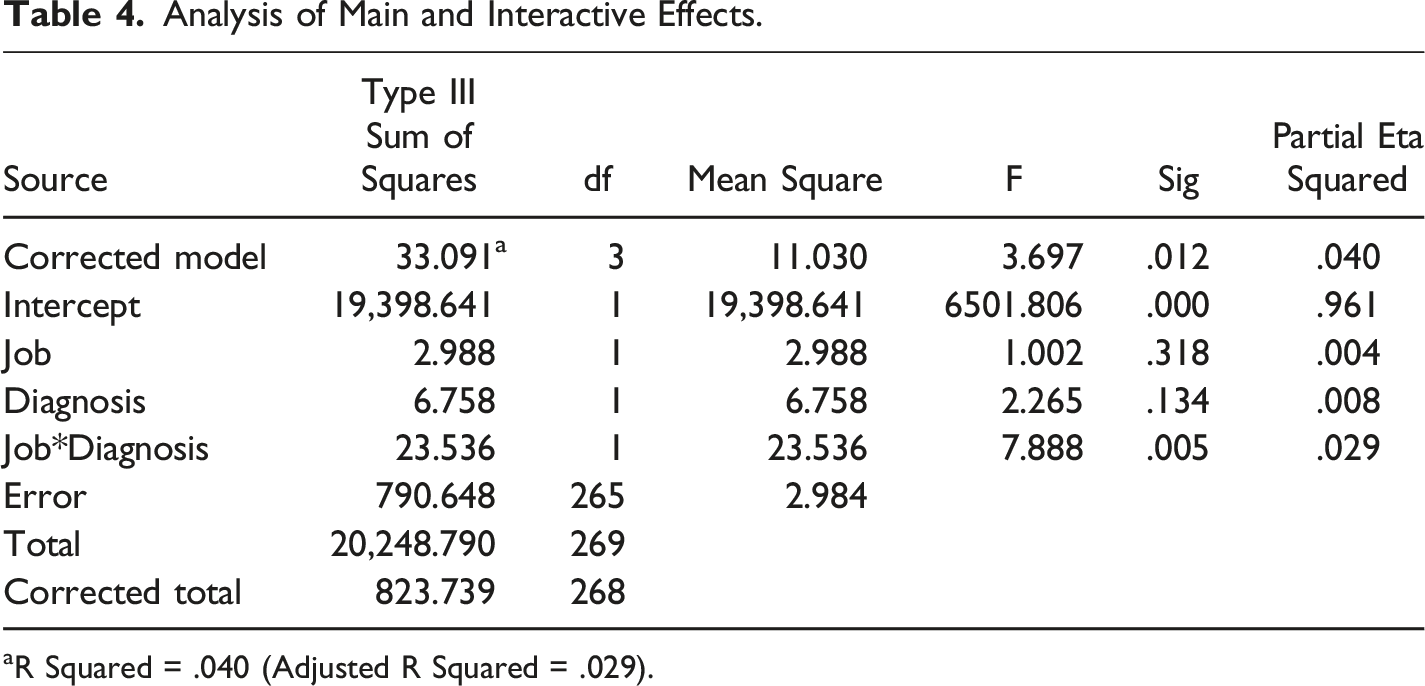
aR Squared = .040 (Adjusted R Squared = .029).
Tests of Simple Effects.
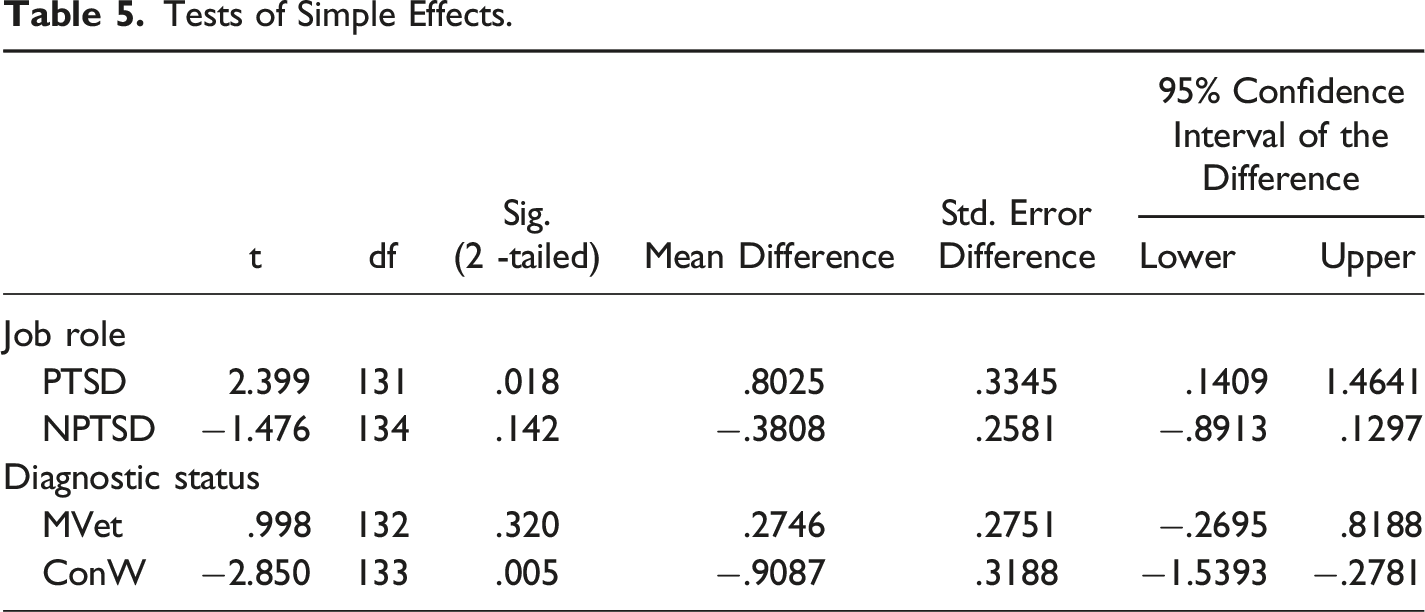
Diagnostic status had no significant impact in the MVet group (t[1132] = 0.998, p > 0.05) meaning that participants were equally likely to identify IPV perpetrated by a MVet whether or not they had a diagnosis of PTSD. However, in the ConW group a significant difference was found (t[1133] = -2.850, p = 0.005) with participants giving a higher IPV rating where there was no diagnosis of PTSD. This means that when the perpetrator was a ConW the participants were more likely to recognise IPV when there was no diagnosis of PTSD.
Covariates
Analysis of Covariance With Professional Experience of Working With People who Have Experienced IPV as a Covariate.
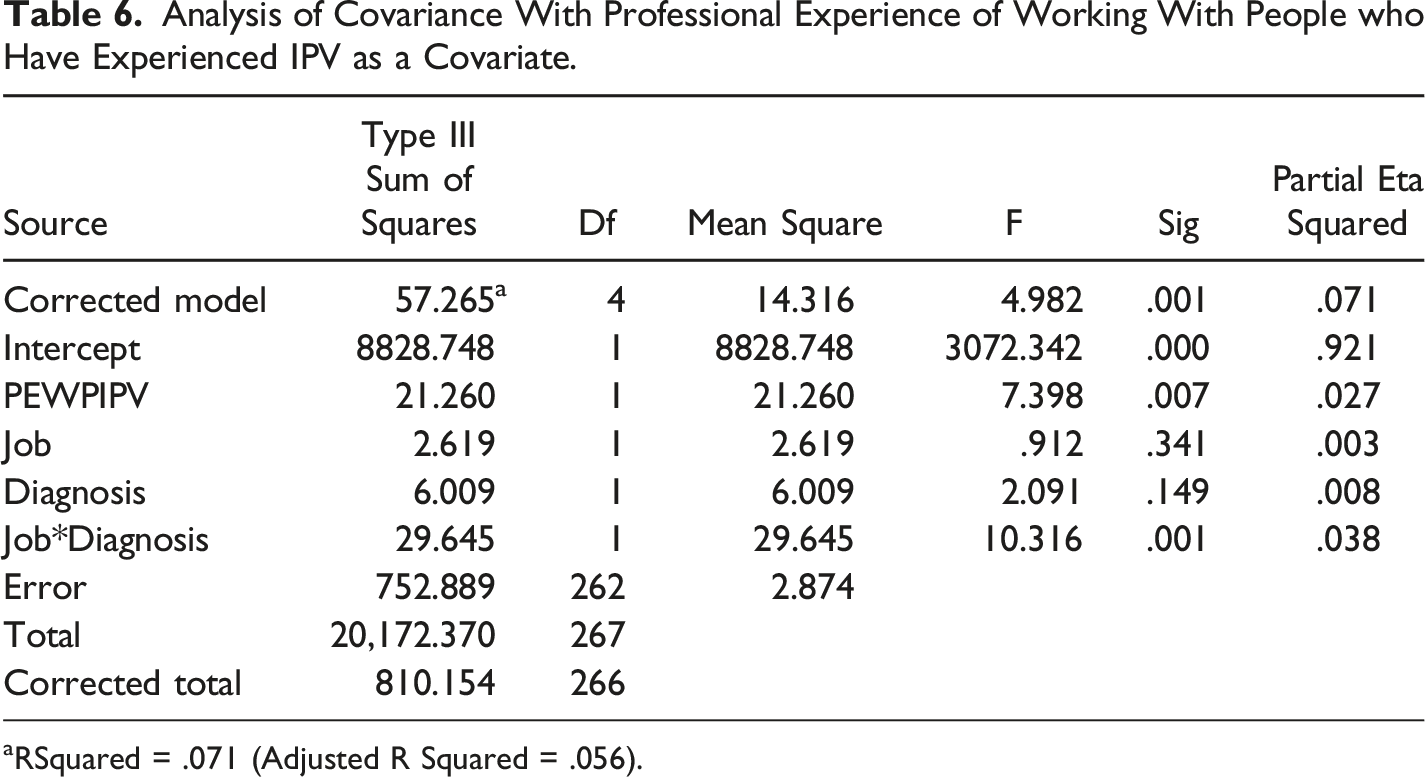
aRSquared = .071 (Adjusted R Squared = .056).
An independent t test (bootstrapped at 1000) was performed in order to identify the direction of the relationship between PEWPIPV and IPV rating. It was found that people who did have professional experience provided a significantly higher rating (t[265,1] = -2.527, p = 0.012). Assumption of homogeneity of regression slope was met. This means that participants who had professional experience in the IPV field were more able to recognise IPV.
Story Completion Task
Data extracts for ‘Describing the Behaviour’.
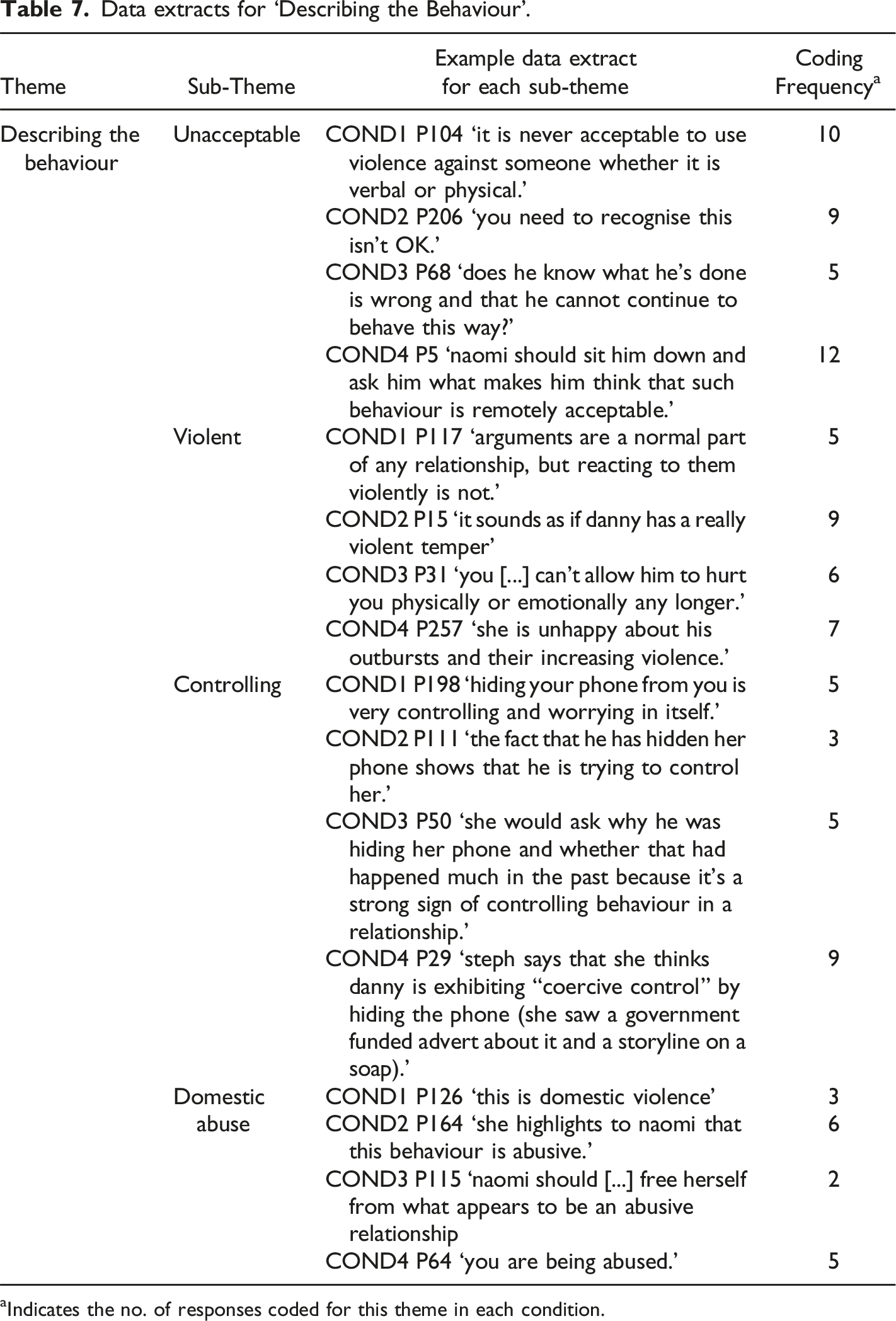
aIndicates the no. of responses coded for this theme in each condition.
Data extracts for ‘Causes of the Behaviour’.
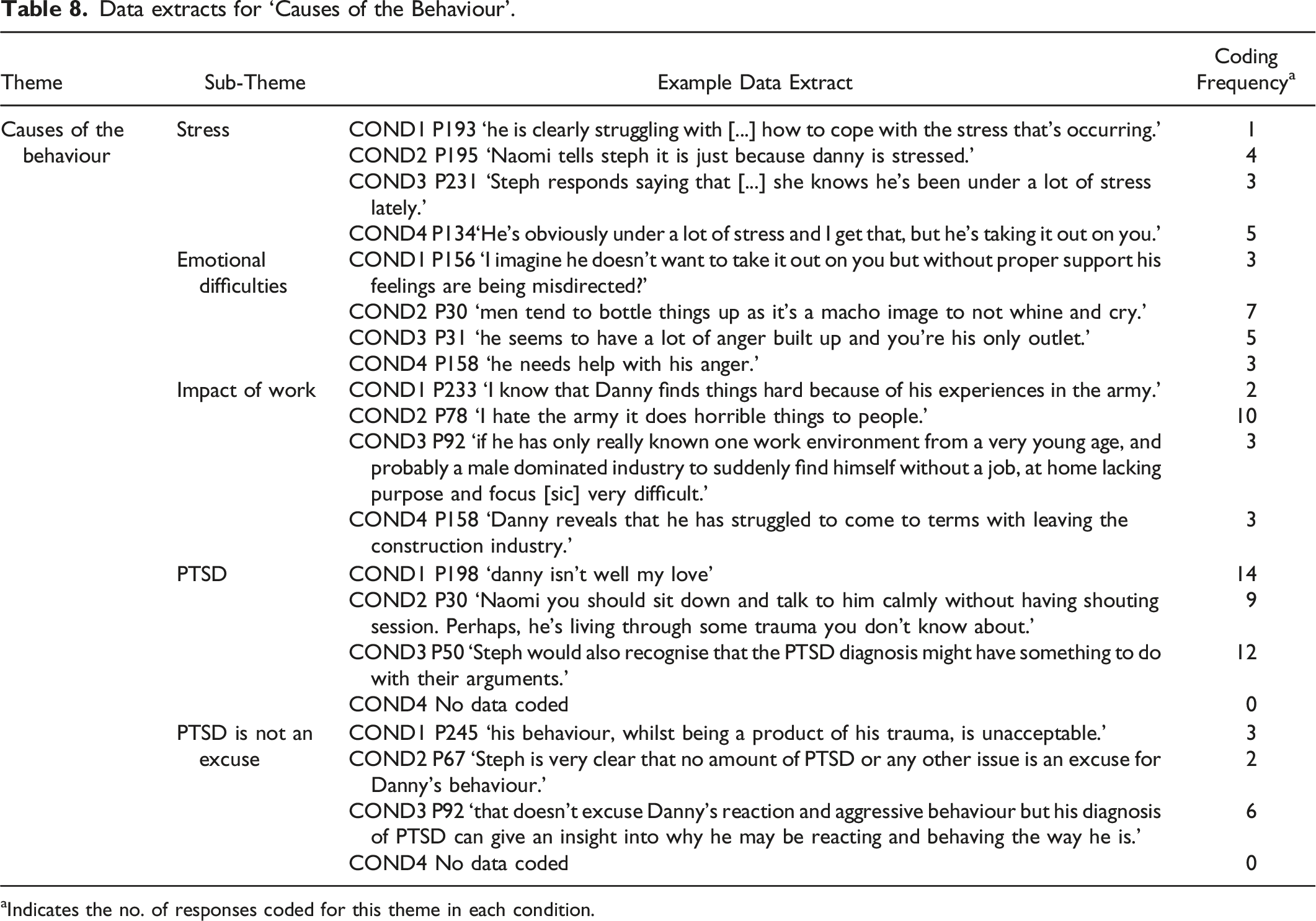
aIndicates the no. of responses coded for this theme in each condition.
Data extracts for ‘Solutions to the Behaviour’.

aIndicates the no. of responses coded for this theme in each condition.
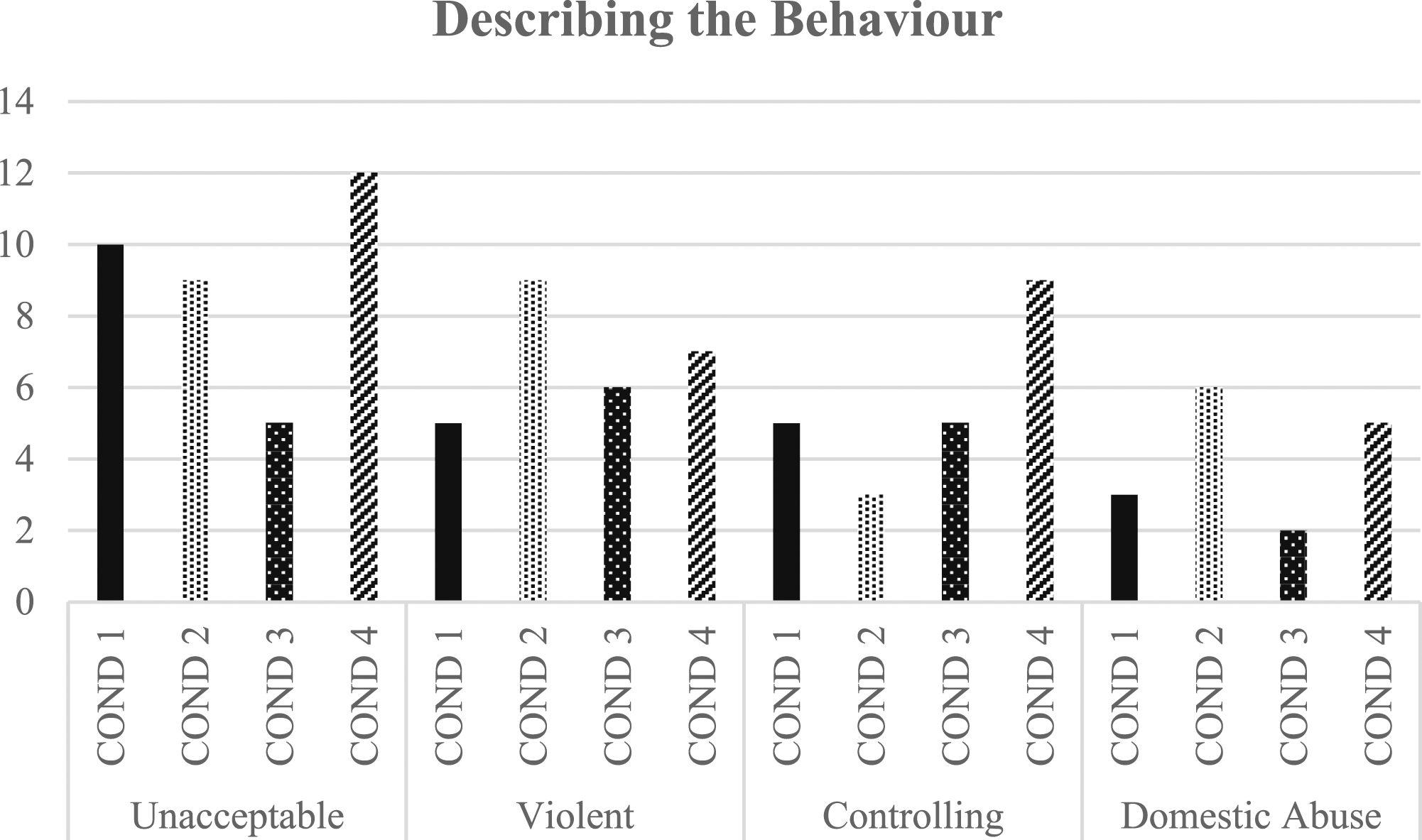
Frequency of coding between groups for ‘Describing the Behaviour’.
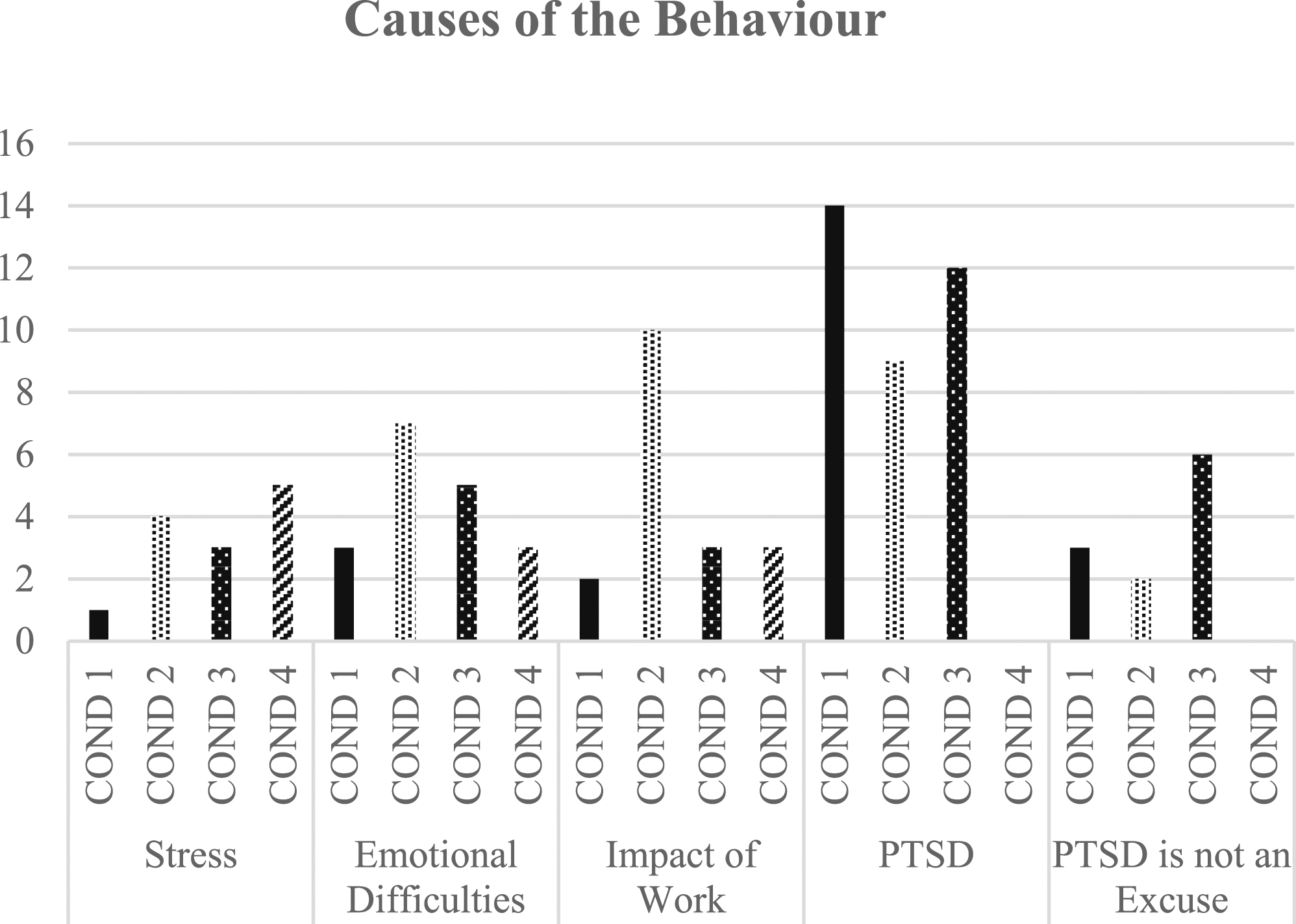
Frequency of coding between groups for ‘Causes of the Behaviour’.
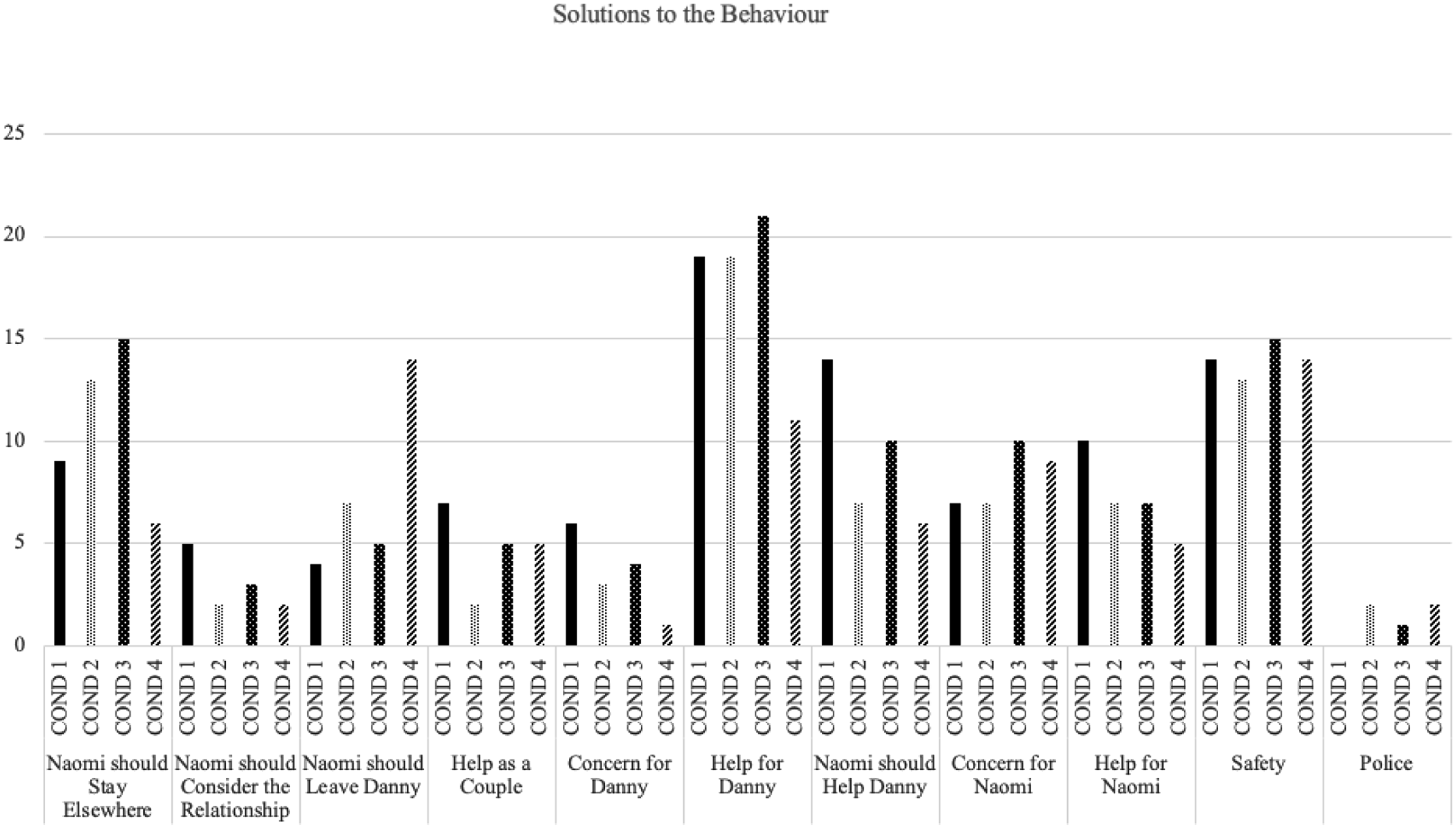
Frequency of coding between groups for ‘Solutions to the Behaviour’.
Describing the Behaviour
Participant responses consistently included a description of Danny’s behaviour with four themes identified with regards to this description: Danny’s behaviour was (a) unacceptable; (b) violent; (c) controlling; and (d) domestic abuse.
Participants described Danny’s behaviour as ‘unacceptable’ although this was less common in COND3 (ConW PTSD). Participants commented upon the aggression, and ‘violence’ displayed by Danny. Some also reflected on the element of control. Interestingly, participants in COND4 (ConW NPTSD) commented more on control than on violence. A few participants used ‘domestic abuse’ or a related term to directly label the behaviour, though this was slightly more frequent in COND2 and COND4 where there was no diagnosis of PTSD.
Causes of the Behaviour
Participants attempted to contextualise Danny’s behaviour, drawing on the story to identify a cause. Themes were: (a) stress; (b) emotional difficulties; (c) the impact of work; (d) PTSD; and (e) PTSD is not an excuse.
In all four conditions participants described how Danny’s behaviour should be understood in the context of ‘stress’. Responses suggested emotional difficulties such as ‘anger’ or a ‘difficulty expressing feelings’ might also be a root cause. The impact of work was again suggested in all four conditions though particularly in COND2 (MVet NPTSD). In COND1 (MVet PTSD), 2 (MVet NPTSD) and 3 (ConW PTSD) participants described how PTSD, trauma and mental ill-health may be causing IPV. However, in each, and most frequently in COND3 (ConW PTSD), a smaller number also suggested that PTSD should not be considered an ‘excuse’.
Solutions to the Behaviour
Participants offered solutions to Naomi according to two themes: (a) The Relationship, and (b) Help. Further subthemes identified within ‘The Relationship’ were ‘Naomi should Stay Elsewhere’; ‘Naomi should Consider the Relationship’ and ‘Naomi should Leave Danny’. Within the theme of Help, sub-themes were Help as a Couple; Concern for Danny; Help for Danny; Naomi should Help Danny; Concern for Naomi; Help for Naomi; Safety and Police.
The Relationship
Participants across the conditions suggested that Naomi should consider staying elsewhere, most indicating that this should be temporary, in order to have time to think. A smaller number suggested that Naomi should consider the future of the relationship, and more explicitly that she should consider permanently leaving Danny, particularly in COND4 (ConW NPTSD).
Help
Some participants suggested that Naomi and Danny should attend couples’ therapy. More often however, responses expressed concern for Danny and indicated that he required individual support, usually via a GP or therapist, though these themes were less frequent in COND4 (ConW NPTSD). Again, in all conditions but particularly COND1 (MVet PTSD) participants suggested that Naomi should take some responsibility for helping Danny either directly, or indirectly by accessing him professional input.
Concern was expressed for Naomi across all four conditions, with the suggestion that she too should access support such as therapy or via domestic abuse charities. However, help for Naomi was a less frequent theme than help for Danny and it was not always clear whether the help should be for her own needs, or to improve her capacity to support Danny. In all four conditions participants questioned Naomi’s safety, often noting the risk of escalating violence. A small number of participants, except in COND1 (MVet PTSD) indicated that Naomi should contact the police.
Discussion
The aim of this study was to investigate public understanding of IPV in the context of military veteran status and a diagnosis of PTSD. The study predicted that the extent to which the public recognise an incident of IPV would be affected by whether a perpetrator is a military veteran with a diagnosis of PTSD when compared to a military veteran without PTSD, a civilian worker with PTSD and a civilian worker without PTSD. This prediction was only partially met.
Whilst job role and PTSD diagnosis were not found to impact independently, a small interaction between the two was found. Although only trending towards significance it is interesting to note that where an individual has a diagnosis of PTSD, their status as a military veteran makes it more likely that the public will recognise IPV compared to a civilian. Assumptions may be made about the abusive potential of veterans, perhaps drawing on discourses regarding aggression in the military (Taft, Watkins et al., 2011), in spite of the evidence which indicates equal rates of IPV in the general population. In turn, this stigmatisation may lead to a stereotyping effect by which abuse is normalised within the cohort.
The presence of PTSD made no difference to recognising abuse perpetrated by a military veteran (compared to no-PTSD/MVet). This was unexpected given the evidence elsewhere that mental ill-health may be used to minimise abuse (Lelaurain et al., 2018). However, the story completion responses indicated that trauma was assumed even where not indicated meaning that the experimental manipulation may not have been effective. As such, the public perhaps make assumptions about military service leading to PTSD, and further that this then explains IPV. An effect of PTSD diagnosis was found in the construction worker condition with participants more able to recognise IPV in the absence of PTSD diagnosis. This is an important finding indicating that the public may conceive of the diagnosis as a mitigating factor in terms of recognising and so reporting abuse in civilian relationships.
The findings add to the growing evidence that demographic factors may not significantly impact upon understanding of IPV (Carlson & Worden, 2005) and demonstrate that this finding holds true in the context of military veteran status and PTSD. The only experiential factor shown to relate was professional experience of working with people who have experienced abuse. Interestingly, this is distinct from the work of Carlson and Worden (2005) who grouped both professional and indirect personal experience together, and found a correlation with abuse recognition. It is of note that professional experience of working with PTSD or in a military context did not improve recognition. This may highlight limited understanding in these professions, as has been more widely researched in health and social care sectors (Bradbury-Jones et al., 2014; Buck & Collins, 2007; Johnson et al., 1994; Ramsey et al., 2012; Robinson et al., 2018; Saletti-Cuesta et al., 2018).
The secondary hypothesis of this study was that military veteran status and diagnosis of PTSD would impact on public discourse with regards to IPV. Again, this hypothesis was only partially met. Thematic analysis of the story completion task did not lead to any themes unique to the interaction of military veteran status and a diagnosis of PTSD. Nonetheless, findings contribute to the more general literature and furthermore the frequency analysis identified themes that may be particularly pertinent to discourse regarding IPV in this cohort.
In line with Carlson and Worden (2005), findings indicated that the public identify threatening and controlling behaviour (perpetrated by a husband towards his wife) as unacceptable. However, seen alongside the IPV rating analysis, lack of acceptability does not necessarily tally with absolute confidence that behaviour constitutes abuse. This discrepancy confirms findings elsewhere (Carlson & Worden, 2005) and is concerning given the evidence that victims may require social and professional support in order to identify experiences as domestic abuse (Barnett, 2001; Bradbury-Jones et al., 2014).
A related concern is that participants tended to focus more on the acts of physical aggression than the controlling behaviour, particularly where a diagnosis of PTSD was indicated or assumed. This suggests that both in the military veteran context and more widely a diagnosis of PTSD may lead people to focus on physical risk, as has been found elsewhere (Robinson et al., 2018; Taylor & Sorenson, 2005) and helps to make sense of the uncertainty many participants demonstrated on the IPV rating scale. Given that abuse rarely begins with overt physical harm (Barnett, 2001), the finding suggests that the public, including professionals, may not recognise early indicators of abuse and act on them prior to escalation.
In terms of understanding the cause of IPV, the study found clear evidence of ‘conditional logic’ (Lelaurain et al., 2018) by which participates contextualised abuse. A new finding is the extent to which PTSD is used to frame IPV both in military relationships and more generally as borne out in the significantly lower IPV recognition when the perpetrator was a construction worker with PTSD compared to one without. Furthermore, in a military context the public appear less likely to consider current stressors or acknowledge that PTSD cannot justify abuse. Victims of IPV in military relationships may therefore be particularly vulnerable to discourses that prioritise the victim status of the perpetrator. This aligns with emerging evidence that military partners can feel obliged to support perpetrators experiencing post-conflict distress (Finley et al., 2010; Gray, 2015), thereby limiting social support and help-seeking.
Public discourse regarding solutions to IPV is an under-researched area (Taylor & Sorenson, 2005) and the findings here offer a number of useful insights. PTSD diagnosis (stated or assumed) appeared to focus participants on the needs of the perpetrator, meaning that victims in military veteran relationships may be particularly vulnerable to having their needs overlooked.
Victim safety was raised by participants across conditions and so it is interesting to note that contacting the police was rarely mentioned, even where they were clearly able to identify IPV according to the IPV rating scale. The extent to which this may reflect concerns regarding the efficacy of police intervention (Leisenring, 2012) or a lack of understanding with regards to IPV and the law is unclear. Again, this may be particularly pertinent in a military context where veterans and their family manage a transition from internal to civilian jurisdiction.
Limitations
There were a number of limitations to the study that should be borne in mind. Men and older adults were not adequately represented, nor did the ethnic identities of participants adequately represent the British population. In addition, the questions used to determine relevant professional and personal experience may not have adequately differentiated between the two. In spite of efforts to minimise priming, the study clearly recruited an expert sample which may go some way to explain the heavy skew towards greater recognition of IPV and the link made between IPV and PTSD in both military conditions.
The measures used were developed specifically for this study and without psychometric validation the results using the IPV rating scale should be treated with caution. Most participants wrote less than the 10 lines requested for the story completion task meaning that the level of nuance hoped for was not achieved. It may be that the incident described was too clearly IPV and a more subtle account of abuse may have promoted greater diversity and complexity of response.
Future Research
IPV may be associated with a range of psychopathology (Shorey et al., 2012) and so research into the ways in which other diagnoses impact upon understanding of IPV is of interest. Important evidence is emerging regarding bi-directional violence as well as PTSD as a risk factor for being victim to IPV in military relationships (Misca & Forgey, 2017; Sparrow et al., 2017; Tharp et al., 2016). The minimisation of female violence in public discourse (Carlson & Worden, 2005; Sorenson & Thomas, 2009), the role of mental distress in mitigating violence found in this study and the promotion of hyper-masculine ideals (Taft, Watkins et al., 2011) may have particularly toxic implications for male victims of abuse in the military which warrants investigation.
Recommendations for Practice
The findings in this study confirm that public awareness campaigning needs to move beyond basic condemnation of IPV (Carlson & Worden, 2005). Campaigns may do well to focus on less overt behaviours including threats, control and coercion making clear that these constitute IPV and demand action which can include, but should not be limited to police involvement. Professionals working in mental health and military contexts would benefit from training to identify these forms of IPV particularly given the greater prevalence of escalation to high risk behaviours (Aronson et al., 2014) and the importance of early intervention as identified by the Ministry of Defence (2018). Public and professional perception of PTSD as a mitigating factor in IPV should be addressed. Targeted campaigning should be sensitive to the ways in which the victim status of the perpetrator may be prioritised in military relationships.
Conclusion
This study was the first to look specifically at public understanding of IPV in the context of military veteran status and PTSD and adds a number of new findings to the literature. Results indicated that the public are more likely to recognise IPV when it is perpetrated by a military veteran than a civilian with PTSD, and they are less likely to recognise abuse perpetrated by a civilian with PTSD, than without. Both public and professionals are less likely to acknowledge controlling behaviour. PTSD may be seen to mitigate IPV and in a military context prioritise the needs of the perpetrator in public consciousness. Awareness campaigns are advised to focus on clarifying what constitutes IPV and to consider the particular vulnerabilities of partners of abusive military veterans to discourses which prioritise the needs of the perpetrator.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.