
Abstract
Introduction
As the leading cause of cancer deaths and being the 2nd most diagnosed cancer (American Cancer Society [ACS], 2019), lung cancer causes substantial psychological morbidity that is important in its own right and often compromises treatment (Page & Adler, 2008). After treatment, patients undergo follow-up care as prescribed by their oncologist. This typically requires that they are screened for any cancer recurrence across the course of a few months to annually, depending on how early they have received treatment (ACS, 2022). Undergoing these scans on a regular basis can lead to an increased level of anxiety in preparing for the results. The anxiety associated with these scans is so pervasive across all cancer types that it has been termed ‘Scanxiety’ (Feiler, 2011). Scanxiety is characterized by a fear that (1) current treatments have failed, as reflected by one’s disease returning or progressing, (2) they may have to switch or add treatments, and (3) the fear of death (Portman, 2018). While most work has examined the prevalence or severity of scanxiety, little research has examined how scanxiety fluctuates in the context of one’s scan (Bui, Liang, et al., 2021). A meta-analysis from Bui, Liang, et al. (2021) found that out of 57 studies examining scanxiety, only 14 reported a statistical comparison of scanxiety before and after one’s scan, and the timing of the pre- and post-measurement varied from 4 weeks before to 1 year after. This is problematic as a patient may be going through scans frequently and so waiting an extended period to gather this information may lose the temporal sensitivity of scanxiety. Therefore, it is important to investigate the variability in anxiety and coping among those with lung cancer, in order to understand how one adjusts to their new routine for the rest of their lives after lung cancer treatment.
The anxiety one goes through in anticipation of their upcoming scan is fraught with various effects. Bauml and colleagues (2016) found that increased scanxiety among lung cancer patients with recurrent or metastatic non-small cell lung cancer (NSCLC) was related to impaired quality of life, specifically impacting emotional well-being. Bui, Blinman, et al. (2021) also conducted a qualitative study and found common themes in the manifestations of scanxiety such as changes in mood, impaired concentration, and physical symptoms like insomnia and fatigue. While these symptoms are similar to those seen with general anxiety disorder (Substance Abuse and Mental Health Services Administration, 2016), scan-related anxiety is specific to a group of individuals who must undergo a common and recurrent stressor (i.e., CT scans) for the rest of their lives.
Within-Person Perspective of Stress and Coping
Health psychologists have long utilized models of stress and coping to understand how individuals cope with and adjust to various challenges that occur within a person’s environment (Lazarus & Folkman, 1984; Moos & Schaefer, 1993), with the primary focus of understanding how one copes after experiencing a stressor. In addition, coping research has examined how environmental or organizational factors are related to coping strategies between people (Somerfield, 1997). When looking at cancer adaptation research specifically, researchers have stressed the importance of looking at change in coping behaviors based on a specific stressor versus a broad category, as this considers the unique circumstances that accompany specific stressful events, such as it is with patients with lung cancer and recurring CT scans (Somerfield, 1997). For example, individuals with lung cancer who have undergone curative-intent treatment and have CT scans every 6 months may vary in how they cope with upcoming scans based on how old they are, how long it has been since they have been diagnosed, as well as any family history of lung cancer. Therefore, between-person differences are an important factor to consider in understanding cancer adaptation.
Applied coping research can take a more in-depth look at coping with cancer by examining within-person fluctuations in coping. Specifically, examining a group of people with a unique stressor (e.g., CT scans) with similar characteristics (e.g., curative intent treatment) across time to see how they change in relation to their own coping. This allows researchers to investigate how the relationship between coping and scanxiety changes across time, as well as how person-level characteristics can impact this relationship. By examining how patients fluctuate in their coping and anxiety across time, researchers can investigate at what points it is at its highest for patients with lung cancer approaching their upcoming CT scans. Scanxiety among patients with lung cancer has been shown to be at its highest in the week prior to one’s scan (Bauml et al., 2016). Therefore, investigating the temporal sensitivity of scanxiety and coping, requires a unique approach to capture daily fluctuations in these concepts.
Anxiety and coping have been shown to fluctuate day-to-day (Neupert et al., 2016; Pearman et al., 2022) so it is important to understand these changes among a population of individuals to whom coping with anxiety is extremely prevalent; namely, patients with lung cancer approaching their CT scans. One such design that has been shown to reliably reflect day-to-day fluctuations, is a daily diary design which are typically “self-report instruments used repeatedly to examine ongoing experiences” (Bolger et al., 2003, p. 580). Daily diary designs reduce the likelihood of retrospection and increase reliability and validity by reducing measurement error (Bolger et al., 2003). Scanxiety occurs prior to one’s scan, so reducing retrospection is paramount as investigating this phenomenon involves looking forward, or preparing in advance, instead of looking back. Diaries help researchers get a better understanding of how one behaves in their natural setting; gathering information on “life as it is lived” (Allport, 1942, p. 56). Nesselroade (1991) describes intraindividual variability as short-term changes that can potentially be reversible, which is particularly important in applied coping research, as managing specific problems that occur daily is a primary goal in cancer adaptation intervention research (Somerfield, 1997).
Proactive Coping
When considering the importance of temporal investigations of anxiety and coping for patients with lung cancer and their upcoming scans, one must consider more stable coping (proactive) and less stable coping (anticipatory) strategies for this upcoming stressor, rather than their reactive response to the stressor. This is because patients know that their scans are always upcoming, and as a result, experience great deals of stress and engage in behaviors to try and manage this stress and anxiety. Proactive coping is a type of coping where individuals engage in efforts to prevent or modify how a stressor unfolds; and is considered more stable over time (Aspinwall & Taylor, 1997). With this type of coping, individuals may not know when or how the stressor will occur and unfold, but they engage in activities or behaviors to help offset stressors before they develop (Aspinwall & Taylor, 1997). A key feature of proactive coping is when the stressor occurs, as it involves preparing in advance and focusing on future events (Aspinwall & Taylor, 1997).
In the context of patients with lung cancer and scanxiety, knowing that a problem may arise is not enough to promote healthy adjustment to lung cancer maintenance and treatment. While some research has examined proactive coping strategies in breast cancer patients (Fujimoto & Okamura, 2021; Lisica et al., 2019), these efforts are examined in between-person contexts, and proactive coping efforts are recorded only at one point in time. Patients with lung cancer are in a unique situation where they know a stressor may be upcoming but are not always sure when it will occur (i.e., scheduling CT scans). Therefore, it is important to investigate how coping is reflected in this population across periods of time to see how it may fluctuate as a patient approaches their scan. While proactive coping is thought of as more stable, some research has found that it fluctuates across two time points (Miao et al., 2017), suggesting that repeated measurements across time may also reflect a similar trend. Thus, it could be fruitful to investigate proactive coping monthly among those with lung cancer.
Anticipatory Coping
In contrast to proactive coping, anticipatory coping may occur when an individual knows when an upcoming stressor will occur (Feldman & Hayes, 2005). While proactive and anticipatory both unfold before a stressor occurs, anticipatory coping involves targeted cognitive and behavioral efforts to prepare for a known upcoming stressor as it approaches (Feldman & Hayes, 2005). Feldman and Hayes (2005) designed the Measure of Mental Anticipatory Processes (MMAP), aimed at gathering four types of anticipatory coping that involve recurrent thought processes in preparation for the stressor; these include plan rehearsal, problem analysis, outcome fantasy, and stagnant deliberation. Plan rehearsal and problem analysis are thought to be associated with more positive outcomes, as they involve problem solving and accurately defining and analyzing the stressor, respectively. While the other two, stagnant deliberation and outcome fantasy, are thought to be associated with negative outcomes as they involve thinking of the problem with no progress or avoidance of the problem (Feldman & Hayes, 2005). As Neupert et al. (2016) pointed out though, the beneficial nature of these coping efforts was investigated in between-person designs that were devoid of context and lacked the understanding of within-person fluctuations across time.
Feldman and Hayes (2005) did however investigate anticipatory coping at two different time points, separated by 13 weeks, among a group of individuals known to be in a highly stressful environment (i.e., law students) and found that plan rehearsal predicted more positive thoughts towards the end of the semester, while outcome fantasy and stagnant deliberation were related to more negative thoughts. Neupert et al. (2016) took this one step further and examined the daily fluctuations of anticipatory coping with daily arguments among older adults and found that on days when older adults engaged in outcome fantasy, they reported decreases in well-being. Among the cancer population though, there is little research that examines anticipatory coping efforts in response to a known upcoming stressor, though some have examined this indirectly. For example, when preparing for the known side effects of cancer treatments (e.g., hair loss), Frith et al. (2007) found that the behaviors women engaged in strongly reflected that of anticipatory coping (e.g., affective and behavioral rehearsal). These findings suggest that investigating anticipatory coping methods among those with cancer could be beneficial to promote better outcomes (Borsellino & Young, 2011; Somerfield, 1997).
Age and Cancer-related Psychological Outcomes
In addition to examining how coping and anxiety fluctuate daily for patients with lung cancer, it is also important to examine how these relationships differ between people by person-level factors such as age. Age is an important consideration in cancer adaptation, as it has strong ties to the idea of one’s ‘social clock,’ which is a societal expectation of when significant life events are expected to occur (Neugarten, 1976). When it comes to lung cancer, these diagnoses are typically expected around age 65 or older (American Cancer Society, 2019), so if someone is diagnosed younger than this age, it may cause significant distress. Costanzo and colleagues (2009) investigated how aging impacts psychosocial adjustment to surviving cancer across time and found that younger survivors (<63) experienced more psychological distress post-diagnosis, suggesting that being “too soon” with their diagnosis, or not at the expected age, was related to increased mental health issues. Similarly, young women undergoing cancer treatments have sometimes been thrown into premature menopause and report increased physical and psychological issues as a result (Rosenberg & Partridge, 2013).
Present Study
Understanding how coping strategies are related to levels of anxiety within-person, and how person-level factors influence this relationship, can inform larger studies to implement ways to prepare in advance to reduce scan-related anxiety associated with upcoming scans. This is critically important as patients with lung cancer have these scans for the rest of their lives (American Cancer Society, 2022). Past research is either cross-sectional or if longitudinal, based on only a few observations across a wider timespan (Bui, Liang, et al., 2021), so little is known about the process of coping and anxiety that unfolds within a person over time in relation to their upcoming scan.
Objective
The primary aim of this work was to identify future-focused coping strategies that are related to low anxiety levels, within a person amid their scan. While no work has looked at how proactive and anticipatory coping relate to scan-related anxiety among patients with lung cancer, some work has shown how these types of coping are related to positive or negative outcomes. Therefore, the following hypotheses guided the current study.
Hypotheses
1. A negative association was hypothesized between proactive coping and scanxiety. This is because proactive coping has been shown to be related to reduced depressive symptoms and anxiety among college students (Greenglass & Fiksenbaum, 2009; Griva & Anagnostopoulos, 2010), preventing stressful events among older adults (Neubauer et al., 2019), and reducing stress, depression, and anxiety among patients with cancer (Kumar & Bharti, 2021). 2. For daily anticipatory coping, a positive association was hypothesized between stagnant deliberation or outcome fantasy and daily scanxiety. Research among college students and older adults have shown that these types of coping are typically related to more negative outcomes such as depressive symptoms, anxiety, or decreased well-being (Feldman & Hayes, 2005; Neupert et al., 2016), which was expected to reflect the lung cancer population as well. 3. Next, a negative association was hypothesized between plan rehearsal or problem analysis and daily scanxiety since past work shows that these strategies are associated with better outcomes such as positive thought processes; but previous work only shows this trend using a between-person design (Feldman & Hayes, 2005). 4. Lastly, given the previous relationships between age, coping, and cancer outcomes, an exploratory hypothesis investigated whether the relationships between anticipatory or proactive coping and scanxiety are different across age. Being “on-time” or “too soon” with a cancer diagnosis can have different psychosocial effects depending on where one is in the life course, so this hypothesis was tested to see how this operates in the present sample of patients with lung cancer.
Methods
Participants
Twenty five participants were recruited through a lung cancer non-profit organization in central North Carolina, as well as through snowball sampling, (
Measures
Monthly Measures
Proactive Coping
The 6-item Proactivity Scale from Aspinwall et al. (2005) was used to assess individuals’ “preference for planning for adverse events and expending resources to prevent them or to reduce their impact” (p. 365). Participants were asked, “Rather than spending every cent I make, I like to save for a rainy day.” and “Planning only makes a person unhappy, since plans hardly ever work out” (reverse scored). These items were answered on a 5-point Likert scale from 1 (strongly disagree) to 5 (strongly agree). Monthly means were calculated for each participant, with higher scores representing higher levels of proactive coping (α = .90).
Scan-Related Anxiety
The Impact of Event Scale (IES-6; Sundin & Horowitz, 2002) as modified by Bauml et al. (2016) for lung cancer scan screenings, examined monthly scan-related anxiety. It was modified for this study with a cognitive reset to reflect the last 30 days, and participants were asked to think about how distressing each difficulty (e.g., “I tried not to think about it” and “I had trouble concentrating”) had been for the past 30 days with respect to their scan. Participants responded on a Likert scale of 0 (not at all) to 4 (extremely) and monthly means were calculated for each participant, with higher scores representing higher levels of scan-related anxiety (α = .85).
Daily Measures
Anticipatory Coping
The 15-item adapted version (Neupert et al., 2016) of the Measure of Mental Anticipatory Processes (Feldman & Hayes, 2005), assessed coping with future stressful events. Two stressor domains were assessed: health and ‘other’, though the present analyses were focused on the health domain. The health-related prompt was modified to ask “Today, when you think about your upcoming scan, how often do you…”, and respondents were presented with items related to four factors of anticipatory coping. Five items related to Problem Analysis (e.g., “I think about why the problem is happening”) (α = .78), three items related to Plan Rehearsal (e.g., “I think about the solution in a step-by-step fashion”) (α = .60), five items related to Stagnant Deliberation (e.g., “I think about the problem without making progress on it”) (α = .79), and two items related to Outcome Fantasy (e.g., “I daydream about the problem fixing itself”) (α = .44), were presented. Each item was answered on a 5-point Likert scale ranging from 1 (never) to 5 (always). Daily mean composite scores were created for each of the four factors for each stressor with higher scores indicating a greater amount of anticipatory coping behaviors performed.
Scan-related Anxiety
The Impact of Event Scale (IES-6; Sundin & Horowitz, 2002) as modified by Bauml et al. (2016) for lung cancer scan screenings, was used to assess daily scan-related anxiety. This survey was modified with a cognitive reset to reflect the last 24 hours. Participants were asked to think about how distressing each difficulty has been for the past 24 hours with respect to their scan. Responses were on a Likert scale of 0 (not at all) to 4 (extremely) and included items such as “I tried not to think about it” and “I had trouble concentrating”. Daily mean scores were computed for each participant, and higher scores represented higher levels of scan-related anxiety (α = .85).
Procedures (Screening and Consent)
Participants answered a screening survey which included questions about inclusion criteria. These criteria were that participants must have been diagnosed with lung cancer, were within 6 months of their next scheduled scan, received curative intent treatment (i.e., intended to remove all cancer completely as it is localized via surgery, chemotherapy, etc.; ACS, 2019), were English speakers, were at least 18 years old, and were willing to provide their emails to be contacted for repeated assessments. If participants indicated in the screening survey that they were interested in participating, the research team scheduled a telephone call to explain the study procedures and obtain informed consent.
Procedures (Day 1, Monthly, & Daily)
On Day 1, which was the day following the telephone call, participants were sent emails at 6 a.m. EST that included the demographics survey and either their monthly survey or daily survey, depending on whether their upcoming scan was within the next 30 days. The demographics survey asked questions regarding gender, age, race, education, marital status, personal and family cancer history (e.g., date of diagnosis, cancer site, treatment received, and date of treatment received), and scan history. The monthly survey asked questions regarding proactive coping and scan-related anxiety framed in the context of the last 30 days. The response rate of the possible 59 monthly surveys was 100%.
Daily measures were sent starting 7 days before the scan, as well as the day of the scan. All daily surveys asked about anticipatory coping and scan-related anxiety framed for the past 24 hours. Out of the possible 200 days of daily surveys for the participants, 146 were valid, resulting in a 73% response rate. After completing the daily surveys, participants were emailed an online gift card and thanked for their participation.
Ethical Considerations
Before data collection, researchers received approval from North Carolina State University's institutional review board. Throughout the study, all ethical guidelines were followed.
Analytic Strategy
Multilevel modeling (MLM; Raudenbush & Bryk, 2002) was used to analyze repeated assessments within-person, focusing on changes in coping and scan-related anxiety on a monthly and daily basis. Multilevel modeling allows participants to function as their own controls, meaning their average scores are compared to their fluctuating reports. It also allows researchers to obtain estimates of person-level effects (i.e., age) that may be related to within-person relationships between coping and scan-related anxiety. MLM uses all available data from each participant, regardless of their completion rate. For this study, separate models were conducted for the daily and monthly data where the within-person predictors were coping (monthly: proactive, daily: anticipatory), the between-person predictor was age, and the dependent variable was scan-related anxiety.
Results
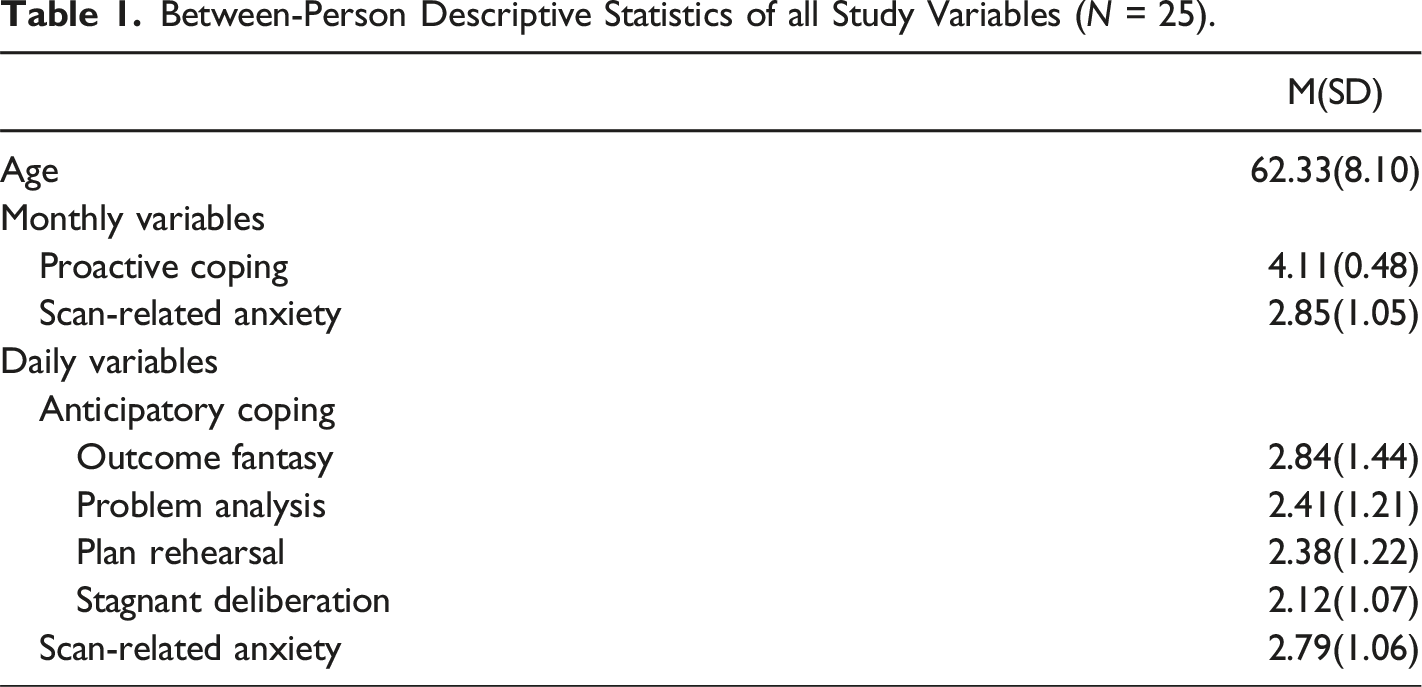
Between-Person Descriptive Statistics of all Study Variables (N = 25).
When reporting current CT scan outcomes, 72% of the participants chose to report their current CT scan results. These were open-ended items and of those who did respond, most reported “NED - No evidence of disease” or “Stable” (50%), some reported uncertain outcomes such as “was hard for them to read in parts” (22%), or that they needed additional treatment such as “having surgery” (11%). Some did not provide any feedback (17%). Before beginning the main analyses, the proactive coping and the anticipatory coping subscales were person-mean centered. This method allows participants’ daily or monthly responses to be compared to their own average for each scale (Raudenbush & Bryk, 2002). Age was also grand-mean centered to create a meaningful 0 to be used in the analyses, by subtracting the sample mean age from each participant’s age (Raudenbush & Bryk, 2002).
Unconditional Models
To begin the main analyses, fully unconditional multilevel models were run on each of the outcome variables to ensure sufficient variability within-person (i.e., monthly and daily level) and between-person (i.e., person-level) (see Neupert et al., 2006; Raudenbush & Bryk, 2002). In a fully unconditional model, only the intercept is included with all other predictors left out (Curran, 2000; Nezlek, 2001). One monthly and one daily model were examined, which required two separate fully unconditional models for each of the outcomes.
Unstandardized Coefficients (Standard Errors) of Multilevel Models of Monthly Proactive Coping and Anxiety.
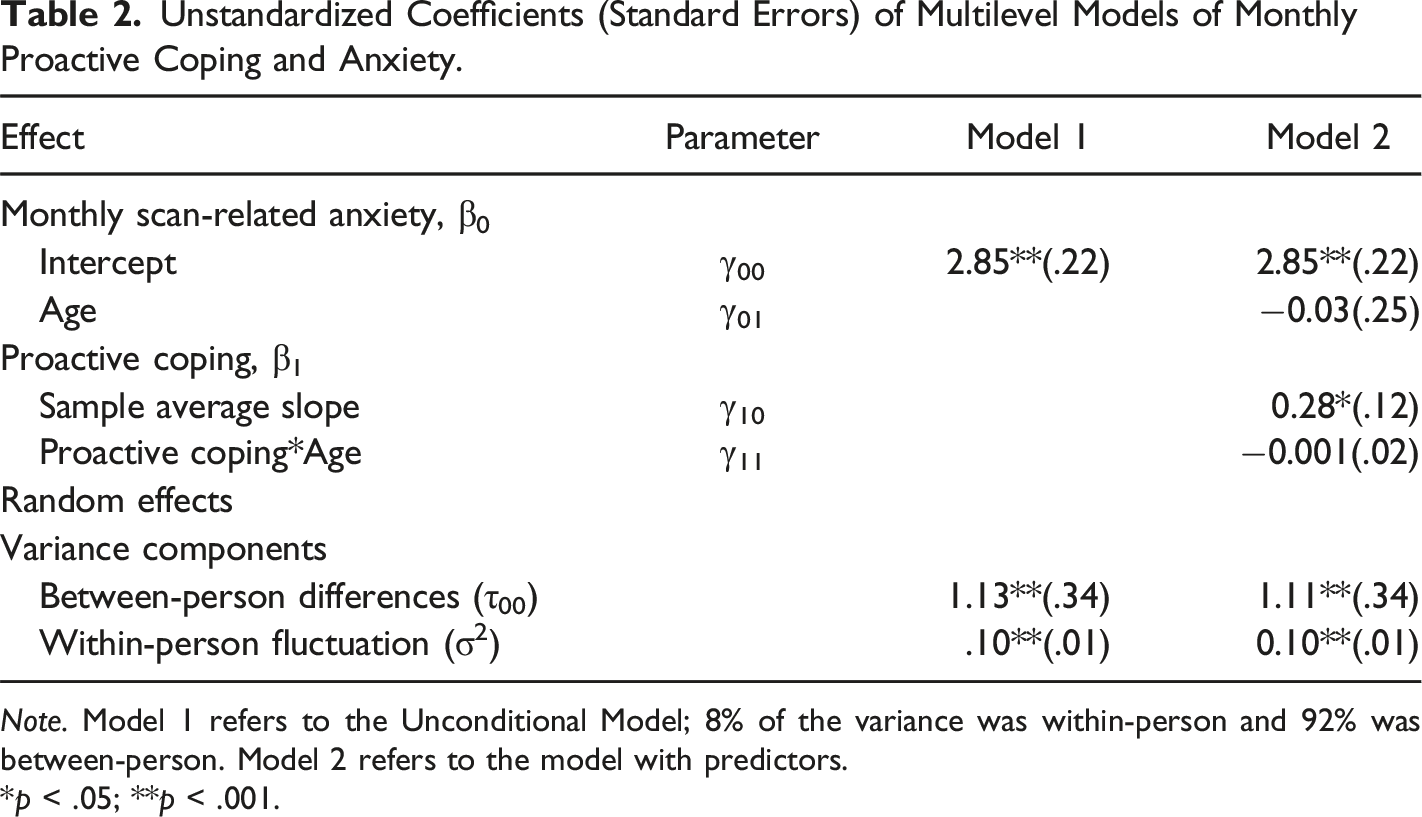
Note. Model 1 refers to the Unconditional Model; 8% of the variance was within-person and 92% was between-person. Model 2 refers to the model with predictors.
*p < .05; **p < .001.
Unstandardized Coefficients (Standard Errors) of Multilevel Models of Daily Anticipatory Coping and Anxiety.
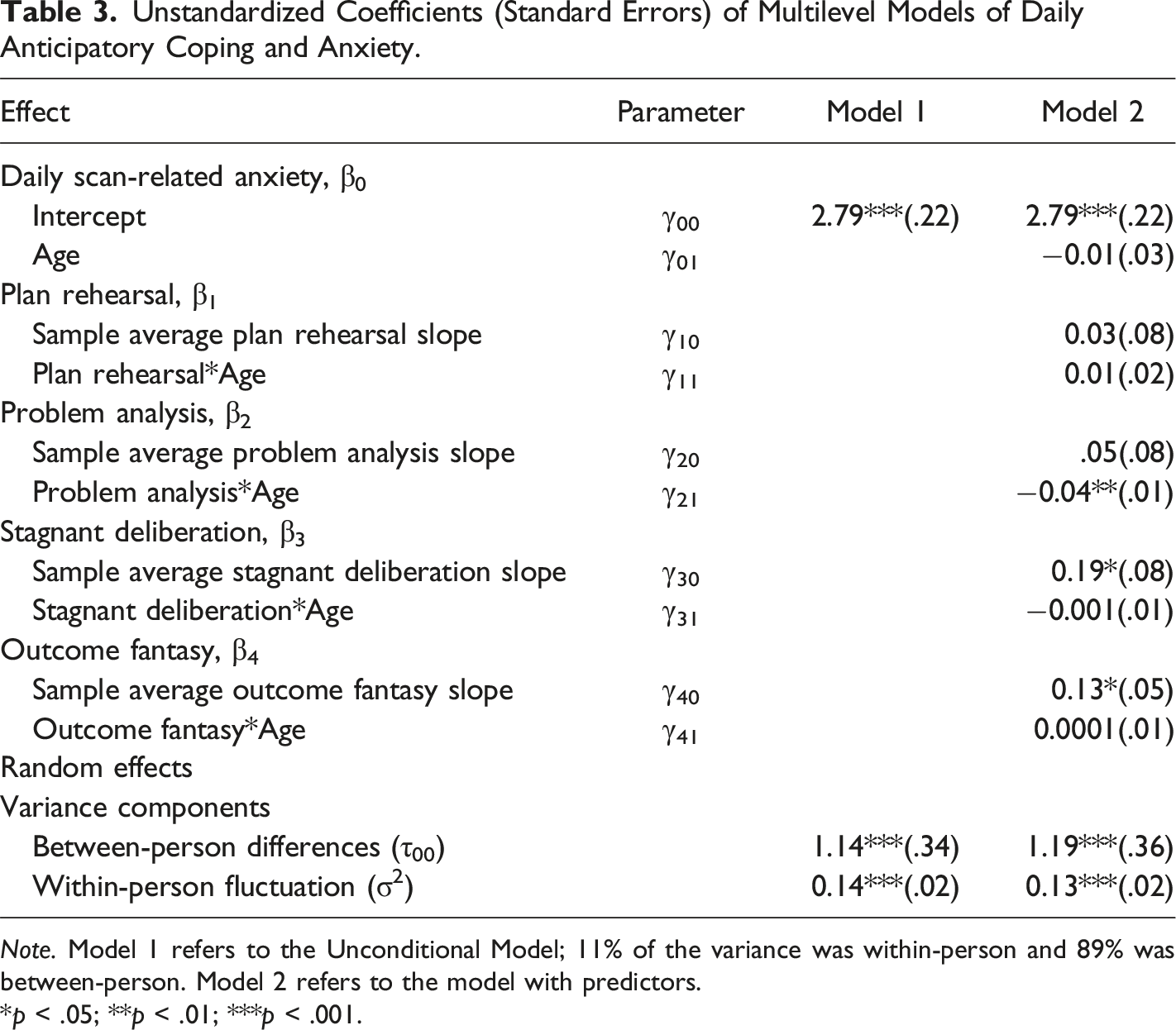
Note. Model 1 refers to the Unconditional Model; 11% of the variance was within-person and 89% was between-person. Model 2 refers to the model with predictors.
*p < .05; **p < .01; ***p < .001.
Monthly Model
To examine how proactive coping was related to scan-related anxiety in the months approaching one’s scan, as well as how this relationship differs by age,a non-random varying slopes multilevel model was run. This model constrains the slopes from person to person, so that the within-person relationship between coping and anxiety varies only as a function of the person-level variable (i.e., age). Using the person-mean centered proactive coping score, the relationship between proactive coping and monthly scan-related anxiety was tested, as well as whether there were age differences in this relationship. Results showed that on months when participants reported lower than their own average proactive coping, they also reported significantly lower scan-related anxiety for that month (see Model 2 of Table 2). However, there was no significant relationship between age and scan-related anxiety, and there were no age differences in the relationship between proactive coping and anxiety (see Model 2 of Table 2).
Daily Models
To see if anticipatory coping before one’s scan was related to daily scan-related anxiety levels, a non-random varying slope multilevel model was used. As with the monthly model, the slopes were constrained from person to person and used the person-mean centered anticipatory coping scores (i.e., plan rehearsal, problem analysis, stagnant deliberation, and outcome fantasy). This model tests whether each of the anticipatory coping scales were uniquely related to daily scan-related anxiety and whether there were age differences in any of these relationships. Results showed that on days before one’s scan when participants reported lower stagnant deliberation than their own average, as well as lower outcome fantasy than their own average, they also reported significantly lower scan-related anxiety for that day (see Model 2 of Table 3). There was no significant relationship between age, problem analysis, or plan rehearsal and scan-related anxiety before one’s scan. However, there was a significant interaction between problem analysis and age in predicting scan-related anxiety before one’s scan. Specifically, on days before the scan, when middle-aged participants reported more problem analysis, they also reported increases in scanxiety for that day (see Figure 1). Before scan daily problem analysis and scan-related anxiety as a function of age. Note. The slope for middle-aged participants (age 43–62) is significant (.18(.08), p = .027), while the slope for the older participants (age 63–78) is not (−.01(.16), p = .93). *p < .05.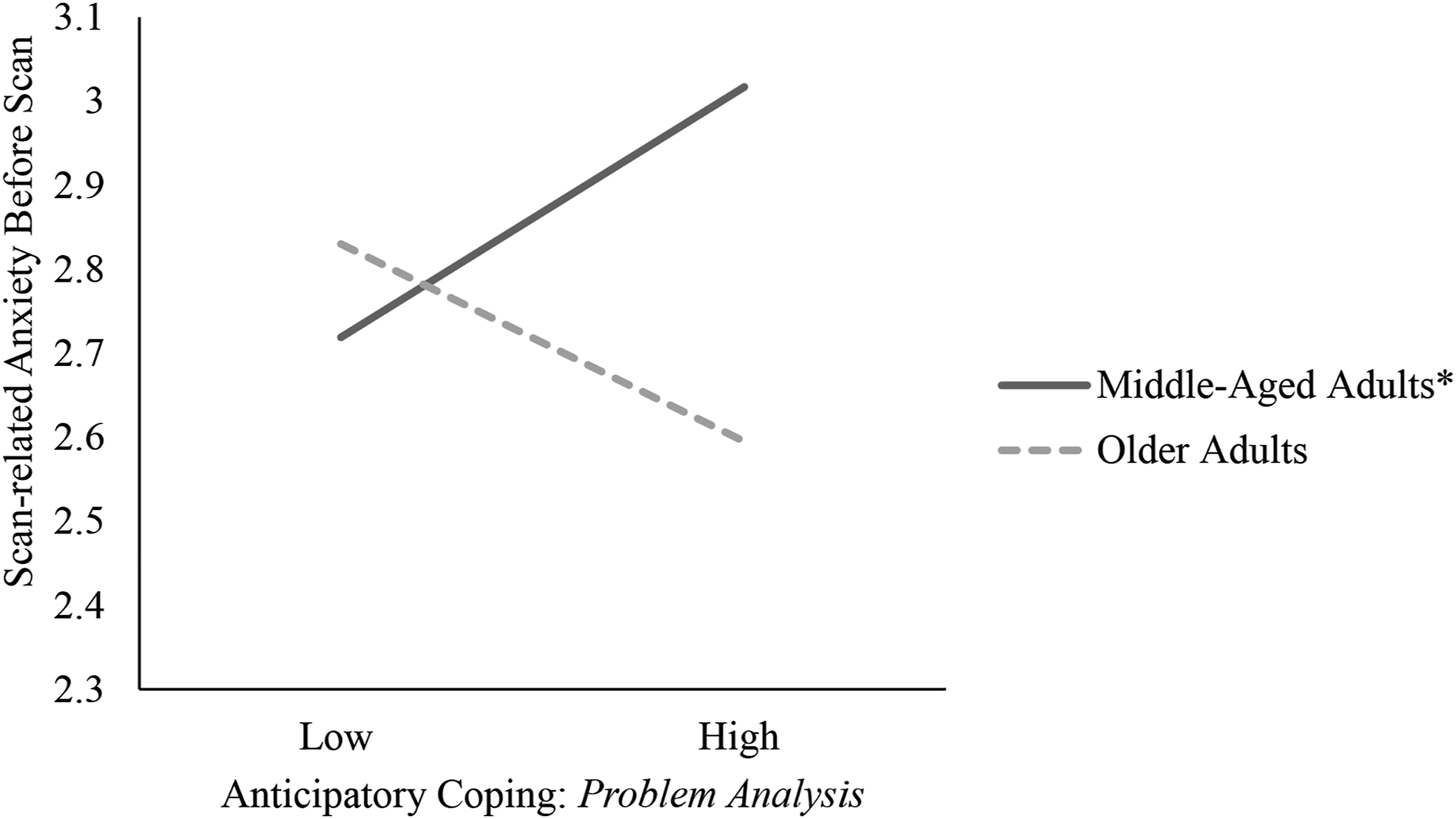
Given that 96% of the sample was female, the daily and monthly models were re-run excluding male participants and all patterns of results remained the same.
Discussion
The goal of the present study was to investigate how coping (proactive and anticipatory) and scan-related anxiety fluctuate among patients with lung cancer in the months and days prior to their CT scans, and how age may impact these relationships. Results from the unconditional models showed that the within-person variability to be explained in scan-related anxiety was significant. The fact that scanxiety is not stable and fluctuates day-to-day suggests that it can be intervened and improved on for this population, as suggested by Nesselroade (1991).
Proactive Coping
Given past work (Greenglass & Fiksenbaum, 2009; Griva & Anagnostopoulos, 2010; Kumar & Bharti, 2021; Neubauer et al., 2019) a negative association between proactive coping and scanxiety was hypothesized. However, these results suggested a positive relationship. Specifically, on months when people decreased their proactive coping they also experienced decreased scanxiety. While the authors are unaware of current research that has found this relationship, there is a great deal of literature on the benefits of focusing on the present rather than thinking about the future among patients with cancer. One such method of focusing on the present, rather than being future-oriented, is mindfulness. Mindfulness involves “paying attention in a particular way: on purpose, in the present moment, and non-judgmentally” (Kabat-Zinn, 2009, p. 4). A meta-analysis done by Ledesma and Kumano (2009) found that mindfulness-based stress reduction (MSBR) techniques are related to alleviating anxiety and stress among patients with cancer. In a more recent review, Musial et al. (2011) found that MSBR programs can improve quality of life and reduce distress in patients with cancer. These findings could explain why focusing on the future, specifically in patients with lung cancer approaching CT scans, may be counterproductive in reducing anxiety. Future research should continue to investigate present-focused versus future-focused thought processes and their relationship to scanxiety among those with cancer.
Anticipatory Coping
In line with one hypothesis regarding daily relationships, there was a positive association between two forms of anticipatory coping and scan-related anxiety. Specifically, on days when participants reported increases in outcome fantasy and stagnant deliberation, they also reported increases in scanxiety, after controlling for the other forms of anticipatory coping. Past research among those with cancer has shown that increased behaviors such as distraction and normalization increase in the days before one’s scan (Bui, Blinman, et al. (2021)). These behaviors are similar to how Feldman and Hayes (2005) defined outcome fantasy - fantasizing desired outcomes and ignoring details of problem-solving. Stagnant deliberation consists of thinking about the problem without making progress on it (Feldman & Hayes, 2005). Similar to stagnant deliberation, rumination has also been shown to be related to increased levels of anxiety and depression in patients with cancer who were in remission (Liu et al., 2018); yet rumination is more backward focused. This means that with increases in these behaviors, and their relationship to increased levels of depression and anxiety (Feldman & Hayes, 2005), it would not be surprising that these forms of anticipatory coping are also related to increased scan-related anxiety when the stressor has been defined. When considering future applications of this work to the cancer community, a positive relationship suggests that a decrease in these behaviors also relates to decreases in symptoms of depression and anxiety. Therefore, future intervention and implementation work could focus on reducing these behaviors in order to reduce scanxiety for those approaching their upcoming scans.
Problem Analysis Effect Depends on Age
There was only one significant interaction between age and anticipatory coping as it relates to daily scan-related anxiety. Specifically, middle-aged adults who reported increased levels of problem analysis also reported increases in scan-related anxiety for that day, after controlling for other forms of anticipatory coping. For older adults, there was no association between daily problem analysis and scanxiety.
Problem analysis involves the active contemplation and meaning of the problem in future stressful situations (Feldman & Hayes, 2005). Some aspects of problem analysis, including accurately defining the problem, are essential in problem-solving interventions used to treat depressive and/or anxiety disorder (Zhang et al., 2018). Yet, middle-aged adults in the study (i.e., 1 SD below M) reported increases in scan-related anxiety when using this strategy compared to older adults. Part of the benefit of problem analysis is that it involves accurately defining the problem and allows the individual to gain insight into the experience, which clinicians can use in clinical interventions D'Zurilla & Nezu, 2001; Stiles et al., 1990). This process may get complicated when looking at those with cancer who see the problem as an abnormality in their aging process and fixate on it.
Cancer has progressively been diagnosed in adults younger than the average age of 65; as a result, the field of geriatric oncology has been established to investigate how aging and cancer are related to general outcomes (Blank & Bellizzi, 2008). Neugarten (1976) described the idea of the ‘social clock’ as a way individuals define life events and whether they are to be expected at a time in one’s life. As previously mentioned, if certain critical events such as a diagnosis of cancer are not ‘on-time’ with when it is expected in the lifespan, it can elicit a great deal of anxiety and other mental health problems (Jones et al., 2014; Neugarten, 1976; Park et al., 2018). For patients with lung cancer, this could be amplified if they are not able to explain their diagnosis through other factors (e.g., no history of smoking, no family history of lung cancer, etc.). Therefore, when middle-aged adults try to analyze and make sense of the problem, they are unable to and may perpetuate that anxiety when they think about their upcoming scan. For future intervention work, it would be important to take this into consideration, as it may not be helpful to focus on defining the problem and making sense of it. Intervention and implementation work should consider factors like age when developing strategies to reduce anxiety among individuals with cancer.
Limitations and Future Directions
While this study was the first of its kind to track how coping efforts are used to prepare for a unique upcoming stressor (i.e., CT scans), there were some limitations. The only modification to the anticipatory coping items was to alter the lead-in so that participants were directed to “think about your upcoming scan”. Given the relatively low reliability of the outcome fantasy subscale, future work may consider further modifications to be even more cancer specific to boost reliability. Conducting community feedback work on the measures within larger lung cancer populations to investigate the validity and reliability of these items could be useful.
Another limitation of this study was that various between-person differences were not able to be investigated due to the relatively small sample size. Multiple factors can influence how one deals with their scanxiety as they approach their scans. For example, cancer stage has been shown to be related to coping strategies, as reflected in a systematic review from Thomsen et al. (2010) that found that individuals with advanced cancer diagnoses engaged in more emotion-focused versus problem-focused coping. Many participants in the sample had extensive experience and familiarity with the CT process, as 60% of the sample had 10 or more CT scans since their cancer diagnosis. Even though the sample had experience with CT scans, there were still significant within-person fluctuations in coping as well as scanxiety, supporting the claim that scanxiety is a persistent and invasive experience (Bauml et al., 2016) and that effective coping strategies could be useful. A further limitation to this study is that the results are less generalizable to male lung cancer patients given their low representation in the sample.
Scanxiety, as mentioned, involves the fear of one’s disease returning, treatments failing, and/or the fear of death (Portman, 2018). Proactive and anticipatory coping may be important for scanxiety because both involve pre-emptive efforts that may alleviate these fears, yet may also have some counterintuitive effects as shown in the present study. Proactive coping, for example, involves efforts to modify how a stressor unfolds, which may reflect some underlying perceptions of control. Past research has shown that patients with lung cancer hold a higher health-related internal locus of control (De Valck & Vinck, 1996; Lin & Tsay, 2005), so future work should incorporate views on control to see how this may impact one’s scanxiety if they feel responsible for the outcomes of their upcoming CT scans. Similarly to proactive coping, the results of the current study showed that stagnant deliberation and outcome fantasy, two factors of anticipatory coping, were related to increases in scanxiety in the days before one’s scan. These coping behaviors involve thinking about a problem without being able to solve it, and imagining desired outcomes, respectively. When thinking about health locus of control, if patients do not have actionable items to help improve their diagnosis, they may experience increases in scanxiety. Again, future work should incorporate locus of control as an antecedent to resulting scanxiety, to see how it may interact with coping strategies in predicting scanxiety levels.
Applications
While this study has some limitations, there are various clinical applications that can be used in future intervention and implementation research. Scanxiety is a persistent and intense experience for patients with cancer still undergoing regular CT scans. Regardless of the outcomes of the scan, scan-related anxiety can continue to cause distress to cancer patients (Bauml et al., 2016). Although clinicians and patients alike recognize the importance of understanding scanxiety, little work has examined how it fluctuates in the months and days prior to the scan (Bui, Blinman, et al. (2021)). This means that intervention and implementation work cannot occur without a clear understanding of the problem. In the current study, there were significant relationships between coping strategies that are related to reduced scanxiety, as well as how age impacts this relationship, in the months and days before one’s scan. Particularly, middle-aged adults may require tailored coping strategies in the days before their scan to help reduce scan-related anxiety. Applied work should continue to investigate these relationships and how best to intervene.
Conclusion
This study was the first of its kind to investigate how scanxiety and coping fluctuate among a population who encounter CT scans on a frequent basis, as well as how age plays a role in this relationship. The most important takeaway from this work is that patients with lung cancer need help in managing their anxiety in the months and days prior to their scans, and therefore, future work should continue to develop effective ways to alleviate this anxiety. Lung cancer impacts a large portion of the population, so finding ways to reduce these poor outcomes needs to be paramount in cancer outcome research.
Footnotes
Acknowledgments
We thank Lyndsey N. Graham for her assistance in data collection. We also thank Dr Edwin Fisher for his guidance in lung cancer research and for connecting us to the Lung Cancer Initiative (LCI). LCI helped in the recruitment of patients with lung cancer, which made this project possible.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project described was supported by the National Center for Advancing Translational Sciences (NCATS), National Institutes of Health, through Grant Award Number UL1TR002489, and a pilot award, 2KR1382102, awarded to Victoria J. Dunsmore. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.