
Abstract
Previous research assessing correctional worker (CW) mental health has seldom assessed for differences based on jurisdiction or diverse occupational categories. The current study was designed to provide a nuanced quantitative examination of mental health disorder prevalence and related problems among CWs and to qualitatively explore the varying social contexts surrounding CW well-being. We reflect on how we overcame unanticipated challenges and disruptions (e.g., technology, COVID-19 pandemic) throughout the design, launch, and analysis of the survey, and illustrate how our national study, driven by a rigorous methodological approach and collaborative research design, builds on the extant CW mental health and wellness literature.
Introduction
Canadian correctional workers (CWs) are a historically under-researched sector of public safety personnel (PSP; Ricciardelli, 2019). In 2016, researchers launched a research project designed to provide a national Canadian assessment of diverse PSP, including CWs (Carleton et al., 2018a). The study results evidenced that CWs, broadly defined, were (1) frequently exposed to potentially psychologically traumatic experiences (Carleton et al., 2019) and (2) the exposures were associated with clinically significant symptoms of diverse mental health disorders (Carleton et al., 2018a), including suicidal behaviors (Carleton et al., 2018b). Many CWs in the original survey (54.6%) screened positive for at least one mental health disorder (Carleton et al., 2018a). The original results were limited because CWs were assessed collectively without consideration for different jurisdictions or institution levels (i.e., federal, provincial, and territorial), and without stratifying respondents by occupational classification (e.g., correctional officer, probation officer, teacher, and nurse). International research examining CWs also typically focuses on correctional officers (COs), aggregates all CW categories together, or tends to be conducted internally to the organization, potentiating stigma-related biases, all of which may mask important nuances (Armstrong & Griffin, 2004; Bourbonnais et al., 2007; Ghaddar et al., 2008; Griffin et al., 2010, 2012; Haynes et al., 2020; Lambert, 2006; Lambert & Hogan, 2018). The Provincial and Territorial Correctional Worker Mental Health and Well-being Study (CWMH) was designed to build directly on the original survey and results (Carleton et al., 2018a) by providing more nuanced assessments of CWs in Canada, assessing for differences across jurisdictions and occupational classifications of CWs. Moreover, we wanted to understand why the prevalence of mental health disorders was high and the contexts informing such challenges.
The CWMH was formally launched in 2018, although the project began in 2017 with an online survey disseminated in Ontario, the largest province of Canada in terms of population size. The investigation expanded to the remaining provinces and territories from 2018 to 2023. Specifically, we did not conduct one large national study. Instead, replications were carried out across every province and territory, serving as a national study, and with the intent to start by providing quantitative data to determine mental health disorder prevalence among CWs stratified by jurisdiction and occupational group. We then planned to analyze qualitative data collected through open-ended survey questions to help contextualize and build upon the quantitative estimates. The research evolved to include comparisons across the replications conducted with the other 12 provincial and territorial correctional systems in Canada, providing a wide array of knowledge on CW mental health and well-being.
Several initial result sets have already been published using the data collected from Ontario and other provinces and territories. The findings have clarified: (1) the mental health disorder prevalence of CWs in Ontario specifically (Carleton et al., 2020), as well as across provinces and territories (Ricciardelli et al., 2024); (2) the suicide behaviors prevalence of CWs in Ontario (Carleton et al., 2022) and Manitoba specifically (Ricciardelli et al., 2022a); and (3) the types and frequencies of potentially psychologically traumatic event exposures among CWs in Ontario specifically (Ricciardelli et al., 2022c, 2023a). We have also evidenced the prevalence of difficulties with mental health knowledge, stigma, and service use intentions (Coulling et al., 2024; Johnston et al., 2022, 2024; Johnston & Ricciardelli, 2023), alcohol use (Ricciardelli et al., 2023b), and cannabis use (Taillieu et al., 2024). The results have built off of our previous work to substantively increase our collective understanding of CW mental health, well-being, and vocational experiences across jurisdictions and specific CW work categories.
Our purpose for the current article is twofold: First, we outline our research designs, detailing any differences or similarities between the surveys deployed in each provincial and territorial correctional service (i.e., some services asked for modifications or additions) and how the published knowledge or that which is intended for publication fits together, focusing on interconnections and uniqueness among produced and disseminated research (i.e., a map of disseminated knowledge). Second, the project involved highly sensitive data collections that require care and understanding to appreciate the experiences and perspectives of CWs fully; as such, we also provide insights into how we engaged study tools and collaborative efforts to meet ethical guidelines and procedures and overcome emergent challenges. We also reflect on strategies adopted to circumvent disruptions encountered through technology and the unanticipated COVID-19 pandemic.
Methods and Procedure
Study Overview
The CWMH mixed methods (quantitative and qualitative) study employed an online survey with open- and closed-ended items. The survey followed established guidelines for web-based surveys (Ashbaugh et al., 2010). Survey items queried demographic and background information, self-reported assessments of various mental health symptoms using established questionnaires, and open-ended response items about a variety of workplace conditions and considerations. Participants could choose to skip questions, and certain questions only displayed if screening criteria were met; as such, the number of individual questions answered varies.
Objectives and Framework of Inquiry
We operationalized CWs as all persons working in the correctional services under the related Department or Ministry within each Canadian province or territory. We operationalized wellness as health, and included social, physical, and psychological dimensions (World Health Organization, 2020). Within these operationalizations, we intended to quantify diverse stressors (i.e., operational [e.g., job content]; organizational [e.g., job context]) and mental health disorder prevalence proportions among territorial and provincial CWs. Our research questions included:
What is the prevalence of mental health disorder(s) symptoms among CWs, stratified by occupational position, and their care or help seeking behaviors? What are the social contexts and contents underpinning the prevalence of symptoms of mental health disorders, help seeking behaviors, and perceptions of care and treatment? How can CWs with perceived mental health needs be best organizationally supported when seeking or needing help, treatment, access to care, or other health resources?
Our intention in answering these broad research questions was to inform the mental health and wellness strategies of each provincial and territorial correctional service in Canada. Our research was guided by “appreciative inquiry,” an approach related to Weber's concept of Verstehen (Platt, 1985) and rooted in a position of appreciation, empathy, or participatory understanding of social phenomena, and driven by the point of view of participants (see Liebling et al., 1999). We approached each organization wanting to understand employee mental health and wellness, recognizing employee challenges when addressing occupational health, and remaining open about options for moving forward. We reflected on the need to expand the nascent evidence for informing change efforts related to wellness practices, policies, procedures, and organizational culture.
Survey Design and Data Collection
Data were collected with a series of province/territory specific web-based surveys consistent with the original pan-sector nationwide prevalence survey (Carleton et al., 2018a). The surveys were launched in collaboration with employers and unions in each jurisdiction beginning with Ontario in 2017, and Newfoundland and Labrador following shortly after in early 2018. Contacts within each jurisdiction were solicited through several communication channels (e.g., professional networks, email and phone inquiries, internet-based research). After initially contacting someone within the correctional service of each jurisdiction, the Principal Investigator and research team made further inquiries to ensure all relevant stakeholders were present for discussions regarding the content of the survey instrument and the specific survey launch.
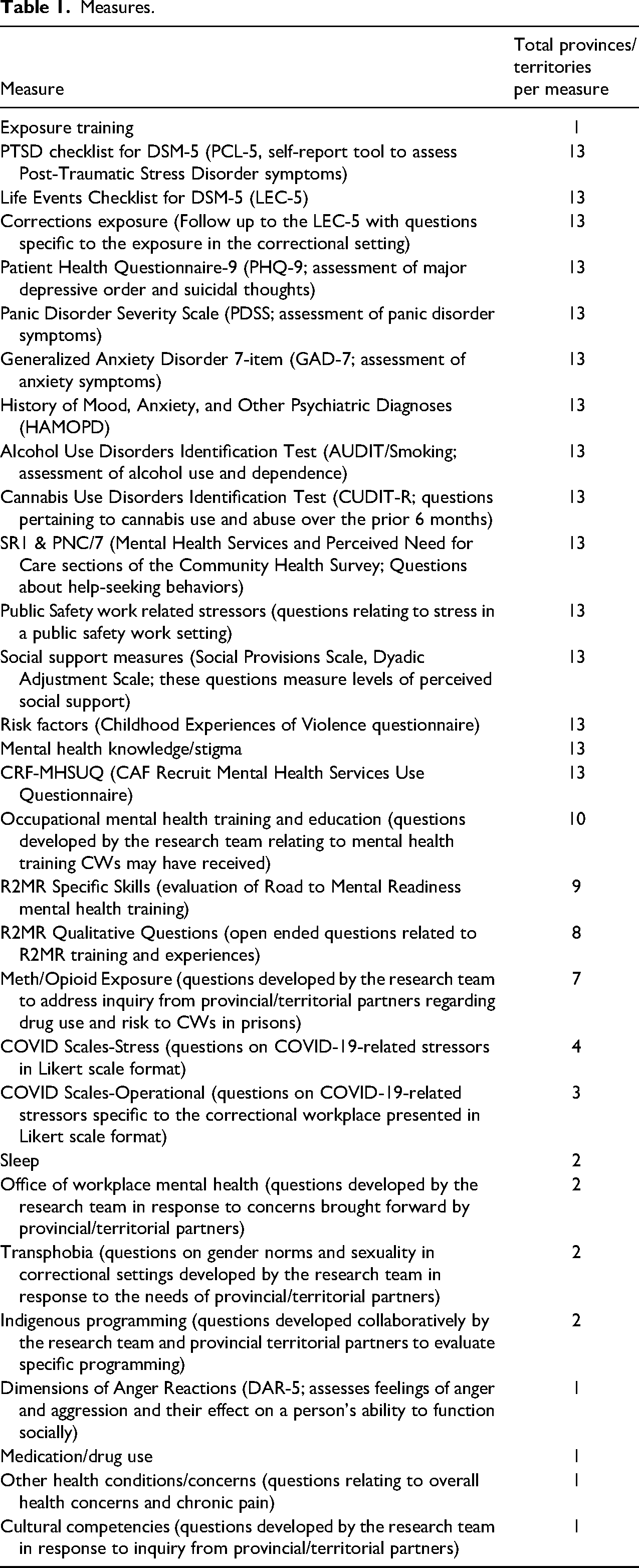
The research team ensured survey content was appropriate and relatable to workers by working closely with key contacts in each location. Most survey elements were consistent across jurisdictions to support national analyses. However, there were survey variations specifically requested by select jurisdictions (e.g., cultural competency measures and questions relating to drug exposure; see Table 1 for survey-specific measures). Survey elements and response options were tailored as needed to reflect differences in staffing and organization across provinces and territories. For example, job titles and categories of employment are not uniform across all correctional services. In some jurisdictions, job titles were combined to protect anonymity among smaller participant samples.
Measures.
Participant Recruitment and Survey Launch
Ministerial/departmental correctional and union representatives invited their employees and membership to participate in an anonymous and confidential online survey, available in English or French, via their email listserv of employees/members. There was overlap between listservs, precluding definitive sampling frame parameters and response rates, as noted in published study limitations. Interested respondents were provided with an email link to an online consent form, study information page, and survey. Participation was voluntary, and average survey response times ranged from approximately 25 min to more than 60 min. The study was approved by research ethics boards at the University of Regina (REB #2017-098), Memorial University of Newfoundland (ICEHR #20201330-EX), and the Affiliated Health Sciences Centre Research Ethics Board at Queen's University (#6024787). However, the Queen's University co-principal applicant was not affiliated with surveys outside of Ontario.
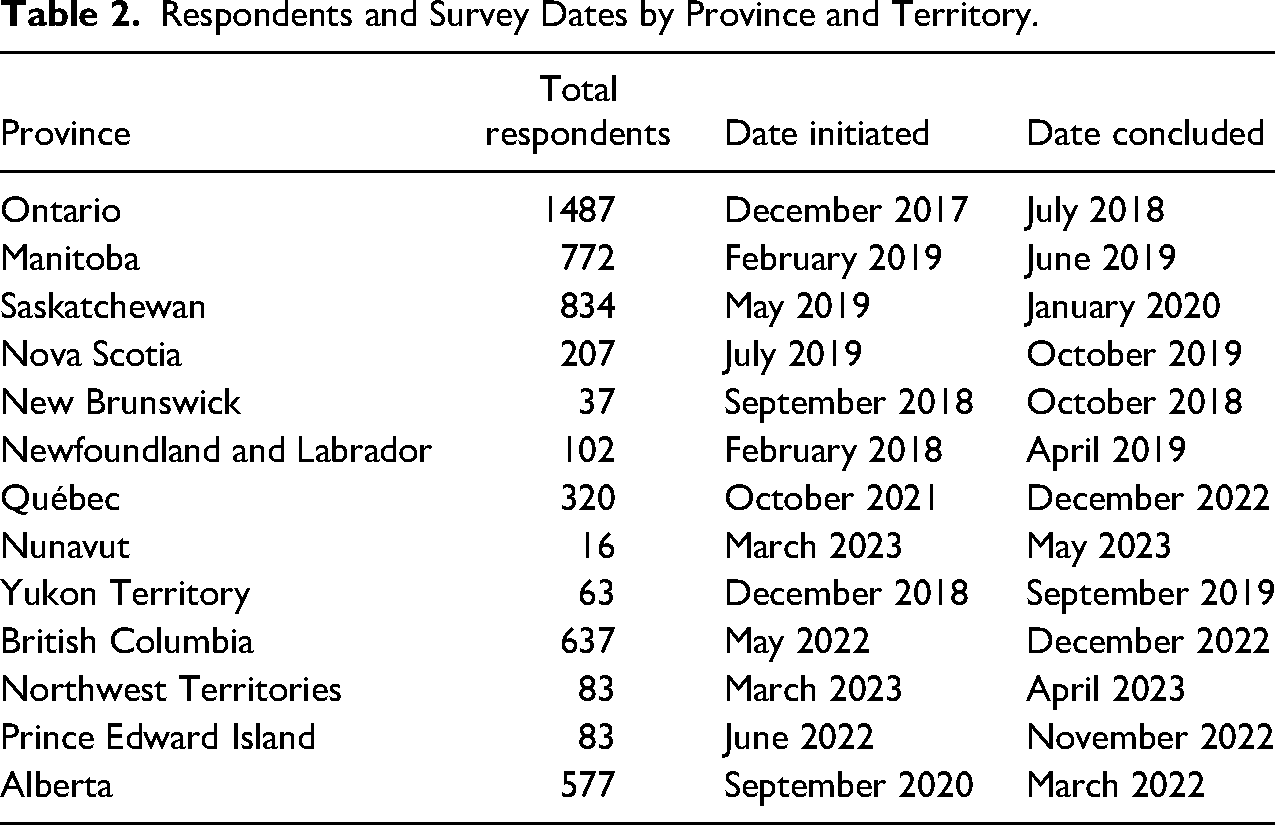
The email invitations were distributed by jurisdiction with local correctional and union representatives leading communications. Respondents were encouraged to answer all questions in the survey, but they were not required to answer any given item. Item-by-item voluntary responding produced variable response rates throughout the datasets. The study spanned almost 6 years, beginning in Ontario on December 8, 2017, and recorded its final responses in Nunavut on May 5, 2023. Surveys launched in Ontario, Manitoba, Saskatchewan, Nova Scotia, New Brunswick, Newfoundland and Labrador, and Yukon Territory were completed prior to the COVID-19 global pandemic (see Table 2 for details). Surveys launched in Alberta were completed during the COVID-19 pandemic, beginning May 22, 2020, and ending March 14, 2022. After Alberta, surveys were launched in British Columbia, Prince Edward Island, Québec, Northwest Territories, and Nunavut. The surveys in the Northwest Territories and Nunavut were completed on April 13, 2023 and May 5, 2023, respectively (see Table 2).
Respondents and Survey Dates by Province and Territory.
Analyses
The questionnaire included close-ended response questionnaires assessing: CW demographics; mental health disorders (using established and validated self-screening tools); mental health knowledge; mental health training; support networks; potentially psychologically traumatic event exposures; correctional-specific traumatic event exposures, risk factors; COVID-19 impact (during COVID-19 surveys); and other variables of interest (see Table 1 for details). Statistical analyses have included, but have not been limited to, descriptive statistics, multivariate regressions, and hierarchal linear models (HLMs).
Complementing each close-ended response questionnaire is at least one qualitative open-ended item requesting context for the questionnaire responses. Responses to the open-ended items ranged from a few words to several paragraphs. A team of research assistants used QRS NVivo to code qualitative data derived from the open-ended item responses, after first constructing a codebook, and then drawing on a constructed semigrounded emergent theme approach (see Ricciardelli et al., 2010), the team transferred codes with frequent notation to primary, secondary, and tertiary themes (Charmaz, 2014; Glaser & Strauss, 1967) or parent, child, and grandchild nodes (per NVivo terminology). The team developed the codebook by reviewing all data materials and created mutually exclusive and exhaustive groupings tied to topic, subject, tone, and position. The development process first used a subset of the data; then, after codes were saturated, the codes were compared across researchers to ensure comprehensiveness, and then aggregated to construct the codebook for all survey responses. The team completed comprehensive and detailed quality checking to ensure consistent adherence to categorizations when coding, which also offered an opportunity to discuss discrepancies in interpretations or challenges with coding decision making.
Codes were denoted as “nodes” in NVivo; as such, the team ensured themes were constituted only when multiple participants described similar experiences, interpretations, or understandings. Interesting and informative data emerged suggesting uniqueness in experiences; such cases were not identified as themes. Instead, such cases were recorded as interesting occurrences (n=<5; i.e., consistent with reporting decisions for quantitative results), and excluded from data analyses. The team grouped pertinent data into one document to analyze responses to each qualitative item, reading narratives first to become immersed in the data, and then coding the data to align with the codebook. The analytic plan was designed to facilitate an empirically driven sense of the entire dataset and to identify key themes across responses (Corbin & Strauss, 2015).
Overall, qualitative analyses tended to target one to two questions, although one article analyzed the responses to six questions in Ontario (McKendy et al., 2021). We offer a graphic depiction of the interconnected research results in Figure 1, which addresses how knowledge around CW mental health and its impacts developed and triangulated through published findings on mental health disorder prevalence, experiences with organizational and operational stress, traumatic exposures, suicide behavior and thoughts, as well as considerations for treatment, help-seeking, and related mental health stigma.
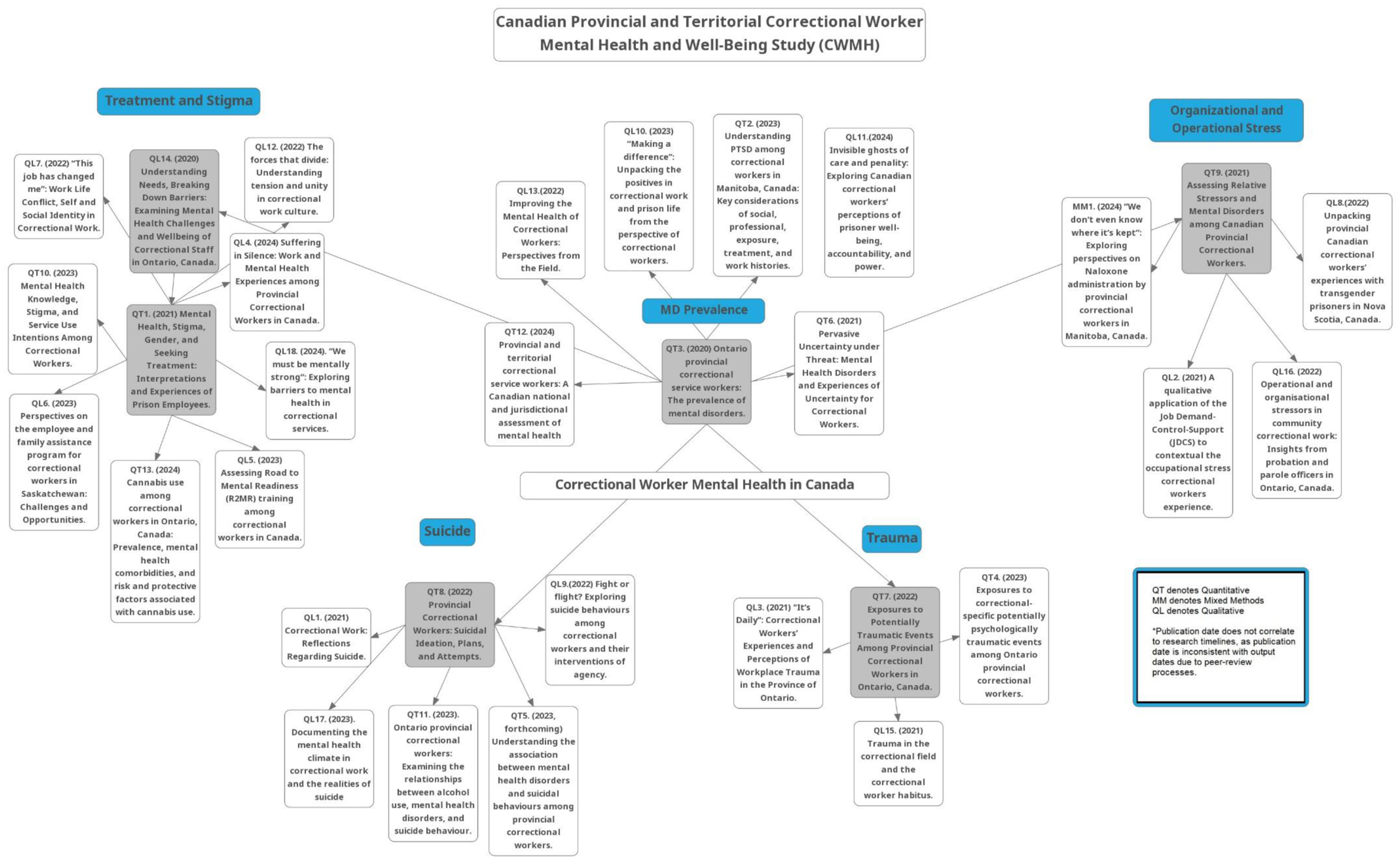
CWMH peer-reviewed articles and connectivity. CWMH=Canadian Provincial and Territorial Correctional Worker Mental Health and Well-Being Study.
Benefits of Collaborative Research Design
We followed a methodologically consistent and collaborative approach in each jurisdiction, but offered flexibility to support varying cultural/occupational contexts and mandates. The core of each survey replicated the Ontario survey, which was derived from the original (Carleton et al., 2018a) and then tailored in collaboration with CW representatives. For each subsequent survey, revisions were made based on the needs and interests of the specific jurisdiction. The intentional core design built on previous work allowed for broad comparisons across datasets. Stakeholders were provided with the nuances of survey design to maximize the idiosyncratic tailoring and to underscore the potential individual and collective benefits of participation.
Thus, the surveys were co-created with each correctional service, often including the applicable union, and increasing collective engagement. The research plan was operationalized based on dialogues with all stakeholders to ensure maximum participation, and all involved researchers supported data analyses and knowledge translation efforts. We worked to minimize our institutional footprint (i.e., staying at arm's length) and prioritize rigorous data collection that “balances the need for both internal and external validity (quantitative) or trustworthiness, credibility, and plausibility (qualitative)” (Reio & Werner, 2017, pp. 440–441). Data collection was variable with respect to jurisdiction start points and benefited from collaborative efforts that mitigated typical logistic challenges such as approval processes, survey adaptation, and survey dissemination. Services have remained receptive of study findings and report ongoing commitments to improving CW wellness (see Ricciardelli et al., 2022b).
Meeting Ethical Requirements and Overcoming Technological and Operational Challenges
We created each survey in Qualtrics, a secure web-based survey software used frequently for mixed-methods data collection. The research team encountered unique challenges that required customized solutions to deliver a user-friendly survey instrument that met all ethical obligations as required by institutional ethics review, research review boards (e.g., research boards where existent at different correctional services), and stakeholders (e.g., ministry or union representatives). Responses were kept confidential and anonymous. The survey included many sensitive questions, including asking participants to identify their most impactful potentially psychologically traumatic event exposure(s), and queries about suicide thoughts, behaviors, plans, and attempts (Carleton et al., 2020, 2022; Ricciardelli et al., 2020, 2023a).
The survey was lengthy and, based on early feedback, respondents were given the ability to take a break from the survey and return later to complete the survey. All participants were allowed to complete the survey while at work and on work computers, potentiating participation, but this created procedural and ethical challenges we had to overcome. Qualtrics allows users to “Save progress.” However, this function utilizes an internet browser's cache and browsing history to save responses to surveys. Thus, responses provided through a public or shared workstation could not be kept confidential or anonymous, and participants could inadvertently gain access to another person's survey responses. Conversely, in prisons and some community correctional services offices, network security measures did not allow data saving to browser caches; this prevented respondents from accessing the survey at all, depending on the firewalls in place at their facility. The research team collaborated with Qualtrics support, a team of testers, and contacts in each jurisdiction to implement collaborative solutions to maintain anonymity, while preserving the functionality of the survey by allowing responses to be saved directly to Qualtrics rather than a local browser cache.
The solution required participants to generate a randomized access code to serve as a unique identifier for Qualtrics prior to beginning the survey. Generated codes were automatically associated with one default email address, and a contact list was created based on this information. As a default email address was used for all participants across all versions of the survey, there was no way a participant could be re-identified based on their responses alone. Respondents were instructed to save their access code to re-access the survey as needed. The solution was propagated for each jurisdiction and retested the solution to ensure workability. The research team relied on the use of private browsers such as Google Chrome Incognito to replicate the user experience on secured workplace networks. Collaborators on site in each jurisdiction also participated in the testing phase of each survey, ensuring that as much as possible survey accessibility issues were addressed prior to the start of recruitment.
We also acknowledged the challenges for participants in completing a long survey of potentially stressful questions regarding their mental health, well-being, and employment perspectives. Each version of the survey included contact information for relevant mental health and wellness resources specific to their jurisdiction. The same resources were reiterated throughout the survey to facilitate participant awareness, particularly after questions about suicidal ideation, planning, and/or attempts.
In certain jurisdictions, employers wanted to ensure participants were paid for time spent participating, even if they did not complete the survey during their regular work shift. The research team supported such efforts by collecting contact details of participants separate from the survey responses. Respondents who completed the entire survey were shown a screen confirming the submission of their responses, and then given a link to a separate Qualtrics-hosted survey. The second survey prompted respondents to enter their contact and employment details to receive payment for their participation time. Responses to the second survey were then provided to the employer to facilitate participant compensation.
Collecting Data in Times of Uncertainty: COVID-19 Context
The CWMH was originally designed to survey all 13 provincial and territorial correctional systems concurrently after the Ontario survey; however, the concurrent data collection proved unfeasible for multiple reasons. Engagement with stakeholders in each jurisdiction underscored the diversity of services regarding processes for consultation, content review, piloting, and final approval. Indeed, correctional services and practices vary across Canada (see Ricciardelli, 2019 for a review of services in the Appendix), and the collected dataset allows for potentially important and unprecedented comparisons across systems. We worked with each correctional service from the initial outreach stages through to launch dates to ensure the process was inclusive and representative of the unique and overlapping needs of each province or territory. The study was launched in each location based on a timeline set by leadership in each service.
We completed surveying correctional services in seven jurisdictions by Spring, 2020; specifically, Ontario, Manitoba, Saskatchewan, Newfoundland & Labrador, Nova Scotia, New Brunswick, and Yukon Territory. COVID-19 was declared a global pandemic by the World Health Organization (WHO) on March 11, 2020 (World Health Organization, 2024). Accordingly, we were required to pause data collection for nearly 18 months to comply with guidelines put forth by the Memorial University of Newfoundland and service partners. During the pause, we ensured all surveys for the remaining jurisdictions were ready for imminent launch upon the restrictions being lifted. The pause also introduced a new dynamic to the study; namely, the ability to cross-sectionally examine differences in mental health disorder prevalence pre- versus one year into the COVID-19 pandemic. We restarted data collection Fall, 2021, fully completing data collection by early Spring, 2023.
The study group (comprising a national sample) and the emergence of COVID-19 informed and changed our processes of data analyses in four ways. First, we wrote articles based on initial data collected from the province of Ontario, both qualitative and quantitative. Second, we wrote articles based on qualitative data collected from six subsequent provinces and territories to inform the contexts and contents of their work experiences, culture, and mental health frameworks pre-COVID-19. Third, we are writing articles based on quantitative data with comparisons between a combined “pre” COVID-19 dataset relative to a combined “during” COVID-19 dataset and until May, 2023 in the “recovery” phase. The comparisons are necessary to assess for possible differences that may be associated with impacts of COVID-19 on CWs. Fourth, we wrote articles based on qualitative data about the various impacts on CWs “during” COVID-19 and to assess for differences in contexts and contents of work experiences, culture, and mental health frameworks during-COVID-19.
Discussion
We first conducted a study of CWs in Ontario, Canada, establishing our methods before replicating 12 times across the remaining Canadian provinces and territories. Replication remains a key for supporting generalizability of results (Haig, 2022), which is the essence of psychology and other related disciplines as a “cumulative science” (Flora, 2020). We argue our replications have robustly supported evaluations of correctional mental health and wellness, underscoring early (Carleton et al., 2018a) and subsequent results evidencing CWs experience mental health disorders and challenges more frequently than the general population (see Ricciardelli et al., 2024). The numerous replications evidence homogeneity among Canadian CW mental health challenges, despite variability with respect to jurisdictions.
We worked collaboratively with unions and Ministries/Departments overseeing correctional services to strengthen recruitment. We also acknowledge how the COVID-19 pandemic impacted participation, as jurisdictions surveyed during the pandemic had lower participation likely due to public health measures impacting occupational responsibilities. Singh et al. (2020) described health research as a “casualty of the pandemic” where much research was significantly diminished or suspended entirely “because of either COVID-19-related legal restrictions or logistical, staffing or operational concerns” (p. 625). In the context of the current study, COVID-19 appears to exacerbate ethical and practical challenges with respect to data collection.
We emphasize the importance of how collaborative research designed with relevant stakeholders is instrumental to success, especially when unique and unprecedented challenges arise (i.e., technological and pandemic). Our emphasis aligns with methodological arguments found in the Participatory Action Research literature (Greenbaum et al., 2020). Our research design allowed us to administer surveys that met the unique needs of the different services and to provide data that ensured the desires of services were represented and responded to the challenges each service faced both collectively (i.e., mental health) and uniquely (i.e., methamphetamine and fentanyl crisis). We also employed a mixed-methods approach, with quantitative tools to assess mental health disorder prevalence, and qualitative tools to help contextualize statistical results. Our intention and research questions were always to identify the scope of challenges and give voice to the interpretations of those experiencing the challenges, collectively informing efforts toward effective solutions.
Limitations
Perhaps our most important limitation was based on our inability to survey all 13 jurisdictions simultaneously while accommodating required customizations. The COVID-19 pandemic also paused the study, impacting correctional services and our data collection in unpredictable ways. Internal factors creating limitations included individual and organizational selection biases (i.e., who was surveyed was very dependent on interest as well as the organization's process, access, and intention), as well as attrition during survey completion due to survey length. Other limitations included the sampling method precluding knowing the response rate and using anonymous online reliable and valid self-report of current symptoms rather than clinical interviews and including lifetime assessments. We also are limited by the smaller potential sample size in select territories and provinces where there are smaller correctional systems and fewer employees. Participation was lower during COVID-19, which might reflect more people being on leave or staffing changes tied to the pandemic. Using cross-sectional data also prohibits discussions of causality. Qualitative data are limited in that we did not conduct interviews and thus had no opportunity to probe for clarification or additional information. Future interview-based research should be conducted to provide more robust context for informing mental health disorder prevalence and help-seeking among Canadian provincial and territorial CWs.
Conclusion
To date, our national study is the most comprehensive study of CW mental health in Canada and internationally. The investigation was based on empirical needs for replication and extension of previous work to test for generalizability and variability of mental health assessments across Canadian provincial and territorial correctional systems in Canada. The mixed-methods data facilitated nuanced and contextualized assessments of CW mental health and related experiences across jurisdictions. We worked through extensive challenges and interruptions to complete the data collections, and we will continue to examine and evaluate the lived experiences of CWs, focusing on the interconnections and uniqueness that illuminate the CW workplace and CW wellness. The breadth and depth of the data collection will help to clarify similarities and differences among CWs, stratified by jurisdiction and occupational subgroups, importantly extending the growing body of literature on CW mental health in Canada. As is often needed when undertaking large research projects, we encourage resilience and teamwork among scholars invested in mental health research, treatment, and organizational solutions for correctional services and PSP, more broadly. We hope our detailing of the trials and successes of this work will be useful to the research community who may encounter similar challenges going forward.
Footnotes
Authors’ Note
Authors’ contributions
All authors meet the ICMJE criteria for authorship, RR responsible for conceptualization, research design, obtaining funding, data analysis, data collection, drafting, editing, and ethical approval, collaborator recruitment and management, and project administration and supervision. EA responsible for project administration, TLT responsible for data analysis. MSJ responsible for data analyses. SD responsible for data analyses. RC responsible for data analyses, MSC responsible for data analyses, MC responsible for drafting and reviewing. BB responsible for data coding and analyses. KH responsible for project administration, RNC responsible for conceptualization, research design, and editing. TOA responsible for project oversight and project supervision. All authors responsible for writing the manuscript. All authors responsible for editing and revising the manuscript. All authors have read and approved the manuscript.
Acknowledgements
The authors express their appreciation and gratitude toward all those informing the research design and implementation of each study, which includes government officials, correctional workers, community and professional stakeholders, unions, research assistants, colleagues, and participants.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Workplace NL and the Government of Alberta as well as the Canadian Institute of Health Research (a catalyst grant).