
Abstract
This study tested the impact of a diet and exercise intervention on its impact on self-rated sleep, health, and wellbeing among a sample (n = 64) of UK police officers and staff. Using a pre- and post-intervention testing design, UK police officers and staff were exposed to a month-long diet and exercise intervention. Measurement before and after the intervention included self-rated sleep quantity, sleep quality, and sleep latency (how long it took to fall asleep), as well as self-rated satisfaction with health and wellbeing. Study results revealed that the training significantly improved officer self-reported sleep (+31 minutes per 24 h period) and reduced self-reported sleep latency (−12 minutes). Furthermore, ratings of satisfaction with health and wellbeing improved. This study indicates that promoting diet and exercise among police officers and staff might be beneficial to sleep health. Health and safety management has traditionally been a reactive process. However, a more proactive approach to risk management has many benefits in terms of improving quality of life, along with reputational, budgetary and community safety benefits. Sleepiness is both a personal and organizational risk factor, hence mitigating sleepiness should be approached as a shared responsibility.
Introduction
Policing is a professional group that is marked by sleep restriction, chronic fatigue, and long-term health and wellbeing problems (Allison et al., 2022; Amendola et al., 2011; James et al., 2017; Vila, 2000; Violanti et al., 2013). This in part due to the stressful nature of policing (Hesketh et al., 2015) and in part because of working extended shifts that do not always align with the human body’s biological drive to sleep at night and be awake during the day (Belenky et al., 2003, 2014; Dement and Vaughan, 1999; Satterfield and Van Dongen 2013). The consequences of sleep restriction for police include performance, safety, and health deficits and have been well documented (James et al., 2017; Peterson et al., 2019).
From a performance perspective, sleep restriction impairs moral decision making, which is critically important for how officers and staff interact with members of the public (Belenky et al., 2014; James et al., 2018). From a safety perspective, sleep restriction has equivalent effects to being drunk, whereby being awake for 24 h is comparable to a 0.10 blood alcohol content (BAC) rate (Dawson and Reid, 1997; Williamson and Feyer, 2000). From a health perspective, police officers and staff are at increased risk of disease compared to members of the general public. For example, policing is associated with increased risk for cardio-vascular, gastro-intestinal, and metabolic diseases (James et al., 2017), sleep disorders (Rajaratnam et al., 2011; Vila, 2000, 2006), and psychological disorders such as post-traumatic stress disorder, substance use disorder, and suicide (Violanti et al., 2013).
Given that shift work is unavoidable in policing and that the job is inherently stressful, strategies for mitigating these effects and safeguarding officer health and wellbeing are critical. One major approach has been fatigue management training and sleep health education (James et al., 2024). Several policing studies have investigated the effectiveness of this approach, with some promising results. For example, researchers at the National Institute of Occupational Safety and Health (NIOSH) developed an online fatigue management training program and then tested its effectiveness using a sample of police from across the United States. They found that the program significantly reduced sleep latency (time to fall asleep) and nighttime awakenings. The program also resulted in reductions to sleepiness, nightmares, difficulty staying awake during the day, and difficulty getting things done (James et al., 2022).
A further study to investigate a fatigue training intervention was conducted within the Royal Canadian Mounted Police (RCMP). Researchers tested the impact of a 4-h in person training program covering the topics of sleep science, sleep disorders, and fatigue countermeasures and found that participants had significantly reduced symptoms of insomnia, and significantly increased satisfaction with sleep (James et al., 2017). The UK National Police Wellbeing Service - Oscar Kilo, has tested the impact of fatigue management training and found it to have a positive impact on members’ sleep, health and wellbeing (James et al., 2022a). Fatigue management training significantly increased sleep quantity by 25 minutes per 24-h period, from 6.9 hours before the training to 7.3 hours after the training. These results all suggest that fatigue management training shows promise in promoting officer wellbeing. The results also justify the exploration of additional strategies to promote police wellbeing, given the risks this population faces in both the day-to-day job and in their long-term health.
As a follow up to the Oscar Kilo fatigue intervention evaluation, the current study developed and evaluated a diet and exercise program, that is complementary to the fatigue management training. The health benefits of diet and exercise are extensive and universally acknowledged (Leske et al., 2024; Pranoto et al., 2024). Given the increased risk of cardiovascular, gastrointestinal, and metabolic disease among police employees (sworn and civilian: James et al., 2023), efforts to promote heart and gut health could increase police lifespan. Increased cardiovascular, gastrointestinal, and metabolic disease risk within this population have been associated with stress, shift work, reduced sleep, reduced physical activity, and poor dietary choices (Lockie et al., 2022). A comprehensive and holistic diet and exercise program could help reduce these risks in an elevated risk population. Further to this, the benefits show potential promise at contributing directly to sleep health and fatigue management for shift workers (Binks et al., 2020; Burrows et al., 2020), thus resulting in improvements to organizational effectiveness. Despite potential promise, few diet and exercise interventions have been evaluated within policing, and those that have tend to focus on weight loss versus holistic health and wellbeing including sleep health (Čvorović et al., 2018). The current study addresses this gap in the research literature.
Methods
The diet and exercise intervention evaluation used a within-subject design, taking baseline measurements from a convenience sample of 64 UK police officers and staff.
Participation was voluntary, and inclusion criteria were that participants had to be shift working police officers or civilian staff. Testing occurred in a police force in the North East region of England over a 3 month time frame in early 2023. The study was advertised within the force area by way of advertising posters and internal email communications.
Data was collected while participants were off shift via an electronic survey which was sent to all participants both at baseline and post intervention. We did not control when participants took the survey, and officers from multiple different shifts participated.
Baseline measurements consisted of a survey made up of the following validated instruments: The World Health Organization Quality of Life (brief) scale – WHOQOL- BREF to measure quality of life and other aspects of wellbeing including satisfaction with health, diet, and exercise (measured ordinally on 5-point scales with higher scores indicating higher satisfaction with health); The Epworth Sleepiness Scale (ESS) to measure sleepiness during waking periods including driving safety risks (measured continuously from 0 to 24 with higher scores indicating greater sleepiness and risk and typically 10+ representing the cutoff for excessive sleepiness); and the Pittsburg Sleep Quality Index (PSQI) to measure self-reported sleep health (sleep quantity measured continuously in hours and minutes asleep, sleep quality measured continuously from 0 to 21, and sleep latency or time to fall asleep measured continuously in minutes). As such, the program was evaluated not just on its impact on perceived sleep and fatigue, but also on its impact on broader health and wellbeing outcomes.
The diet and exercise program was created specifically for this study, lasted for 1 month, and provided officers with recommendations on what to eat and when, and how to exercise and when. The program was emailed to participants. Several considerations here were important: (1) In both diet and exercise, members were given variety (a “menu” of sorts to choose from, rather than a recipe of exactly what to eat and how to exercise). This was important as not all people have the same tastes or get the same enjoyment out of a particular exercise regime. For example, yoga was encouraged, given its benefits for stress reduction as well as core strength, but variations and alternatives were provided for members who were not likely to get involved in yoga. (2) Peer support was encouraged and fostered to maximize buy in to and compliance with the intervention. This is an important consideration as behavioral interventions can be difficult to stick with, especially for members who are not accustomed to exercising and eating healthy food options. (3) Exercise bouts were no longer that 20 minutes, and did not require specialized equipment. Nor were meal plans expensive or time consuming to prepare. Where possible, bought / take out options were recommended that are nutritious. (4) Participants were instructed to limit nighttime calories to 250, given that the body is not designed to process food at night when our circadian rhythms dictate that we should be sleeping (James et al., 2017).
During the program, members were asked to keep a food, exercise, and sleep diary, which we used to track adherence to the program. After the month-long training intervention, follow-up measurements (the same as baseline) were taken from members to evaluate the effectiveness of the program.
Specific objectives were to investigate whether participation in the diet and exercise program impacted participant perceptions of quality of life, sleep health (quantity, quality, and latency or time taken to fall asleep), and waking sleepiness. Hypotheses were: (1) Following the intervention, participants would have significantly improved quality of life scores as measured by the WHOQOL- BREF. (2) Following the intervention, participants would have significantly increased self-reported sleep quantity, as measured by the PSQI. (3) Following the intervention, participants would have significantly reduced self-reported sleep latency (minutes taken to fall asleep) as measured by the PSQI. (4) Following the intervention, participants would have significantly improved self-reported sleep quality, as measured by the PSQI. (5) Following the intervention, participants would have significantly reduced self-reported waking sleepiness scores as measured by the ESS.
Descriptive statistics were generated for all hypotheses, and then t-tests were used to test for statistical significance in continuous outcomes (sleep quantity, sleep quality, sleep latency, waking sleepiness), with Cohen’s d to estimate effect sizes. Ordinal outcomes (quality of life variables) were tested for significance using Mann Whitney with odds ratios (OR) to estimate effect sizes.
Results
Sixty-four members participated in the intervention, with strong adherence, monitored via their daily diaries (approximately 75% adherence). 26% were between the ages of 35 and 44, with another 22% between 45 and 54. There was approximately 50% women, and 25% police staff (not sworn officers). All but two participants were British-White. The most frequently observed shift pattern for sworn officers in the sample was 12-h shifts, following a 2-day, two-night with a 7a.m. (day) start rotating schedule, a so-called tidal rota. Police staff predominantly worked standard 9a.m. to 5p.m. work days with no night shifts and were in a mixture of roles, including crime scene management and control room staff.. About 30% of the sample had worked some overtime in the prior week to testing, however only one had done more than 8 hours of overtime. The most typical commute time was less than 30 minutes.
Quality of life
Quality of life (WHOQOL) results (N = 64).
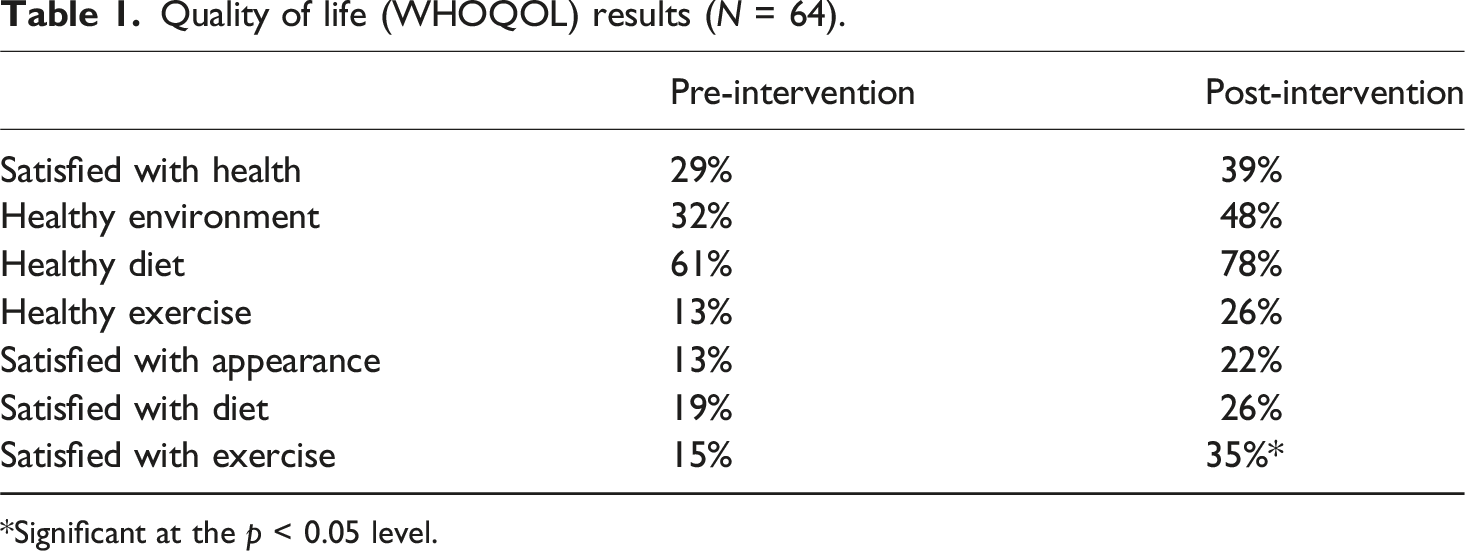
*Significant at the p < 0.05 level.
Sleep health
The PSQI allowed us to test for various dimensions of self-reported sleep health. The first was self-reported sleep quantity per 24-h period, which increased from a mean of 6.36 hours (382 minutes), SD = 51 minutes before the training, to 6.88 hours (413 minutes), SD = 1.23 hours after the training (see Figure 1). This self-reported increase of 31 minutes per 24-h period is encouraging, and consistent with our previous findings from the fatigue management training evaluation. This increase was statistically significant (t = 2.12; df = 72; p = .02) with a moderate effect size (Cohen’s d = 0.53). Average self-reported sleep quantity per 24 hours before and after the diet and exercise intervention (N = 64).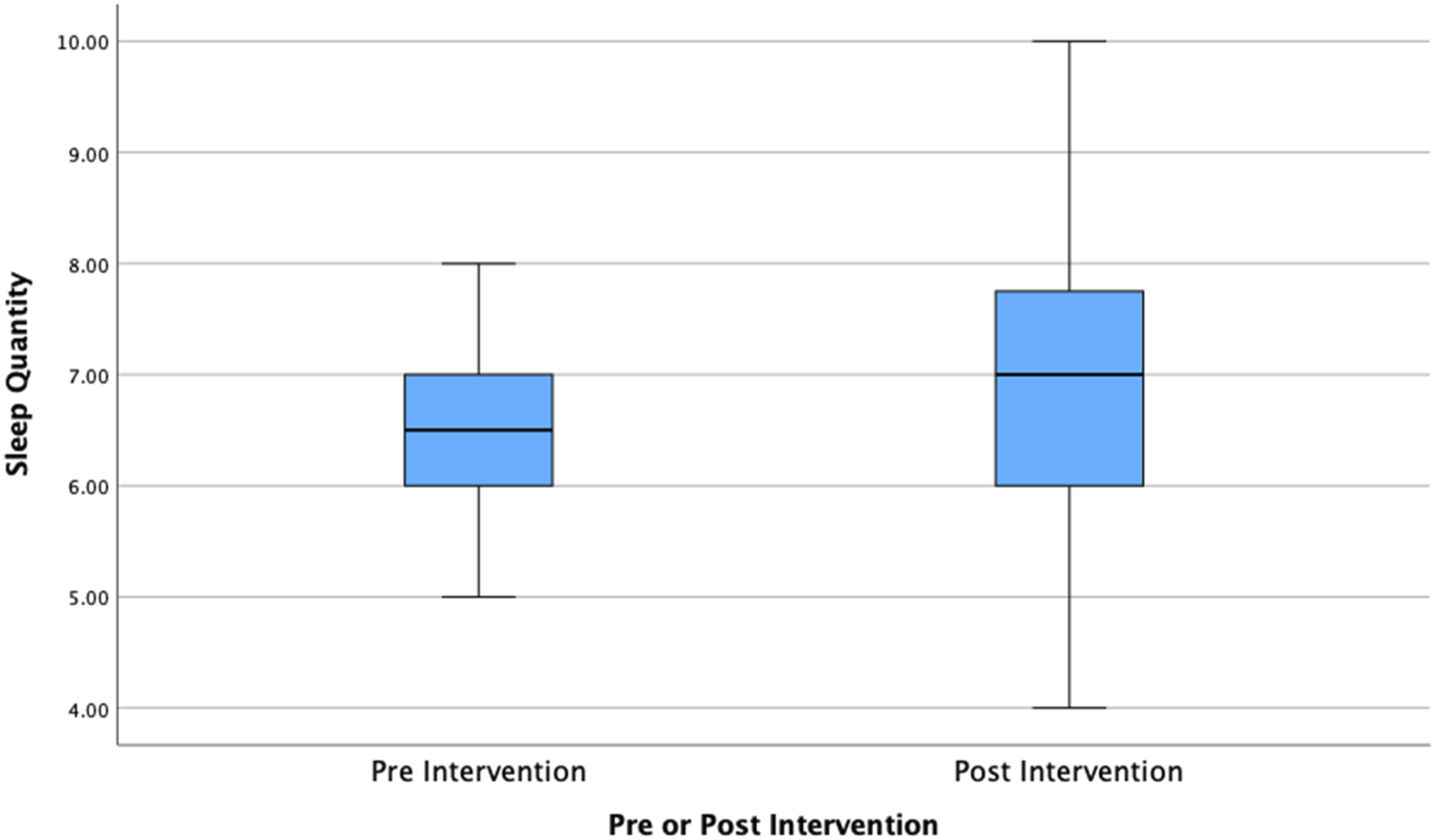
There were also improvements to self-reported sleep latency (amount of time it took participants to fall asleep) following the intervention. The PSQI data revealed that police officers and staff went from taking on average 35 minutes (SD = 30) to fall asleep before the training to 23 minutes (SD = 19) to fall asleep after the training (see Figure 2). This approximate 12-min reduction was statistically significant (t = 1.66; df = 69; p = .03) with a moderate effect size (Cohen’s d = 0.43). Self-reported sleep latency (time in minutes to fall asleep after going to bed) before and after the diet and exercise intervention (N = 64).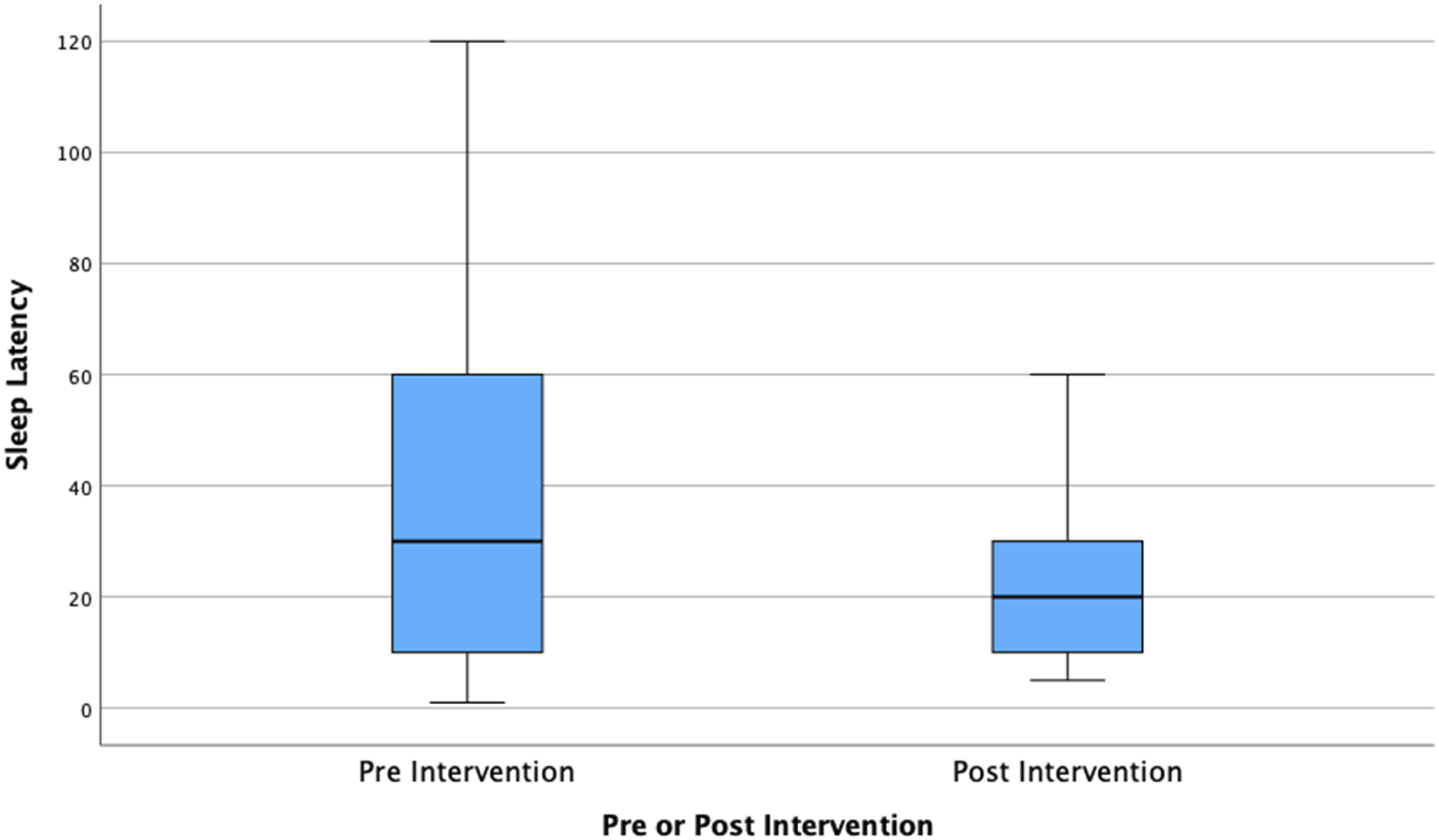
We did not find a statistically significant improvement to self-reported sleep quality following the training intervention.
Daytime sleepiness
To measure daytime sleepiness the ESS was used. This calculates the risk of falling asleep while doing various activities, including the critical activity of driving. It is measured on a scale of 0–24. Before the intervention, participants average score was 6.47 (SD = 4.34) and after the intervention it was 5.32 (SD = 4.02). Although this difference moved participants from the “higher than normal sleepiness” category to the “lower than normal sleepiness category” it was not statistically significant at the p < .05 level, thus observed improvements might be due to chance (Figure 3). Self-reported daytime sleepiness before and after the diet and exercise intervention (N = 64).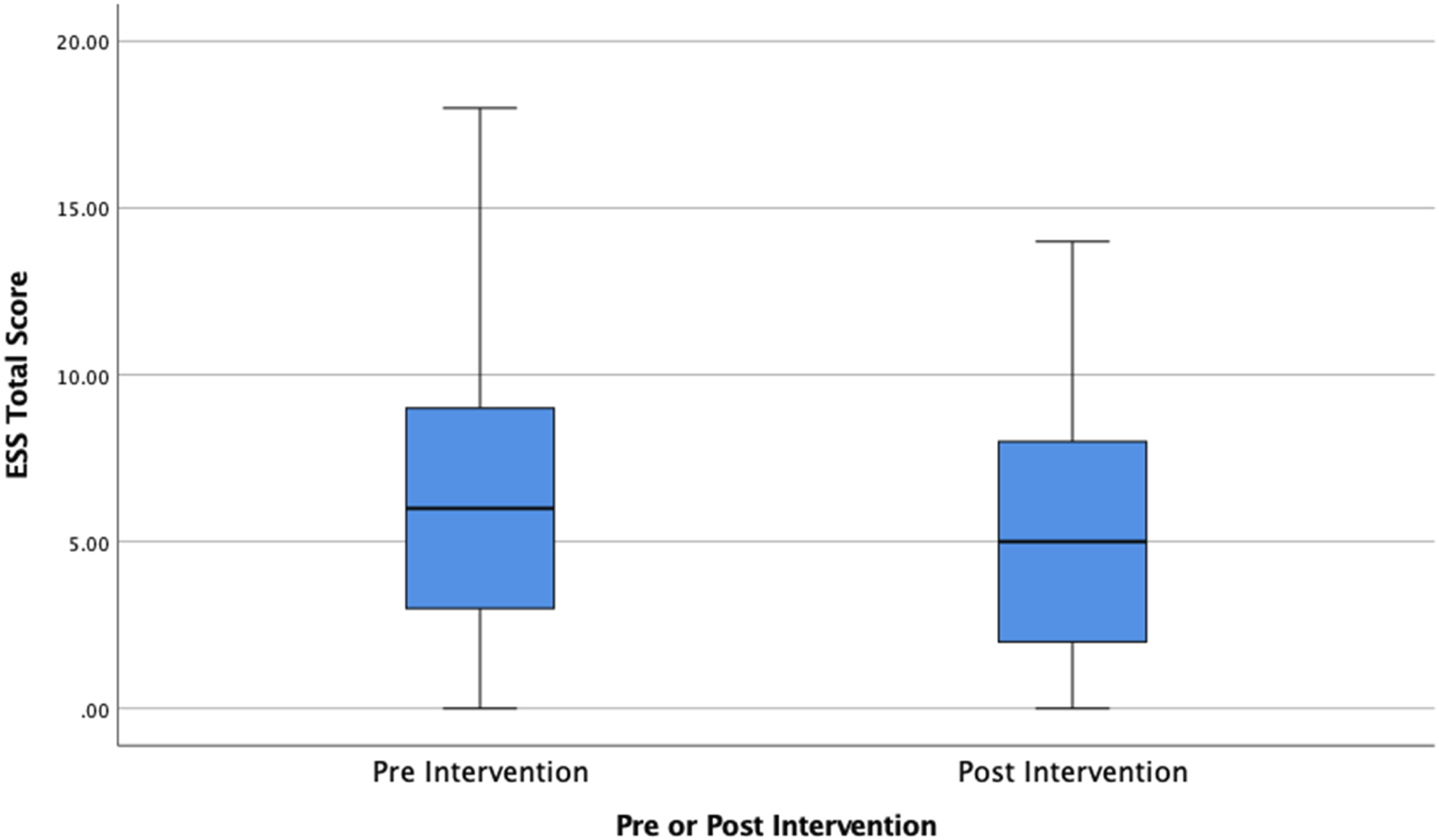
Discussion
This study evaluated the impact of a diet and exercise intervention on police officer and staff self-reported sleep, health, and wellbeing. Several notable findings are worth considering from this evaluation. The intervention had a significant and positive impact on self-reported sleep quantity and latency. Participants reported that sleep quantity increased by 31 minutes per 24 h period following the intervention, which was not only statistically significant, but also a clinically meaningful result (Dawson et al., 2021) with a moderate effect size. It is possible that the diet and exercise program had a positive impact on perceived sleep directly via improvements to diet and exercise. That participants also had significant reductions in self-reported sleep latency or time to fall asleep supports this possibility. It is also possible that given the majority of the sample worked at least some night shifts, the reduction in nighttime calories to 250 between the hours of 10p.m. and 6a.m. may have resulted in better ability to catch up on sleep during the day. Additional research is required to better understand the potential mechanisms by which a diet and exercise program can specifically improve police officer and staff sleep.
The subject of sleep health has featured as a cause for concern in all the recent Wellbeing surveys of UK policing. Graham summarized these in a report for the UK Government addressing the police workforce (Graham et al., 2023). The majority of frontline officers and a large number of civilian staff work irregular hours or rotating shift patterns. This in itself is known to cause sleep reduction and disturbances, and is associated with increased physiological sleepiness, along with performance degradation, impaired decision making, accidents and various health problems (Vila, 2006). Improved nutrition, along with a physically active lifestyle can help to mitigate these associated health risks. Within this study the only significant quality of life improvement we observed following the intervention was to satisfaction with exercise, despite increased numbers of participants claiming satisfaction with all elements of measured quality of life following the intervention. Improvements to police officer and staff health and wellbeing were also observed. It is possible that the research design was unable to detect anything but moderate to large effect sizes. Additional research with larger samples is needed to explore the positive impacts of a diet and exercise program for promoting general health and wellbeing.
A notable limitation of the study was the simple pre and post design. Lack of a control group restricts our ability to determine generalizability of results, or whether temporal factors impacted participants during the testing time frame. Given some promising results, future research could employ randomized control trial (RCT) designs to test the impact of this type of intervention more rigorously on police sleep, health, and wellbeing. Another limitation was reliance on subject self-report data for sleep quality. Future research should consider objective measures of sleep monitoring such as actigraphy. Relatedly, diet and exercise were also tracked via self-report, and subsequent studies should consider more objective measures such as step monitoring and meal photo logging. A third limitation was that our convenience sample likely resulted in selection bias (those particularly interested in diet, exercise, and sleep might have been more likely to sign up) and potential positive response bias. Finally, we did not explore persistence of intervention related behavior change. Future research should investigate result longevity to determine dosage needed for sustainable program success.
Health and safety management has traditionally been a reactive process, however, a more proactive approach to risk management has many benefits in terms of improving quality of life, along with reputational, budgetary and community safety benefits. Sleepiness is both a personal and organizational risk factor (Schutte, 2010), hence mitigating sleepiness should be approached as a shared responsibility. Interventions such as this, supported by the organization, not only assist with ensuring employees are well rested and performing at their best, but also improve the relationship between the organization and employees, by improving Perceived Organizational Support (POS) (Eisenberger et al., 1986).
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.