
Abstract
Professional quality of life (ProQoL) variables, compassion fatigue (CF), compassion satisfaction (CS) and burnout are understudied in the police population. Here, we examine any associations between ProQoL and anxiety, depression and personal QoL. Study 1: A cross-sectional survey (N = 100) demonstrated CF and burnout are significantly associated with higher anxiety and depression, whereas CS is significantly associated with lower anxiety and depressive symptomology. When controlling for CS, CF is still significantly associated with higher anxiety and depression. Study 2: Semi-structured interviews (N = 6) revealed themes of perceived awareness and personal impacts of ProQoL. Police interventions should focus on ProQoL variables as the root cause of common mental health complaints.
Introduction
Police work can be a dangerous and stressful occupation, as it involves routinely dealing with threats to safety. Police officers are more susceptible to mental ill-health than the average civilian, with 90% of police personnel having experienced stress or mental ill-health at work (MIND, 2016). Police officers respond to potentially traumatic incidents and are required to help traumatised individuals as part of their job (Jacobson, 2012). Secondary exposure to trauma can have detrimental impacts on front-line workers’ wellbeing (Berzoff and Kita, 2010; Birch et al., 2017; Craig and Sprang, 2010); however, the positive and negative effects of trauma exposure in police personnel is an understudied area. There is a need for additional research regarding the impacts trauma exposure and stressors have on police officers. This multi-study paper aims to examine and explore associations between professional quality of life variables (ProQoL; Stamm, 2002), namely compassion fatigue (CF), compassion satisfaction (CS), burnout and common mental health complaints in UK police officers from the northwest of England.
Compassion fatigue, compassion satisfaction and burnout
Compassion fatigue is a detached state felt when an individual routinely deals with distressed individuals and is often referred to as the ‘cost of caring’ (Figley, 1995). CF has been described as the convergence of secondary traumatic stress and cumulative burnout (Cocker and Joss, 2016), which can impact personal and professional life. CF shares symptoms with post-traumatic stress disorder (PTSD), but rather than symptoms resulting from personal trauma, symptoms are caused by occupational stressors, such as attending a sudden death or dealing with a child sexual abuse case. The term ‘compassion satisfaction’ can describe feelings of increased motivation and satisfaction from helping individuals who have experienced adverse events, which in turn can improve occupational performance and quality of life (Stamm, 2002). Burnout is conceptualised as prolonged occupational stress (OS) that has not been successfully managed (World Health Organisation, 2020). There is a wealth of literature around CF, CS, and burnout among health care professionals (Hooper et al., 2010; Ray et al., 2013; Van Mol et al., 2015). However, comparable literature on police officers is limited, even though they too face occupational stressors such as poor management, lack of support from senior ranks, and increased workload (Purba and Demou, 2019).
Compassion fatigue, compassion satisfaction, burnout, anxiety and depression as an integrating framework
Research has sought an integrating framework for CF, CS, burnout, anxiety and depression in emergency service personnel. For instance, a two-part Australian study of nurses found that burnout and CF positively correlate with anxiety and depression levels, while CS negatively correlates with anxiety and depression levels (Hegney et al., 2014). A qualitative follow-up study (Drury et al., 2014) identified the importance of social networks, leadership, and coping strategies to build psychological wellbeing in nurses. The findings suggest that personal resilience is heightened by robust social and collegial support. The Risk Reflective Assessment Model (RRAM; Hegney et al., 2014) states that professional quality of life factors CF, CS and burnout interact with potential contributing factors of anxiety and depression. To date, the RRAM has been applied to explain factors influencing nurses’ wellbeing (Hemsworth et al., 2020) but has not yet been extended to other emergency service personnel, such as police officers. The RRAM could be applicable for police officers, as both roles involve the exposure to stressful situations and require a display of compassion towards service users.
Compassion fatigue, compassion satisfaction and burnout in police officers
Police officers can experience CF and CS facing critical incidents such as violent offenders and maltreatment of children (Cross and Ashley, 2004). Research suggests years of service in the police force positively correlate with CF (Battle, 2011). In addition, officers who have had a previous perceived trauma also report higher rates of CF and burnout and lower rates of CS (Battle, 2011). Literature states CS and burnout are significant predictors of CF in police officers (Papazoglou et al., 2019), while another study among police officers identified a significant negative correlation between CF and CS (Grant et al., 2019).
Compassion fatigue is likely to occur in police officers who are unaware or ignore the presence of its cues and continue to perform their duties without seeking help (Papazoglou et al., 2020). If symptoms of CF are ignored over time, this could have detrimental effects on police officers’ wellbeing. CF may also worsen through lack of appreciation from the community and organisational stressors, resulting in mental ill-health (Papazoglou et al., 2020). Given the prevalence of CF and CS in police-related work, it is necessary to examine the extent to which these variables are associated with common mental health complaints.
Anxiety and depression in police officers
Mental illness in the workplace is a significant ‘economic burden’; it is estimated 16 million days are lost annually due to stress, anxiety, and depression (Office of National Statistics, 2020). Highly stressful occupations, such as police work, can negatively impact physical and mental health (Phythian et al., 2022). A study of 534 UK police officers revealed that 12% disclosed a mental health diagnosis and 26% suffered with mental illness (Jetelina et al., 2020). These aforementioned factors can cause dissociation and attentional deficits (Wang et al., 2020), thus difficulty making acute decisions and negatively impacting police officers’ occupational performance (Arnetz et al., 2009; Covey et al., 2013).
Police officer suicide rates are on the rise with an average of 23 officers’ each year taking their own lives between 2010 and 2017, representing an increase of 33% since 2009 (Townsend and Savage, 2019). Therefore, it is imperative that mental ill-health in police populations is addressed. Literature recognises a mental health stigma within the police; consequently, seeking help is avoided due to presumptions from others that this behaviour is malingering (Bell et al., 2021). There has been a gradual shift within the emergency services towards a pro-active approach to promoting officers' wellbeing (Wild et al., 2020). Since 2017, Oscar Kilo (OK), The Blue Light Wellbeing Framework (BLWF), and The National Police Wellbeing Service (NPWS) have been launched in the UK, demonstrating a national effort to promote wellbeing in police officers (College of policing, 2018). However, it has been observed that the delivery of such frameworks can be inconsistent and it is unclear which programmes have undergone external evaluation, thus having little empirical support (Phythian et al., 2022).
Work–home interference
Quantitative workload has been consistently found to be a predictor of work–home interference (WHI; Peeters et al., 2004; Dikkers, 2008). Negative workload reactions are not only an antecedent to WHI but also a consequence (Dikkers et al., 2007). A Dual-Process Model of WHI (DPM; Bakker and Geurts, 2004) proposes that job demands are related to feelings of exhaustion, and job resources to work-related flow. Job demands, such as a high workload, predict higher anxiety and depression levels in employees, while job resources, such as social support from colleagues or a positive leadership climate, buffer the effect of job demands in terms of reduced emotional exhaustion, anxiety and depression levels (Demerouti et al., 2001). The DPM has been used to explain WHI among police officers (Martinussen et al., 2007). Increased WHI over time and for a long duration can lead to a deterioration in physical and mental health of police officers (Geurts et al., 2003; Van Hooff et al., 2005). Previous qualitative studies have analysed police officers' experiences of social interactions following traumatic incidents (Evans et al., 2013), although they have not explored how professional quality of life variables may impact on the mental health and personal lives of police officers.
COVID-19 pandemic
During the COVID-19 pandemic, UK police officers were designated ‘essential workers’. Essential workers were at higher risk of exposure to the virus due to being in close contact with others, even during national lockdowns when infected cases and death tolls were high (Office of National Statistics, 2020). The pandemic obliged officers to be continuously more hypervigilant of their own environment and who they were in contact with at work to protect themselves and their families. Daily exposure to the added stress, safety protocols, and social distancing policies may have limited officers' ability to cope in the role by exasperating everyday work stressors (Stogner et al., 2020; Tehrani, 2022).
Aims of study
This research will be the first study to examine the associations between CF, CS, and burnout, and anxiety and depression levels in UK police officers and to explore how police officers experience these quality of life variables. The study aims to assist in decision-making, regarding the strategies that could be implemented by forces to build and maintain psychological wellbeing among police personnel. Here, we present data from two studies. Study 1 examines CF, CS, and burnout and their associations with anxiety and depression. It is hypothesised that (1) CF, CS, and burnout will be associated with anxiety among police officers; (2) CF, CS, and burnout will be associated with depression among police officers; and (3) CF will still be associated with higher anxiety and depression, even when CS is controlled for. Study 2 aims to contextualise the findings from Study 1, providing a complementary interpretation of officers' awareness of CF, CS, and burnout and exploring the personal impacts of occupational stress.
Study 1: Methodology
The study used a nested mixed methods design. This consisted of a cross-sectional survey (Study 1), with participants invited for additional interviewing after completion of the survey (Study 2; DeLuca and Rosenblatt, 2010). Study 1 and Study 2 took place in July and August 2020. Quantitative and qualitative raw data from this study can be found on the Open Science Framework (OSF), along with supporting documentation (osf.io/mn26b). All procedures were approved by Manchester Metropolitan University’s ethical review panel.
Design
Study 1 used a regression design with three independent variables (IV; CF, CS, and burnout) and two dependent variables (DV; anxiety and depression). Data was collected following the first UK lockdown in response to COVID-19. Previous literature outlines the strains of being a front-line worker during the pandemic which illustrates the importance to control for the effects of the pandemic on police officers in this study, as it may play a role in their mental wellbeing.
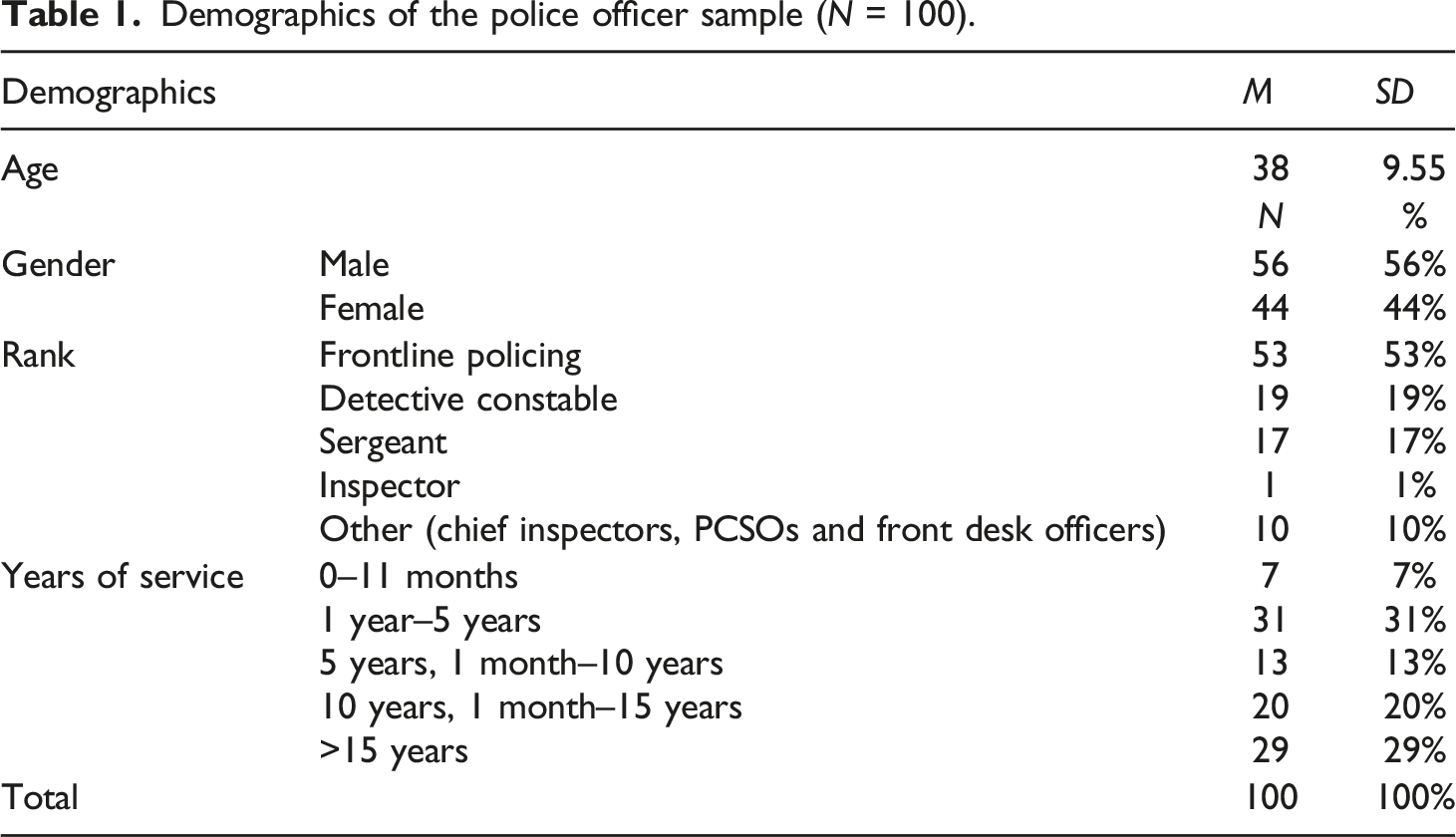
Participants
Demographics of the police officer sample (N = 100).
Materials
Compassion fatigue, compassion satisfaction and burnout
The Professional Quality of Life Scale (ProQoL5; Stamm, 2002) was used to measure CF, CS and burnout symptoms in the last 30 days on a scale from 1 (never) to 5 (very often). This is a 30-item self-report scale containing three 10 item sub-scales for CF (α = 0.82), CS (α = 0.91) and burnout (α = 0.75). ProQoL5 items include: ‘I can’t recall important parts of my work with trauma victims’ (CF), ‘I believe I can make a difference through my work’ (CS) and ‘I feel bogged down by the system’ (burnout). The wording of items on the measure were altered slightly for the police sample. For example, the original ProQoL5 item: ‘I find it difficult to separate my personal life from my life as a (helper)', was adapted to “police officer”. The ProQoL5 has been psychometrically validated in various studies (Stamm, 2002) and is a reliable measurement tool, with alpha coefficients ranging from 0.85 to 0.94 (Bride et al., 2007; Stamm, 2002).
Anxiety
The Generalised Anxiety Disorder-7 (GAD-7; Spitzer et al., 2006) assessed self-reported anxiety. Participants rated how often they have been bothered by various problems over the last 2 weeks, on a four-point scale from 0 (not at all) to 3 (nearly every day). The GAD-7 has good reliability and validity (Spitzer et al., 2006), which was reflected in the current study (α = 0.92).
Depression
The Patient Health Questionnaire-9 (PHQ-9; Kroenke et al., 2001) was implemented to assess self-reported depression. The PHQ-9 and the GAD-7 are designed to be used in concord, as they use the same 4-point scale, with the same categories for mild, moderate, moderately severe and severe depression symptomology. One item on the PHQ-9 relating to suicidal ideation was removed in this study, due to its anonymous nature. The PHQ-9 is regarded as a reliable and valid measure of depression severity (Kroenke et al., 2001), with the remaining eight items demonstrating high reliability (α = 0.90). Demographic data was collected from participants including age, gender, rank, and years of service. Additional COVID-19 related questions were asked to assess the extent to which the COVID-19 pandemic affected participants quality of life, which may have interfered with their self-reported psychological distress.
Data analysis
To assess whether CF, CS and Burnout are associated with anxiety and depression, six hierarchical regressions were conducted using SPSS 25. Self-reported anxiety and depression were the DVs (three models with anxiety as the dependent variable and three models with depression as the dependent variable). Demographic control variables (age, gender, rank and years of service) were entered in step one, with COVID-19 variables entered in step two, followed by the independent variables (CF, CS and burnout) in step three. IVs were entered in three separate models and measured separately for their association with both anxiety and depression because it was recognised that measuring all IVs in the same model could have raised issues with multicollinearity. A further regression analysis was run to assess whether CF was still associated with higher anxiety and depression when CS was controlled for in the model. If CF is no longer associated with higher anxiety and depression levels when CS is controlled for, this will indicate symptoms of CS reducing CF.
Study 1: Results
Descriptive statistics
Descriptive statistics for compassion fatigue, compassion satisfaction, burnout, anxiety and depression (N = 100).
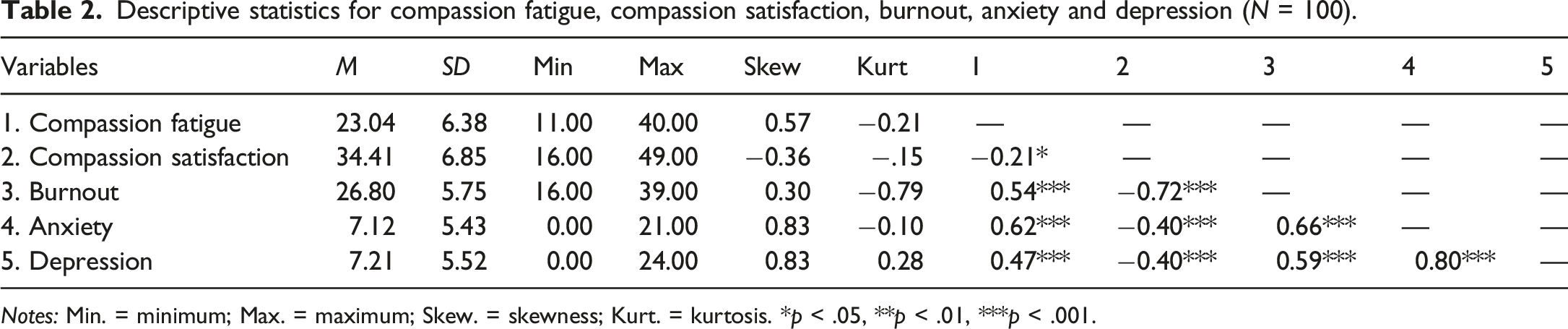
Notes: Min. = minimum; Max. = maximum; Skew. = skewness; Kurt. = kurtosis. *p < .05, **p < .01, ***p < .001.
Hierarchal regression analyses
Summary of the hierarchal regression analyses for compassion fatigue, compassion satisfaction, and burnout and their associations with anxiety (N = 100).
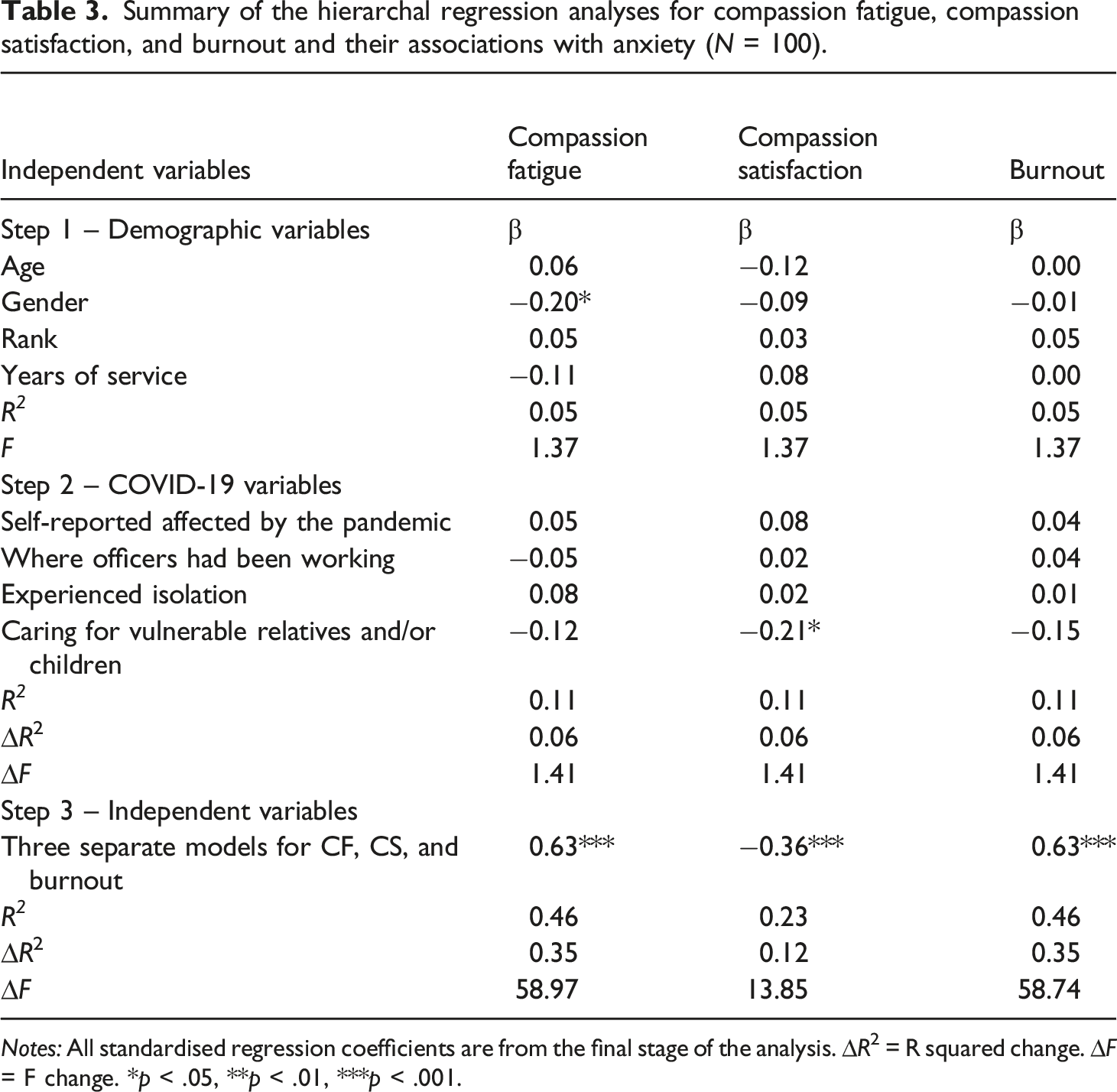
Notes: All standardised regression coefficients are from the final stage of the analysis. ∆R2 = R squared change. ∆F = F change. *p < .05, **p < .01, ***p < .001.
Summary of the hierarchal regression analyses for compassion fatigue, compassion satisfaction, and burnout and their associations with depression (N = 100).
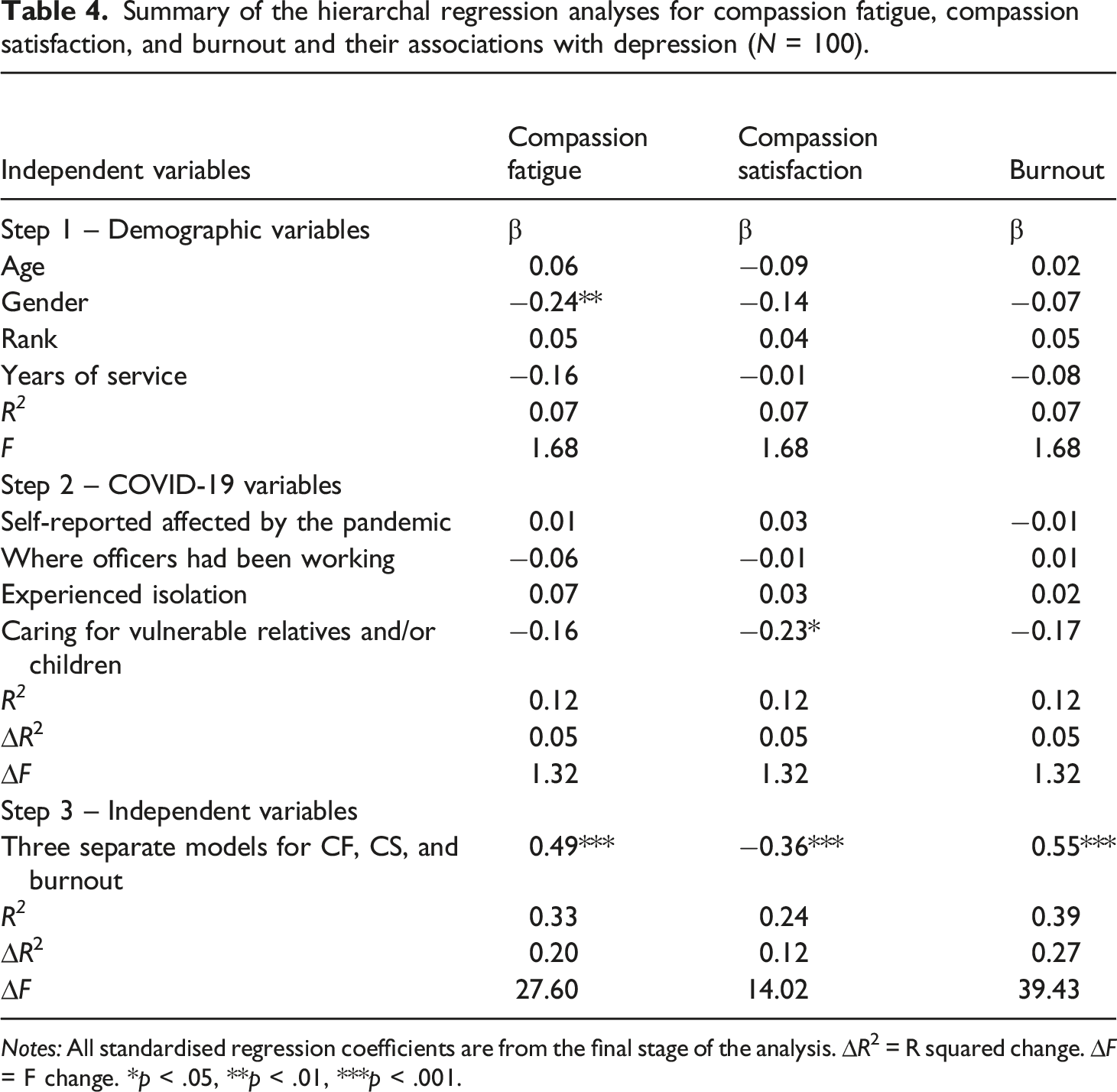
Notes: All standardised regression coefficients are from the final stage of the analysis. ∆R2 = R squared change. ∆F = F change. *p < .05, **p < .01, ***p < .001.
Hierarchical regression models were then run to investigate whether CF was still associated with higher anxiety and depression scores when CS was controlled for in the analysis. A regression model explained approximately 46% of the variance in anxiety (Adj. R2 = 0.46, F (10.99) = 9.50, p <.001). CF was still significantly associated with higher anxiety severity, when CS was controlled for in the model (β = −0.24, p =. 004). Another regression model explained 32% of the variance in depression (Adj. R2 = 0.32, F (10.99) = 5.70, p < .001). CF was significantly associated with higher depression severity, when CS was controlled for in the model (β = −0.28, p = .003). A correlation analysis was conducted between CF and burnout, to rule of concerns over similar R2 values. There was a moderate positive correlation between these variables (r = 0.54), therefore because this correlation was not strong (r ≥ 0.07), this confirms they are independently measuring different constructs.
Study 1: Discussion
From the regression analyses it is evident that hypotheses 1, 2 and 3 can be accepted. The results show that CF and burnout are significantly associated with higher anxiety and depression levels in the police sample, supporting previous research in nurses (Hegney et al., 2014). Contrary to previous research (Grant et al., 2019), police officers experienced moderate levels of CF and CS. Furthermore, the current findings oppose previous findings that there is a significant negative correlation between CF and CS (Grant et al., 2019). The current findings build on the Risk Reflective Assessment Model (RRAM), as this could be applied to not only registered nurses but police officers as well. The RRAM shows ProQoL variables, anxiety and depression function in an integrative framework (Hegney et al., 2014). The current study extends this framework to police officers, demonstrating professional quality of life variables are significantly associated with self-reported anxiety and depression severity.
Study 2: Methodology
The aim of Study 2 was to provide a contextualised understanding of officers’ experiences through the intensive study of particular cases (Polit and Beck, 2010). The study explores officers’ awareness of ProQoL and the personal impacts of occupational stress (OS). Study 2 also aims to build on Study 1 by exploring officers’ perceptions of how ProQoL impacts their personal life.
Design and epistemology
Study 2 used a qualitative research design informed by a critical realist position that unobservable structures cause observable events (Archer et al., 2013). For example, quality of life is not directly observable, but it can cause observable events such as somatic disturbance.
Participants
Participants were recruited via expression of interest at the end of the survey in Study 1. Six participants (50% male) were selected from 36 expressions of interest, using stratified sampling and contacted via email to take part in the interview stage. Participants of various ranks and years of service ranging from 4 to 24 years were recruited.
Materials
Interview schedule
Each interview started with a question asking officers to describe their career in the police force to date. This question allowed for further demographics such as years of service, department and rank to come to light. Following this, respondents were asked the first set of interview questions which aimed to gauge officers' perceived awareness and experiences of CF, CS and burnout. For example, ‘Do you have an awareness of what Compassion Fatigue is? Could you describe it to me in your own words?’ followed by ‘Do you believe you have experienced this in the last month?’. Further interview questions were informed by previous literature relating to WHI (Dikkers et al., 2007; Geurts et al., 2003; Martinussen et al., 2007; Van Hooff et al., 2005). For example, ‘Do you think that your work as a police officer interferes with your home life? If so, could you give me an example?’
Procedure
Semi-structured interviews were conducted and audio-recorded via Skype. Interviews lasted approximately 20 minutes. Audio recordings were transcribed with participants’ permission using pseudonyms and removing other personally identifiable information. After participation, officers were emailed the debrief form and encouraged to ask any questions.
Data analysis
A thematic analysis was performed using NVivo 12 software. The process of analysis involved transcribing interviews, picking out codes and grouping common codes into themes. Themes were then labelled as sub-themes within three overarching themes, which gave a holistic picture of the overall topics revealed in the analysis.
Study 2: Results & Discussion
Here we present three themes: (1) Perceived awareness of the psychological impacts of CF, CS and burnout; (2) Personal impacts of OS; and (3) Positive coping strategies for OS.
This theme relates to police officers’ perceptions of CF, CS, and burnout. Although many participants were not familiar with the terms, they were able to explain the emotions underpinning them. All participants perceived to have experienced CF during their work as police officers. Officers described their experiences of CF as having a ‘loss of sensitivity’, feeling ‘numb’ and the psychological responses to critical incidents becoming ‘blasé’. All participants perceived that they had felt CS throughout their career. Participants described a ‘sense of purpose’, ‘pride’, ‘relief’ and having made a ‘positive difference’ for the victims. This further supports the theme that officers possessed a perceived awareness of the psychological impacts of the ProQoL variables. Longer serving, higher ranking police officers perceived to have experienced burnout at some point in their careers. Officers described burnout as having an ‘unmanageable workload’ that causes ‘stress and exhaustion to the point where you just physically can’t come to work’.
Participants demonstrated an underlying awareness of the impacts of the conditions (CF, CS, and burnout) despite some officers displaying ambiguity towards the terms themselves. When asked if officers had an awareness of compassion satisfaction, responses initially indicated ambiguity in most cases, followed by a perceived awareness of feelings associated with compassion satisfaction. For example, ‘I don’t really to be honest, but what I would guess is when you’ve made a positive difference’ and ‘it’s not a phrase I’ve heard before, but I could imagine it’s a reward’. Another officer did not express initial ambiguity; ‘CS for me would be like a feeling of a job well done… feeling like you’ve got a purpose and I’d done something well for a victim’. This officer possessed an awareness of the construct as well as its related effects.
Officers not only demonstrated a perceived awareness of the psychological effects caused by the ProQoL variables but also believed they had first-hand experiences of these conditions, which is inconsistent with Papazoglou et al. (2020) who claim that those who are unaware of CF are more at risk of its symptomology. The current research paper demonstrates that perceived awareness of CF’s symptomology does not necessarily lower the prevalence of experience for police officers. Although consistently with previous research, risk could be maximised through ignorance of symptoms (Papazoglou et al., 2020) or mental health stigma (Bell et al., 2021).
Senior officers discussed their fears that front-line officers are more at risk of CF due to the nature of their roles. All detective constables and response police officers on interview self-reported some distress in the last 30 days. Therefore, CF may be role-orientated, with front-line officers being at higher risk. When a chief inspector was asked if they had experienced CF in the last month they responded: ‘Me personally no, but I am really concerned that my staff perhaps do’. Furthermore, a sergeant discussed that to maintain a work-life balance it is important to ‘hold a line’ and ‘not be manipulated or pressured’ into taking on more work when you already have a high workload. They disclosed; ‘It is not so easy when you’re young and new in the job, you tend to just be compliant and do what you’re told. But that’s where we break people. That’s what we see time and time again.’
This theme was separated into three sub-themes regarding the different impacts both mental and physical outside of work:
Sub-Theme 2.1: Pre-occupation with Workload Causing Disruptions to Family/Social Life
Working out of hours to catch up on ‘relentless’ workloads trends throughout the analysis and it seems officers believe this is a barrier against OS when this could be contributing to it.
‘it is easier for me to do that hour at home at night because that helps me cope more easily. Do I wish I didn’t have to do it? Yes I do’.
Disruptions to family and social lives induces different negative emotions between participants, for example, one officer describes feeling ‘angry’, ‘resentful’ and ‘bitter’ because of their workload interfering with their home life. Although others depict feeling a sense of ‘guilt’ for prioritising their work over spending time with the family. This sub-theme is consistent with previous literature that quantitative workload predicts WHI (Peeters et al., 2004; Dikkers, 2008).
‘Guilt’s a big one. Not spending time with the family, because when you do your minds elsewhere, you’re thinking about jobs, thinking about catching up on tasks’.
Sub-Theme 2.2: Self-Deprecation
The analysis suggested that officers sometimes feel like failures because they are struggling with their unmanageable workload. A sergeant discussing their front-line officers, says ‘they feel like they’re a failure but it’s not, it’s an organisational failure because there is too much work and not enough people to do it’. Self-deprecation can induce feelings associated with depression, such as worthlessness (Ratsch, 2012); therefore, organisations should be made aware of this to avoid deterioration of police mental health.
Sub-Theme 2.3: Vicarious Trauma & Pre-occupation with work-related events
Some officers disclosed how exposure to certain situations in their personal lives can trigger vicarious trauma they have experienced in the line of duty. A sergeant discussed how they had ‘attended a lot of child deaths over the years’, which they say induced ‘anxiety’ when they had a child of their own. This ‘anxiety’ resulted in them being hypervigilant as they would ‘always be checking the baby monitor’. A detective discussed the personal impacts of attending sudden deaths at work. They disclose; ‘You can imagine what (death) looks like but until you’ve seen it and you’ve got that image like that’s the thing you go back to. It makes you feel a bit empty, no emotion there… but obviously I’d never say what my mental image is to people, because you know that could be traumatising for people to hear’.
These responses not only support the notion of WHI influencing the relationship between OS and wellbeing (Geurts et al., 2003) but emotionally the induction ‘anxiety’ and feeling ‘empty’ can be related directly to CF (Battle, 2011). Officers discuss the experience of PTSD like symptoms as they relive the trauma of others, on exposure to cues. Participants explain the circumstances to which triggers the psychological distress, which in the transcripts is commonly associated with death (Sugimoto and Oltjenbruns, 2001). Numerous officers did not believe their line of work had a physical impact on their personal lives; however, it is evident the impacts of OS induce struggles with mental wellbeing.
There was a pattern in terms of difficulty unwinding and trouble to ‘switch off’ after work. Both quantity and content of their workload induces sleep disturbance in several participants, thus impacting on officers’ quality of life. This sub-theme suggests that these officers are at risk of CF (Neylan et al., 2010). Contrary, officers with more years of service disclosed finding it easier to unwind because they have more experience in the job role. Another officer explains he does not find it difficult to unwind anymore, and he puts this down to impending retirement; ‘nothing really bothers me now because I don’t really care that much because I’m going, I can walk away’.
Sub-themes here were curated based on consistently reoccurring coping mechanisms that participants mentioned during interviews. Although officers discussed their personal struggles with OS, a pattern of positive coping mechanisms to combat OS were noticed across the transcripts.
Sub-Theme 3.1: Personal Support Networks
Communication with loved ones seems to help officers cope with OS, in particular when their loved ones can relate emotionally. This sub-theme is consistent with previous literature regarding coping mechanisms for OS among nurses (Drury et al., 2014). However, it is noteworthy that respondents discuss the use of personal support networks for example, ‘that kind of 10, 15-min period just talking over the dinner table and getting your wow’s and worries a day out is a bit of a coping mechanism for me’. However, at work feel unable to seek support due to a mental health stigma (Bell et al., 2021) and unconscious emotion invalidation.
Sub-Theme 3.2. Police Recognition
Recognition from the force and members of the public is critical for maintaining and increasing CS. Police officers state that they feel a lack of recognition or support from the force, such that ‘everyone’s out for themselves’ and they ‘just have to get on with it’. This demonstrates how job resources are not being utilised in this force, resulting in officers being more at risk of anxiety and depression (Van Hooff et al., 2005). However, when the public appreciate and celebrate officers demanding work, it acts as an external coping mechanism for combatting OS (Demerouti et al., 2001; Papazoglou et al., 2020). For example, one officer disclosed, ‘The thank you cards that we get from families and members of the public when you realise that you have made a positive difference to them in difficult circumstances, that’s hugely satisfying’. Similarly, another officer said, ‘sometimes there can be a negative perception of the police but actually knowing that we can get things right…’. In this case, personal impacts of OS such as self-deprecation could be alleviated by recognition for their commitment and hard work.
Overall discussion
Study 1 results infer that ProQoL is significantly associated with anxiety and depression in UK police officers. The Risk Reflective Assessment Model (RRAM; Hegney et al., 2014) may be applicable to police officers in that anxiety and depression interact with ProQoL. Further support comes from Study 2, as the psychological impacts of police work are consistent with symptoms of burnout and CF, further indicating the integrative framework. The present research reveals a need for treating CF directly, as well as increasing CS in the police. Previous research has focussed on how CS can be increased in the workplace (Harr, 2013). While this research confirms the importance of enhancing CS (Andersen et al., 2015; Grant et al., 2019), it does not alleviate symptoms of CF. The current study demonstrates CF was still significantly associated with anxiety and depression levels when CS was controlled for in the analysis. It is possible that CF and CS are not mutually exclusive, but co-occurring. Therefore, interventions ignoring the root causes of CF and focussing on increasing CS are not sufficient to alleviate common mental health complaints. Interventions delivered to police officers should not solely focus on enhancing CS, but mitigating CF.
Study 2 complements Study 1 by gaining reflections first-hand, from officers regarding how OS impacts their personal lives, which align with symptoms of CF and burnout. Impacts of OS and WHI were primarily caused through both the quantity (e.g. the frequent disclosure that ‘there is too much work to do, and not enough officers to do it’.) and content (Officers disclose reliving the trauma of others on exposure in their personal lives on exposure to cues) of officers workload. Death was a common cue, by which officers described feeling emotionally detached or having anxiety out of work due to these traumatic experiences. However, positive coping mechanisms such as support networks and recognition were identified, which are suggested to be effective for combatting CF (Pfifferling and Gilley, 2000). Although these mechanisms assisted in coping, levels of CF, burnout, anxiety and depression still exist in the sample substantially with evidence of moderate levels. The majority of officer’s self-reported moderate levels of CS, however, there is a need for improvement. CF and CS levels in this sample are both higher than the levels observed in Grant et al. (2019) sample. With a large proportion of respondents experiencing CS in this sample of police officers, likewise to previous research with a sample of child protection workers (Conrad and Kellar-Guenther, 2006); it is not feasible to ignore bold indications of such variables (CF and CS) co-existing. Thus, organisations need to focus on directed treatment to alleviate negative workload reactions.
Strengths & limitations
This multi-study paper’s most profound strength is the mixed methods approach. Combining quantitative and qualitative methods can promote more scientifically sound and transferable findings, through synergistically merging qualitative stakeholder engagement with quantitative outcomes to inform intervention, planning, implementation, evaluation, and monitoring (Ivankova and Wingo, 2018). The study was conducted during the early COVID-19 pandemic, which could have influenced the mental health symptoms reported by officers. However, this was accounted for in quantitative analyses, with results indicating that the pattern of findings would be obtained regardless of COVID-19 impacts.
Study 2 provides insightful personal accounts of officers' awareness of CF, CS, and burnout, and experiences of OS to complement the quantitative findings of Study 1. However, the cross-sectional nature of Study 1 limits inferences about causality. Accordingly, future research should adopt longitudinal designs to determine long-term impacts of CF, CS, and burnout on police officer wellbeing.
Theoretical implications
A potential future endeavour for researchers is the idea that CF and burnout could be role-orientated. Senior officers discussed how they are concerned for their front-line police officers, as they believe they are at higher risk of developing CF due to being exposed to emotionally fuelled situations daily. Within officer interviews, it was clear there seems to be a ‘grin and bear it’ culture within the police, that ‘everybody is in the same boat’ and this invalidates officers' emotions, as they seem to believe it is expected of them to deal with secondary traumatic stress themselves (Bell et al., 2021). Research suggests police officers are more resilient than the average civilian (Andersen et al., 2015), and evidence ‘hardiness’ to modify the effect of occupational stressors (Allison et al., 2019). Therefore, academics could focus future research on whether resilience in police officers impacts upon ProQoL interactions with anxiety and depression.
Implications for practice
ProQoL variables can be used as a focal point in intervention to combat anxiety and depression in police officers (Figley, 2002; Kiley et al., 2018). This research will assist organisational decision-making regarding focussing interventions on treating CF as opposed to merely increasing CS in police officers. It is evident organisations are making efforts to improve officers’ wellbeing through programmes such as the ‘Blue Light Wellbeing Framework’, which has elements of increasing CS (Phythian et al., 2022). The present study suggests boosting CS by attempting to improve resilience and educating officers on CF alone is not sufficient to alleviate its symptoms. Although wellbeing initiatives have developed, officers are still suffering from mental ill-health. Organisations could focus more heavily on CF antecedents to tackle mental health complaints such as anxiety and depression. It could be that there is a need for more widespread implementation of frameworks to be accessible to a wider population of officers. From the current analysis, we suggest a more person-centred approach could be better in practice due to the varied nature of individuals’ experiences. Ideally, providing in-house counselling opportunities to all front-line officers would benefit their wellbeing.
Conclusions
This mixed method study demonstrates that CF, CS, and burnout are significantly associated with self-reported anxiety and depression in police officers. Impacts of CF, CS, and burnout are consistent with the literature; however, Study 1 shows the positive effects of CS do not override the negative effects of CF, unlike previous research. Symptoms of CF (emotional numbness) and burnout (overwhelming workload) keep the cycle of OS going. The current study suggests police officers possess a perceived awareness of the psychological impacts of CF, CS, and burnout and can describe the emotions attached to these states. Considering self-reported rates of CF in both study 1 and 2, this evidences that even with an understanding of underground emotions police officers are still experiencing CF. The findings from this multi-study paper should be used when considering treatment, assessment, and identification of CF and burnout in police officers, as well as tackling common mental health complaints.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Research ethics
This research gained ethical approval from The Manchester Metropolitan University Ethics committee.