
Abstract
The present study compared the influence of Adverse Childhood Experiences (ACEs) and Cognitive Emotion Regulation Strategies (CERS), on wellbeing and professional quality of life variables, including Burnout, Compassion Fatigue (CF) and Compassion Satisfaction (CS) in Police Officers (POs) versus a community sample. POs reported lower wellbeing, higher burnout and more ACEs. Maladaptive CERS were associated with low wellbeing, CS, elevated burnout and CF in both samples, while adaptive CERS were associated with enhanced wellbeing and better professional quality of life only in POs. Findings indicate the need to tailor prevention and intervention efforts, considering these vulnerabilities and protective factors.
Keywords
Introduction
Despite being a vital activity that allows people to meet their basic psychological needs, working can occasionally become extremely stressful, leading to poor wellbeing, low job satisfaction and poor professional quality of life (Oliver et al., 2023). According to the Centre for Disease Control and Prevention (CDC, 2025), mental wellbeing is a multidimensional construct, including positive functioning, experiencing positive feelings, life satisfaction, and fulfillment in physical, social, psychological, emotional, and economic domains. Emerging evidence suggests that in highly stressful working environments, mental wellbeing and professional quality of life tend to be impacted concurrently (Rikos et al., 2024). Professional quality of life refers to the overall feeling of fulfillment and content individuals experience as a result of their work and can be affected both by the negative (burnout and compassion fatigue) and positive aspects (compassion satisfaction) of one’s occupation, which can arise in service-oriented roles (Stamm, 2010).
Burnout is acknowledged as a major workplace psychological risk and professional hazard, appearing as a potential negative outcome of prolonged or chronic stress at work, where the person is left feeling ineffective and cynical to work (Maslach et al., 1997; Maslach and Leiter, 2016). Another term closely related to burnout, compassion fatigue, was first introduced by Joinson (1992), and was then further developed by Figley (1995) as the ‘cost of caring’ or secondary traumatic stress, arising from frequent exposure to potentially distressing or traumatic life events or material, documented most often in professions that involve protecting, serving or helping others. Compassion fatigue can be described as a state of chronic physical and mental exhaustion caused by an inability to cope with stressors in the workplace, and more broadly in one’s everyday life (Brady, 2017; Cocker and Joss, 2016). Compassion satisfaction, on the other hand, refers to the degree of pleasure and fulfillment derived from helping and serving those in need (Stamm, 2010), and can be considered a source of inner strength that can mitigate against the possible adverse effects from exposure to potentially distressing or traumatic events or material (Brady, 2017; Grant et al., 2019).
Certain professions which expose individuals to chronic stressors (psychological, emotional, physical) make them particularly vulnerable, as these stressors can influence their wellbeing and professional quality of life, affecting people on a personal and professional level. Understanding the variables that can impact mental wellbeing and professional quality of life is crucial in developing targeted preventions and intervention programs that aim to support professionals with their work and aim to improve their wellbeing overall.
Wellbeing, mental health and professional quality of life in police officers
Police officers represent a professional group that is particularly susceptible to chronic stress due to the demanding nature of their job (Violanti et al., 2017). Depending on the specific role and duties they assume, most police officers undertake shift work (e.g., long shifts, night shifts, on-call working) that is known to interfere with one’s daily routine, family life, and life outside of work, and are often exposed to potentially distressing or traumatic events or material that threaten their mental and physical health (Magnavita et al., 2018; Violanti et al., 2017). Certain police roles and duties can also involve split-second decisions to be made within high-risk situations with elevated stakes, requiring them to be hypervigilant in order to protect themselves and others, likely with their threat system activated, thereby contributing to mental health strain and burnout (Alves et al., 2023). Furthermore, many police officers respond to and support vulnerable individuals with complex needs who require compassion and sensitivity (Livingston, 2016). These factors put them at high risk for developing mental health difficulties, including depression, anxiety, Post Traumatic Stress Disorder (PTSD), suicidal ideation, insomnia and poor wellbeing (Violanti et al., 2017; 2021).
Police officers’ professional quality of life can also be impacted as indicated by elevated levels of burnout (Davies et al., 2023; Syed et al., 2020) and compassion fatigue (Brady, 2017) that can arise from exposure to potentially distressing or traumatic events or material, even vicariously through supporting people they serve. These negative symptoms become exacerbated when officers have low organizational support and feel overwhelmed (Brady, 2017). It is argued that one’s capacity for compassion and empathy is affected when working in highly stressful situations for a prolonged period, resulting in reduced motivation to relate to other people’s distress, and has been associated with poorer levels of performance (Grant et al., 2019). Officers described their experiences of compassion fatigue as ‘losing sensitivity’, feeling ‘numb’, and developing a ‘blasé’ attitude to responding to critical incidents (Davies et al., 2023). In fact, police officers’ compassion fatigue has been associated with elevated levels of depression, anxiety, and burnout (Brady, 2017; Cocker and Joss, 2016; Davies et al., 2023; Grant et al., 2019). On the other hand, compassion satisfaction is significantly and negatively associated with burnout and compassion fatigue in police officers (Grant et al., 2019) and therefore has the potential to act as a buffer against them developing mental health symptoms, especially if they feel that their work has social value or impact.
Given the stigma around mental health difficulties, showing signs of mental distress remains a taboo, especially within policing. Police officers continue to report that there is still a fear around being perceived as ‘weak’ when disclosing that something has affected them (e.g., Porter and Lee, 2024; Strickland et al., 2023), and that they are expected to be ‘tough’, emotionally controlled and resilient, and able to deal with adversities as part of their job (Janssens et al., 2021). This has been found to act as a barrier to police officers opening up about their mental health and wellbeing, including challenges at work, and seeking help (Cohen et al., 2019; Phythian et al., 2022; Tsirimokou et al., 2024). As a result, many police officers might try to persevere on their own, which can further exacerbate any symptoms they experience (Porter and Lee, 2024; Violanti et al., 2017). Identifying the unique underlying challenges of policing that are associated with poor wellbeing and low professional quality of life can help inform strategies to better support them.
Adverse childhood experiences, wellbeing and professional quality of life
Adverse Childhood Experiences (ACEs) are potentially traumatic incidents that take place during childhood until the age of 18 years (CDC, 2024) and play a critical role in determining an individual’s wellbeing and mental health (Mercer et al., 2023; Yellowlees et al., 2021). Such experiences include multiple types of abuse and neglect, such as witnessing domestic violence as a child or adolescent, as well as community and/or collective violence (CDC, 2024). According to a recent systematic literature review, 60% of adults globally report being exposed to at least one ACE (Madigan et al., 2023). Individuals who experience a higher number of ACEs are at significantly higher risk of (i) being the victim or perpetrator of violence, (ii) presenting a reduced capacity to deal with stress (and engage in maladaptive avoidant coping, including abusing alcohol/drugs), (iii) report a higher likelihood of attempting suicide, as well as poorer levels of mental health and wellbeing overall, and (iv) report higher levels of burnout and are also more prone to experiencing work-related issues, absenteeism, unemployment, and financial problems in adulthood (Bunting et al., 2018; Hughes et al., 2016; Poole et al., 2018; Tzouvara et al., 2023; Yellowlees et al., 2021). Previous research has highlighted an association between ACEs and burnout in high-demand professions, including health (e.g., doctors, nurses), social care workers and even athletes (Hedrick et al., 2023; Mercer et al., 2023; Trockel et al., 2023; Yellowlees et al., 2021), suggesting that early adversities may increase vulnerability to stress and may have a long-standing impact on individuals both personally and professionally. Furthermore, there is limited research linking ACEs to compassion fatigue or compassion satisfaction and these were conducted with mental health professionals and residential care workers (e.g., Brown et al., 2022; Milne et al., 2024).
Due to the nature of policing, officers on duty might be exposed to adversities at an increased rate, with some of these resembling experiences they had as children. For example, research suggests that ACEs in police officers were positively associated with mental health issues, including PTSD and depression (Violanti et al., 2021). It is also noteworthy to mention that a dysfunctional family environment, and individual traits developed through adversity, as well as experiential motivations, were associated with choosing a career that entails helping or serving others (Bryce et al., 2023). People who adopt caretaking roles early, enter the helping profession in adulthood as an extension of their childhood roles or as a desire to remedy harm that was caused to them as children (Bryce et al., 2023). Furthermore, emergency personnel are at higher risk of being triggered, or re-traumatized, in addition to their increased vulnerability to experiencing vicarious traumatization (Kessler et al., 2017; Rees and Smith, 2008). According to the diathesis-stress model (Zuckerman, 1999), underlying predispositions to trauma are activated by stressful situations. This would suggest that police officers who experienced ACEs in childhood may be at an increased risk of developing mental health difficulties. Considering the detrimental effects of ACEs to the human body’s stress-response system, and the number of stressors police officers can be exposed to, it is important to further investigate the relationship between ACEs, wellbeing and professional quality of life in police officers, and also compare them with other professionals to examine if they are at higher risk.
The role of cognitive emotion regulation strategies in wellbeing and professional quality of life
Cognitive emotion regulation strategies (CERS) refer to the processes by which individuals attend to and regulate their emotions in response to different events or experiences (Thompson, 1991). These strategies involve how people think about, interpret or make sense of emotional situations, which can help them manage their feelings in adaptive and maladaptive ways (Garnefski and Kraaij’s, 2007). Rumination (repetitive thinking of negative thoughts and feelings), self- and other-blame, and catastrophizing (focusing on irrational thoughts that overestimate the likelihood of negative outcomes), are the four maladaptive CERS proposed in the emotion-regulation model (Garnefski and Kraaij’s, 2007) and have been associated with mental health issues and poor wellbeing (Conway et al., 2024; Kraiss et al., 2020; Kyranides et al., 2024). In contrast, positive refocusing (directing attention to the positive things in a challenging situation), refocusing on planning (considering ways to deal with the unpleasant situation), putting into perspective (minimizing the event’s significance), positive reappraisal (identifying the positive aspects of the unpleasant incident), and acceptance (resigning to what has occurred by simply experiencing any emotions that emerge), represent the five adaptive CERS which have been associated with enhanced wellbeing and decreased mental health issues (Conway et al., 2024; Garnefski and Kraaij’s, 2007; Kraiss et al., 2020).
The ability to effectively regulate one’s negative emotions is essential for maintaining wellbeing, especially in police officers who frequently encounter events and situations that generate strong negative emotions (Conway et al., 2024). However, police officers often find it difficult to recognize and acknowledge that they may be struggling (Arble et al., 2018; Strickland et al., 2023; Tsirimokou et al., 2024), which may be associated to poor emotional regulation. Research among police officers suggests that the use of maladaptive coping strategies, such as avoidance, rumination and catastrophizing, are negatively associated with wellbeing and predicts worse mental health outcomes (Arble et al., 2018; Conway et al., 2024). On the other hand, adaptive strategies like positive reappraisal and refocusing on solving problems (planning) are associated with better mental health outcomes, including higher levels of wellbeing and lower burnout (Alves et al., 2023; Conway et al., 2024). Nevertheless, there is a lack of research exploring the role of CERS and professional quality of life outcomes (compassion satisfaction, compassion fatigue) among police officers. Although this gap remains unexplored in police officers, evidence among other emotionally demanding professions, such as healthcare providers, suggests that maladaptive coping strategies predict higher levels of burnout and compassion fatigue (Bamonti et al., 2022), whereas adaptive strategies, such as cognitive reappraisal, predict higher levels of compassion satisfaction and lower levels of burnout (Măirean, 2016). Considering, therefore, the nature of policing, where officers frequently encounter situations and incidents that generate strong negative emotions, in addition to ongoing demands and substantial responsibilities, it is important to understand how they manage and regulate these emotional challenges, and the extent to which different regulation strategies affect police officer’s wellbeing and professional quality of life.
One pathway that has been examined to link early adversity with mental health difficulties in adulthood is through emotion dysregulation or the inability to identify and regulate one’s own emotions. More specifically, a longitudinal study found that emotion regulation meditated the relationship between ACEs and psychological and physical outcomes using a community sample (Cloitre et al., 2019). ACEs affect typical development which contributes to more frequent use of maladaptive instead of adaptive coping strategies, which can then impact individuals on a personal and professional level. For example, ACEs can influence the types of coping strategies people utilise, leading to even greater vulnerability for depression and anxiety (Huh et al., 2017). Nevertheless, the association between ACEs, adaptive and maladaptive strategies, wellbeing and professional quality of life in police officers, remains unexplored to date and it is important to examine if these vulnerabilities are unique to police officers or extend to other professional groups.
Current study
The main aim of this study was to investigate how early ACEs and current coping strategies can impact wellbeing and professional quality of life (including burnout, compassion fatigue and compassion satisfaction) in police officers, and examine if these factors are unique to them or extend to other occupational groups. Given the pronounce role of emotion dysregulation on maladjustment for individuals with ACEs, the present study additionally examined if adaptive and maladaptive CERS served as mediators to wellbeing and the different professional quality of life variables. To our knowledge, this is the first study to examine the relationship between these variables in detail in police officers and compare them to other professionals recruited from the community. It is important to compare police officers to other occupational groups to examine if these variables constitute unique risk factors for police officers or apply to other professionals also. For example, ACEs have been documented in police officers (Violanti et al., 2021), and it would be important to examine if they report more ACEs compared to other professionals, and if this puts them at risk for displaying poor wellbeing and affects them professionally (reporting higher burnout and compassion fatigue rates). Furthermore, it would be useful to examine if police officers have effective (or ineffective) regulation strategies compared to other professional groups, that help (or impede) them in the workplace. Compassion fatigue and compassion satisfaction have been documented in healthcare, education and community service professionals (Cocker and Joss, 2016; Pérez-Chacón et al., 2021) but we also need to examine them in relation to other professionals as most occupations entail working or providing a service to people. While not all professionals care for their patients/clients in a traditional sense (nursing/treating them), they do provide a service, and care for their needs and affairs (lawyers, accountants, architects).
In line with the existing literature, it is hypothesised that police officers compared to other professionals recruited from the community, will report elevated levels of burnout and compassion fatigue, lower wellbeing and compassion satisfaction, higher rate of ACEs, more frequent use of maladaptive CERS and less frequent use of adaptive CERS. It was further hypothesized that ACEs will impact wellbeing and professional quality of life variables (burnout, compassion fatigue and compassion satisfaction) through the more frequent use of maladaptive CERS and that this mediation effect will be more prominent in police officers, compared to other professionals.
Methods
Participants
A total of 135 participants took part in the study. Two participants’ entries were removed from the dataset due to a large amount of missing data and 8 participants did not report specifically what they practiced (occupation). This resulted in a final sample of 125 participants who were included in the analysis. The sample included police officers (n = 55; Mage = 40 years; SD = 9.03; 29 males) and a control community sample (n = 70; Mage = 31 years; SD = 14.03; 25 males). When asked to report their occupation some police officers reported more vague responses such as “police officer”, “police constable” or “working in law enforcement” (n = 34) while others provided more details either about their rank (9 detectives, 1 detective superintendent) or their duties. More specifically some reported they were working as cybercrime examiners (n = 2), digital forensic support officers (n = 3) or forensic computer analysts (n = 4), specializing in child abuse and exploitation (n = 2) or as crime scene investigators (n = 4). Regarding the community sample, the following professions were reported: sports related professions (n = 4), accountants (n = 2), architect (n = 1), solicitor (n = 1), managers/directors (n = 7), consultants (n = 3), corporate employees/in finance (n = 3), human resources (n = 1), marketing (n = 4), communication coordinator (n = 1), IT (n = 4), caregiver (n = 1), nurse (n = 1), dentist (n = 1), doctors (n = 4), physiotherapist (n = 1), mental health professionals (n = 6), in education (n = 6), research (n = 1), freelance editor (n = 1), film maker (n = 1), in retail (n = 4), barista/waitressing (n = 7), intern (n = 1), receptionist (n = 1), self-employed (n = 3). Police offices were all residing in the United Kingdom while 24.30% of the community sample were resisting outside the United Kingdom at the time of completing the study. Data collection took place between September 2023 and June 2024.
Procedure
The study was granted ethical approval by the Department of Clinical and Health Psychology's research ethics committee at the University of Edinburgh. The members of the research team shared the link to the online survey via email to their professional networks and research collaborators, including contacts at UK police forces. Although this technique is susceptible to various forms of bias, such as selection bias (Parker et al., 2019), it is particularly useful for accessing populations with specific characteristics through connected personal networks outside of institutional contexts (Dragan and Isaic-Maniu, 2013). The study was further advertised to recruit individuals from other professions by sharing a link to the online survey via various social media platforms, including Instagram, Facebook, and WhatsApp. Participation in the study was voluntary. A secure online platform (Online Surveys) was used for setting up and distributing the survey. Participants were provided with a link to the online survey. After reading the information sheet, they were asked to confirm that they were 18 years or over, fluent in English, and provided consent. Participants were then presented with a series of demographic questions, including age, sex assigned at birth, status of employment, their occupation or last occupation and current country of residence. The online survey took approximately 25–35 min to complete. At the end of the online survey, participants were provided with a debriefing sheet and were thanked for their participation.
Measures
The Warwick-Edinburgh Mental Well-Being Scale (WEMWBS; Tennant et al., 2007)
The WEMWBS scale was used to assess well-being which includes 14 items, positively phrased. Each item (e.g., “I’ve been feeling optimistic about the future”) was rated using a scale from 1 (none of the time) to 5 (all of the time). The total score was computed by adding the score of all the items, with scoring ranging from 14 to 70. Higher scores indicate higher levels of well-being, while lower scores (more specifically less than 40) have been reported to indicate high risk for depression (Taggart et al., 2016). The WEMWBS has good content validity, internal consistency (Cronbach alpha ranging from .89 to .91) and test-retest reliability (.83) (Taggart et al., 2016; Tennant et al., 2007). In the current sample the WEMWBS was found to have high internal reliability as the Cronbach’s alpha was .94.
Professional Quality of Life Scale: Compassion Satisfaction and Fatigue (ProQOL-CSF-R-IV; Stamm, 2010)
The ProQOL-CSF-R-IV scale has 30 items and was used to assess three distinct but related sub-scales: Burnout (α = .70; “Because of my work, I feel exhausted”), Compassion Satisfaction (α = .86; “I get satisfaction from being able to help people”), and Compassion Fatigue or Secondary Traumatic Stress (α = .85; “I feel as though I am experiencing the trauma of someone I have helped”). Each construct has 10 items which are rated on a 6-point Likert-type scale ranging from 0 (never) to 5 (very often). Each item explores how often during the previous month the participant experienced a series of emotional states. Higher scores in each of the dimensions indicate higher levels of burnout, compassion fatigue and compassion satisfaction. This scale has been utilized in previous studies assessing police officers (Grant et al., 2019; Miller et al., 2017; Papazoglou et al., 2019) and has demonstrated satisfactory internal consistency and discriminant validity (Brady, 2017; Keesler and Fukui, 2020; Stamm, 2010).
Adverse Childhood Experiences International Questionnaire (ACE-IQ; WHO, 2020)
The ACE-IQ is a 31-item self-report scale designed by the World Health Organization (WHO) to assess exposure to three domains of adverse experiences which include 13 sub-dimensions of ACEs based on the work of Felitti et al. (1998). The first domain is childhood maltreatment and includes five sub-dimensions: the experience of emotional (e.g., “Did a parent, guardian or other household member yell, scream or swear at you, insult or humiliate you?”), physical (e.g., “Did a parent, guardian or other household member spank, kick, punch or beat you up?”) or sexual abuse (e.g., “Did someone touch you or fondle you in a sexual way when you did not want them to?”) and emotional (e.g., “Did parents/guardians understand your problems and worries?”) or physical (e.g., “Did parents/guardians not give you enough food even when they could easily have done so?”) neglect. The second domain is family dysfunction also consisting of five sub-dimensions: participants were asked if they grew up in a household in which a member was abusing alcohol/drugs, had chronic mental issues, had been incarcerated, or was violently treated (e.g., “Did you see or hear a parent or household member in your home being slapped, kicked, punched or beaten up?”), or if they had experienced parental separation due to divorce or parental loss. The third domain assessed violence outside the home and includes three sub-dimensions, bullying, witnessing community (e.g., “Did you see or hear someone being beaten up in real life?”) or collective/war violence (e.g., “Were you beaten up by soldiers, police, militia or gangs?”). Exposure to a category of ACEs requires a positive response to at least one of the items in the sub-dimension. A total number of ACE categories to which the participant had been “exposed” was summed to create a total score ranging from 0 to 13. The ACE-IQ is a reliable and valid measure of adverse experiences (Christoforou and Ferreira, 2020). In the current sample the Cronbach’s alpha was .74.
Cognitive Emotion Regulation Questionnaire (CERQ; Garnefski et al., 2002)
The CERQ is a 36-item self-report questionnaire which examines specific cognitive coping strategies individuals apply after experiencing negative or stressful situations (Garnefski and Kraaij, 2007). The scale has nine theoretically discrete subdimensions (with four items each), which can be grouped into adaptive and maladaptive Cognitive Emotion Regulation Strategies (CERS). There are four maladaptive CERS including: blaming self (α = .91, e.g. “I feel that I am the one who is responsible for what happened”), blaming others (α = .92, e.g. “I feel that others are responsible for what has happened”), catastrophizing (α = .81, e.g. “I continually think how horrible the situation has been”) and rumination (α = .87, e.g., “I dwell upon the feelings the situation has evoked in me”). There are also five adaptive CERS: positive refocusing (α = .93, e.g., “I think of something nice instead of what has happened”), positive reappraisal (α = .89 e.g., “I think I can learn something from the situation), putting into perspective (α = .88, e.g., “I think that other people go through much worse experiences”), refocus on planning (α = .86, e.g., “I think about a plan of what I can do best”), and acceptance (α = .86, e.g., “I think that I have to accept that this has happened”). Participants were asked to rate each statement in terms of how they feel or act in response to stressful or threating life events on a Likert scale ranging from 1 (almost never) to 5 (almost always). The CERQ scale has shown to have good validity and high reliability in different languages and cultures (Garnefski et al., 2002; Garnefski and Kraaij, 2007; Kyranides et al., 2024).
Statistical analysis
To examine if there were significant differences across the variables under study, the sample was divided into (i) police officers (participants who reported working for a police force) and (ii) the control, community sample. Independent samples t-tests were run to examine differences between the two groups. To assess which variables had a stronger relationship with wellbeing, burnout, compassion fatigue and compassion satisfaction correlation analyses were run to examine their associations with ACEs, and CERS. Additionally, hierarchical linear regressions were performed with wellbeing and the variables assessing professional quality of life (burnout, compassion fatigue and compassion satisfaction) as the outcome variables. Furthermore, mediation analyses were conducted examining the mediating effect of CERS, on the relationship between ACEs on wellbeing, burnout, compassion fatigue and compassion satisfaction.
Results
Means, standard deviations (SD), for the study variables presented separately for police officers and the community sample.
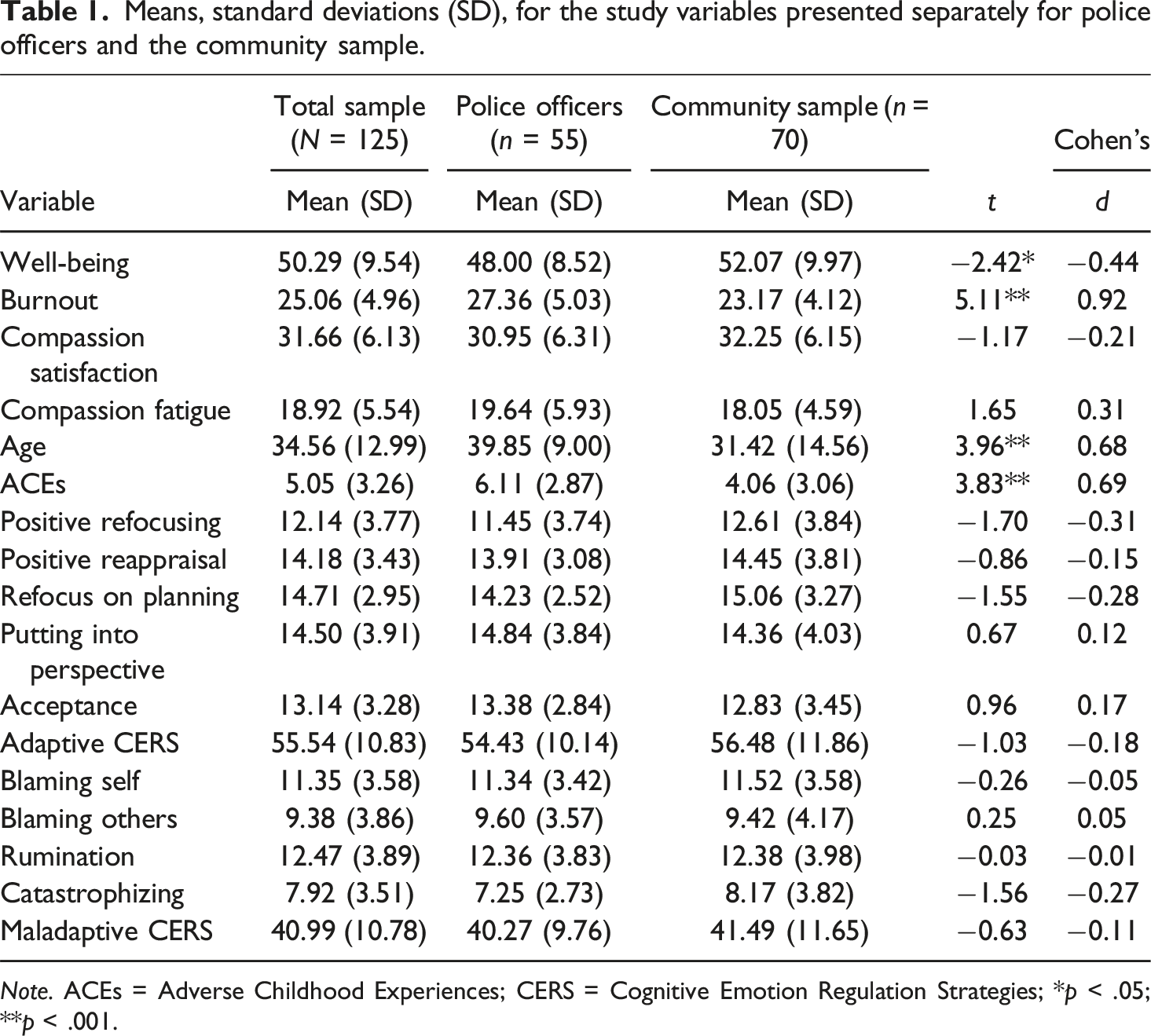
Note. ACEs = Adverse Childhood Experiences; CERS = Cognitive Emotion Regulation Strategies; *p < .05; **p < .001.
Correlations for the main study variables for police officers (n = 55 below the diagonal) and the community sample (n = 70 above the diagonal).
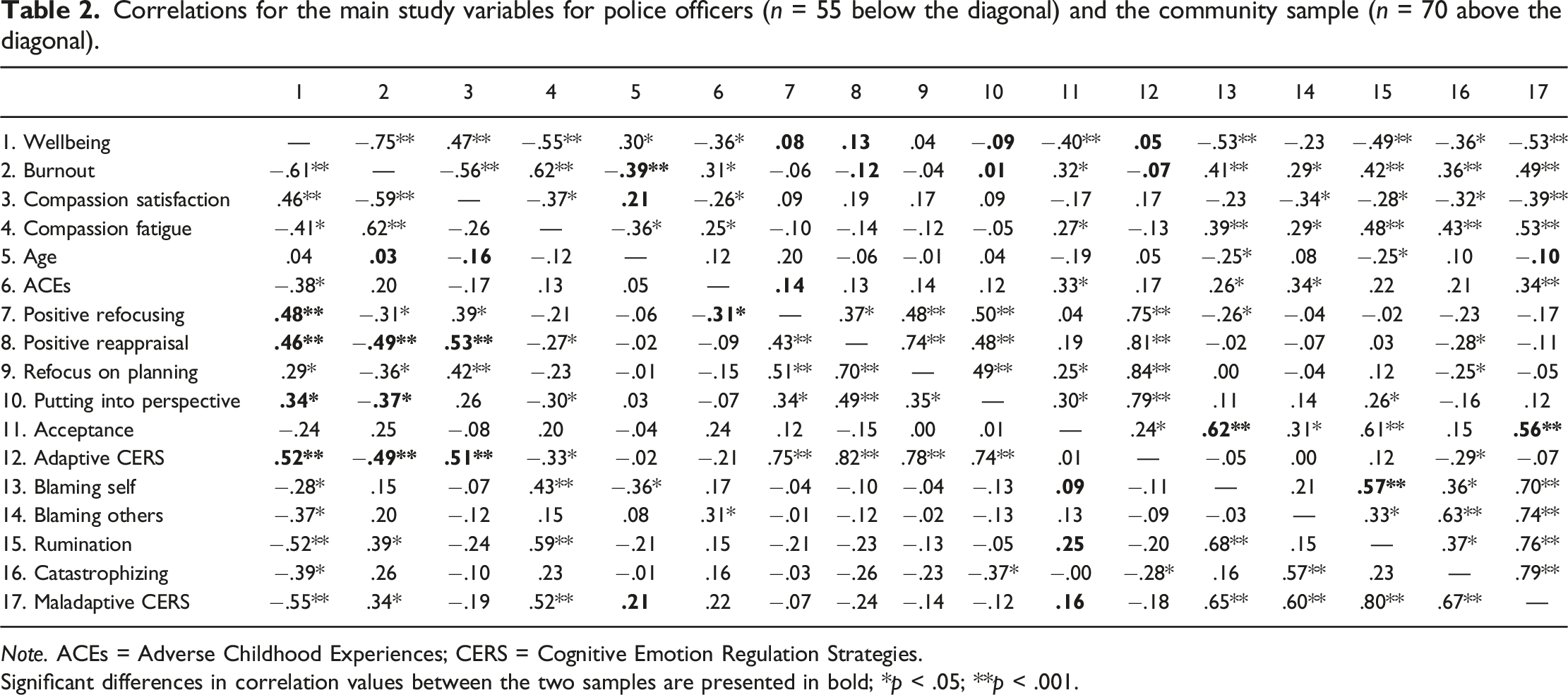
Note. ACEs = Adverse Childhood Experiences; CERS = Cognitive Emotion Regulation Strategies.
Significant differences in correlation values between the two samples are presented in bold; *p < .05; **p < .001.
In both samples, burnout was significantly positively correlated with compassion fatigue (r = .62 for POs; r = .62 for the CS), maladaptive CERS (r = .34 for POs; r = .49 for the CS) more specifically rumination (r = .39 for POs; r = .42 for the CS), and negatively correlated with compassion satisfaction (r = −.59 for POs; r = −.56 for the CS). Burnout in the police officers was negatively correlated with the adaptive CERS (r = −.49 for POs; r = −.07 for the CS), more specifically positive reappraisal (r = −.49 for POs; r = −.12 for the CS), and putting into perspective (r = −.37 for POs; r = .01 for the CS) and these correlation values were significantly different to those obtained from the community sample. In both samples, compassion fatigue was positively correlated with maladaptive CERS (r = .52 for POs; r = .53 for the CS) more specifically self-blaming (r = .43 for POs; r = .39 for the CS) and rumination (r = .59 for POs; r = .48 for the CS). With regards to compassion satisfaction a stronger positive correlation was identified for adaptive CERS in police officers compared to the community sample (r = .51 for POs; r = .17 for the CS) more specifically positive reappraisal (r = .53 for POs; r = .19 for the CS) and these differences were significantly different in the two samples.
Hierarchical linear regression analyses were conducted to explore the impact of the different variables on wellbeing, burnout, compassion satisfaction and compassion fatigue, which were performed separately for the police officers and the community sample. Demographic variables (age, biological sex) were entered in step 1, ACEs were entered in step 2, while adaptive and maladaptive CERS were entered in step 3. As the sample of police offices was smaller, the adaptive and maladaptive strategies were grouped together. Acceptance was not included in the adaptive CERS score, as it showed a negative correlation with wellbeing, and a positive correlation with burnout and compassion fatigue in the community sample. The same process was employed for both samples and was run separately for wellbeing, burnout, compassion satisfaction and compassion fatigue.
Regressions
Hierarchical regression analysis for variables predicting wellbeing and professional quality of life in the police officers (n = 55).
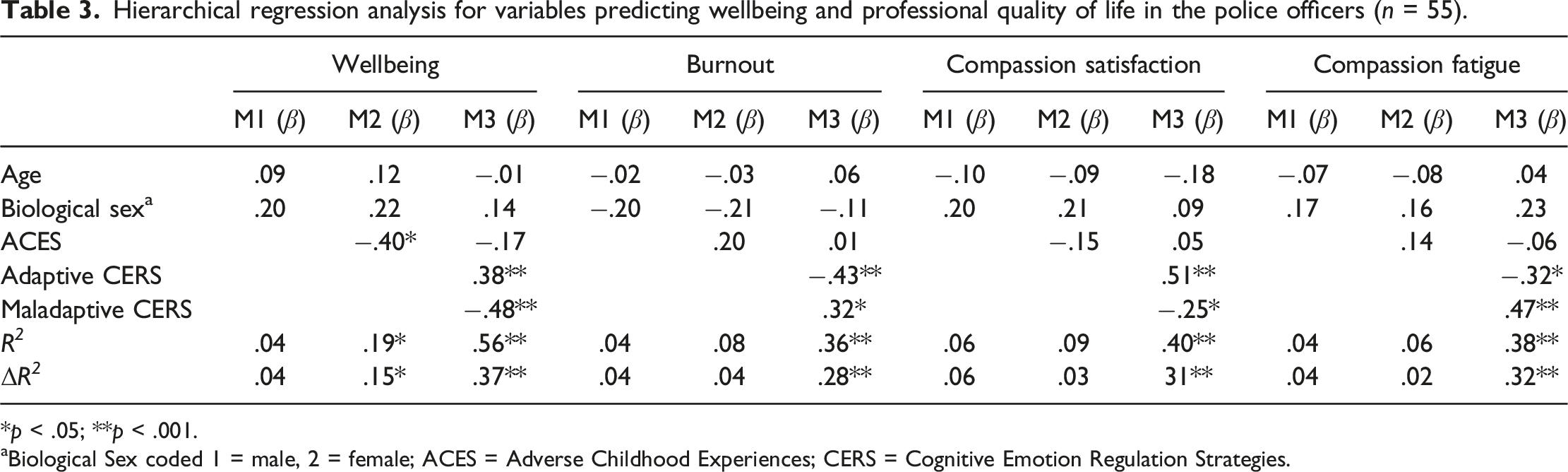
*p < .05; **p < .001.
aBiological Sex coded 1 = male, 2 = female; ACES = Adverse Childhood Experiences; CERS = Cognitive Emotion Regulation Strategies.
Hierarchical regression analysis for variables predicting wellbeing and professional quality of life in the community sample (n = 70).
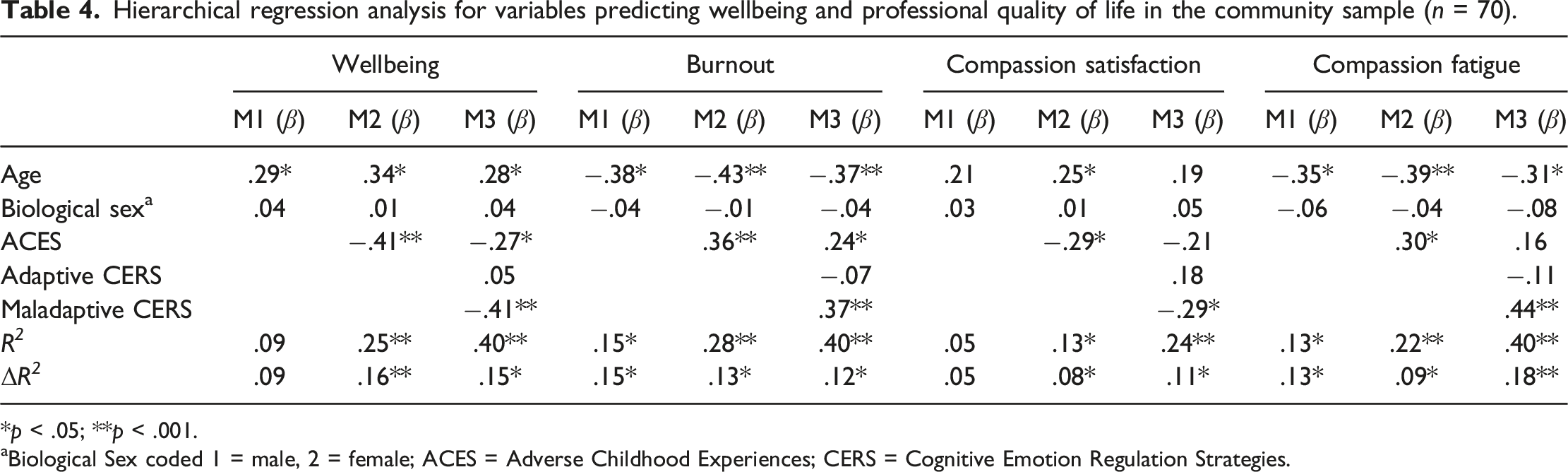
*p < .05; **p < .001.
aBiological Sex coded 1 = male, 2 = female; ACES = Adverse Childhood Experiences; CERS = Cognitive Emotion Regulation Strategies.
Mediation
A series of parallel mediation analyses were conducted to examine if the different adaptive (positive refocusing, positive reappraisal, refocus on planning and putting into perspective) followed by maladaptive (self and other blame, rumination, catastrophizing) CERS, mediate the relationship between ACEs (X), wellbeing and professional quality of life variables (burnout, compassion fatigue and compassion satisfaction; Ys) in police officers while controlling for age and biological sex. Unstandardized coefficients are reported in the text and standartised coefficients are reported in the figures. In the first model examining the total effect of ACEs (X) and Wellbeing (Y) for police officers, using the adaptive CERS as mediators was significant, F(3,50) = 4.10; R
2
= .19; p < .05 (b = −1.19, t = −3.14, p < .01). ACEs significantly predicted less positive refocusing (b = −.44, t = −2.78, p < .01) and in turn positive reappraisal (b = 1.13, t = 2.33, p < .01) predicted enhanced wellbeing in police officers (see Figure 1(a)). No significant indirect effect of ACEs on wellbeing through any of the mediators was found for police officers. The direct effect of ACEs on wellbeing in the presence of these mediators was significant (b = −.83, t = −2.29 p < .05) indicating partial mediation. Similar mediation analyses were conducted with burnout F(3,51) = 1.45; R
2
= .08; p = .24 (Figure 1(b)), compassion satisfaction F(3,51) = 1.58; R
2
= .09; p = .21 (Figure 1(c)) and compassion fatigue F(3,51) = 1.09; R
2
= .06; p = .36 (Figure 1(d)) as the outcome variables, but none of these models were significant. Path standardized coefficients for police officers from mediation analysis using adaptive Cognitive Emotion Regulation Strategies. Note. Age and biological sex were included as covariates. ACEs = Adverse Childhood Experiences; *p < .05; **p < .001.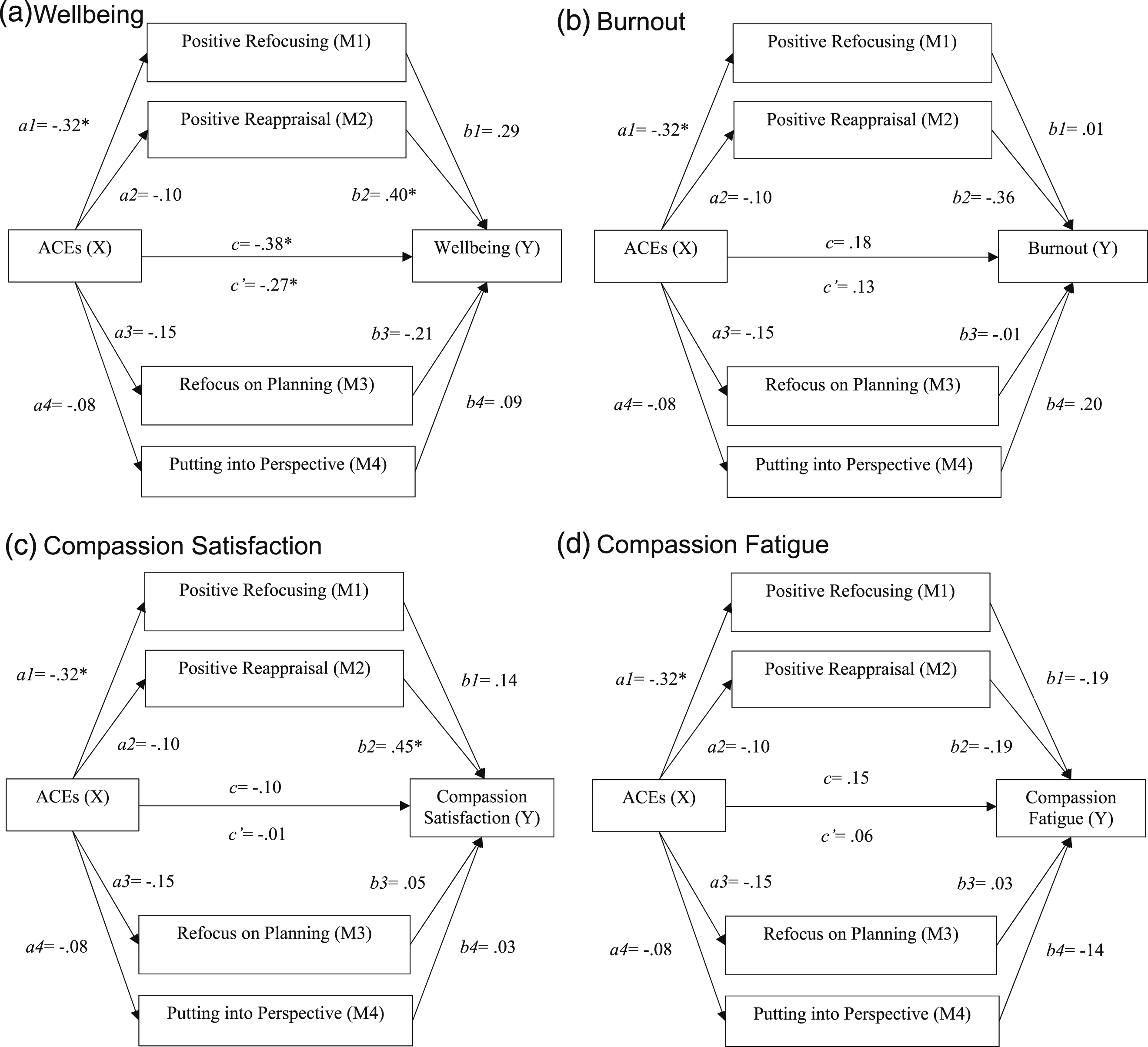
The process was then repeated using the maladaptive CERS as mediators. The total effect of ACEs (X) and Wellbeing (Y) for police officers when examining the maladaptive CERS was significant, F(3,50) = 4.26; R
2
= .21; p < .01 (b = −1.29, t = −3.18, p < .01). ACEs significantly predicted blaming others (b = .44, t = 2.59, p < .05) and ruminating (b = .37, t = 2.03, p < .05) more. In turn, ruminating (b = −1.25, t = −3.58, p < .001) and catastrophizing (b = −.88, t = −2.03, p < .05) predicted poorer wellbeing in police officers (see Figure 2(a)). The indirect effect of ACEs on wellbeing through rumination was the only mediator that was found to be significant (b = .46, 95% CI [−1.10, −0.01]) for police officers. The direct effect of ACEs on wellbeing in the presence of these mediators was also significant (b = −.80, t = −2.13 p < .05) indicating partial mediation (see Figure 2(a)). Similar mediation analyses were conducted with burnout F(3,50) = 1.36; R
2
= .08; p = .27 (Figure 2(b)), compassion satisfaction F(3,50) = 1.66; R
2
= .09; p = .19 (Figure 2(c)) and compassion fatigue F(3,50) = 1.10; R
2
= .06; p = .36 (Figure 2(d)) as the outcome variables, but these models were not significant. Path standardized coefficients for police officers from mediation analysis using maladaptive Cognitive Emotion Regulation Strategies. Note. Age and biological sex were included as covariates. ACEs = Adverse Childhood Experiences. *p < .05; **p < .001.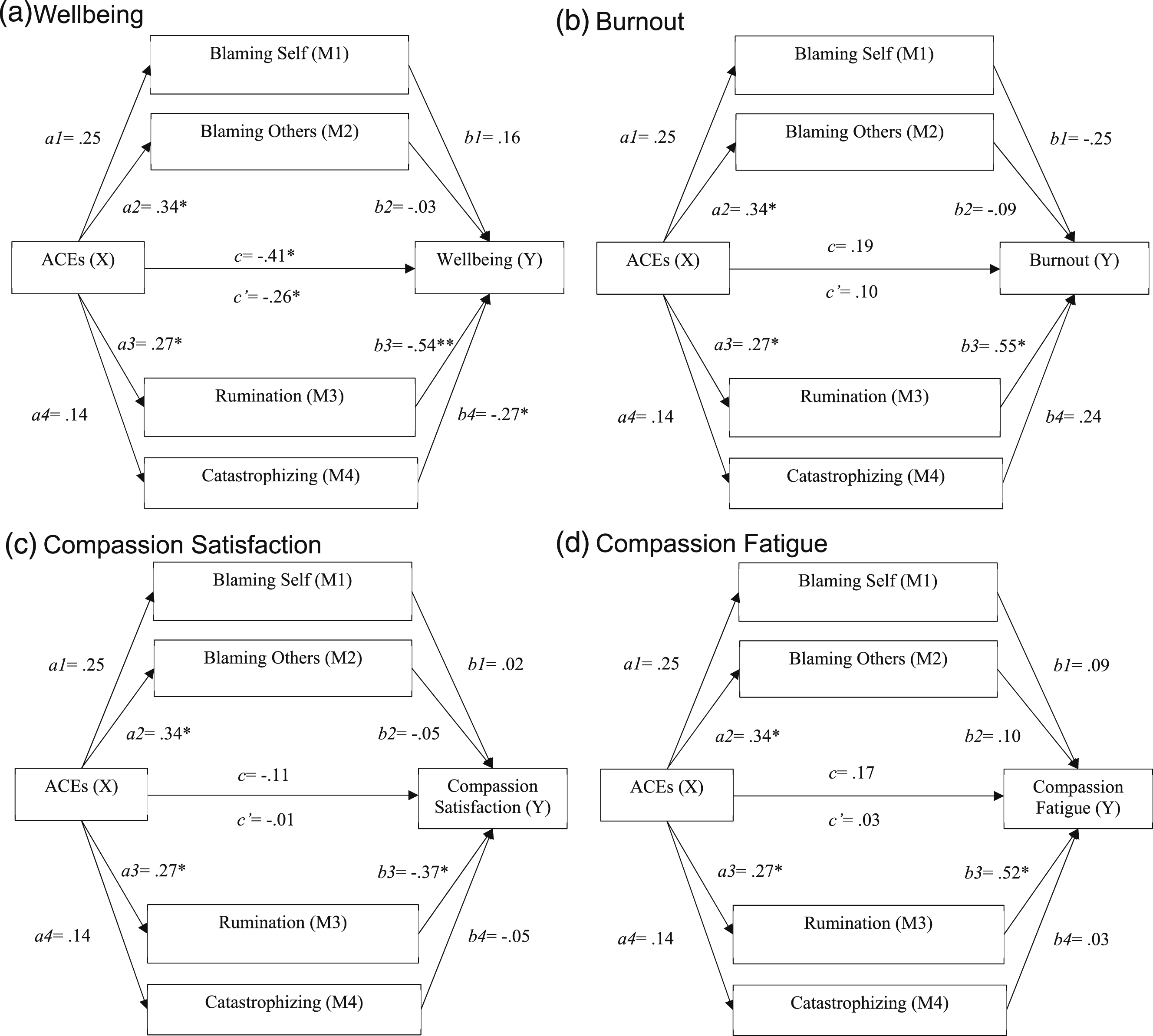
Parallel mediation analyses were also conducted to examine the mediating effect of the different adaptive followed by maladaptive CERS on the relationship between ACEs (X) and wellbeing, burnout, compassion fatigue and compassion satisfaction (Ys) in the community sample, while controlling for age and biological sex. The model examining the total effect of ACEs (X) and Wellbeing (Y) for the community sample, using the adaptive CERS as mediators was significant, F(3,65) = 7.05; R2 = .25; p < .001; the total effect was significant (b = −1.26, t = −3.71, p < .001) and participants age was also significant (b = .22, t = 3.05 p < .01). While ACEs did not predict any of the adaptive CERS, positive reappraisal (b = 1.02, t = 2.55, p < .01) predicted enhanced wellbeing (see Figure 3(a)). No significant indirect effect of ACEs on wellbeing through any of the mediators were found. The direct effect of ACEs on wellbeing in the presence of these mediators was significant (b = −1.32, t = −3.97 p < .001) indicating that in the community sample, ACEs negatively influence wellbeing (see Figure 3(a)). Similar mediation analyses were conducted with burnout F(3,65) = 8.16; R2 = .28; p < .001 (Figure 3(b)); compassion satisfaction F(3,65) = 3.12; R2 = .13; p < .05 (Figure 3(c)); and compassion fatigue F(3,65) = 5.91; R2 = .22; p < .01 (Figure 3(d)); as the outcome variables (Ys). While these models were significant, no significant indirect effect of ACEs on the different outcome variables were found. The direct effect of ACEs on burnout (b = .51, t = 3.47 p < .01), compassion satisfaction (b = −.65, t = −2.72 p < .01) and compassion fatigue (b = .46, t = 2.85 p < .01) and the effect of participants age on the different models respectively (burnout: b = −.12, t = −3.91 p < .001; compassion satisfaction: b = .11, t = 2.05 p < .05; compassion fatigue: b = −.12, t = −3.39 p < .01), in the presence of these mediators were significant, indicating that in the community sample ACEs and participant’s age mostly influenced professional quality of life variables (burnout, compassion satisfaction and compassion fatigue).
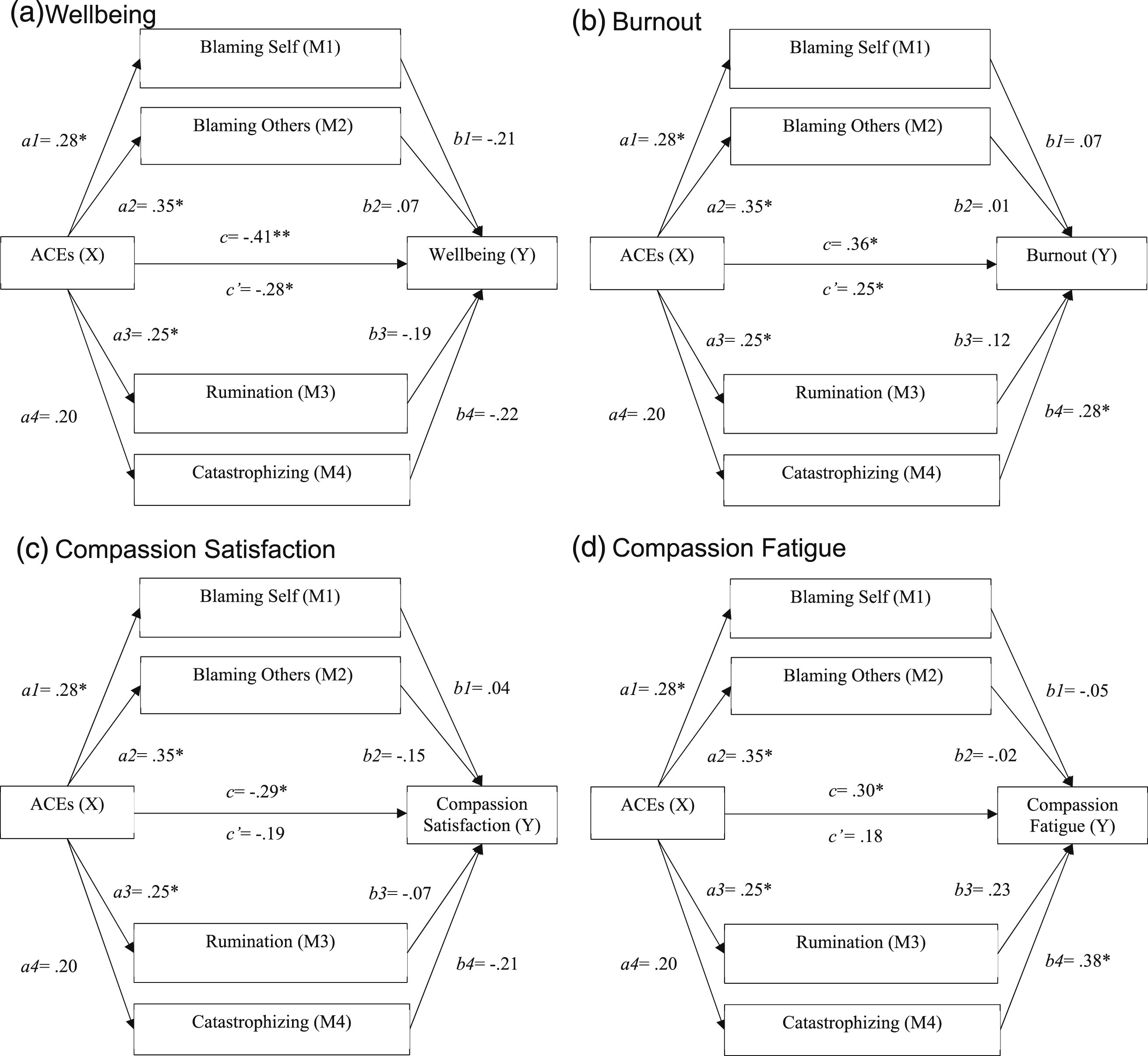
The process was then repeated using the maladaptive CERS as mediators for the community sample. The total effect of ACEs (X) and Wellbeing (Y) for the community sample when examining the maladaptive CERS was significant, F(3,66) = 7.05; R
2
= .25; p < .001 (b = −1.26, t = −3.71, p < .001). ACEs significantly predicted self-blaming (b = .32, t = 2.41, p < .05), blaming others (b = .47, t = 2.94, p < .01) and ruminating (b = .32, t = 2.09, p < .05). However, none of the maladaptive CERS predicted wellbeing in the community sample (see Figure 4(a)). No significant indirect effect of ACEs on wellbeing through any of the mediators were found. The direct effect of ACEs on wellbeing in the presence of these mediators was significant (b = −.87, t = −2.59 p < .05). Also, participants’ age had an effect on wellbeing (b = .22, t = 3.04 p < .01). Similar mediation analyses and findings were conducted and reported for burnout F(3,64) = 8.16; R
2
= .28; p < .001 (Figure 4(b)). Only catastrophizing from the maladaptive CERS predicted burnout (b = .31, t = 2.06; p < .05) in the community sample. The direct effect of ACEs on burnout in the presence of these mediators was significant (b = .34, t = 2.28; p < .05) and participants’ age, had an effect on burnout (b = −.11, t = −3.59; p < .001). While the total effect of ACEs on compassion satisfaction when examining the maladaptive CERS as mediators was significant F(3,64) = 3.12; R
2
= .13; p < .05 (b = −.58, t = −2.44; p < .05), none of the maladaptive CERS predicted compassion satisfaction in the community sample (Figure 4(c)). No significant indirect effect of ACEs on compassion satisfaction through any of the mediators were found. The direct effect of ACEs on compassion satisfaction in the presence of these mediators was non-significant (b = −.38, t = −1.49 p = .14) but participants’ age, had an effect on compassion satisfaction (b = .10, t = 2.05 p < .05) (Figure 4(c)). We also examined if the relationship between ACES and compassion fatigue is mediated by the different maladaptive CERS. The total effect was significant F(3,64) = 5.91; R
2
= .22; p < .01 (b = .43, t = 2.65; p < .05). Only catastrophizing from the maladaptive CERS predicted compassion fatigue (b = .44, t = 2.81; p < .01) in the community sample. No significant indirect effect of ACEs on compassion fatigue through any of the mediators were found. The direct effect of ACEs on compassion fatigue in the presence of these mediators was non-significant (b = .26, t = 1.67; p = .10) but participants’ age had an effect on compassion satisfaction (b = .10, t = 2.05 p < .05) (see Figure 4(d)). Path standardized coefficients for the community sample from mediation analysis using adaptive Cognitive Emotion Regulation Strategies. Note. Age and biological sex were included as covariates. Participant’s age significantly preticted wellbeing (c1 = .34*), burnout (c1 = -.43**), compassion satisfaction (c1 = .25*) and compassion fatigue (c1 = -.39*); ACEs = Adverse Childhood Experiences. *p < .05; **p < .001. Path standardized coefficients for the community sample from mediation analysis using maladaptive Cognitive Emotion Regulation Strategies. Note. Age and biological sex were included as covariates. Participant’s age significantly predicted wellbeing (c1 = .34*), burnout (c1 = −.43**), compassion satisfaction (c1 = .25*) and compassion fatigues (c1 = -.39*); ACEs = Adverse Childhood Experiences; *p < .05; **p < .001.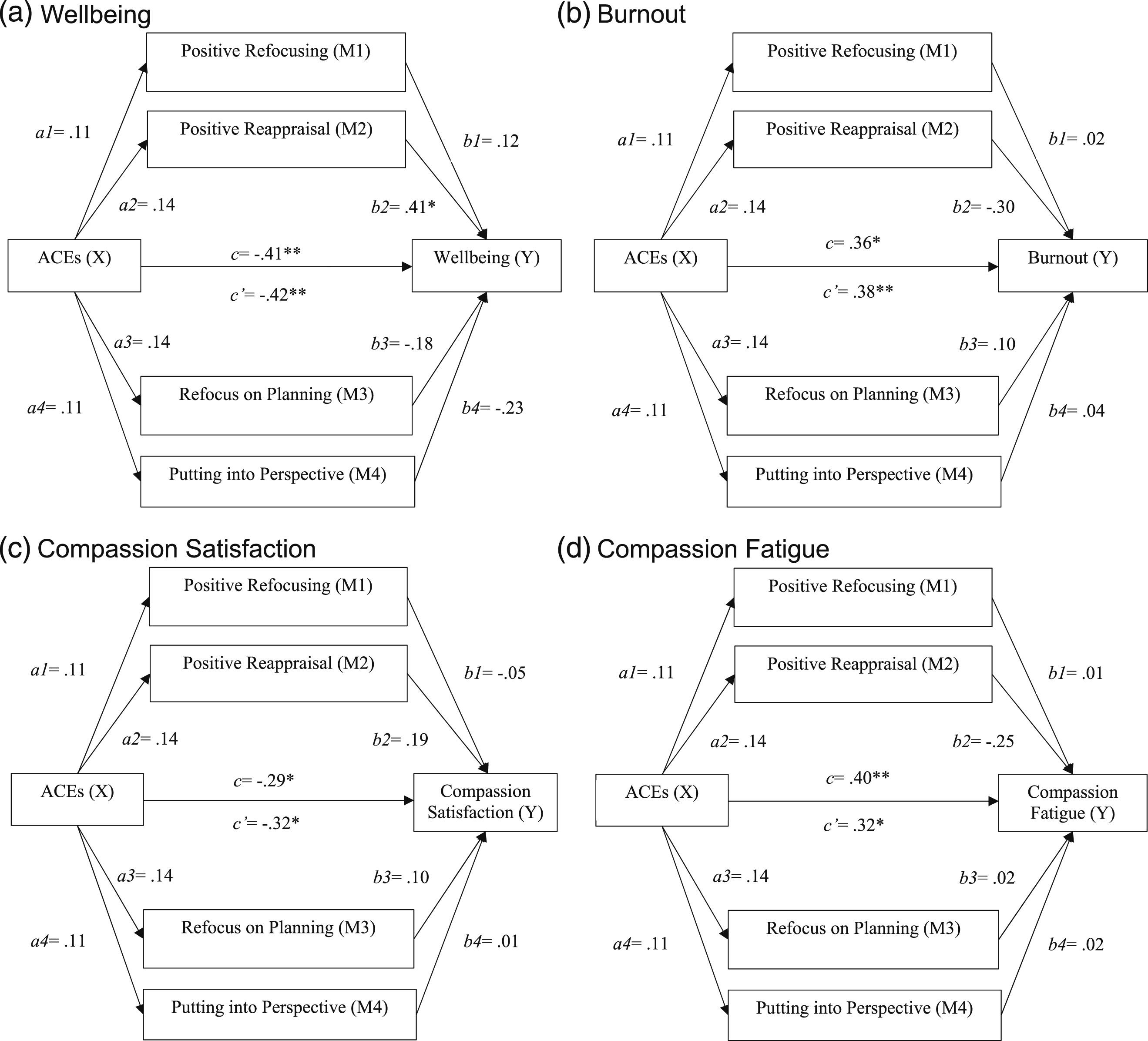
Discussion
The main aim of the present study was to explore factors that contribute to wellbeing and affect the professional quality of life of police officers compared to other professionals recruited from the community. The results highlight that police officers reported lower levels of wellbeing, higher levels of burnout, and a higher number of ACEs, when compared to a community sample, which is generally in line with previous findings (e.g., Backteman-Erlanson et al., 2012; Brady, 2017; McDonald et al., 2022). At the same time, higher ACEs and levels of burnout, as well as poor wellbeing in police officers, was mitigated by increased use of adaptive CERS as compared to the community sample. When examining wellbeing and professional quality of life in police officers, CERS had a stronger influence compared to ACEs. More specifically, maladaptive CERS predicted poorer wellbeing, low compassion satisfaction, and elevated rates of burnout and compassion fatigue, while adaptive CERS predicted the opposite pattern of results (enhanced wellbeing and compassion satisfaction, and low levels of burnout and compassion fatigue). In contrast, in the community sample, only maladaptive CERS arose as a significant predictor in all models associated with poorer wellbeing, compassion satisfaction, and high levels of burnout and compassion fatigue, but adaptive CERS did not. ACEs had an impact on wellbeing and burnout in the community sample, and younger individuals seemed to be at higher risk. The current study also examined how different adaptive and maladaptive coping strategies, mediate the impact of ACEs on wellbeing and professional quality of life variables (burnout, compassion fatigue and compassion satisfaction). ACEs influenced police officers’ wellbeing via rumination, suggesting that ACEs were associated with increased ruminative thinking in police officers which was associated with poorer wellbeing. Findings suggest that there are similar and unique factors related to wellbeing and professional quality of life variables in police officers compared to other occupational groups.
Police officers presented higher burnout rates, with 42% of them identified as high risk (exceeding the 75th percentile cutoff; Stamm, 2010) versus 13% in the community sample, and this prevalence rate is higher than what has been reported by other studies (e.g., 24% focusing on child exploitation investigators; Brady, 2017). Police officers also reported poorer wellbeing, with 20% reporting alarmingly low scores (<40, which has been reported to indicate high risk for depression; Taggart et al., 2016), compared to 12% detected in the community sample. However, other studies report even lower wellbeing scores in police officers (e.g., Jackman et al., 2020). Furthermore, police officers reported experiencing more adversities as children, similar to what has been reported in prior work (e.g., McDonald et al., 2022), however their past experiences did not influence their current wellbeing, but their CERS did (Conway et al., 2024). Several factors could explain this difference: Individuals who chose to become police officers may have developed and effectively use more adaptive CERS as compared to those that did not choose this profession to begin with; hence, while ACEs impacted their maladaptive CERS (ruminating, blaming others), their overall level remained similar to the levels reported by the community sample. Alternatively, this finding may be perceived as indirect evidence of post-traumatic growth in the police force sample. Specifically, owing to higher ACEs, stressors and ultimately burnout scores, police officers become highly resilient, or receive rigorous training (e.g., Chitra and Karunanidhi, 2021) and support that allows them to deal with their past and more recent traumas.
Interestingly, we did not find significant differences in compassion fatigue and compassion satisfaction in the two samples. However, 29% of the police officers (vs 18% of the community sample) showed elevated compassion fatigue and 29% of the police officers (vs 21% of the community sample) reported alarmingly low compassion satisfaction. The prevalence rate for compassion fatigue estimated in the police sample is higher than what is reported in other studies, while the prevalence rate for compassion satisfaction is lower (10% and 40% respectively; Papazoglou et al., 2019). This could suggest that police officers participating in this study had positive feelings about their professional contributions, while effectively managing the routine stressors that are inherent in the nature of their profession at least to a similar level to the community sample. Furthermore, the results suggest that ACEs had a direct effect on influencing burnout and wellbeing, but this was only evident in the community sample. Past adverse experiences seem to have had less of an impact on police officers compassion fatigue and their compassion satisfaction, as they might have received training (e.g., Chitra and Karunanidhi, 2021) that helped prevent past traumatic experiences influencing their current performance. However, the elevated rates of compassion fatigue and low compassion satisfaction detected in the current study should not be ignored and indicate the need to relieve compassion fatigue and promote their ability to experience compassion satisfaction. The Accelerated Program for Compassion Fatigue (Gentry et al., 2002) seems to be promising as it is designed to reduce the intensity, frequency and symptoms associated with compassion fatigue, helping people identify symptoms, recognise triggers, identify and utilise resources and promotes self-compassion, self-care, emotion regulation and developing perceptual maturation, a cognitive skill that allows them to render perceptions about work and self as less toxic (Cocker and Joss, 2016).
Strengths, limitations and future directions
The current study is novel as no prior work to our knowledge examined wellbeing and professional quality of life variables including burnout, compassion fatigue and compassion satisfaction with ACEs and CERS, in police officers and compared them to other professionals. However, the study has limitations that need to be taken into consideration when interpreting the findings. Firstly, this study includes a small number of police officers and this sample might not be representative of the broader police force. We actively recruited police officers, and as such, some bias is inevitable. Furthermore, our community sample included participants from different professions, and this did not allow us to examine or compare police officers to specific occupational subgroups (e.g., in healthcare, education). Secondly, our data were collected during a single assessment, using exclusively self-reports limiting the extent of causal inferences that can be drawn, as it is not possible to determine or to evaluate the long-term impact of these variables on wellbeing, burnout, compassion fatigue and compassion satisfaction. Longitudinal studies incorporating other forms of assessments are needed to replicate the current results with larger samples that would allow comparing police officers to specific occupational groups (firefighters, doctors, nurses) and detect the potential long-term effects.
Implications and conclusion
In terms of policy-based interventions, findings highlight the need to focus on individual as well as organisational factors, to enhance wellbeing, compassion satisfaction and reduce burnout and compassion fatigue (Cohen et al., 2019; Phythian et al., 2022). The current findings also inform the blue light wellbeing framework for police officers documenting the importance of one of the sections: personal resilience which seems to be the least developed (Phythian et al., 2022), with our findings highlighting the importance of incorporating adaptive coping strategies (positive refocusing, positive reappraisal) and replacing maladaptive ones (rumination, catastrophising, blaming others). During the recruitment process companies more generally, who are hiring individuals for demanding positions, including the police force, should incorporate a baseline assessment of employees coping strategies. This would allow them to identify which employees are more vulnerable and need help adopting more adaptive coping strategies which can be introduced in training. Furthermore, companies need to help employees possibly affected by their ACEs stop engaging in maladaptive CERS strategies. Education on the subject should be provided during initial recruitment but also when providing continuing education opportunities so employees and police officers are better able to identify when they are engaging in maladaptive thinking patterns. Furthermore supervisors need to remain vigilant in identifying maladaptive coping, as some professionals might be less likely to seek help themselves (Doyle et al., 2023; Porter and Lee, 2024; Violanti et al., 2017). These results may serve as a call to action for companies more generally and police departments more specifically to cultivate a culture that prioritizes wellbeing and professional quality of life (Phythian et al., 2022; Porter and Lee, 2024).
Footnotes
Acknowledgements
The authors would like to acknowledge the contributions from the following students around their assistance, time and effort in supporting the process of data collection: Aimee McDermott, Sharma Siddhant, Jinjutha Panich, Sanjeevani Deoghare and Julia Grutters.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.