
Abstract
Motor skills enable multi-facetted interactions with the environment and allow children to develop social skills and respond appropriately to situational social demands when interacting with peers and adults. Previous research with clinical samples (e.g., children diagnosed with Developmental Coordination Disorder) showed that children’s motor skills are closely linked to their psychosocial behavior (e.g., prosocial, hyperactive, inattentive, interpersonal), but studies with typically developing children are rare. We sought to fill this research gap by examining relationships between gait variability as an indicator of motor skills and prosocial behavior, problem behavior, and risk-taking behavior in typically developing children. Participants were a large cross-section of 7-13-year-olds (N = 221). They were asked to walk normally across an electronic pathway (GAITRite). We assessed their gait variability (i.e., stride time, stride length and stride velocity). Their parents completed the Strengths and Difficulties Questionnaire that assessed their child’s prosocial behavior, hyperactivity, emotional symptoms, and any conduct or peer relationship problems. Parents also provided information on an adapted scale of the Tridimensional Personality Questionnaire assessing risk-taking behavior. We used multilevel modeling to account for individual interdependence and to analyze the maximum number of strides for each participant. Children with greater stride length variability and velocity showed significantly less prosocial behavior, had more emotional symptoms and demonstrated less risk-taking behavior. Stride time variability was not significantly related to any variables. These results align with past findings that gait is sensitive to motor skill differences, and they extend past findings of these associations between gait and facets of intra- and interpersonal characteristics among children within clinical disorders to typically developing children.
Introduction
Motor behavior has been associated with psychosocial skills and general wellbeing in that the accuracy and coordination of movement is essential to psychological and social development (Mancini et al., 2019; Piek et al., 2006). This relationship might be explained with the embodied cognition theory, according to which motor skills facilitate social interaction (Harbourne & Berger, 2019). Optimal motor development in young children may enable play with peers, which, in turn, supports the development of social skills and interpersonal relationships (Mancini et al., 2019). Accordingly, children with poor motor skills are often victims of social ostracism as well as bullying and show low self-esteem (Missiuna & Campbell, 2014).
Several studies suggest that poor motor skills are a risk factor to optimal development in several domains of psychosocial functioning (Mansoubi et al., 2020). In previous studies, the term “poor motor skills” has been used as an umbrella term, covering a variety of observations that describe clumsy or uncoordinated behavior (Bejerot et al., 2013). Typically, investigators have used three methodological approaches to measure children’s poor motor skills: (a) diagnostic determinations of developmental coordination disorder (DCD; e.g., according to the DSM-V); (b) standardized measures of motor performance (M-ABC-2; Henderson et al., 2007) for identifying motor skills that are below the 16th percentile in relation to the general population and indicate potential DCD; and (c) parent observations as determined through parent-completed questionnaires such as the DCD-Questionnaire which indicates or suspects DCD below a score of 46–57, depending on the age group (Wilson et al., 2009). These methods of operationalizing motor deficits have been applied within clinical samples, based on certain cut-off values. However, a more dimensional view with continuous rather than categorical perspectives or groupings of motor abilities may suggest similar associations for typically developing children.
The Environmental Stress Hypothesis has conceptualized how children’s poor motor skills may contribute to emotional difficulties in which children internalize emotional discomfort such as anxiety and depression (Cairney et al., 2013; Mancini et al., 2016). According to this theoretical framework, poor motor coordination is a primary stressor that increases a risk for experiencing intra- and interpersonal conflicts (e.g., decreased self-esteem or experiences with bullying) that in turn lead to internalizing problems (Blank et al., 2019; Cairney et al., 2013). Past empirical evidence has supported this relationship between poor motor skills and children’s mental health and behavioral problems when these variables have been studied in children with clinical conditions (Bouffard et al., 1996; Cantell et al., 1994; Mancini et al., 2019; Skinner & Piek, 2001). This association has seemed to begin early in life, as shown by a longitudinal study that examined the development of gross motor skills up to the age of four years and later assessed anxiety and depression scores at school age (Piek et al., 2010). The authors found gross motor skill development at early childhood predicted later emotional symptoms. This increased risk of intrapersonal difficulties was also supported by an increased probability of lower prosocial skills, hyperactivity, inattention, and emotional symptoms in children with poorer motor skills than their peers (Lingam et al., 2012). In addition, children with poor motor skills have appeared more nervous and less sociable, and they have experienced more social exclusion from peer play (Engel-Yeger & Hanna Kasis, 2010; Smyth & Anderson, 2000; Zwicker et al., 2012). These interpersonal difficulties were further supported by research findings that children with poor motor skills spend more time alone, report fewer friends, interact less positively with peers and perceive less social support (Lingam et al., 2012; Mancini et al., 2019; Poulsen et al., 2008). Even though children with poor motor skills are at greater risk of being bullied and victimized (Bejerot et al., 2013; Campbell et al., 2012; Piek et al., 2005), there has been no evidence that they are at significant risk for more externalizing behavior problems such as conduct problems (Lingam et al., 2012), as less is known about the relationship between motor skill difficulties and delinquent behavior such as lying, cheating and stealing. Also, novelty seeking, risk-taking and reward dependence have not yet been examined in relation to children’s poor motor skills.
As a consequence of their negative social experiences, children with poor motor skills have often used avoidance as a coping strategy (Bouffard et al., 1996), and they have been seen to withdraw from situations that may involve motor competence. This avoidance may emerge due to children’s fear of failure and peer criticism, and it may create a vicious circle, such that reduced social interactions yield fewer opportunities to practice motor skills, with accentuated movement problems which result over time (Cairney et al., 2013; Skinner & Piek, 2001), leading to further reductions in social participation and even greater risk of emotional and behavioral problems (Schoemaker & Kalverboer, 1994; Zwicker et al., 2012). Whereas poor motor skills are often seen as a primary stressor for developing emotional and behavioral problems, as suggested by the Environmental Stress Hypothesis, this relationship may be more reciprocal than has been previously assumed (Cairney et al., 2013; McClelland & Cameron, 2019). Research examining the bidirectional nature of these associations and the potential cascading effects has been sparse to date and is needed now.
In the present study, we attempted to build upon prior research by using a novel methodological approach in which we assessed children’s gait as an indicator of their motor ability, and we related gait functioning to inter- and intra-personal behavior. Gait is a type of locomotion which requires coordination between the central nervous system and lower limb motions (Adolph & Berger, 2006). Infants reach the motor milestone of walking at around the first year of life (World Health Organization, 2006). Afterwards, their gait reaches a stabilized and mature pattern at around seven years of age (Adolph et al., 2003), with some gait characteristics such as gait variability still under development well into adolescence (Danion et al., 2003; Hagmann-von Arx et al., 2016). Considering this lengthy developmental progression, gait variability is a sensitive measure of general motor skill development and it may be used to reflect poor motor ability (Van Emmerik et al., 2005) and study the reciprocal relationship of poor motor ability and psychosocial functioning.
Several investigators have suggested a specific relationship between gait and facets of a child’s intra- and interpersonal characteristics (e.g., Mansoubi et al., 2020; Schneider et al., 2014). When infants learn to walk, their relationships to objects and other people change, which, in turn, allows them to make changes in their initiation of social interactions (Iverson, 2010) to create a context for acquiring psychosocial skills (Karasik et al., 2011). Consequently, when children’s motor abilities are not age-appropriate, they may impact general behavior and psychosocial functioning (Hagmann-von Arx et al., 2016). Further evidence comes from research showing that emotional states can be reflected in the human gait. For example, the work “Show me how you walk and I tell you how you feel” demonstrated that negative (i.e., angry) emotional walking was associated with enhanced brain activation (Schneider et al., 2014). Similarly, Atkinson et al. (2012) found an increase in brain activity for happy body movements. Gross et al. (2012) showed that adults increased their walking speed when they felt joy and anger. In studies with clinical samples, investigators have suggested relationships between decreased gait speed and anxiety (Zhao et al., 2019) and depressive symptoms (Lemke et al., 2000; Michalak et al., 2009). Finally, in studies focusing on the relationship between gait and social victimization, several investigators demonstrated that walkers’ self-reported experiences in victimization were associated with more vulnerable gait cues (i.e., less synchronous, less fluid, long or short strides) as identified by naïve observers (Blaskovits & Bennell, 2019; Grayson & Stein, 1981).
Despite this focus on gait in adult studies, investigations of the relationship between children’s gait and their intra- and/or interpersonal difficulties have been rare. To our knowledge, only one recent study examined this relationship in a sample of 13-year-olds (N = 76). This research team found that children with more emotional symptoms and overall behavior difficulties walked faster with shorter steps (Mansoubi et al., 2020). Clearly, more research with children of a broader age range and involving a larger array of intra- and interpersonal characteristics is needed. Our aim in the current research was to study these associations in a large, cross-sectional sample of typically developing 7-13-year-old children. We assessed children’s gait variability objectively and reliably with an electronic pathway and measured their intra- and interpersonal characteristics with parental reports. Given that gait variability shows a considerable developmental progression well into adolescence (Danion et al., 2003; Hagmann-von Arx et al., 2016), we focused on this specific indicator of children’s gait. We hypothesized that children with higher gait variability would show fewer prosocial skills, more hyperactive behavior, more emotional symptoms and more peer problems. We also explored relations between gait variability and both conduct problems and risk behavior.
Method
Participants
Participants’ Descriptive Statistics for Key Variables Including the Correlation Matrix for Parent-Completed Questionnaires.
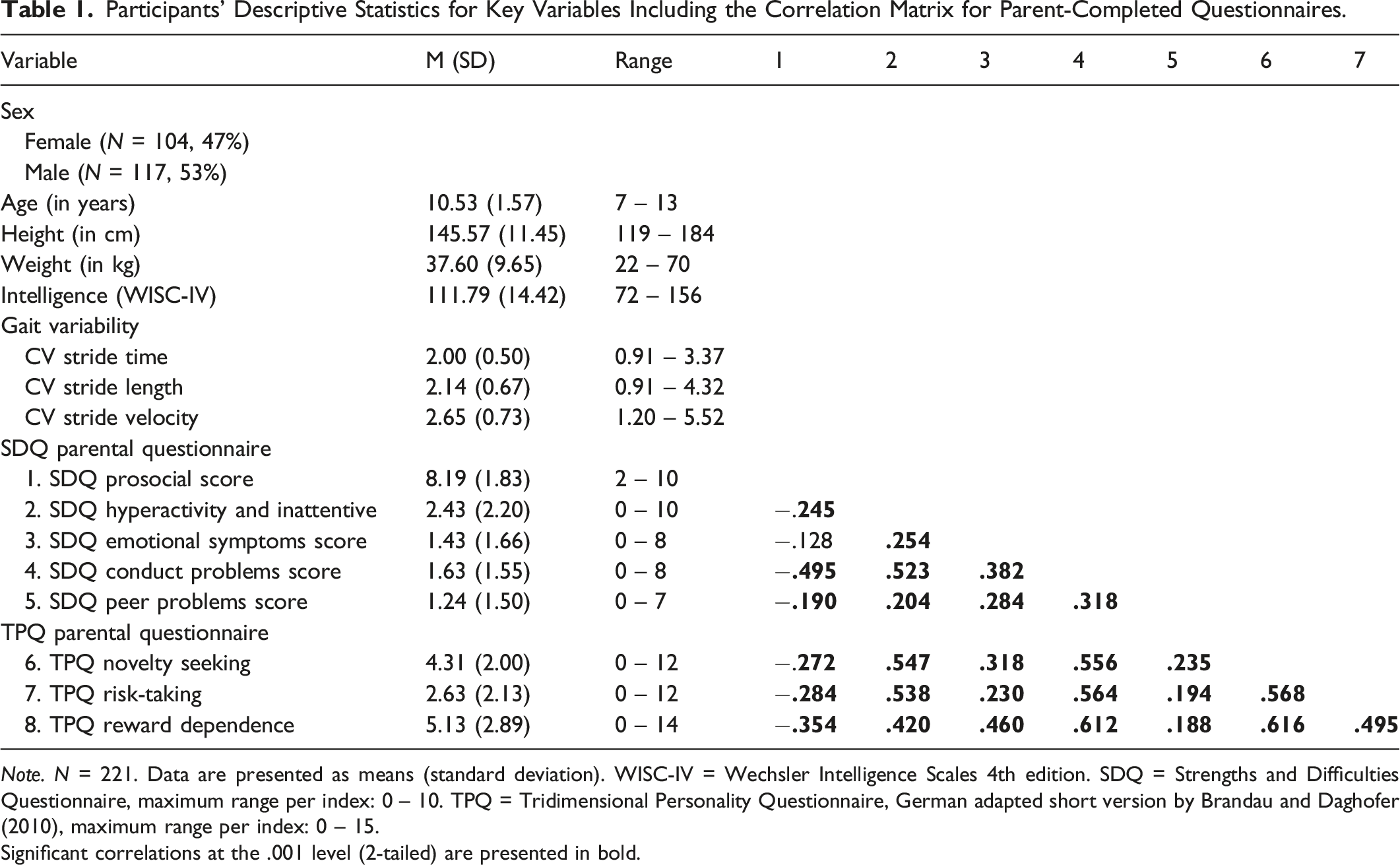
Note. N = 221. Data are presented as means (standard deviation). WISC-IV = Wechsler Intelligence Scales 4th edition. SDQ = Strengths and Difficulties Questionnaire, maximum range per index: 0 – 10. TPQ = Tridimensional Personality Questionnaire, German adapted short version by Brandau and Daghofer (2010), maximum range per index: 0 – 15.
Significant correlations at the .001 level (2-tailed) are presented in bold.
Measures and Procedure
Prior to assessing participants’ normal walking, we gathered their anthropometric data (e.g., height, weight and leg length). They then walked over an electronic carpet system at their own self-selected pace. To account for children’s varied intellectual functioning, we gathered data regarding their performance on four subtests (Vocabulary, Matrix Reasoning, Letter-Number Sequencing, and Coding) of the German version of Wechsler Intelligence Scale for Children 4th edition (Petermann & Petermann, 2011; Wechsler, 2004). These were pro-rated to yield an estimated summary intelligence score (Waldmann, 2008) that we could use as a control variable.
Parent Reports
Participants’ parents completed several standardized questionnaires, including the Strengths and Difficulties Questionnaire (SDQ; Goodman, 1997) to assess children’s prosocial and problem behaviors, and an adapted version of the Tridimensional Personality Questionnaire (TPQ; Brandau & Daghofer, 2010; Cloninger et al., 1991) assessing children’s risk-taking behavior.
The SDQ is a reliable and valid screening tool in which parents can identify behavioral problems in children aged 4–16 years (present sample: total α = .71; strength α = .72; difficulties α = .81). The questionnaire can be separated into five subscales with five items each on a 3-point Likert scale (Goodman, 1997). The strength domain is measured by the first subscale: (a) prosocial behavior (e.g., “considerate of other’s feelings”). The other four subscales measure difficulties: (b) hyperactive and inattentive behavior (e.g., “restless, overactive”); (c) emotional symptoms (e.g., “often seems worried”); (d) conduct problems (e.g., “often lies or cheats”); and (e) peer problems (e.g., “generally liked by other children”).
Based on Cloninger’s three-dimensional model of personality (Cloninger et al., 1991), the TPQ was adapted and validated into a short 15-item parental questionnaire in German (2010). This version permits a reliable assessment of children’s risk-taking behavior (present sample: α = .86). Notably, Cloninger’s dimension “harm avoidance” was reversed into the dimension “risk-taking” (Brandau et al., 2011). This adapted questionnaire consists of three subscales with five items each on a 4-point Likert scale: (a) novelty seeking (e.g., “interrupts monotonous activities”); (b) risk-taking (e.g., “does things others find risky”); and (c) reward dependence (e.g., “easily frustrated”).
Walking Assessment
We assessed children’s walking ability with the gait assessment system GAITRite (CIR Systems, NJ), an objective, reliable and valid measure of gait (Dusing & Thorpe, 2007). The GAITRite is a 7 meter long carpet in which over 23′000 sensors are embedded. Additional 1.25 meter inactive sections in the beginning and end of the carpet accounted for effects of acceleration and deceleration. In the present study, we included two cross-sectional samples, with one subsample (n = 88) completing 4 walks across the electronic walkway and the other subsample (n = 133) completing 8 walks. 1 The GAITRite recorded different gait parameters: temporal (stride time), spatial (stride length) and spatial-temporal parameters (stride velocity). The analysis focused on participants’ stride-to-stride fluctuations (i.e., gait variability), represented by the coefficient of variation (CV; Yogev et al., 2005).
Statistical Analyses
We determined and excluded outliers (mean ± 3 SDs) within the gait parameters (1.14%). Further, we computed gait variability on three variables (a) stride time, (b) stride length and (c) stride velocity (e.g., CV stride time = stride time standard deviation/stride time mean x 100). Since participants repeated their normal walking for 4-8 walks, these data showed a differential, nested structure, with subsequent walks being more closely related with respect to gait characteristics as opposed to, for example, the first and last walk. The use of a multilevel modeling (MLMs) approach took this difference and individual interdependence into account and allowed an analysis of the maximum number of strides for each participant. Moreover, MLMs are a form of regression models which determine standardized coefficients and p-values but have the advantage of considering potential grouping of the data.
We conducted a two-level structural analysis model to examine the relationships between children’s gait and their intra- and interpersonal characteristics. In Level 1, we analyzed gait variability across individual walks (CV stride time; CV stride length; CV stride velocity); and, in Level 2, we included characteristics of the individual child (age, sex, intelligence, and parental report). Sex was coded with ‘-1’ for females and ‘+1’ for males. Previous studies have often included age, height and weight as control variables, but age correlated highly with height (r = .835) and weight (r = .716), as did height with weight (r = .854) and this potential collinearity was confirmed through the diagnostic values in the present data (VIF > 3). Therefore, only age was included in the following analyses to prevent collinearity issues. 2 Missing values were handled with the maximum likelihood estimation approach. Three separate models were conducted for each gait variability. In the null model, age, sex, and intelligence were included as level 2 effects. Subsequently, a full model was computed by adding the dimensions of the SDQ and the TPQ as level 2 effects to the null model. To test the effects of these intra- and interpersonal characteristics, the full model was then compared to the null model. The Statistical Package for the Social Sciences (SPSS, Version 26, IBM Corp.) was used for these MLMs analyses, and statistical significance was set at p < .05.
Results
An overview of the children’s demographic and anthropometric characteristics and other descriptive statistics can be found in Table 1. The first full model with children’s CV stride time did not significantly improve the model fit compared to the null model (χ2 = 13.23, df = 8, p = .104). Thus, even though some variables reached significance in the full model of CV stride time, those were not interpreted. However, the models with CV stride length (χ2 = 30.33, df = 8, p < .001) and CV stride velocity (χ2 = 20.52, df = 8, p < .01) resulted in a significant improvement of the model fit after adding the variables of the SDQ and TPQ to the null model.
Variance Contributed by SDQ and TPQ Scales, and Control Variables in Children’s Gait Variability: Linear Mixed Models.
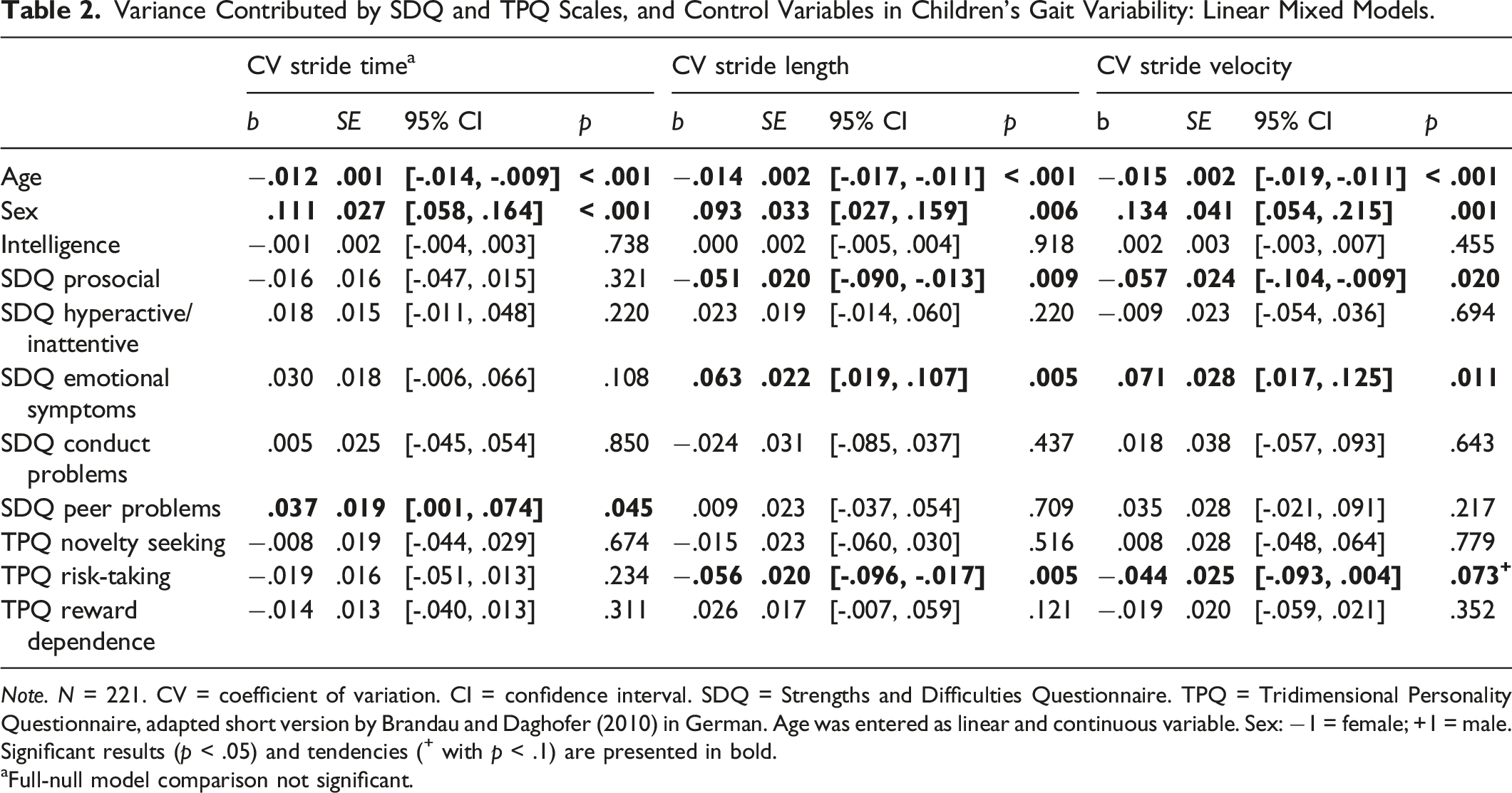
Note. N = 221. CV = coefficient of variation. CI = confidence interval. SDQ = Strengths and Difficulties Questionnaire. TPQ = Tridimensional Personality Questionnaire, adapted short version by Brandau and Daghofer (2010) in German. Age was entered as linear and continuous variable. Sex: −1 = female; +1 = male.
Significant results (p < .05) and tendencies (+ with p < .1) are presented in bold. aFull-null model comparison not significant.
The models with CV stride length and CV stride velocity demonstrated similar patterns. Children’s gait variability in normal walking (stride length: b = −.051, p < .01; stride velocity: b = −.057, p < .05) was related to their prosocial behavior. In addition, gait variability (stride length: b = .063, p < .01; stride velocity: b = .071, p < .05) was also significantly related to children’s emotional symptoms. More concretely, we found that children whose parents rated them with more prosocial behavior walked with less variable stride length and stride velocity. Furthermore, children with more emotional symptoms walked with higher variability in stride length and velocity. Additionally, the relationship between risk-taking and gait variability was significant for CV stride length (b = −.056, p < .01), while there was a tendency toward a significant relationship between risk-taking and CV stride velocity (b = −.044, p = .073), such that children with lower risk-taking behavior showed a higher gait variability.
Discussion
In the present study, we examined associations between gait variability and facets of intra- and interpersonal behavior in a large, cross-sectional sample of typically developing 7- 13-year-olds. As hypothesized, we found that children with fewer prosocial skills showed higher gait variability in both stride length and stride velocity. This result is in line with previous research focusing on children with DCD, showing that children with this diagnosis more often played alone, or watched other children playing or moving around without being engaged in peer play (Smyth & Anderson, 2000). This isolation and lack of peer interaction carries risks for continued poor social and motor skills (Cairney et al., 2013; Smyth & Anderson, 2000). Secondly, as hypothesized, our findings suggested that children with more reported emotional symptoms (e.g., physical discomfort, nervousness, sadness and anxiety) produced higher gait variability in stride length and velocity. These results are also in line with previous research (Mansoubi et al., 2020) and support the Environmental Stress Hypothesis (Cairney et al., 2013). Thirdly, as opposed to previous research with children diagnosed with DCD, associations between gait variability and the subscales of hyperactivity and peer problems revealed non-significant effects in our sample of typically developing children. However, our findings of non-significant effects regarding conduct problems are in line with one previous study (Lingam et al., 2012), which similarly demonstrated that children with motor weaknesses did not show an increase in conduct problems.
Our exploratory research regarding associations between gait and risk-taking behavior revealed inverse relations between risk-taking and gait variability in stride length and stride velocity. Children who were reported to engage in more risky activities and overestimate their own skills showed more gait regularity with respect to stride length and stride velocity. Conversely, this result implies that children who were reported to be less risk-taking and more cautious showed higher gait variability. A possible explanation could be that children with riskier behavior seek more demanding situations and explore their boundaries. These situations often involve higher physical activity and may train various aspects of children’s motor abilities, which may lead, in turn, to less gait variability. In addition to this finding, measures of novelty seeking and reward dependence were not significantly related to gait variability.
Strengths, Limitations and Directions for Further Research
Overall, strengths of this study included a large sample, with multiple gait repetitions that were measured objectively and reliably. Moreover, measurements of all walks were included by the MLMs approach that accounted for the interdependence between walks. The sensitivity of gait variability and the evaluation of all questionnaire scales enabled precise, comprehensive, and transparent reporting. In that respect, a possible limitation was our reliance on parent reports of their children’s behavior. Especially, in later childhood, adolescents have been found to report more internalizing and externalizing problems in self reports than were reported by their parents (Seiffge-Krenke & Kollmar, 1998). Since our youngest participants were 7 years old, self-reports were not feasible in this study. Supportively, there has been satisfactory internal consistency between parental- and self-report on the SDQ (Koskelainen et al., 2000). Future studies might include self-reports, interviews and more objective measures of children’s behavior. Furthermore, even though we included a wide age range (7–13 years) of participants, future investigators might examine the relationship between children’s gait and their intra- and interpersonal characteristics at ages above and below this age range. It seems likely that results may differ across and between age groups, as developing social behavior contributes to the major developmental tasks across the first years of life (Williams & Berthelsen, 2017), and internalizing as well as externalizing problems change across childhood and adolescence (Wong et al., 2021). In addition, future studies should include information of onset age of walking to clarify potential effects on variability. Our cross-sectional research design is a further limitation that prevents causal assumptions between these correlations. An additional longitudinal study with crossed-lagged design testing these relationships would be informative going forward.
Conclusion
In summary, data from this study provide insights into how children’s normal walking relates to their psychosocial behavior. We found significant relationships between gait variability and children’s prosocial behavior, their emotional symptoms, and their risk-taking behavior. These findings are in line with earlier research in clinical populations demonstrating that intra- and interpersonal behaviors are related to children’s body movements (Simpson et al., 1993). However, our findings add dimensionality to this association, since we show that typically developing children whose motor weaknesses are not categorized as clinically significant also show associations with intra- and inter-individual characteristics, leading to the conclusion that typically developing children at the lower end of motor abilities similarly as clinical samples should be entitled for support programs and interventions. Especially, as the current significant associations are found above effects of age, children do not seem to outgrow their gait variability. An important implication of these findings is that an awareness of children’s early motor difficulties, perhaps with gait in particular, can be a path toward early identification of and early interventions for children at risk for emotional and interpersonal problems.
Footnotes
Author’s Note
The present data have not been presented at a conference. Furthermore, the present research is neither available on a listserv nor on a website.
Acknowledgments
We thank our interns and master students involved in the research project “Cognitive and Motor Development” at the University of Basel, Switzerland for their help with data collection and data entry. We are grateful to the Research Fund of the University of Basel, Switzerland (Project: Thinking while Walking: The Relative Influence of Different Executive Functions on Children’s and Adults’ Gait, Grant number DPE2158) for funding the present research. The funding source had no involvement in study design, collection, analysis, and interpretation of the data, the writing of the manuscript, and the submission process.
Author Contributions
Declaration of Conflicting Interests
The authors declare that there are no conflicts of interest and that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research Fund of the University of Basel, Switzerland. Project: Thinking while Walking: The Relative Influence of Different Executive Functions on Children’s and Adults’ Gait. Grant number: DPE2158.