
Abstract
High levels of perceived motor competence and low levels of actual motor competence in youth populations have been reported world-wide. Both perceived and actual motor competence have been deemed independent correlates of health and physical activity (PA) behavior, and past research has indicated that their alignment may be linked to more consistent PA. Moreover, there is potential for a movement-based intervention to strengthen the alignment between perceived and actual motor competence, perhaps then guiding future health, PA, and community sport engagement globally. Thus, the objective of this study was to investigate the effectiveness of an 8-week movement-based intervention on increasing the alignment (i.e., veridicality) between PMC and AMC among Irish adolescent youth. We collected data on adolescents (n = 324; females = 149; M age = 14.5, SD = 0.88 years) across six second-level schools in Ireland, including measurements of actual and perceived, motor competence at pre- and post-intervention. We observed low levels of actual in contrast to high levels of perceived motor competence. We found a small but significant veridical alignment between perceived and actual motor competence, but there was no intervention effect on alignment. Future research should prioritize a longer intervention duration that targets student learning and understanding in order to develop veridical perceptions in adolescents that might sustain their participation in PA.
Keywords
Introduction
Physical Activity (PA) levels remain low across the globe (Farooq et al., 2020). As low PA levels are associated with a higher degree of obesity, and increased risk of non-communicable diseases, increasing PA levels must become a core part of efforts to improve the health of future generations (Farooq et al., 2020; Mannocci et al., 2020). Within the Irish context, these trends remain prevalent and disconcerting, with only 13% of Irish children meeting current recommendations for 60 minutes of PA per day (Woods et al., 2018). Improving PA levels in adolescents may improve their mental health and bone mineral density (Faienza et al., 2020; Murphy et al., 2020). Actual Motor Competence (AMC), refers to any form of goal-directed human movement, and it is a crucial component to physical health and wellbeing (Bardid et al., 2019; Robinson et al., 2015). AMC is viewed as a critical contributor to long-term PA participation, and high levels of AMC have been associated with greater cardiorespiratory and health-related fitness (Cattuzzo et al., 2016; Lubans et al., 2010). There is also strong evidence that a healthy weight status is linked with improved AMC, and unhealthy weight status can act as an antecedent or a consequence of poor AMC (Engel et al., 2018).
While AMC proficiency levels vary by region, common findings indicate that young children currently possess below par movement skills compared to children of previous generations (Bolger et al., 2021). Mean scores for AMC in global research are consistently close to the mid-way point for targeted expectations, in China (n = 282; M age 8.4, SD = 0.56 years; Chan et al., 2018), and cross-culturally (n = 358; 191 males; 167 female; M age = 8.35, SD = 0.65 years), based on a study conducted in Germany and Australia (Tietjens et al., 2020). Weaker results were found in Brazil (n = 2,337; 1,194 male, 1,183 female; M age = 7.4, SD = 1.9 years), where less than half of the children between the ages of 3 to 10 years demonstrated proficiency across all locomotor skill
Philpott et al (2020) recently examined age-related AMC associations in Irish adolescents (n = 373; M age = 14.38, SD = 0.87 years) and further supported the stagnation of basic AMC with proficiency levels above 40% only evident for two skills – the run and the catch (Philpott et al., 2020). Undeveloped AMC among Irish adolescents may contribute to declines in their PA behavior in both their adolescence and adulthood (Lester et al., 2017; Lunn et al., 2013).
The influence of perceived motor competence on AMC and PA habits must also be considered, especially in light of emerging evidence of their connection (Tietjens et al., 2020). Perceived Motor Competence (PMC) refers to a person’s belief in their ability to perform goal-directed human movement (i.e., their estimation of their own level of AMC) (Estevan & Barnett, 2018). In early theoretical constructs of PMC and physical perceptions (i.e. Competence Motivation theory) higher levels of perceived competence were desirable, as high perceptions were associated with greater task persistence and motivation for PA (Harter, 1978). High self-perception levels have been associated with greater motivation and PA engagement, and greater motivation for Physical Education (PE) participation in recent studies (Estevan, Bardid et al., 2021; Harter, 1978). While there is some evidence that higher levels of overall PMC are associated with PA (Visser et al., 2020), stronger associations were found specifically between object-control related PMC and PA (Slykerman et al., 2016). Notably, in global research, overestimation of personal competence has been commonplace among children and adolescents (Rogers et al., 2018; Van Veen et al., 2020), and it has been problematic, as it may lead to dangerous risk taking culminating in injury, and has been associated with lower levels of PA, compared to accurate estimations of ability (Schmidt et al., 2013b; Utesch et al., 2018). Irish children and adolescents have similarly been found to have high PMC, despite their low levels of AMC (O’Brien et al., 2018; Philpott et al., 2020) with similar findings reported globally across different physical self-perception toolkits such as the Physical Self-Perception Profile, the Self-Perception Profile for Children, and the Pictorial Movement Scale for Children (Barnett et al., 2008; Rogers et al., 2018; Vedul-Kjelsås et al., 2012). Consistent findings of high levels of perceived competence across these toolkits have led researchers to question the alignment between perception toolkits and AMC tests (Estevan & Barnett, 2018). New research examining this alignment of PMC and AMC values, known as ‘veridicality’ has now emerged (Clark et al., 2018).
Veridicality, in this context, relates to the accuracy or alignment of perceived and actual motor competence (Schmidt et al., 2013a, 2013b). Concurrent research has suggested that the accurate estimation of AMC may form a key role in consistent PA participation (Morano et al., 2020; Utesch et al., 2018). Veridical perceptions have also been associated with higher levels of achievement motivation (i.e., a desire to meet goals) and persistence toward success (Horn, 2008).
Researching the accuracy of PMC in relation to AMC has been cited as a critical new need (Clark et al., 2018; Morano et al., 2020). Given a relative paucity of research on adolescents in relation to PMC (De Meester et al., 2020; Lander et al., 2019), applying veridicality research to this age group is also important, as the adolescent period is fraught with frequent dropouts from sport and PA participation (Bryant et al., 2014; Lunn et al., 2013). Adolescent cognitive development has led some to predict greater accuracy of PMC (De Meester et al., 2020; Stodden et al., 2008), but overestimation of personal AMC within this age group has been very common (Philpott et al., 2020; Rogers et al., 2018). In this context, our purpose, in this research, was to investigate the effectiveness of an 8-week movement-based intervention on increasing the veridicality between PMC and AMC among Irish adolescents. We hypothesised that adolescents’ enhanced cognitive development would contribute to their improved veridicality.
Method
Study Design and Participants
Data were collected pre- and post-intervention as part of a larger randomized controlled trial (RCT) with Irish adolescents focusing on AMC. Ethical approval for this study was granted by the Social Research Ethics Committee at University College Cork. Second-level schools were invited based on the following minimal inclusion criteria: (a) qualified PE teachers on staff; (b) first-year, second-year and third-year classes of adolescents (age 12–16 years old); (c) participants taught PE for a minimum of 80 consecutive minutes each week; and (d) all schools had access to a gymnasium hall. One class from years 1 to 3 across each school was randomly selected by the school principal and PE teacher(s) for participation. Schools were pair matched (Belton et al., 2019) prior to data collection on the following criteria: socioeconomic status (disadvantaged; non-disadvantaged); gender (single-sex boys; single-sex girls, mixed gender); facilities (PE hall and outdoor pitches) and school size (small: 0–299 students, medium: 300–599 students, and large: 600+ students).
This process resulted in three school pairs equally matched, two large single-sex boys non-disadvantaged schools, two medium single-sex girls non-disadvantaged schools, and two small mixed-gender disadvantaged schools across Cork city, in the province of Munster in Ireland. A randomization process was conducted following participation agreements from the school. From the resulting pairs, one school in each pair was randomly allocated to either the control group or the intervention group prior to pre-test participation using a random number generator (Belton et al., 2019). As other variables were kept constant, any differences in the constant variables between these groups was likely to be caused by the intervention (Hariton & Locascio, 2018).
Subsequent to the approval granted by school principals and teachers, consent forms and information sheets were distributed to each respective class group. Informed parental consent and child assent were required before any adolescents could partake in the study. Both schools and participants were informed that participation was entirely voluntary, and they were free to withdraw of their own volition at any time. In terms of the research rigor inherent to school-based measurements, it is important to note that the principal investigators for this study were qualified second-level school specialist PE teachers, as recognized by the Teaching Council of Ireland.
Consenting second-level school students from years 1 to 3 (age range: 12.23–16.37 years), participated in the project. Across the six schools a total of 488 students were eligible to participate. Final consent and full attendance were provided by 324 participants at pre-intervention testing (females = 45.9%; M age = 14.5, SD = 0.88 years; 66.4% of full sample) and by 243 at post-intervention testing (retention rate of 75%).
Intervention Design
Project FLAME (Fundamental and Functional Literacy for Activity and Movement Efficiency) is a multi-component school-based movement-oriented intervention targeting AMC and functional movement. FLAME is theoretically underpinned by the developmental model of motor competence which proposes that PMC, AMC, and PA are interconnected and work in a spiral fashion to promote positive or negative health outcomes (Stodden et al., 2008). In this theoretical model, improving AMC will develop PMC, and PA and ensure a continuous positive spiral culminating in the attendees’ healthier weight status and better levels of physical fitness. More veridical perceptions of motor competence may also emerge when targeting AMC, as may the association between improved veridicality and sustained PA (Stodden et al., 2008; Utesch et al., 2018). The Project FLAME intervention consists of four critical components designed to develop AMC and improve veridicality (see Figure 1): (a) Teacher component, (b) Student component, (c) Whole-School component and (d) Digital component.
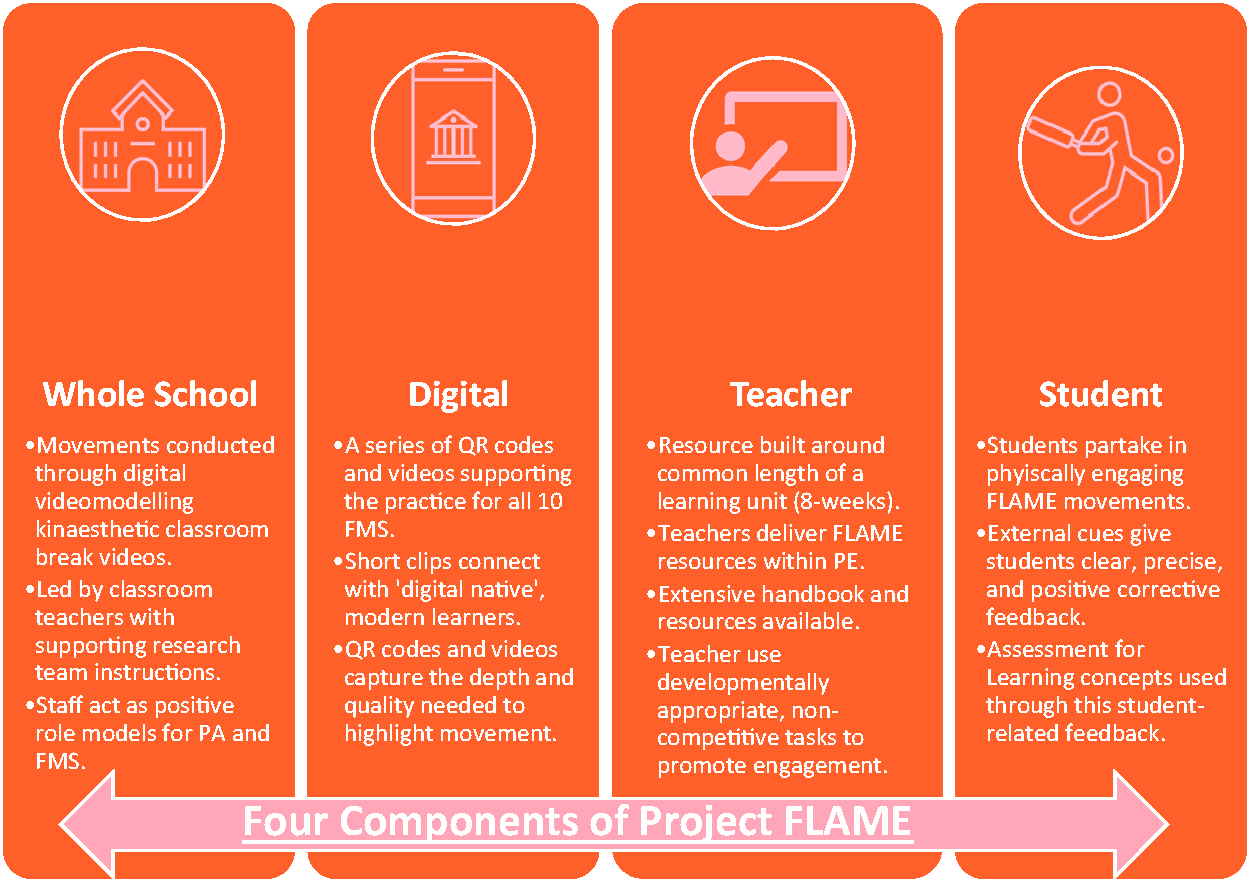
Four Components of Project FLAME: Whole-school, Digital, Teacher, and Student.
Teacher Component
Prior to the intervention, specialist PE teachers received a total of four hours of professional development from the research team in how to deliver the intervention within the PE class. This training involved a comprehensive overview on how to utilize the Project FLAME intervention handbook in-class. The handbook contained comprehensive details on how to use the resources, an activity planner section, and details of how each movement aligns to the PE curriculum. Critically, this training provided regular support (mid-intervention meetings, in addition to WhatsApp messaging threads and email conversations with all intervention schools) for PE teachers during the intervention process. The training sessions aimed to find the correct balance between consuming too much of the teachers’ time and providing sufficient detail for teachers to lead the intervention and utilize the handbook materials confidently.
FLAME activities were designed for 20-minute sections to permit seamless integration into standard 80-minute PE lessons. The research team recommended that activities be incorporated at the start of lessons, but teachers could integrate them as they saw fit. As FLAME was devised by practicing PE teachers (research team), there was high importance given to creating a practical and sustainable intervention to implement in PE without extensive oversight from the researchers. The 8-week intervention duration was selected to make the project feasible for teachers to operate as a learning unit. This rationale is supported in systematic reviews which deemed the ecological validity and sustainability of interventions in schools without researcher support to be a key consideration of AMC and PA-related school projects (Lai et al., 2014; Ma et al., 2021).
Student Component
Students serve as active components of Project FLAME through their participation in its activities and games, while student-centred pedagogical tools are also employed to assist learning and development. The FLAME element of external cues is a novel and effective way of developing skills in young children and athletes (Abdollahipour et al., 2017; Pascua et al., 2015). External cues were provided for each of the movements assessed in the project. An external cue focuses less on the inner mechanics of a movement (i.e., Knee flexed at 90 degrees), and relates instead to the effect (i.e., ‘act like you are balancing a cup of tea on your knee, try not to spill it!’) or the outcome of the movement (Wulf, 2013). External learning cues have been shown to be effective for developing numerous motor skills, including throwing, underarm rolling, sprinting, jumping, and balancing (Abdollahipour et al., 2017; Pascua et al., 2015; Wulf, 2013). This external emphasis also recalls elements of Assessment for Learning (AfL), as it allows teachers to provide students with simple, positive, constructive feedback on how to improve their AMC with such assessment critical to second-level Irish curricula and modern PE classes (Black & Wiliam, 2010; Department of Education and Skills, 2015; Tolgfors, 2018).
Students’ improved AMC and increased knowledge of their own movement ability achieved through providing informed feedback was expected to improve veridicality. Increased knowledge and understanding of a topic has been linked to improved levels of actual ability and greater ability to engage in self-evaluation in many diverse fields (Dunning & Helzer, 2014; Kruger & Dunning, 1999).
Whole-School Component
A whole-school interdisciplinary approach to learning is deemed best practice in current Irish second-level education (MacPhail et al., 2018). In keeping with this theme in this study, teachers and principals were encouraged to collaborate and connect with PE colleagues to foster positive attitudes towards PA and motor competence development through a series of ‘kinaesthetic classroom’ videos that utilized digital video modelling by members of the research team to promote AMC. General classroom teachers could use these videos, of the research team partaking in different activities, in any classroom setting to provide support and encourage students to participate in motor skill related activities and improve their skills. This video modelling concept has previously demonstrated success in boosting AMC with younger children (Bulca et al., 2020).
Digital Component
The electronic/hardcopy handbook contained 50 videos and activities across all 10 AMC skills assessed by the project with unique QR codes (i.e. Quick Response codes, serving as weblinks to activities and games) and visual external learning cues for each movement. The QR codes were situated alongside activity diagrams in the handbook, providing practical examples of activity development tasks and games. QR codes provided PE teachers with immediate access to the suite of skill development tasks and games through a smartphone or tablet tha
Data Collection Methods
Prior to data collection, all undergraduate, pre-service or graduate PE teachers underwent 3-hour field researcher training on the AMC and PMC measurement protocol. This training involved an objective, criteria-informed process to ensure that field staff were consistent in administering the measurements. On data collection days in various schools, research assistants demonstrated their ability to comply with the AMC and PMC protocols to the principal investigators prior to the arrival of study participants. Additionally, field staff were given a descriptive research handbook detailing the protocols associated with all data collection phases. Pre- and post-intervention test data were collected with participants in their respective class groups (maximum n = 27). All measurements (AMC, self-report PMC questionnaires) were completed during a typical PE class (duration range 80 minutes).
Measures
For the AMC measurements, Apple iPads on a fixed stanchion recorded each participant’s execution of the requisite skill. Camera positioning and angles were kept consistent at all times to ensure capture of total body movement (O’Brien et al., 2016). Pre-testing (i.e., baseline data before the intervention) commenced in Jan/Feb 2019, and post-intervention data collection occurred in May 2019. Between January and May, students in the control schools continued with their regular PE lessons, independent of Project FLAME, while students in the intervention schools participated in PE lessons with a Project FLAME focus on the three active FLAME components (digital, teacher, and student) within a whole-school context with the kinaesthetic classroom.
Actual Motor Competence (AMC)
AMC is a frequently cited global or umbrella term that reflects a variety of previously published terms in relation to human movement (Robinson et al., 2015), including fundamental movement skills (FMS) (Logan et al., 2018). Ten FMS, the “building blocks” of sporting engagement and lifelong PA (Logan et al., 2018), were assessed in this study in three separate categories: locomotor (i.e., vertical jump, horizontal jump, run, skip, maximum score = 34), object control (i.e., catch, kick, two-handed strike, overhand throw and stationary dribble maximum score = 40) and stability (
The Test of Gross Motor Development (TGMD) (Ulrich, 1985), TGMD-2 (Ulrich, 2000) and the Victorian Fundamental Motor Skills Manual (Victoria Department of Education, 1996) were used to assess these FMS. Moderate to excellent construct validity and reliability has been established for the TGMD-2 with children (Barnett et al., 2014; Cools et al., 2009; Rey et al., 2020). Though not commonly used with adolescents, subsequent validity work for the TGMD-2 has deemed its usage with adolescents acceptable with good-to-excellent reliability values, and a good fit following confirmatory factor analysis reported in a previous study (Issartel et al., 2017). The Victorian FMS manual has also shown acceptable reliability and validity among both childhood and early adolescent groups, with this tool deemed a ‘benchmark’ assessment for Australian adolescents (Lander, Morgan, Salmon, Logan, et al., 2017; Victoria Department of Education, 1996). At the beginning of each data collection session, participants were informed about the FMS testing procedures (i.e., the first performance being practice and the second and third trials being recorded). Field researchers first demonstrated accurate skill technique once for participants to observe. No feedback was given during or after performances of any skill. Th
Perceived Motor Competence (PMC)
The McGrane et al. (2016) Physical Self-Confidence Scale is the first valid and reliable instrument for assessing adolescents’ physical self-confidence at a skill-specific FMS proficiency level. This Likert scale measurement tool has shown excellent test-retest reliability (r = 0.92) and possesses good content and concurrent validity (r = 0.72) (McGrane et al., 2016) when compared to the Physical Self-perception Profile (Fox, 1990). The Physical Self-Confidence Scale (McGrane et al., 2016) was modified in this study to measure participants’ PMC for their FMS proficiency by altering the question stem from “how confident are you at performing” to “indicate how well you can perform ____ (e.g., kick).” In this modification, we followed expert advice and recent research regarding the alignment of test batteries (De Meester et al., 2020; Estevan & Barnett, 2018). Referring to competence ensured better alignment with past research in PMC and reduces a problem within PMC research of “definitional blurring” that occurs when unclear alignment between measurement tools and constructs leads to incorrect data interpretation assumptions (Shearer et al., 2018).
Within this PMC scale, participants were asked to rate their competence at performing the 10 FMS, based on a 1-10 Likert scale in which “1” indicated being not competent at all and “10” indicated being very competent. Participants completed the PMC questionnaire item by item separately and independently from other participants after they performed each FMS test. They returned to the group after completing the relevant question. The 10 FMS selected for AMC and PMC testing were selected due to their critical role in Irish sporting and PE cultures (O’Brien et al., 2016). Among participants in the current study, a Cronbach’s alpha coefficient showed good internal consistency for the PMC scale (Cronbach alpha coefficient of 0.84 overall, 0.73 for the object control subscale, and 0.80 for the locomotor subscale). The PMC questionnaire participant responses were collected via pen and paper, and later entered into statistical programming software by the research team.
Data Processing and Analysis
Prior to the FMS data scoring, we established inter- and intra-rater reliability using 10% of the data set. Two raters (principal investigators) double coded this data subset to determine both their intra- and inter-rater reliability (Logan et al., 2017). They were required to reach at least 95% intra- and inter-rater agreement for all 10 FMS. Each rater then coded half of the full dataset. All data analyses were completed with JASP (JASP Team, 2020), SPSS version 25.0 for Windows, R Software (Version 4.0.2, www.r-project.org) and RStudio Software (Version 1.3.1056, www.rstudio.com), primarily using the package nlme (Pinheiro et al., 2021) and tidyverse (Wickham et al., 2019). We set the statistical significance level at p < .05.
We calculated descriptive statistics for FMS at both the individual skill and composite score levels. These data were normalized on a 0–1 scoring basis and are presented in the tables below such that a score of 1 reflected a maximum score of 84 (i.e., all 10 FMS skills mastered – meeting all performance criteria – across two trials), All PMC data is presented in terms of its raw overall value with a minimum score of 10 and a maximum score of 100 across the ten movements. We calculated any differences between the control and intervention participants groups at pre-intervention using Bayesian independent t-tests with a Cauchy prior. Bayes Factors (01) for the test of equality (i.e., no difference) indicate the ratio of the probability of no difference between control and intervention group. We determined the strength of the analyzed relationships (i.e. small, moderate, large) using the Cohen’s (1988) guidelines in which a standardized beta coefficient of β = 0.10 – 0.29 denoted a small correlation, β = .30–0.49 denoted a moderate correlation, and β ≥ 0.50 denoted a strong correlation, respectively (Cohen, 1988). To analyse the effect of the main hypothesis of improved veridicality, we calculated multilevel regression models with time observations on level 1 that were nested in persons on level 2. We conducted complete cases analysis in order to examine whether between-group effects differed from the intention to treat data analysis. PMC was the dependent variable, while individual variation of children’s level of PMC was allowed by adding a random intercept to the model. Different models were calculated in order to analyze the veridicality effect. First (model 1), only AMC was added to the model predicting PMC in order to analyze the strength and the direction of the association between PMC and AMC scores. Second (model 2), age and sex were added in order to control for these variables. In model 3, the treatment (intervention) interaction term with AMC was added. In model 4, we added the interaction of AMC, the treatment and time (pre-post).
Results
Overall, 486 children (48.5% female; M age = 14.50, SD = 0.88 years) from six schools participated in at least one AMC or PMC test at pre- or post-intervention. Table 1 shows their demographic and pre-test characteristics by intervention or control group membership. Descriptive statistics for participants’ primary outcome measures by group at pre- and post-intervention can be found in Table 2. There was no significant difference at pre-test between intervention and control groups on either AMC (Bayes Factor = 7.6:1 probability of no difference) or PMC (Bayes Factor = 5.58:1 probability of no difference).
Demographic and Pre-Test Participant Characteristics in Intervention and Control Groups.
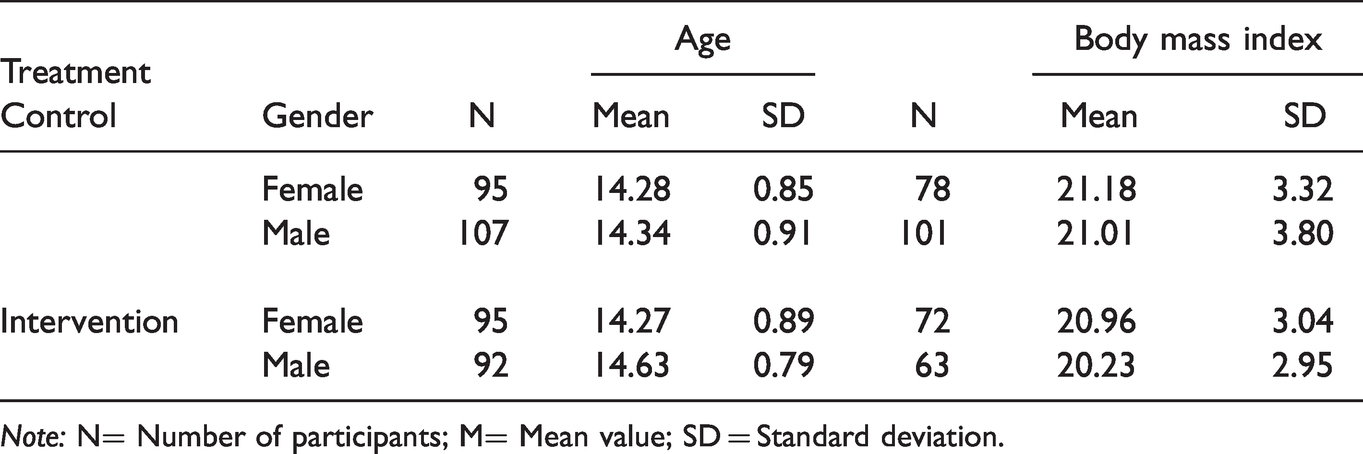
Note: N= Number of participants; M= Mean value; SD = Standard deviation.
Mean Actual and Perceived Motor Competence Scores at Pre- and Post-Testing for Male and Female Participants.
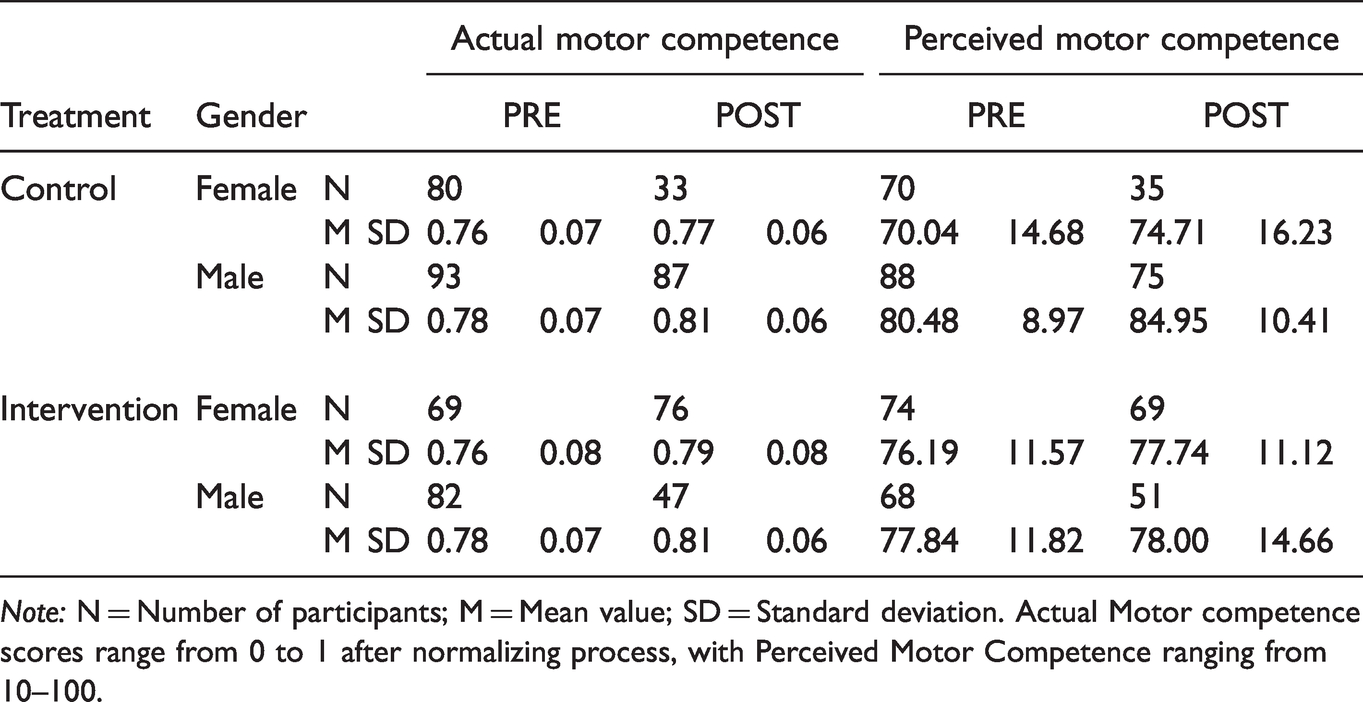
Note: N = Number of participants; M = Mean value; SD = Standard deviation. Actual Motor competence scores range from 0 to 1 after normalizing process, with Perceived Motor Competence ranging from 10–100.
The hypothesis of improved veridicality from the intervention was analyzed using multilevel models. Table 3 shows summaries of the modelling process. Initial veridicality data in model 1 (i.e., just AMC and PMC veridicality) indicated a significant small correlation between these variables at post-intervention (β = .24, p < .001). After controlling for age and sex in model 2, a significant and robust small effect (β = .23, p < .001) was still evident. However, model 3 revealed no significant intervention effect on the veridicality between AMC and PMC. Similarly, in model 4, there was no significant intervention*time effect. However, general veridicality was still shown by a small effect in all four models. Neither the intervention nor the 8-week time period between pre- and post-testing were associated with a greater relationship between PMC and AMC scores. As a further result, across all models, age showed no significant effect on PMC, but there was a gender effect on PMC (β = .53, p < .001).
Results of the Four Multilevel Regression Models.
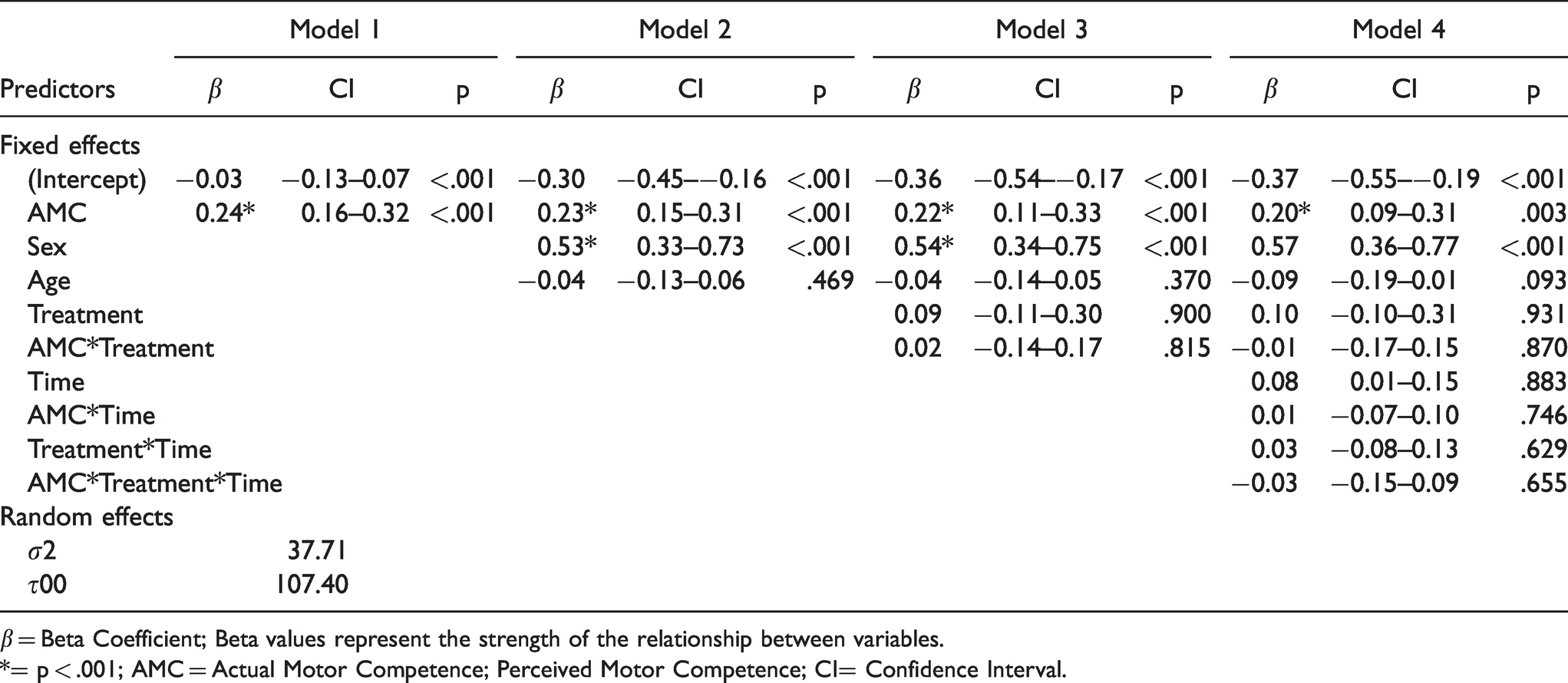
β = Beta Coefficient; Beta values represent the strength of the relationship between variables.
*= p < .001; AMC = Actual Motor Competence; Perceived Motor Competence; CI= Confidence Interval.
Discussion
The purpose of this study was to examine pre- and post-intervention veridicality between adolescents’ PMC and AMC with the hypothesis that a movement-based intervention would improve it. To the author’s knowledge this was the first study to focus on AMC and PMC alignment in an Irish context, and it must be noted that this randomized controlled trial highlighted a lack of AMC proficiency despite high levels of PMC among Irish adolescents. With regard to our main hypothesis, we found no significant intervention effect for improving the veridicality of the AMC/PMC relationship.
At pre-test, there was no difference between the intervention and control groups on either PMC or AMC. The veridicality between AMC and PMC in our large adolescent sample was small but statistically significant at post-intervention. While the observed value was low, correlations in the small to moderate range are commonly found within adolescent research samples (De Meester et al., 2016; Rogers et al., 2018). A previous study among Belgian adolescents, (n = 215; 66.0% boys; M age = 13.64, SD = .58 years) reported a moderate correlation, while a comparable Australian study (n = 173 M = 12.48, SD = .34 years) similarly reported a small correlation between FMS and PMC (De Meester et al., 2016; Rogers et al., 2018). The intervention did not lead to statistically significant improved veridicality between PMC and AMC, possibly because 8-weeks was too short a period for this intervention to effect veridicality by invoking requisite changes in participants’ skills and perceptions. While short-duration interventions (i.e., 6-weeks) have previously successfully developed both PMC levels (and more general physical self-perceptions) and AMC levels (as separate constructs), it would appear that greater time is needed to improve their mutual alignment (Bryant et al., 2016; Burgess et al., 2006).
Prior interventions examining improvements and/or alignments in perceptions have typically lasted between 10–12 weeks (Lander et al., 2019; Schmidt et al., 2013b).While intervention tasks in this study prioritized engagement in PA and AMC, further intervention refinement may be necessary to include more fun and social interaction which might precipitate greater autonomy, and self-reflection. Such tools have proven effective in previous AMC and PMC-related interventions among adolescent youth (Morgan et al., 2012). A change in pedagogical methods might also be necessary in order to invoke the realistic self-perceptions that are essential to longer-term sport and PA participation (Lander et al., 2019; Schmidt et al., 2013b).
Given the minimal influence of age on veridicality of PMC and AMC among participants in this and previous studies, it seems possible that self-perceived motor competence (though remaining high) stabilizes developmentally when approaching adolescence (Philpott et al., 2020; Van Veen et al., 2020). More data from adolescent samples is required to examine whether AMC/PMC alignment improves during this juncture, though a recent meta-analysis reported no significant effect of age on this relationship or on other measures of physical self-perception (De Meester et al., 2020). It seems possible that young people reach a ‘plateau’ of self-perception, whereby perception values remain consistently high and are hard to change during the adolescent period (Philpott et al., 2020; Rogers et al., 2018).
As PMC levels have been consistently high and alignment between PMC and AMC across studies has remained in the small to moderate range, it seems to remain essential to target improvements in AMC with intervention programs (De Meester et al., 2020). Studies that have examined AMC/PMC alignment following intervention are limited in number. However, an AMC focus with strong student-centered learning methods successfully improved the relationship between measures of strength and physical self-perceptions among Swiss adolescents (n = 246; M age = 11, SD = .56 years) through a teaching method known as the individualized teacher frame of reference (Schmidt et al., 2013b). This pedagogical style included positive feedback, student journaling, self-reflection, and self-directed learning for muscular strength and endurance work (Schmidt et al., 2013b). The intervention had a significant effect in improving veridicality between physical self-concept and actual strength among both over-estimators and under-estimators from baseline to post-test (Schmidt et al., 2013b). It would appear that improved ability combined with greater participant understanding and learning, developed through more student-centered approaches, could be key to improving AMC/PMC veridicality (Lander et al., 2019; Schmidt et al., 2013b).
A gender effect for PMC (see Table 3), with males recording higher values than females was found, and greater AMC/PMC veridicality was reported among males in comparison to females. It has been common in past studies too for males to report higher PMC, with such findings reported in Chinese, Finnish, and cross-cultural (i.e., German-Australian) studies (Chan et al., 2018; Niemistö et al., 2019; Tietjens et al., 2020). Reasons for disparate gender perceptions are believed to be primarily sociological (Tietjens et al., 2020). Female PA is often less prioritized or promoted by society than male PA, resulting in lower social support (from peers or family), encouragement, and opportunities for girls to be active, to develop competence, and to experience positive feelings that might spur sport participation (O’Brien et al., 2021). Differing social priorities often mean that females bond and socialize in non-sporting or physically active settings, when compared to males, for whom sport settings appear pivotal in the formation and identification of peer relationships (Timler et al., 2019). These influences on female perceptions may account for females feeling more marginalized and less capable of performing motor skills (Horn, 2018).
High levels of PMC and other forms of physical self-perception are common among adolescents (Lander et al., 2019; O’Brien et al., 2018), and this pattern was found in this study, with mean PMC values across pre- and post-intervention measures among both males and females above 70 (on a scale with a maximum score of 100). While participants’ PMC values were exceptionally high, no participant in our sample at pre- or post-intervention testing actually mastered all 10 of our measured FMS even though separate research showed these capacities to be evident from the age of six (Gallahue et al., 2019). Low AMC and high PMC findings from this and other studies suggest that overestimation of AMC (i.e. high levels of perception, not matched by actual skill ability) is an important contributor to the lack of AMC/PMC veridicality (O’Brien et al., 2018; Philpott et al., 2020). High levels of perception are quite common across the globe, with this ‘overestimation’ issue reported among childhood and adolescent studies across different measures of perception in regions such as Norway, Australia, and Spain (Estevan, Bardid et al., 2021; Lander et al., 2019; Vedul-Kjelsås et al., 2012).
High PMC values can be beneficial and have been associated with greater inclinations for PA, participation in PE, and higher levels of well-being (De Meester et al., 2020; Estevan, Bardid et al., 2021; Visser et al., 2020). The sensitive adolescent period, fraught with personal, social, and biological changes, may account for this tendency to overestimate personal motor competence as adolescents seek to preserve a confident image in front of peers (Estevan, Menescardi et al., 2021).Promoting veridical alignment with high levels of PMC and high AMC would appear to be critical. High levels of PMC unsupported by actual competence can have negative consequences in that this non-veridicality has been associated with lower levels of PA (Utesch et al., 2018).
Examining future trends and directions in the area of PMC and veridicality, it seems probable that developing a greater understanding and knowledge about movement and skills may be inherent to more aligned perceptions (Lander et al., 2019). Improved accuracy in alignment has long been theorized to be a pivotal component of improved motivation towards PA (Harter, 1982; Stodden et al., 2008). To develop more realistic perceptions, knowledge and understanding would appear to be critical as informed by the Dunning-Kruger Effect (DKE). The DKE suggests that those lacking competence are often unaware of their ability level or falsely assume they possess greater ability than their actual capacity (Kruger & Dunning, 1999). While not yet researched within the AMC/PMC field, it is possible that the DKE is influencing findings of high PMC and low AMC. Study participants with low levels of AMC may be unable to accurately quantify and understand what constitutes a high movement ability, leading them to overrate their actual skills. Thus, improving participants’ movement awareness, knowledge and understanding may be an alternate route toward improved AMC/PMC veridicality, and a basis for further refinements within the Project FLAME intervention (Lander et al., 2019; Philpott et al., 2020).
Limitations and Directions for Further Research
A limitation of this study is that all participants were selected from a single county in the south of Ireland in an urban setting making them potentially unrepresentative of Irish adolescents (and adolescents in other countries) from rural backgrounds. Secondly, we did not monitor the fidelity of the FLAME intervention in the schools during the practice sessions because we sought to mimic an authentic school environment. Though we did use a follow-up questionnaire completed by teachers, possible insufficient adherence to our intervention protocol is a limitation that should be corrected in future research. Additionally, PMC self-report data in this study and in others may have been susceptible to a positive response bias that was not managed through instrument validity scales. Future investigators might utilize social desirability scales to help determine the influence of this variable. This study indicates that longer duration interventions are required to positively impact veridicality among adolescent youths. The implications for future research include the need to increase intervention length, provide greater autonomy and responsibility to students to improve their engagement, and motivation in intervention participation. Finally, the cross-sectional nature of this research limits the ability to make inferences regarding causal relationships between the variables of interest. To gain greater insight into the relationship between PMC and intervention-manipulated AMC, longitudinal research designs would be ideal.
Conclusion
We documented in this study that Irish adolescents, like those from other countries, tend to exhibit low levels of AMC and high levels of PMC. We hypothesized that overestimation of motor competence relative to actual motor competence, rife among adolescents, might be ameliorated with a targeted PE intervention in Project FLAME. We were unable to affect a significant improved veridicality between PMC and AMC values through this intervention, possibly because of its length. We thoroughly discuss here the possibility of developmental stabilization of high PMC during adolescence, possible bases for gender differences in AMC/PMC, the possible role of a distorted awareness and understanding of personal movement skills among adolescents that might be an alternate or adjunct intervention target for future investigators, and several specific limitations of this study.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Partial funding of this project was awarded by Sport Ireland under the Dormant Accounts Fund. The funding bodies had no input on study design, analysis, or the writing of this paper.