
Abstract
This study is an exploration on potential gender differences in sibling grief over perinatal loss. 30 adult siblings’ recollections were analysed to identify possible differences along the instrumental-intuitive continuum. A statistical analysis (ANOVA) on word frequencies indicated that the intensity of the emotional experiences did not differ between men and women, as there were not any significant differences in the function words reflecting such contents. Women referred to third persons, the delivery process, and the act of naming their deceased siblings more frequently. A subsequent qualitative context analysis revealed that these third persons were mainly family members and hospital staff. Men were more specific in their recollections, mentioning exact names and other types of data related to the loss while women focused more on the emotional significance of the experience. Our results may contribute to the development of personalized interventions for families struggling with disenfranchised grief.
Introduction
Bereaved siblings are often identified as forgotten mourners in the professional literature. Relatives and friends attempt to isolate them from the traumatizing event; and most professionals focus on parental grief when a perinatal loss occurs (Davidson, 2018; Funk et al., 2018; Kempson & Murdock, 2010). The (usually benevolent) endeavours to protect the children from the traumatic experience by not relating the loss have an adverse impact as complicated grief may occur, threatening bereaved siblings’ physical and psychological wellbeing (Boelen et al., 2020; Doka, 1999; Fernández-Alcántara et al., 2021; Kersting & Wagner, 2012). Symptoms may include impairments in daily functioning, isolation, identity disruption, sensing life as meaningless, and emotional problems that persist over the years (Boelen et al., 2020; Prigerson et al., 2021). Precipitating factors for complicated grief include the lack of adequate social supports and appropriate cultural practices, such as death and mourning rituals. If the loss is unexpected and information is not available concerning the loss, or the deceased person is a child, then these become further triggers for complicated grief/Prolonged Grief Disorder (PGD), a diagnosis that has been included in the text revision of Diagnostic and Statistical Manual of Mental Disorders (DSM-5-TR 2022) (Boelen & Lenferink, 2022; Neimeyer et al., 2014; Pilling, 2003; Shear et al., 2013; Simon, 2013; Smith & Ehlers, 2020). Responding to mourners’ specific needs and validation of their experiences may promote post-traumatic growth in several dimensions, including one’s self-perception, positive changes in personal relationships, spiritual orientation, and an overall appreciation of life (Johnsen & Afgun, 2021).
This study addresses the potential differences between male and female mourners and aims to identify the unique needs of siblings who experience perinatal loss in the family. Such differences are often captured in a contrast between an intuitive, emotive, help-seeking mode and an instrumental, cognitive style focused more on problem solving. Recently, these variations have been reinterpreted as endpoints of a continuum rather than a rigid dichotomy and factors other than gender have been introduced (Doka & Martin, 2010; Versalle & McDowell, 2005). Stelzer and associates (2019) have noted that the linguistic markers of gender differences in bereavement have not been studied extensively so far. In this paper, we examine bereaved siblings’ recollections about perinatal loss. Are the above differences reflected in their present-day narrative recollections, and if yes, how?
Background
Perinatal loss is the death of an infant due to miscarriage, stillbirth, or neonatal death (Fenstermacher & Hupcey, 2013; Kersting & Wagner, 2012). In Hungary, involuntary abortion and foetal loss equals to approximately 15,000 cases per year, and about 400 of these losses occur in late pregnancy or shortly after birth (Központi Statisztikai Hivatal, 2022). The domestic definition excludes miscarriage (foetal death before the 24th week of pregnancy) and defines a relatively short interval, 168 hours for neonatal death (SZNSZK-OGYEI, 2010). In this study, authors adhered to the domestic definition of perinatal loss.
Classical theories of grief as an emotional reaction to the loss focussed on bereaved persons’ detachment from the lost person. In the light of a new conception, bereavement theory, it is a unique intersubjective process that is about sustaining connectedness to the lost person and the reconstruction of the bereaved person’s identity: “individuals can maintain a healthy connection to the deceased and in fact even find the bereavement experience transformational” (Fenstermacher & Hupcey, 2013, p. 9). This conception of continuing bonds (CB) focuses more on the unique reconstruction processes than the phases of grieving (Budak, 2015).
Perinatal loss has not been acknowledged as a meaningful loss before the 1970s. The change in researchers’ and practitioners’ perspectives was substantiated by (1) elaborations on attachment theory, explaining maternal bonding during pregnancy, (2) an increased social sensitivity to bereaved mothers’ sufferings, and (3) improvements in neonatal care (Fenstermacher & Hupcey, 2013; Horey et al., 2021). These changes occurred much later in Hungary, a closed society before the transition of the social system in 1989. Constructive, humane guidelines concerning bereavement care after perinatal loss were introduced only in 2010 (SZNSZK-OGYEI, 2010). This document, however, mentions the surviving siblings only once and assumes that siblings’ problems are always a result of their mothers’ anxiety, depression, and grief. The mother’s complicated grief is indeed an important factor, as adult family members’ complicated grief is a potential source of mental problems for the child (Erlandsson et al., 2010). However, siblings do not experience grief only as mediated by their mother. They have their own stories, sorrows, worries and reliefs, and they also encounter very diverse reactions on part of the family and their personal social network. Siblings may experience guilt over the loss in their attempts to control the uncontrollable (Simon, 2013). For them, grief is often a “loss of innocence” (Funk et al., 2018, p. 13), affecting their family roles, future visions, and overall childhood experiences. Their grief may isolate them from their friends and acquaintances (Clarke et al., 2012; O’Leary & Gaziano, 2011).
Siblings inevitably suffer a double loss: they do not only lose their deceased baby brother or sister but also their parents as they knew them before. In their study on various groups of bereaving persons, Smith & Ehlers (2020) concluded that bereaved parents are “a particularly vulnerable group” (p. 11). Perinatal loss is often a life-transforming experience for the entire family (Clarke et al., 2012; Hughes et al., 2001; Leon, 2001; O’Leary & Gaziano, 2011; Rostila et al., 2016). In their review article on perinatal bereavement, Fenstermacher and Hupcey (2013) conclude that the process has not a definite endpoint, it may even last a lifetime and extend to future pregnancies.
Sibling grief over perinatal loss is a prototypical event of disenfranchised grief, “a loss that is not, or cannot be, openly acknowledged, publicly mourned or socially supported” (Doka, 1999, p. 37; Zampitella, 2011). Parents’ and grandparents’ silent stories, though these are meant to be protective acts, will have a destructive impact on the lives of the next generations (Cassidy, 2021; Koltai, 2007; Mortell, 2015; Rober, 2002).
A common consequence is the replacement or vulnerable child syndrome. Parents with unresolved grief may expect their next child to “substitute” the deceased child by giving up their own identity. This is a parental expectation that can never be met. The vulnerable child syndrome is the result of an overprotective parental attitude that becomes a source of separation and individualization difficulties for the child (Lamb, 2002). Budak (2015), however, has suggested a reconsideration of the syndrome in the light of the new bereavement theory. Individual variations e.g., “gift child” versus “inadequate replacement” or internal versus external CB, significantly influence recovery processes (Budak, 2015). Parentification, on the other hand, is a reversal of roles: parentified children assume responsibilities for the grieving parents’ wellbeing, or, if the parents are unable to care about the other siblings, for the surviving siblings. Instrumental (task-focussed) and emotional parentification often have a destructive impact on the children’s future lives, including low self-esteem, inter- and intragenerational problems, low academic achievement, and severe psychopathology. Positive outcomes are also possible, such as the development of problem solving and coping skills and an improved mental health status. The intergenerational transmission of parentification as a family pattern may also occur (Cassidy, 2021; Hooper, 2011).
In a previous explorative study using Interpretative Phenomenological Analysis (IPA) (Bornemisza et al., 2021) authors have identified similar themes in adult siblings’ narratives, such as post-traumatic growth, spiritual orientation, the significance of ritual elements, the strong wish to identify the deceased sibling as a family member and a person (either by constructed or CBs); silenced stories, destructive communication patterns within the family and outside the family, the enmeshment of parental grief and own grief, parentification, iatrogenesis, and fears from a similar experience in one’s own life.
Gender Differences
An important source of gender differences is that the mother has a very strong physical relationship to the infant who is literally part of her body. For them, this a CB in the bereavement process whereas both the father and the siblings must first construct the bond in the cases of involuntary abortion or stillbirth (Cassidy, 2021; Meyer, 2015).
There are general communication differences between women and men (Tannen, 1990), as well as specific differences in social relationship maintenance patterns focusing more on social contacts (females) or on joint activities (males) (Roberts & Dunbar, 2015). Sensitivity to stressful and emotionally valent contents is also different (Rahmi et al., 2018). In sum, men use language more instrumentally, highlighting its representative function. Women are characterized by a more relational language use and express their emotions more openly through language (Stelzer et al., 2019). These differences may present themselves along the instrumental-intuitive continuum in grief experiences (Martin & Doka, 2000; Versalle & McDowell, 2005). The main phases and symptoms of grief are similar in the two genders: a recent study (Lundorff et al., 2020) could identify differences in early symptom development only among highly stressed individuals, 6.8% of the entire sample. In this study, men were characterised by an acute and decreasing reaction while women “showed an adjourned, mounting grief reaction” (p. 168.) Similarly, symptom intensity for PGD, characterising 8.4% of the entire sample, was higher among women (Smith & Ehlers, 2019). The surface manifestations of grief (as diagnostic criteria for PGD) are somewhat different in the two genders. Women’s intensive emotions include sadness and guilt, they openly vent their feelings and seek external support to share these feelings. Men’s grief is characterized by anger, aggression, and fears from losing control over the events. They might want to be “strong”, defend the family from external threats and manage the daily life of the family. Their grief experience can be covered by these surface phenomena that the wife may interpret as emotional coldness. Therefore, both parents might become isolated in their grief experience (Kersting, 2005; Leon, 2001; McCreight, 2004; Oikonen & Brownlee, 2002; O’Leary & Thorwick, 2006; Turton et al., 2006).
Though risks for post-traumatic stress disorder (PTSD) and PGD are higher among women mourners, their deliberative rumination as a sustained focus and contemplation on emotional contents (in contrast with unproductive and harmful brooding contemplation) is a precipitating factor for post-traumatic growth (Johnsen & Afgun, 2021; Lundorff et al., 2020).
Gender differences in the verbal markers of disintegrated experiences
Recurrent studies have confirmed that certain verbal contents are indicative of speakers’ emotional state, further, their psychopathology or recovery from a mental disorder (Ehmann, 2002; Kézdi, 1995; László et al., 2013; Pennebaker & Seagal, 1999; Priest, 2020; Stelzer et al., 2019; Stephenson et al., 1997; Weintraub, 1981; Wiener & Mehrabian, 1968). In linguistics, “content words with specific meanings and function words orienting the speakers in spatial, temporal and relational dimensions related to the contents were traditionally differentiated” (Moeschler, 2016, p. 175). Moeschler (2016) has proposed the term procedural meaning for function words, “guiding the processing of conceptual information.” The use of such contents is not pre-planned, their processing takes little time and speakers can hardly recall them when remembering the contents of a text (Chung & Pennebaker, 2007). Procedural contents as negation, first person singular pronoun use, and distancing/generalizations were related to suicide threat/crisis experiences, loss of control, or an overall negative emotionality (Chung & Pennebaker, 2007; Kézdi, 1995; Stelzer et al., 2019; Wiener & Mehrabian, 1968). LIWC, a valid instrument comprises such contents and can be utilized for comparative studies using English language texts (Pennebaker & Seagal, 1999; Pennebaker et al., 2015; Stelzer et al., 2019). In a study by Steltzer and associates (2019) certain linguistic correlates of grief narratives were analysed by using LIWC. Authors’ overall results have confirmed the gender similarity hypothesis (there are no salient differences in grief), except for self-referent contents that occurred more frequently in women’s narratives.
Research Questions
1. Do trauma-related procedural contents indicating the intensity of the emotional experience differ with the two genders? 2. Is women’s more emotional-intuitive and relational focus reflected in their narratives in any ways? 3. Are there any gender differences in the recollections on a childhood trauma in the core conceptual meanings, such as death, birth, references to family members and self-reflective contents? Do these differences mirror the intuitive-instrumental continuum?
Sample
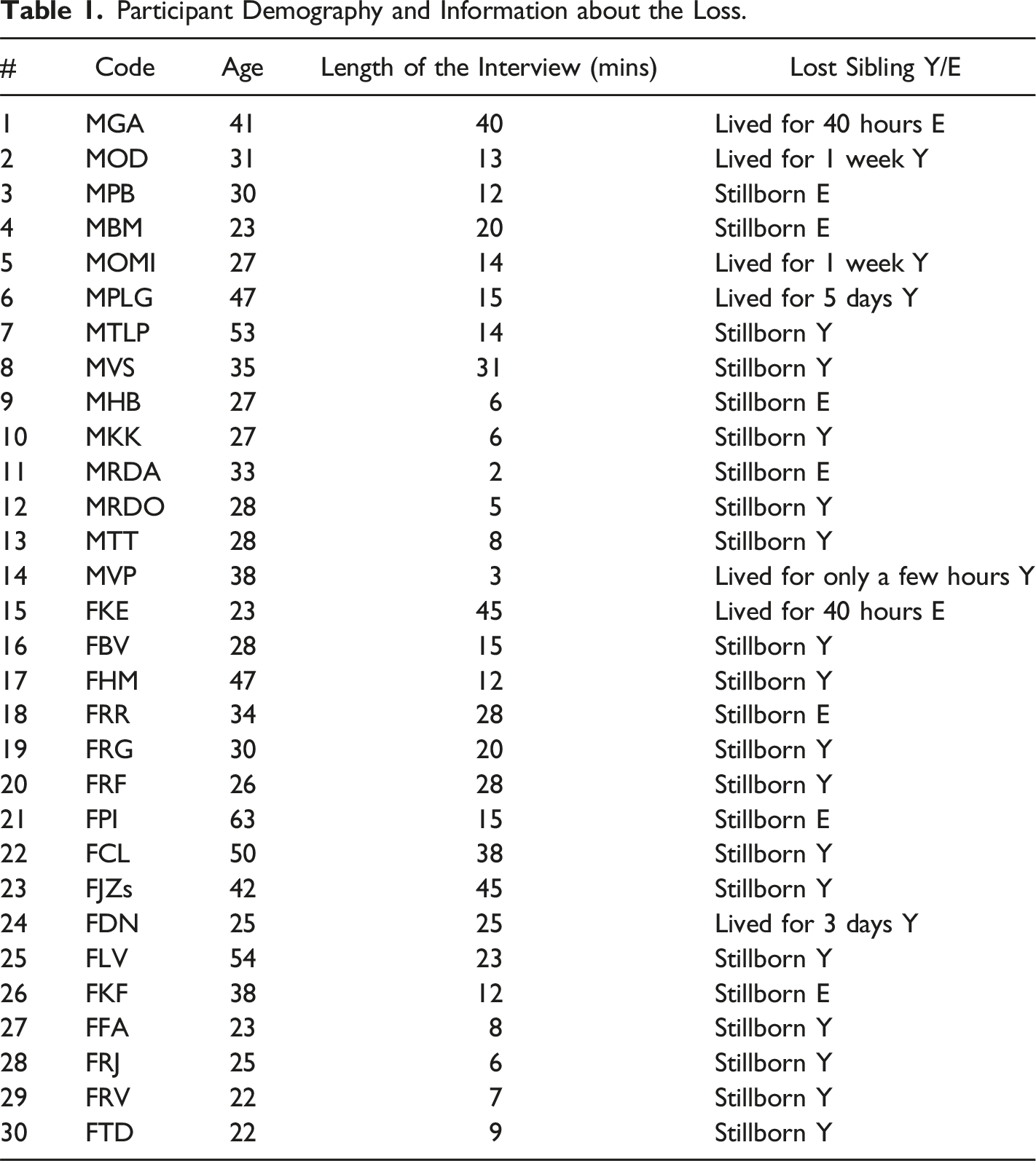
Respondents in this study have experienced the loss of a sibling, or the impact of such a loss in the family prior to their birth. The total sample included 30 participants, 16 women and 14 men, and none of the respondents identified themselves as other. Age range was between 22 and 63 years (M = 34.00; SD = 11.01). Respondents were invited by the first author through her professional network as a childbirth educator. Semi-structured in-depth interviews were conducted in the interviewees’ home. Respondents were told that they are free to withdraw or refuse to answer a given question; and were also informed about anonymity and confidentiality. The language of the interviews was Hungarian. The opening question of the interview was “Please tell me the story of the loss of your sibling” (Funk et al., 2018, p. 2). Further themes comprised parental grief as the respondents experienced it, the impact of the loss on the surviving sibling’s life, intergenerational transmission, and individual and family-level coping with the loss. The interviewees consented to audio recording, to verbatim transcription of their texts, and the publication of the results. Consolidated criteria for reporting qualitative research (COREQ) (Tong et al., 2007) were followed throughout the data collection and analysis except for one suggestion on participant validation. Here we followed Finlay’s (2020) advice and did not show the respondents the transcripts. Trauma-related narratives are even more fragmented than other transcriptions of real-life conversations and respondents are not used to this feature.
Participant Demography and Information about the Loss.
Method
No salient gender differences were identified in our previous IPA study (Bornemisza et al., 2021). In this research we continue with a quantitative analysis incorporating mainly procedural contents (function words) that may reflect the emotional intensity of the experience. ATLAS.ti, a tool enabling qualitative as well as text-specific quantitative analyses was used to explore the differences. We chose this option as LIWC is not available in Hungarian, an agglutinative language. As a first step, a word frequency list was made comprising all the words in the 30 interviews. Words exceeding 0.1% were categorised to build a search bibliography. This list was complemented by search expressions that have proven relevant in the previous IPA study such as words related to birth, name giving, and death. This way 17,146 of a total of 35,646 words (48%) were categorised. The search bibliography and its translation are available in Table A1 in Appendix 1. To analyse potential gender differences, we had to balance the gender ratios, so we used Box Plot descriptive statistics to see if there were any outliers along age, and we were able to filter out two participants from the female group (see Figure 1.). We finally used data from N = 14 females (M
age
= 31.07; SD = 9.58) and N = 14 males (M
age
= 33.43; SD = 8.58) for the most accurate results in the quantitative analysis. Age distribution in the two groups.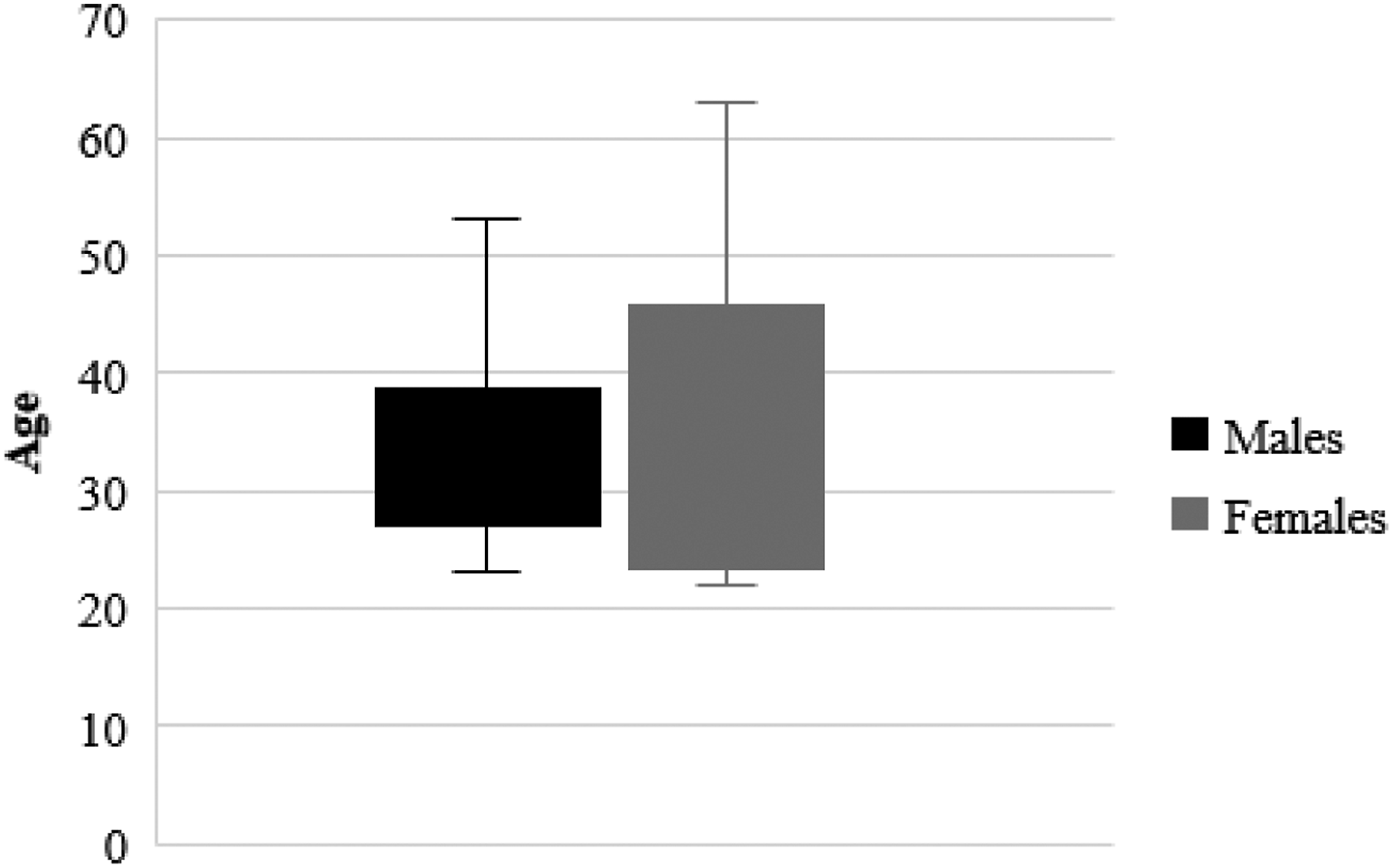
As a next step in this mixed methods study, following a quan-qual sequence (Teddlie & Yu, 2007), we explored the contexts of the conceptual meanings, relying on a traditional method known as keyword-in-context (KWIC) in content analysis (corpus linguistics). Keyword-in-context was performed wherever significant differences had been identified in the statistical analysis to identify the meanings attached to these contents in male and female respondents’ interviews. ATLAS.ti 8.00 was used to assist the qualitative analysis and enhance its reliability. Contexts (sentences) for the key terms were retrieved and then these sentences were further analysed by the authors.
Results
Results of the Quantitative Analysis
IBM SPSS Statistics 26.0 was used, and ANOVA was applied to compare the data from the two groups. For the significant results, Effect size was also computed (partial eta-squared: η 2 = Treatment Sum of Squares/Total Sum of Squares). To interpret the partial eta-squared effect size Cohen’s (1988) guideline was used: small effect up to 0.01, medium effect up to .06, and large effect up to .14.
Gender differences along the codes.
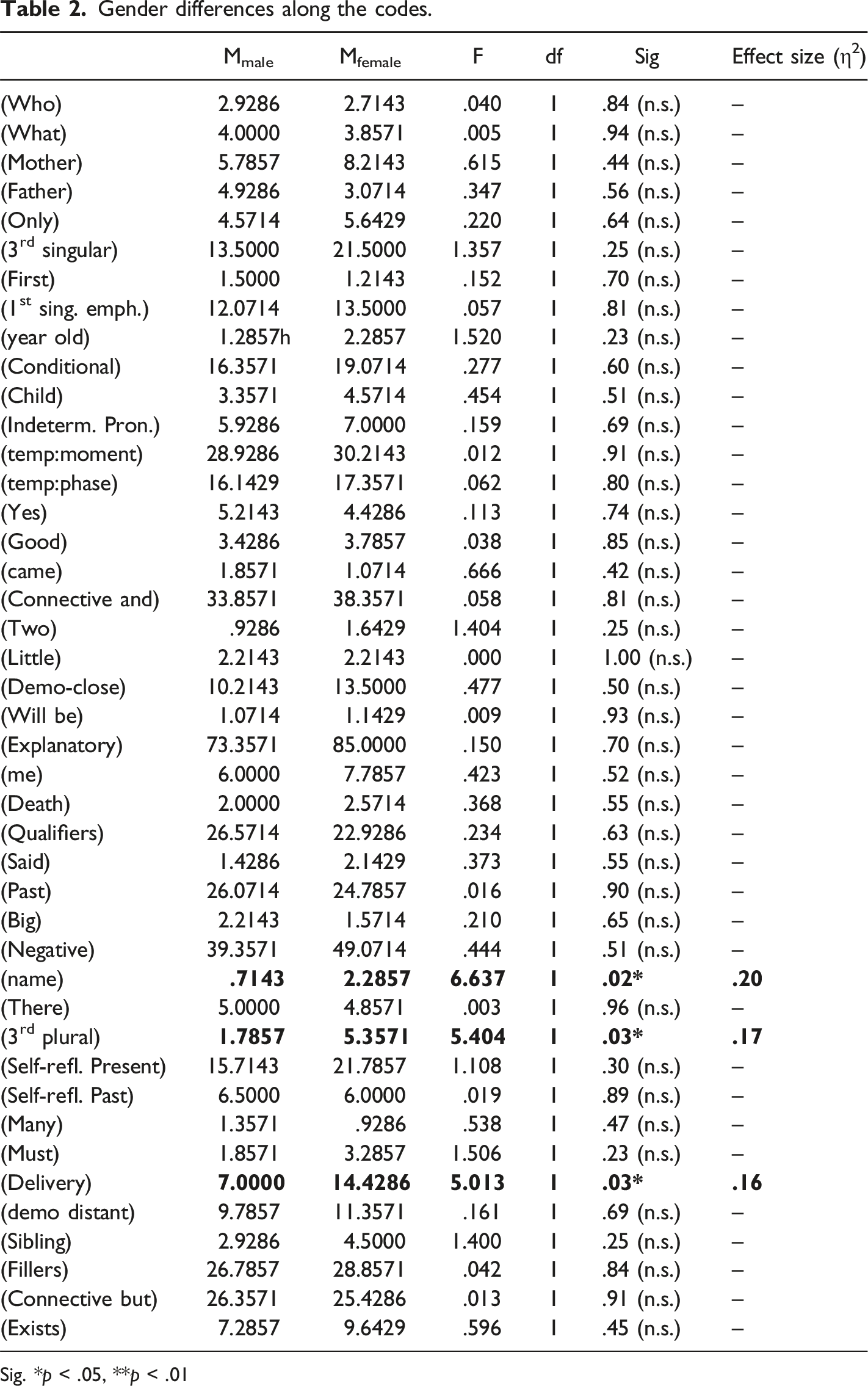
Sig. *p < .05, **p < .01
The qualitative Component: A Contextual Analysis For The Codes “Name” And “Delivery”
“Name” occurs more frequently among women, who, at the same time, speak about the theme less specifically, while men often mention the individual names. Of the 30 interviews, 12 female respondents raised this theme that resulted in 36 quotations, and only five occurrences of first names could be identified. Only five males spoke about names in the altogether 15 quotations but mentioned 13 specific names in the retrieved quotations. In the examples below, quotations from the same respondents are merged, and are separated by (…). Grammatical mistakes were not corrected in the verbatim translations as these often reflect the chaotic nature of the experience.
Examples: quotations on naming and names in women’s narratives
FDN: No…well, in some way he must have been registered and, uhm, now I am unable to remember he…we (in the family) all have two names, two Christian names.
FHM: Practically I inherited that name.
FJZ: Suddenly I realized that for me…that, that I have refused the name András because of this…that this is somehow not okay.
FRG: if someone mentions her in the family then they call her by my name as this is how she would have been called but it has never been clear if she was officially given this name or they had only wanted to, or I do not even know if these (stillborn) babies are registered or not.
Examples: quotations on naming and names in men’s narratives
MGA: …and we did not even write a name on it (the tombstone) as he is Peter (meaning stone).
MPLG: My parents always told me why I have two names, but I do not know any other grave (…) I consider my name as something special, that I am also G. I have two names, and this is so good for me.
Naming the deceased infant is an important act for the siblings as it facilitates construing the bond and reconstructing the experience. Siblings’ uncertainties are reflected in the recollections (“has never been clear”, “did not even write a name”, “unable to remember”). Having a first and a middle name is not a general custom in Hungary and this custom is related to the loss in the surviving siblings’ narratives. The “replacement child” phenomenon is mentioned in a negative (“call her by my name”), a neutral (“inherited”) and in a positive context: (“this is so good for me”).
Quotations on the deceased sibling’s birth (women)
FHM: Practically, he was buried though it was offered not to bury him as stillborn babies are easily managed (sigh) by the hospital, it is not necessary to bury them, but daddy insisted on the burial, I think. (…) hadn’t the labour started, my mummy would have died too (…) and then my younger brother was born but it is evident…well, surely the whole family was shocked but we have never spoken about it, about that…surely there was the pain and when I was born I was absolutely overwhelmed by their care and I can still feel it as I was a spoiled child in those days.
FJZ: And she had to deliver the baby naturally and my mum has always highlighted that she had to deliver a dead baby (…) I think I can accept it… can imagine how my mum could have felt about it since I also delivered or, rather, was pregnant.
FKE: …and my mum, of course, was sleeping and they put my little sister into an incubator as she was a little bit purple and there was a scar on her forehead at the temple (showing) as they accidentally cut her (“double pronoun” 1 in the original) when performing the caesarean section. She did not have any problems, I think she was born with a 9 or 10 Apgar score so she was perfect, perfect (…) and then she (the mother) was in the hospital for several days and she could see the mothers suckling and loving their new-born babies in the neighbouring beds and she…not any more (…) and she tried to ask the delivery nurse to tell her what had happened to her daughter but nobody cared until she began to scream right in the middle of the delivery department that someone immediately should tell her what had happened to her child.
FKF: No, no, this is not a surgery, but she had to deliver the baby and they did not show the baby to her, but he was taken. My mother could not even mourn him and very probably they have never talked about it with my father (…) and my mother told me that in those days you could record your baby’s heartbeat on an audio cassette and she was listening to it for weeks and then had to deliver the baby and it was a stillbirth (…) I myself have never lost a baby but I think this pain cannot be processed, or there is going to be emptiness, and the memory of an unborn child will survive within you.
FPI: This was a deep shock for me as a child … I did not know too much about delivery and I knew that it was painful and what if I was to give birth to a baby and it is such a torment (…) my first impression on the birth of a human child is that my sibling was delivered in an agony by my mother.
FTD: the poor one (the mother) was put in a common room with the mothers of live born babies.
Quotations on the deceased sibling’s birth (men)
MGA: My mum had not been expecting yet and I could dream of a new-born brother who then disappeared. (…) I did not share the information (with the father) and then we packed up her suitcase, really, I packed up for her as my mum could not even move…uhm…well, I did not know that these were the birth throes...but…that she was unable to pack up…she always did these things, packing up…but…that…uhm…well, and my little sister was exultant as she was…and I packed up and my father had not arrived yet and then…then my mum said that I should call him again and then I had the sense to tell him: “Daddy, come home, there’s trouble.” (…) they did not tell me the whole story, all that happened… my mum’s doctor was on holiday and only a resident doctor was there. The baby was not in the right position but despite that the doctor induced the delivery, in a natural way, and my dad told me that my mum had almost died of it, too and they decided on the caesarean section only later… and how, or how…he (the baby) suffered some injuries or there had been some problem before… I have never been told about these.
MHB: We were expecting our little sister and it turned out 2 hours before the delivery that she had died and, actually, this did not make a deep impact on me, I don’t know…I can fully accept that this is…this is natural, that such things do happen.
MPB: He was the first one and if he had been born, he would have been named V.
Not surprisingly, birth is a theme that women raised significantly more frequently. This theme was represented in all the female respondents’ narratives (16) and most of the male respondents’ narratives (12). However, only 67 of the 210 mentions were found in men’s texts and one of them, MGA raised the theme very frequently (24 of the 67 quotations). He as a 13-year-old boy at the time of the loss had to help her mother prepare for the preterm labour and get to the hospital. His involvement was deep and direct: a responsibility disproportionate to his age and role within the family. Contrastingly, MHB, who was not involved in the experience, highlights the common nature of the loss: “such things happen.” Women focussed on the emotional contents and developed an understanding on their mothers’ possible lived experiences (deliver a dead baby; loss of a perfect baby; not showing the baby but previously listening to her heartbeats; delivery as agony; sharing a room with mothers of live babies). Negative attitudes concenring the contemporary “helping” protocol to “manage” the infant’s body (hospital cremation) is reflected in the speaker’s awkward word use. The potential risk of losing the mother – one of the deepest worries for a child – is also mentioned. At the same time, the child born after the loss may receive extra attention and care.
Discussion
Most of our results have confirmed the main findings of our previous study (Bornemisza et al., 2021) as there were very few significant gender differences in this sample. Our results are similar to Seltzer and associates’ (2019) findings on grief narratives. There are more similarities than differences between male and female bereaved persons
Procedural meanings are informative about the intensity of the emotional experience. It seems that the organization of trauma-related texts have uniform characteristics, and a final common pathway is reflected in the similar occurrences of procedural contents. This is a result that can be explained by the phenomenology of crisis experiences: in the chaotic moments of transformations the person’s state or situation will dominate over the stable social roles and personality traits (B. Erdos & Javor, 2021; Kézdi, 1995). As Seltzer and associates (2019) have commented: “Gender differences are most likely to occur in contexts where gender roles are particularly salient.” Sharing the grief experience does not constitute such a context. As for procedural contents, there is only one exception to this general rule: reference to the social network (they, them, with them, for them) is significantly more frequent among women who tend to rely on their social network for support more than men (Kneavel, 2021). However, these mentions – irrespectively of the gender of the speaker – are mostly related to the family, one’s strong social ties (“they” as the parents, the other siblings, or, in a few cases, the medical staff). This again is a finding that can be connected to crisis situations where weak social ties (Granovetter, 1973) lose their significance and persons focus on their close relationships, this known as situative constriction (B. Erdos & Javor, 2021; Ringel, 1973).
We could identify salient differences between two conceptual meanings (content words). Naming the deceased sibling is an act that validates the sibling’s existence as a person, a family member, and a social being. This is important for the surviving siblings as it protects them – to some extent – from disenfranchised grief, and from the irrational but sometimes assumed threat that a child can simply disappear from the life of the family. The topic is more frequent among women who, at the same time, speak about it more vaguely, while men are highly specific, and in their eyes the specific names are important data.
Not surprisingly, a marked difference was found in the use of the expressions related to the birth process. Men referred to it less frequently, focusing on the possible causes and the circumstances. Women’s identification with the mother was much stronger, and with a few exceptions, they focused more on their emotions. MGA, a man was deeply involved in her mother’s delivery process when he was a teenager, and this could explain his highly emotional comments. Women often referred to their parents’, mostly their mother’s perceived or imagined mental state. They clearly captured the experience that their mothers’ bodies “have failed” (Kersting & Wagner, 2012, p. 190). Most speakers also related the event to their own, previous, or anticipated delivery.
The small sample size and the shortness of some interviews are a limitation of this study. People might still be reluctant to share their experiences related to perinatal loss and this was even more so in the past when our respondents suffered the losses. Further, the Hungarian language poses a limitation on quantitative analysis of verbal contents as the variety of suffixes referring to similar procedural contents are extremely high and the suffixes themselves – usually one or two letters only – may have several different meanings.
Conclusion and Clinical Implications
Authors have analysed the potential gender differences in sibling grief on perinatal loss. The analysis has confirmed that the depth of the grief experience does not differ in women and men – but the ways they express it is somewhat different. Men relate more specific data and are less concerned with the delivery process in their recollections, provided they have not been directly involved in the event. Women refer to the members of their social network more frequently, but these mentions are mostly restricted to close family members as strong social ties, and to the medical staff. This can be interpreted as a general characteristics of crisis experiences, known as situative constriction. Further, the recollections are about deaths that occurred several decades ago in Hungary, when perinatal loss was a social taboo, a story not to be shared outside the immediate family or not to be shared at all.
Our explorations have confirmed the long-term impacts of sibling grief over perinatal loss on the surviving siblings’ lives. Early, preferably family-based intervention could protect the surviving siblings from these impacts, such as destructive changes in the family dynamics and structures, and potential impairments in family members’ mental health. Such interventions could help the siblings cope with the lasting and frequently occurring anxieties that they relate to childbirth so that they could live their adult lives according to their own choice.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Note
Search Bibliography
Words with multiple meanings were double-checked using the “confirm always” option of ATLAS.ti. 8.00
Search Bibliography.
Category
Translation
Original Search Bibliography
Who
who|whom|about wholwith who
ki|aki
What
what|about what|with what|
Ami*
Mother
mother|mum*|
anyu*|anya|anyukám*|édesany* |anyá*
Father
father|dad*
apukám|édesap*|apu*|apa|apá*|
Only
only|just
Csak
3rd singular
they|them (to them, with them etc.)
ő|neki|rá|róla|vele
First
First
Első
1st singular (accentuated use)
I
Én
year (old)
year (old)
Éves
Conditional
perhaps|maybe|possibly|might be|if
talán| volna|lenne|lehet|lehetett|ha
Child
child|children
Gyerek*
Indeterminate
Any*
Vala*
Temporal (moment)
then|when|since|after
aztán|akkor|amikor|utána|mikor|után
Temporal (phase, period, length)
Yet, always
már|még|mindig
Yes
Yes
Igen
Good
good|well
jó|jól
came
Came
Jött
Connective and
And
És
Two
Two
Két
Little
Little, tiny
kis|kicsi*
Demonstrative close
this|these
ezt|erről|erre|ezek|
Will be
Will be|will become
Less
Explanatory
as|because|that is
tehát|mert|hogy|azért|úgyhogy|hogyha
Me
(in|with|on etc.) me
magam*|rám|nekem|bennem|engem|velem
Death
died|dead|lived|not alive
meghalt|halott|élt|életben
Qualifiers
such|so|as|this much|that much|very
ilyen|nagyon|úgy|annyira|milyen|így|ennyire|olyan|mint
Said
Said
Mondta
Past
was|were|happenedbecame
történt|volt|lett|voltak
Big
big|great
Nagy
Negative
no|not||never|none|neither|nowhere
nem|sem|se|ne|seho*|semmi*|soha*|nincs*
name
name
név|neve*
There
There
Ott
3rd plural
they|them
velük|ők|őket|nekik
Self-reflective (present)
know|remember|can|think|am|according to me
tudom|emlékszem|szerintem|tudok|gondolom|vagyok
Self-reflective (past)
said|was|knew|thought
mondtam|voltam|tudtam|gondoltam
Many
many|much|a lot
Sok
Must
must|had to|needed|should|have to
kellett|kell|szükséges|kellene |muszáj|
Delivery
delivery|birth|hospital|born|baby
szület*|baba|babá*|szülött*|szülés*|kórház*
Demonstrative distant
That (about) that, those
azt|arról|arra|azok
Sibling
Sibling
Testvér*
Fillers
really|of course|somehow|certainly|let’s say|otherwise|well|surely
igazából|ugye|valahogy|persze|mondjuk|egyébként|szóval|biztos|nyilván|hát|
Connective but
but|or| rather
de|hanem|inkább|vagy
Exists
There is
van