
Abstract
End-of-life (EOL) conversations with relatives or significant others are often avoided. One reason can be negative expectations regarding these conversations. The present study was conducted to develop and initially validate the End-of-Life Conversations – Expectations Scale (EOLC-E). An exploratory factor analysis (N = 307) resulted in a 20-item version with three distinct dimensions: expected own emotional burden (α = .92), expected other person’s emotional burden (α = .94) and communication self-efficacy (α = .89). The EOLC-E total score correlated significantly with communication apprehension about death (r = .62), fear of death (r = .58), death avoidance (r = .52) as well as readiness for end-of-life conversations (r = −.38) and occurrence of previous conversations (r = −.29). Results suggest that the EOLC-E is a reliable and valid instrument to assess death and dying communication expectations. This measure has utility in communication research focusing on optimizing expectations and increasing EOL communication.
Introduction
A large body of research work has demonstrated the high relevance of open communication about death and dying. In the context of medicine and palliative care, this approach facilitates higher congruence between patient’s desired and provided end-of-life (EOL) care (Detering et al., 2010; Mack et al., 2010), as well as reducing distress, anxiety and depression in bereaved family members (Detering et al., 2010). Moreover, it is well documented that aggressive EOL medical treatment is associated with poorer patient quality of life (Wright et al., 2008). Open communication about death and dying is associated with less aggressive medical treatment at the end of life, reduced risk of complicated grief (Wright et al., 2008; Yamaguchi et al., 2017) and overall lower costs for the healthcare system (Starr et al., 2019).
Besides persons with life-limiting illness, healthy and younger individuals can also benefit from EOL conversations (Gerard, 2017). Dealing with one’s own mortality can lead to a reduction of death-related fears (Llewellyn et al., 2016; Mroz et al., 2022), increased insight into expressed end-of-life wishes (Lambert South & Elton, 2017; Llewellyn et al., 2016) as well as clarification of one’s personal values in life (Mroz et al., 2022).
Despite these advantages, EOL conversations are often avoided or postponed to a later point in time (Fried et al., 2005; Seifart et al., 2020). Such postponement might, however, lead to the individual no longer being able to adequately express their wishes, for example due to an unexpected deterioration of their physical condition (Seifart et al., 2020). In a German representative survey, 80% of the sample considered death and dying to be important discussion topics, but only half of the respondents reported ever having explicitly dealt with these topics in any way (Strupp et al., 2021). Similar results have been demonstrated in studies with adolescents and young adults. Although most of them consider following their EOL wishes as important, few have discussed them with family members or loved ones (Tripken & Elrod, 2018).
One reason for the discrepancy between perceived benefits of EOL conversations and their occurrence could be negative expectations regarding a conversation about existential matters with another person. For instance, one recent systematic review focusing on avoidance factors influencing EOL conversations found the expectation of emotionally burden the conversation partner too much or the self-expectation of being unable to address death-related topics in an adequate manner to be decisive factors in explaining this discrepancy (Nagelschmidt et al., 2021).
An expectation is defined as a “conditional belief about the probability of future events, experiences, or information” (Panitz et al., 2021). As expectations generally influence individual’s decisions and shape their behavior in anticipation of events or experiences, investigating the role of expectations is highly relevant in both basic as well as applied psychological disciplines (Panitz et al., 2021). In the context of medical treatment, there is evidence that expectations have an influence on health outcomes across a wide range of medical conditions (Laferton et al., 2017). Therefore, a number of interventions targeting the optimization of expectations have already been developed in this area, for instance in cancer care and cardiology (Rief et al., 2015, 2017; Shedden-Mora et al., 2020). In the EOL context, taking individual, situation-specific expectations into account, might help health professionals to encourage patients and their significant others to engage in EOL conversations at an early stage.
In the past, generic and multidimensional instruments assessing different aspects of expectations regarding medical and psychological treatment have been developed (Alberts et al., 2020; Moss-Morris et al., 2002). In the EOL context, measures have been developed assessing general attitudes towards death (Wittkowski, 2001; Wong et al., 1994) or death-related communication apprehension (Carmack & DeGroot, 2016). However, to our knowledge, no instrument explicitly assessing expectations regarding EOL communication has been developed. Therefore, we developed the End-of-Life Conversations – Expectations Scale (EOLC-E).
In this study, item properties, factor structure, reliability and validity of this scale were assessed in a German community sample. In addition to a structured assessment of expectations concerning EOL communication, the EOLC-E scale could serve to develop and evaluate targeted interventions aimed at modifying negative expectations regarding EOL conversations.
Methods
Scale Development
The EOLC-E was developed with the aim of assessing expectations concerning EOL conversations with a family member or significant other. For this purpose, we created a comprehensive pool of 89 items covering positive as well as negative expectations concerning the course of a conversation itself as well as longer-term consequences and a possible lack of benefit of EOL conversations. To create the item pool, we conducted an extensive literature research and screened the results of 17 qualitatively analyzed interviews (11 with young adults, 6 with older adults) carried out as part of an experimental study investigating psychological interventions to encourage readiness for EOL conversations (von Blanckenburg et al., 2021). The interviews were evaluated by trained bachelor and master students of clinical psychology using thematic analysis by Braun and Clarke (2006).
To improve content validity, the resulting 89 items were rated by a panel of four experts from the fields of palliative care, developmental psychology and clinical psychology. Experts were asked to rate each item on a 6-point Likert scale with regard to its fit to our construct and opportunity was provided for feedback and additional item suggestions. After conducting the expert panel, a small pretest with 28 participants assessed feedback concerning comprehensibility and acceptance of the resulting 85 items (mean age = 53.64, SD = 15.68, 46% female, 54% male). After adapting the items for understanding and the exclusion of several items due to lack of comprehensibility, 66 items remained.
Based on feedback from the expert panel as well as theoretical considerations, we further decided to narrow down the scope of the questionnaire and to only focus on situation-specific expectations regarding the course of the conversation itself. Therefore, all items covering longer-term consequences (35 items) and lack of benefit of end-of-life conversations (6 items) were excluded, resulting in an initial 25-item version of the questionnaire.
Before completing the questionnaire, participant instruction involves imagining a person in one’s life with whom one would most likely have such a conversation and to think of this person when completing the questionnaire. The items cover expectations related to one’s own actions and reactions during the conversation as well as reactions of the other person. All items are formulated as two-part sentences, beginning with the sub-sentence “If I talk to a relative or close friend about my death or dying…” and ending with the respective expectation (e.g. “…it will burden her/him emotionally.”). They are rated on a 6-point Likert scale ranging from 0 (“absolutely disagree”) to 5 (“absolutely agree”), with higher scores indicating more negative expectations.
Participants and Procedure
The study was preregistered in the German Clinical Trials Register (DRKS00025107) and approved by the local ethics committee of the Department of Psychology, Philipps University of Marburg (reference number 2021-32k). Recruitment took place between June 2021 and September 2021. Based on a subject-to-item ratio of 10:1, we aimed for a minimum sample size of N = 250 (Costello & Osborne, 2005). Participants were recruited mainly through university e-mail distribution lists, social media and flyers. In order to reach elderly participants, recruitment also took place in several day care facilities and retirement homes. Participants were eligible if they were aged 18 years or older, understood German sufficiently and had no severe cognitive impairment. The questionnaire set was provided either online or in a paper-pencil form. 444 participants started filling in the online version, 337 completed it. 41 participants were excluded due to implausible processing time for the entire questionnaire set (<10 min) and one due to implausible age information. Thus, data of 295 participants from the online survey were included in further analyses. Fifteen participants fully completed the paper-pencil version. Three were excluded due to systematic answering patterns. The remaining 12 participants were included in further analyses.
Other Measures
Sociodemographic characteristics, experiences with death and communication about death
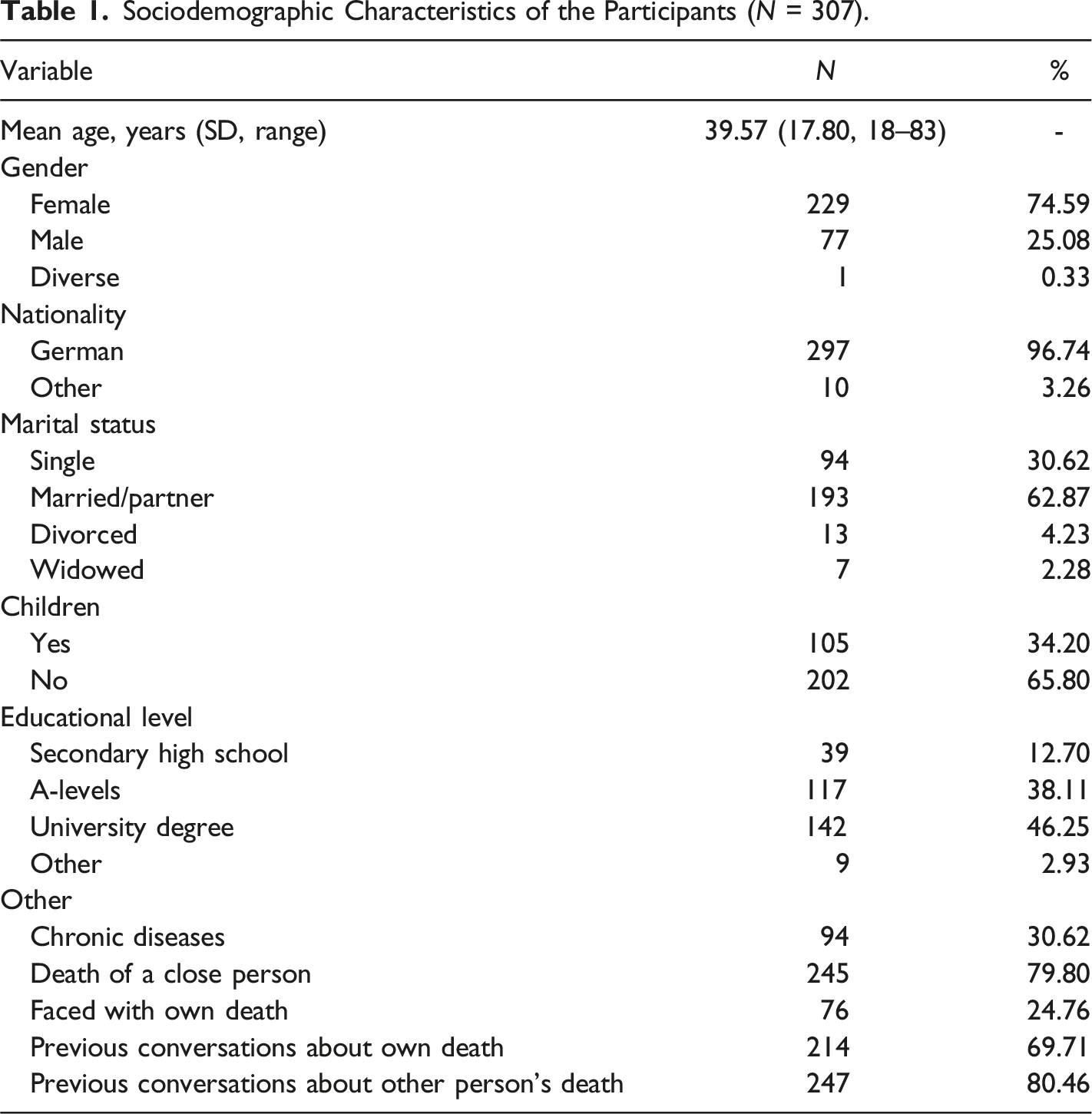
At the beginning of the study, participants were asked questions about their age, gender, marital status and other sociodemographic variables. In addition, previous experiences with death (e.g. death of a close person) and previous EOL conversations were captured.
Communication apprehension about death
In order to assess the participant’s fear associated with communication about death and dying, the Communication Apprehension About Death Scale (Carmack & DeGroot, 2016) was translated into German, using a forward-backward translation procedure (Beaton et al., 2000). Two bilingual native English-German speakers with psychological background supported the translation process. The 12-item CADS consists of the two subscales “communication apprehension” and “communication avoidance”. Items are rated on a 5-point Likert scale ranging from 1 (“strongly disagree”) to 5 (“strongly agree”). In our sample, Cronbach’s α was .92.
Fear of death, death avoidance and neutral acceptance
Fear of death (7 items), death avoidance (5 items) and neutral acceptance (5 items) were assessed using three subscales of the same names, which are included in the German version of the Death Attitudes Profile – Revised (Jansen et al., 2019). Items of the DAP-GR are rated on a 7-point Likert scale ranging from 1 (“strongly disagree”) to 7 (“strongly agree”). In our sample, Cronbach’s α was .90 for “fear of death”, .91 for “death avoidance” and .66 for “neutral acceptance”.
Readiness for end-of-life conversations
The 7-item subscale “readiness“ of the Readiness for End-of-Life Conversations Scale (Berlin et al., 2021) was used to assess the participant’s general readiness to talk about death and dying. The REOLC-items are rated on a 6-point Likert scale ranging from 0 (“absolutely disagree”) to 5 (“absolutely agree”). In our sample, Cronbach’s α was .79.
Anxiety and depression
Anxiety and depression were assessed using the 4-item Patient Health Questionnaire-4 by Löwe et al. (2010), consisting of a 2-item anxiety scale (GAD-2) and a 2-item depression scale (PHQ-2). In this questionnaire, response options to the question “Over the last 2 weeks, how often have you been bothered by the following problems?” are 0 (“not at all”), 1 (“several days”), 2 (“more than half the days”) and 3 (“nearly every day”). In our sample, Cronbach’s α was .76 for the GAD-2 and .80 for the PHQ-2.
Statistical Analysis
For the purpose of item analysis, item selectivity, item difficulty and variance were inspected. Inspecting item selectivity, the corrected item-scale correlation (r itc ) was computed for each item. To inspect item difficulty, the mean score of an individual item was divided by the highest possible score on the respective item and then multiplied by 100 (P i ). Only items with satisfactory characteristics were included in further analyses (requirements for inclusion: r itc > .40, 20 < P i < 80, sufficient variance). Subsequently, an exploratory factor analysis (principal axis factoring) was conducted to explore the underlying factor structure. To allow correlations between factors, an oblique rotation method was chosen. Scree test, Velicer’s MAP test and parallel analysis were conducted to determine the number of factors. Bartlett’s test of sphericity and Kaiser-Meyer-Olkin (KMO) test were conducted to ascertain that the data was suited for factor analysis. Factor loadings λ > .3 were examined in more detail and finally interpreted. Internal consistency was inspected using Cronbach’s α. To examine congruent and discriminant validity, Pearson correlations between the EOLC-E scores and related measures were computed. Furthermore, a multiple regression analysis predicting readiness for end-of-life conversations from the three EOLC-E subscales was performed. All analyses were conducted using IBM SPSS Statistics Version 28.
Results
Sample Characteristics
Sociodemographic Characteristics of the Participants (N = 307).
Items Analysis
Items and Item Characteristics of the EOLC-E.
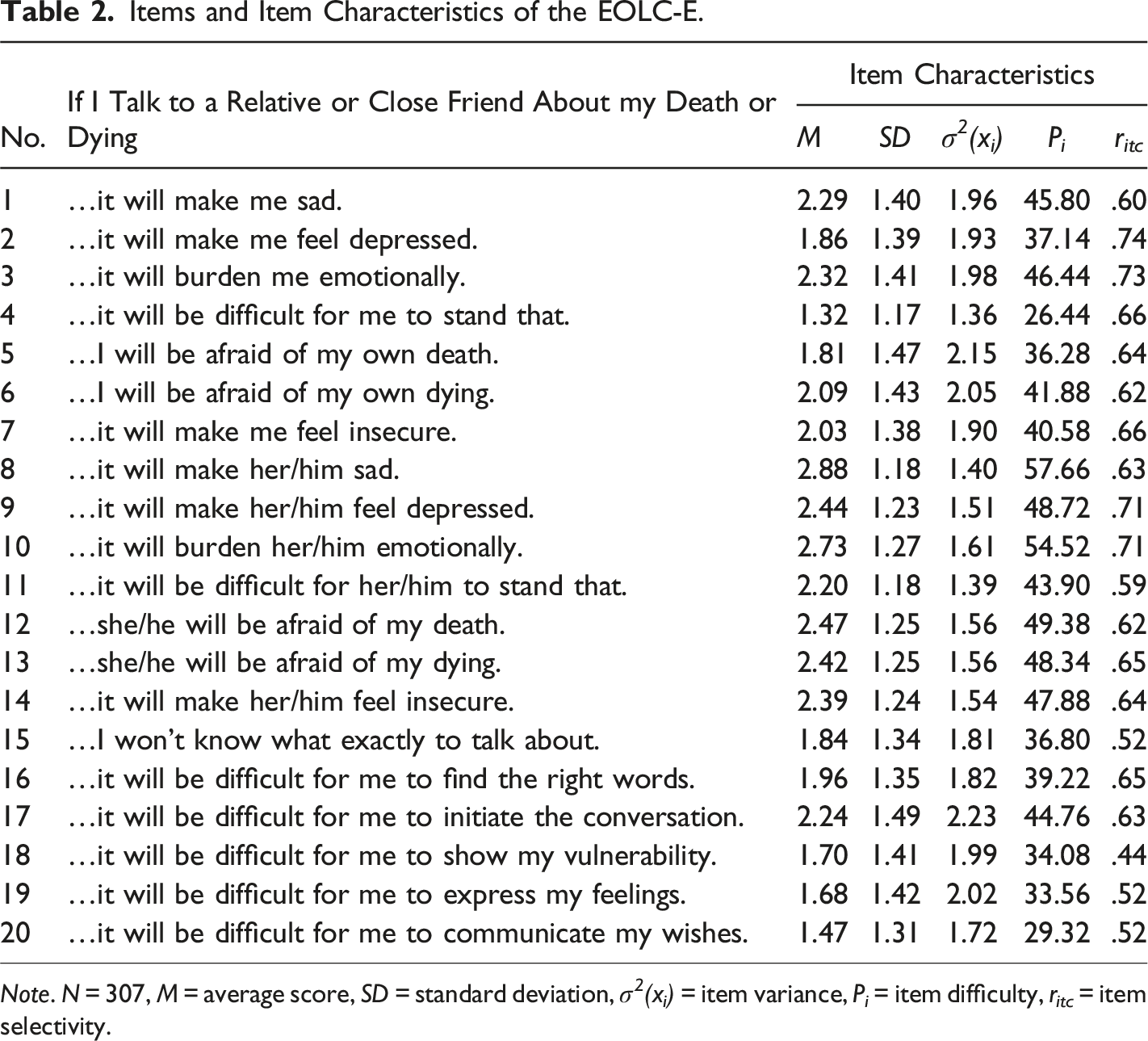
Note. N = 307, M = average score, SD = standard deviation, σ 2 (x i ) = item variance, P i = item difficulty, r itc = item selectivity.
Factor Structure
Data of 307 participants were included in factor analysis. Scree test and Velicer’s MAP test indicated the extraction of three factors. In parallel analysis, eigenvalues from actual data were higher than mean random eigenvalues for the first six factors. However, they were only very slightly above random eigenvalues for a four-, five- and six-factor solution, while they were clearly higher for a three-factor solution. Hence, we decided to extract three factors. Bartlett’s test of sphericity reached significance (χ2 (190) = 5108.13, p < .001) and the KMO value was .90, indicating sample adequacy for factor analysis.
Results of the Exploratory Factor Analysis (Principal Axis Factoring).
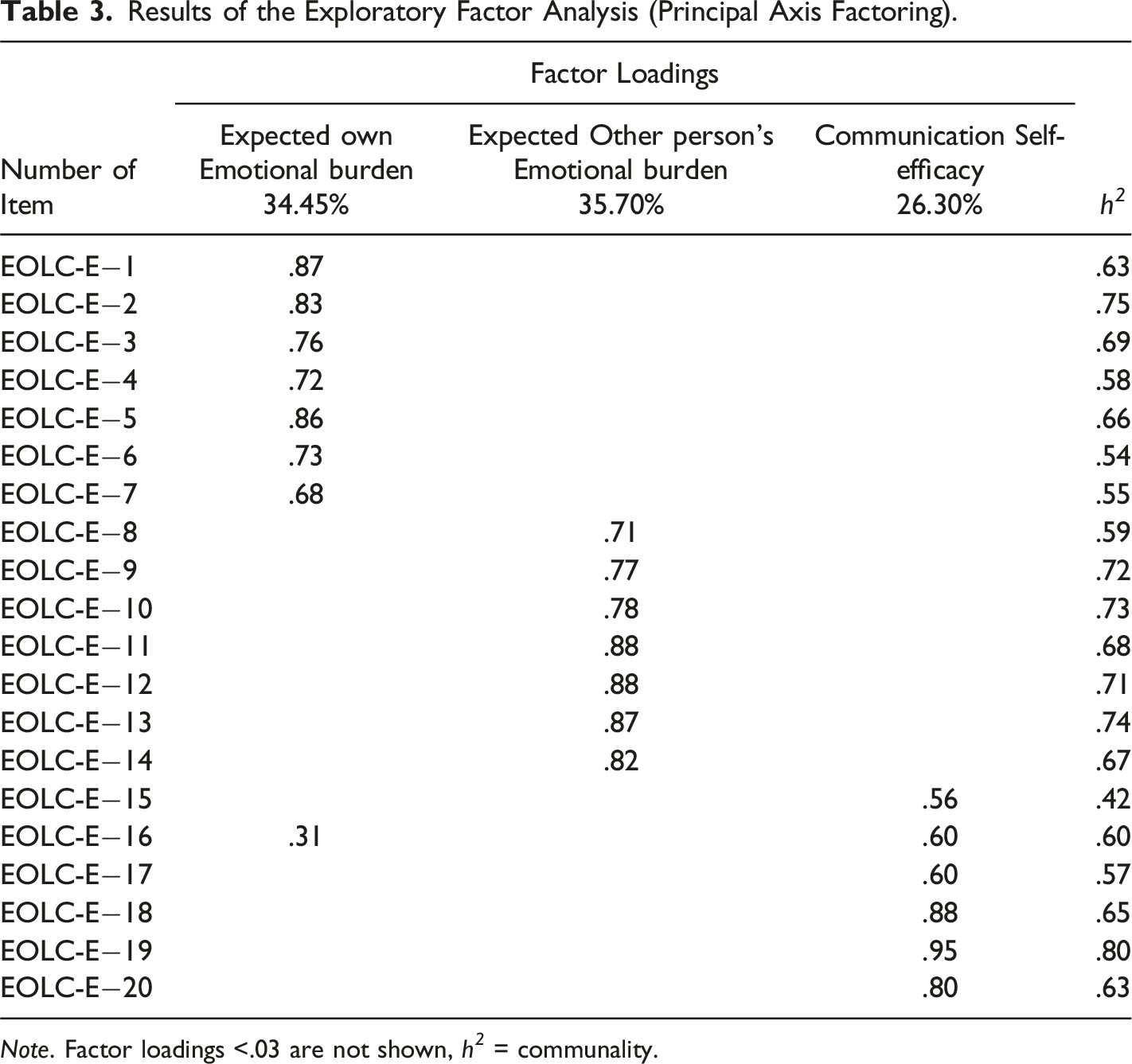
Note. Factor loadings <.03 are not shown, h 2 = communality.
Internal Consistency
Internal consistency was excellent for the total scale (α = .93) as well as for the subscales expected own emotional burden (α = .92) and expected other person’s emotional burden (α = .94). Internal consistency of the subscale communication self-efficacy (α = .89) was good.
Validity
Correlations of the EOLC-E Total Score and the EOLC-E Subscores with Related Measures.
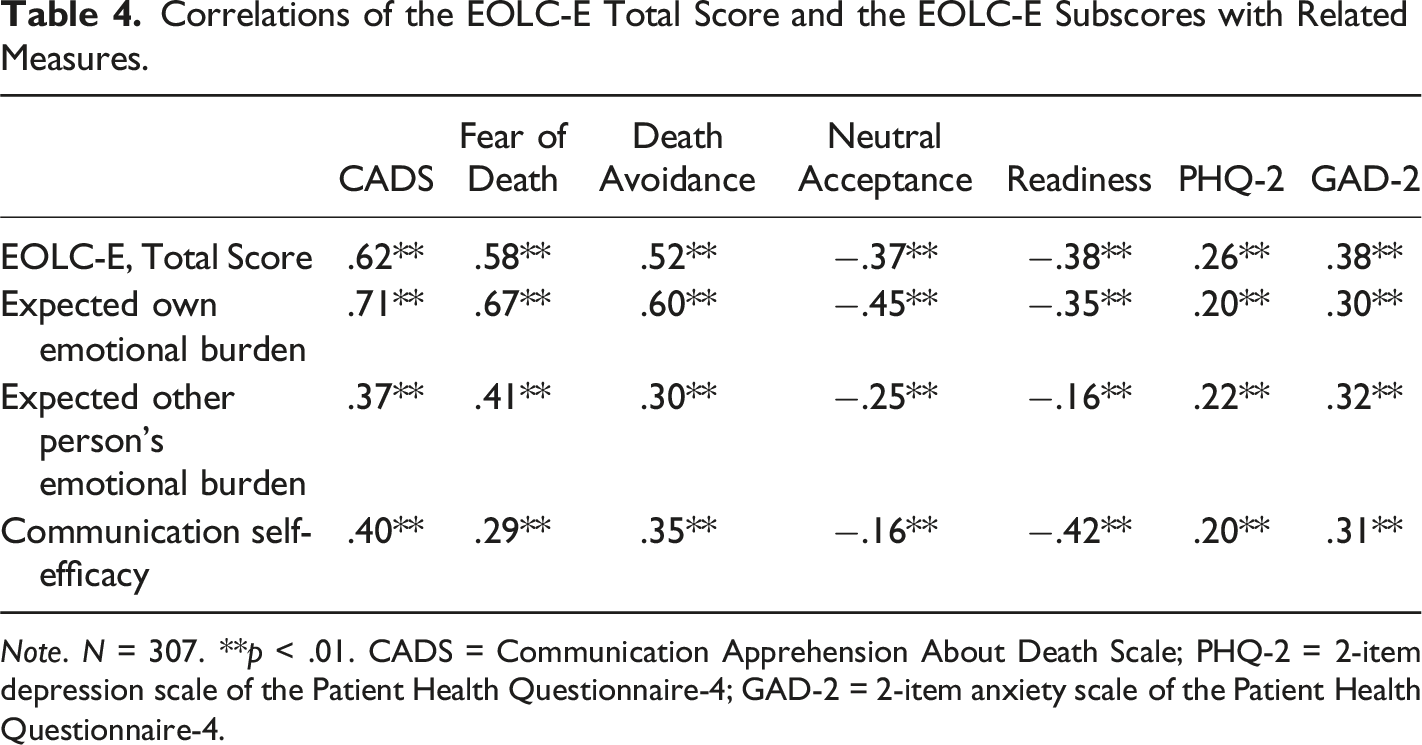
Note. N = 307. **p < .01. CADS = Communication Apprehension About Death Scale; PHQ-2 = 2-item depression scale of the Patient Health Questionnaire-4; GAD-2 = 2-item anxiety scale of the Patient Health Questionnaire-4.
Results of the Multiple Regression Analysis (using Readiness as the Criterion).
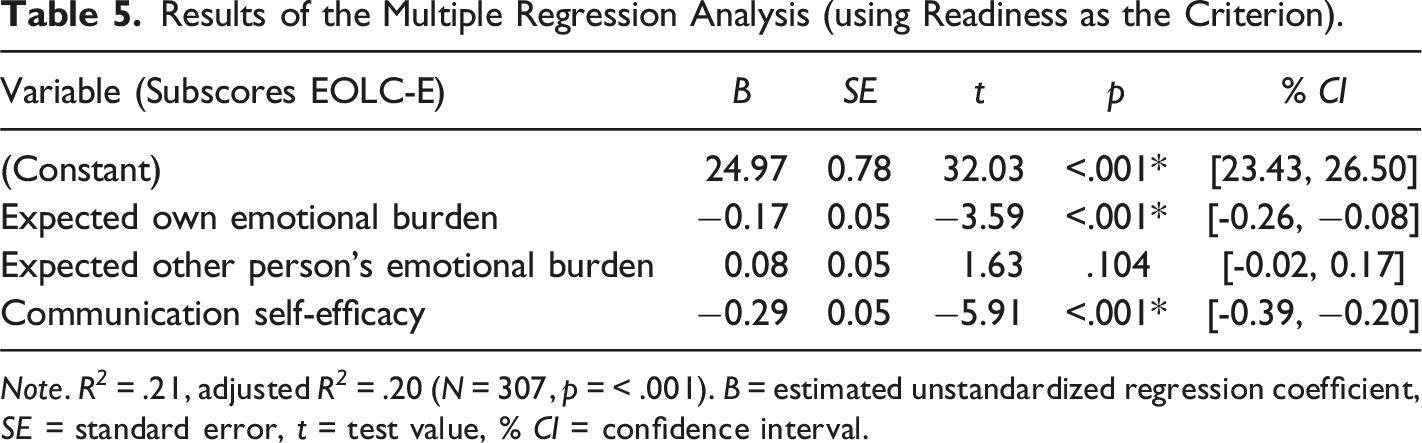
Note. R 2 = .21, adjusted R 2 = .20 (N = 307, p = < .001). B = estimated unstandardized regression coefficient, SE = standard error, t = test value, % CI = confidence interval.
The occurrence of previous end-of-life conversations (dummy-coded variable) correlated negatively with the EOLC-E total score (r = −.29, p < .01). With regard to the subscales, previous end-of-life conversations were associated with less expected own emotional burden (r = −.23, p < .01), less expected other person’s emotional burden (r = −.10, p < .05) as well as less negative expectations regarding communication self-efficacy (r = −.38, p < .01).
Discussion
Despite the many advantages of open communication, EOL conversations are often delayed or avoided by both younger and elderly individuals (Seifart et al., 2020; Strupp et al., 2021; Tripken & Elrod, 2018). One reason can be negative expectations regarding a conversation with significant others. Therefore, we developed and initially validated the EOLC-E scale, addressing these types of expectations.
Exploratory factor analysis resulted in a 3-factor solution. The factors showed good to excellent internal consistency and were clearly definable in terms of content. As cross loadings were low, all items could be clearly assigned to one factor. The first factor covers expectations about one’s own emotional burden during a conversation. This is in line with previous research, identifying the fear of emotional distress caused by EOL conversations as an important barrier (An et al., 2020; Glass & Nahapetyan, 2008). The subscale also includes expectations on an increased fear of death caused by conversations. This is of particular relevance, as fear of death is an important barrier to conversations about EOL preferences, especially for older adults (Glass & Nahapetyan, 2008).
The second factor covers expectations about the conversation partner’s emotional burden when talking about one’s own death. In a systematic review, Nagelschmidt et al. (2021) identified emotional processes, such as mutual protective buffering, as one of the most frequently reported barriers to open EOL communication in the family context. The desire to protect one’s own family or friends from sadness, fear or worries is often reported in literature as a key reason for avoiding end-of-life conversations (An et al., 2020; McGrath, 2004; Zhang & Siminoff, 2003). Moreover, the two items with the highest level of agreement (“…it will make her/him sad”, “…it will burden her/him emotionally”) belonged to this subscale, emphasizing the importance of these expectations. Therefore, it seems reasonable to not only assess expected own emotional burden during a conversation, but also expected other person’s emotional burden.
The third factor includes items related to self-efficacy expectations regarding communication about one’s own death or dying. In literature, there is evidence of a relationship between self-efficacy and the level of open end-of-life communication in the family context (Bachner & Carmel, 2009; Caughlin et al., 2011). Hence, it is important to consider these types of expectations with regard to end-life-conversations. Frequently reported barriers in this context are worries about not finding the right words as well as uncertainties about which topics to discuss (Keeley & Generous, 2015).
In this study, more negative expectations about EOL conversations (higher EOLC-E total score) were associated with more communication apprehension, fear of death and death avoidance as well as less death acceptance and less readiness to engage in end-of-life conversations, supporting convergent validity. Lower correlations with depression and anxiety were found, supporting discriminant validity.
In the multiple regression model, the three subscales explained 21% of variance in readiness to engage in end-of-life conversations, highlighting the important role of expectations. Interestingly, in contrast to the other two subscales, the anticipated emotional burden of the other person did not add significantly to the model. At the same time, however, protecting close persons from emotional burden is reported as a key barrier to EOL communication (An et al., 2020; McGrath, 2004; Zhang & Siminoff, 2003). Additionally, in the present sample, the two items with the highest level of agreement belonged to the subscale expected other person’s emotional burden. One reason for this discrepancy might be that, in contrast to the EOLC-E scale, the measure for readiness rather assessed a general willingness to talk about EOL topics than the willingness to talk about it with a specific person.
In the present study sample, previous EOL conversations were associated with more positive expectations in general. They were further related to less expected own and other person’s emotional burden as well as more positive self-efficacy expectations with regard to EOL communication. Hence, engaging in EOL conversations might reduce fears of potential emotional burden and improve confidence for further conversations. However, as the cross-sectional design does not allow causal interpretations, further research on expectation change caused by conversations is needed, using longitudinal and experimental designs.
The present study has some further limitations. First, 70% of the participants had already had a conversation about their own death and mean scores of individual items as well as subscales were relatively low (suggesting fewer negative expectations in the present sample). Considering that, during recruitment, the study objective was made completely transparent to potential participants, it can be assumed that the sample was more open to EOL communication than the average population. This self-selection bias limits the generalizability of observed mean scores. However, generalizability of the factor structure and correlations is much less likely to be affected (Taylor et al., 2007). Second, we decided to focus on situation-specific expectations. However, other types of expectations might also affect readiness to engage in end-of-life conversations. Third, retest reliability of the EOLC-E has not yet been investigated.
Nevertheless, given the crucial role of situation-specific expectations in basic and applied psychological disciplines (Panitz et al., 2021) as well as medical treatment (Laferton et al., 2017), the EOLC-E can be an important and useful tool. It might help health professionals to better respond to their patients’ expectations concerning end-of-life communication.
Conclusion
Negative expectations are an important barrier to end-of-life communication. The 20-item EOLC-E is a promising instrument, allowing a structured assessment of these expectations. It can be used to develop and evaluate targeted expectation-focused interventions, aiming at increasing EOL communication. Taking individual, situation-specific expectations into account, might help health professionals to encourage patients and their significant others to engage in EOL conversations at an early stage. More research is needed to further examine the impact of expectations on decision-making and behavior in the context of EOL communication.
Footnotes
Acknowledgments
We thank Sophia Pörtner for her valuable support with data collection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation) – project number 290878970-GRK 2271, project 10.