
Abstract
Communication about the end-of-life (EOL) is often avoided, despite its association with positive outcomes for those affected and their caregivers. Negative expectations seem to be a mechanism through which avoidance is maintained. This study examined existing expectations in talking about death to a significant other and validated a caregiver’s version of the End-of-Life Conversation – Expectation Scale (EOLC-E-c) with a German community sample of N = 250. Participants most frequently expected EOL conversations to cause sadness in themselves and the other person. Confirmatory factor analysis supported the original three-factor structure: Expected own emotional burden (α = .92), expected emotional burden of the other person (α = .94), and communication self-efficacy (=.90). Internal consistency of the scale was excellent, and its validity was supported. Using the scale could be valuable for clinicians and researchers in understanding individuals’ expectations concerning EOL conversations and in developing targeted interventions focusing on expectation violation.
Introduction
Despite the inevitability of death, communication about it is often avoided in Western societies. Conversations surrounding death and dying are frequently perceived as taboo, difficult, and distressing (Scheinfeld & Lake, 2019; Wildfeuer et al., 2015). Although the majority of the general population in Germany appears to consider death, dying, and grief to be important topics, only about half engage in discussions addressing these themes (Strupp et al., 2021).
In many Western societies, the processes of dying and death have been increasingly shifted into health care settings, resulting in a significant decline in family involvement (Sallnow et al., 2022). Nevertheless, communication between patients and caregivers remains a crucial aspect of end-of-life (EOL) experiences (Fenton et al., 2024). Such communication has been associated with increased alignment between individuals’ preferences and the care received (Detering et al., 2010), reductions in overtreatment (e.g., non-indicated ventilation and resuscitation) and earlier hospice enrollment. These outcomes are, in turn, linked to improved quality of end-of-life care and death (Wright et al., 2008; Yamaguchi et al., 2017). Additionally, less intensive medical treatment is not only associated with higher quality of life but also with reduced health care costs (Patel et al., 2018; Zhang et al., 2009).
Caregivers often bear responsibility for end-of-life medical treatment decisions, which can lead to emotional distress and persistent doubts about their choices (Wendler & Rid, 2011). Confidence in understanding the patient’s treatment wishes appears to mitigate these negative effects (Wendler & Rid, 2011). Furthermore, postponing or avoiding EOL conversations has been linked to adverse psychological outcomes for family members and significant others including increased stress (Detering et al., 2010), feelings of guilt (Jonasson et al., 2011), depressive symptoms (Bachner et al., 2021; Yamaguchi et al., 2017), anxiety (Detering et al., 2010), reduced personal growth (Generous & Keeley, 2022), bereavement-related distress (Haaksman et al., 2024), and complicated grief (Yamaguchi et al., 2017).
One potential explanation for the gap between the benefits of EOL conversations and their infrequent occurrence lies in individuals’ unfavorable expectations. Expectations are defined as probabilistic beliefs regarding the likelihood of future events, experiences, or outcomes (Panitz et al., 2021). Research has demonstrated that modifying expectations can lead to improved health-related outcomes (e.g., Rief et al., 2017; Shedden-Mora et al., 2020). In the context of EOL conversations, expectations such as the desire to protect oneself or others from emotional distress, and the belief that “positive thinking” precludes discussing death, have been identified as contributing to avoidance (Nagelschmidt et al., 2021). The modification of expectations seems to be a possible mechanism through which EOL conversations can be facilitated. Initial research suggests that expectations regarding EOL conversations can be modified through targeted interventions (Bendel et al., 2025). However, in order to design effective interventions, it is first necessary to identify the specific unfavorable expectations individuals hold. The present study utilizes and validates a newly developed questionnaire to provide a comprehensive overview of common and less frequent negative expectations surrounding conversations about death, with the aim of informing future interventions.
Several instruments assessing aspects of communication about death have been developed and validated including the communication apprehension about death scale (Carmack & DeGroot, 2016) and the death attitude profile-revised scale (Wong et al., 1994). However, these instruments do not explicitly address expectations. The End-of-Life Conversation-Expectation Scale (EOLC-E) was therefore developed, based on literature research and a subsequently evaluated by four experts from palliative care, clinical psychology, and developmental psychology, as the first tool specifically designed to assess expectations related to communication about death and dying (Bendel et al., 2022). Yet, like most existing questionnaires, the EOLC-E focuses solely on individuals’ expectations concerning their own death. Given that conversations inherently involve at least two participants, it is essential to also consider the expectations of those close to the dying person.
This study had two primary objectives. First, it aimed to explore prevailing expectations surrounding end-of-life conversations from the perspective of a significant other (i.e., any person important in the individual’s life) within a German online community sample. Second, it sought to validate an adapted version of the EOLC-E scale, focusing specifically on conversations with a significant other about their death. The psychometric properties and proposed factor structure of the adapted scale were assessed using this sample. Findings from this study contribute to a deeper understanding of caregivers’ expectations in the context of end-of-life communication and provide a foundation for the development of interventions aimed at addressing and modifying identified unfavorable expectations.
Methods
Participants and Procedure
Participants were recruited through in-person interactions, university mailing lists, and social networking sites including Instagram and WhatsApp. The study’s inclusion criteria consisted of being at least 18 years old and having sufficient command of German language to engage with the study material. After providing written informed consent, participants filled out an online questionnaire. A lottery with vouchers (2 vouchers à 50 Euro, 4 vouchers à 25 Euro) and feedback on the study results were offered as incentives for participation. The study was approved by the Ethical Review Committee of the Department of Psychology at Philipps University of Marburg (2021-32k-Amendment) and the study was carried out in accordance with the tenets stated in the Declaration of Helsinki. The study protocol was preregistered in the German Clinical Trials Register (DRKS00034105).
Measures
End-Of-Life Conversation - Expectation Scale – Caregiver Version (EOLC-E-c)
The End-of-Life Conversations – Expectations Scale: Caregiver version (EOLC-E-c) was developed by analogously adapting items from the original German-language scale designed by Bendel et al. (2022) to focus on the death of a significant other instead of one’s own death. This semantic adaptation was conducted by the first author, a native German speaker, and verified by a second native German-speaking researcher to ensure conceptual equivalence and linguistic accuracy. The items reported here are English translations of the German version used in the study. These translations were initially drafted by the research team and subsequently verified by a native English speaker. Instructions prompted participants to imagine having a conversation with a chosen significant other about the significant other’s death and to keep this person in mind while responding to the items. A sample item was “If I talk to a significant other about her/his death or her/his dying, it will make her/him sad”. Participants were asked to indicate their agreement on a 6-point Likert scale from 0 (strongly disagree) to 5 (strongly agree), higher scores indicating increased negative and unfavorable expectations.
Readiness for End-Of-Life Conversations
Participant’s readiness to engage in conversations about death and dying was assessed with the Readiness for End-of-Life Conversations Scale (REOLC; Berlin et al., 2021). A sample item was “I know what advantages talking about the end of my life holds”. Each item was assessed on a scale from 1 (absolutely disagree) to 6 (absolutely agree). Internal consistency was good in this study (a = .80).
Communication About the Death of the Other
Communication about death and illness in close relationships was assessed with the German version of the 5-item Caregiver Communication with Patients about Illness and Death (Bachner et al., 2008; Betker et al., 2024). For the current study, items were converted into the present tense and the broader term ‘significant other’ (nahestehende Person) instead of ‘patient’ (Patient) was used. A sample item was “I avoid talking with a significant other about his/her feelings and fears”. All items were answered on a 5-point Likert type scale from 1 (strongly disagree) to 5 (strongly agree), higher sum scores indicating increased avoidance of communication about death and illness. In the current study, internal consistency was good (a = .81).
Communication Apprehension About Death
Communication apprehension about death was measured using a German version of the 12-item Communication Apprehension About Death Scale (CADS; Carmack & DeGroot, 2016), which had previously been translated by Bendel et al. (2022) for the purpose of validating the initial German version of the EOLC-E Scale. The CADS consists of two subscales “communication apprehension” and “communication avoidance”. A sample item was “I avoid talking about death altogether”. Each item was assessed on a scale from 1 (strongly disagree) to 5 (strongly agree). Cronbach’s alpha in this sample was .92, demonstrating excellent internal consistency of the scale.
Fear of Death, Death Avoidance and Neutral Acceptance
Fear of death, death avoidance and neutral acceptance were assessed using the corresponding subscales in the German version of the Death Attitudes Profile – Revised (Jansen et al., 2019). A sample item was “Death is neither good nor bad”. Participants were asked to indicate their agreement on a 7-point Likert-type scale from 1 (strongly disagree) to 7 (strongly agree). In the current study, Cronbach’s alpha was .91 for “fear of death”, .90 for “death avoidance”, .62 for “death acceptance”.
Trait Anxiety and Trait Depression
Anxiety and depression were measured with the Patient Health Questionnaire-4 (Löwe et al., 2010), consisting of two items on anxiety (GAD-2) and two items on depression (PHQ-2). A sample item was “Over the last 2 weeks, how often have you been bothered by the following problems? Little interest or pleasure in doing things”. Participants were asked to indicate their agreement on a scale from 0 (not at all) to 3 (nearly every day). In the current sample, Cronbach’s alpha was 0.83 in this sample (Cronbach’s α
Sociodemographic Data, Experiences with Death, and EOL Communication
Sociodemographic data (including sex, age, nationality and education level), personal experiences with one’s own mortality and the death of a significant other, as well as prior engagement in EOL communication, were assessed with self-constructed dichotomous (yes/no) items. To explore reasons for the lack or avoidance of EOL conversations, participants were presented with a list of seven potential contributing factors. For each factor they were asked to indicate whether the factor was a reason (yes), was not a reason (no), or if they had already had these conversations often (I have already spoken about it often).
Statistical Analysis
All data was analyzed using IBM SPSS Statistics 28 with a statistically significant threshold of p ≤ .05 on two-tailed analyses, except for the confirmatory factor analysis, which was conducted using the lavaan package (Rosseel, 2012) for Jamovi (The Jamovi Project, 2025). Confirmatory factor analysis was performed to assess factorial validity and was based on the three-factor model presented by Bendel et al. (2022). Mardia’s standardized coefficient for skewness was 63.4, χ2 (1540) = 2644, p < .001, and for kurtosis it was 507.0, z = 17.9, p < .001 indicating non-normality of the data. Consequently, the robust maximum likelihood method was used. To determine the model fit, the following standard fit requirements were considered: χ2-statistics, Comparative Fit Index (CFI), Standardized Root Mean Square Residual (SRMR), Root Mean Square Error of Approximation (RMSEA), Tucker-Lewis -Index (TLI). Cut-off values of CFI and TLI ≥0.90 were indicative of good fit and SRMR and RMSEA ≤0.08 were indicative of an acceptable fit (Brown, 2015; Schermelleh-Engel et al., 2003). Cronbach’s alpha was used to measure internal consistency of the total scale and its subscales. Pearson correlations were calculated between the EOLC-E-c scale and related measurements to examine validity of the scale.
Results
Sample Characteristics
Sample Characteristics
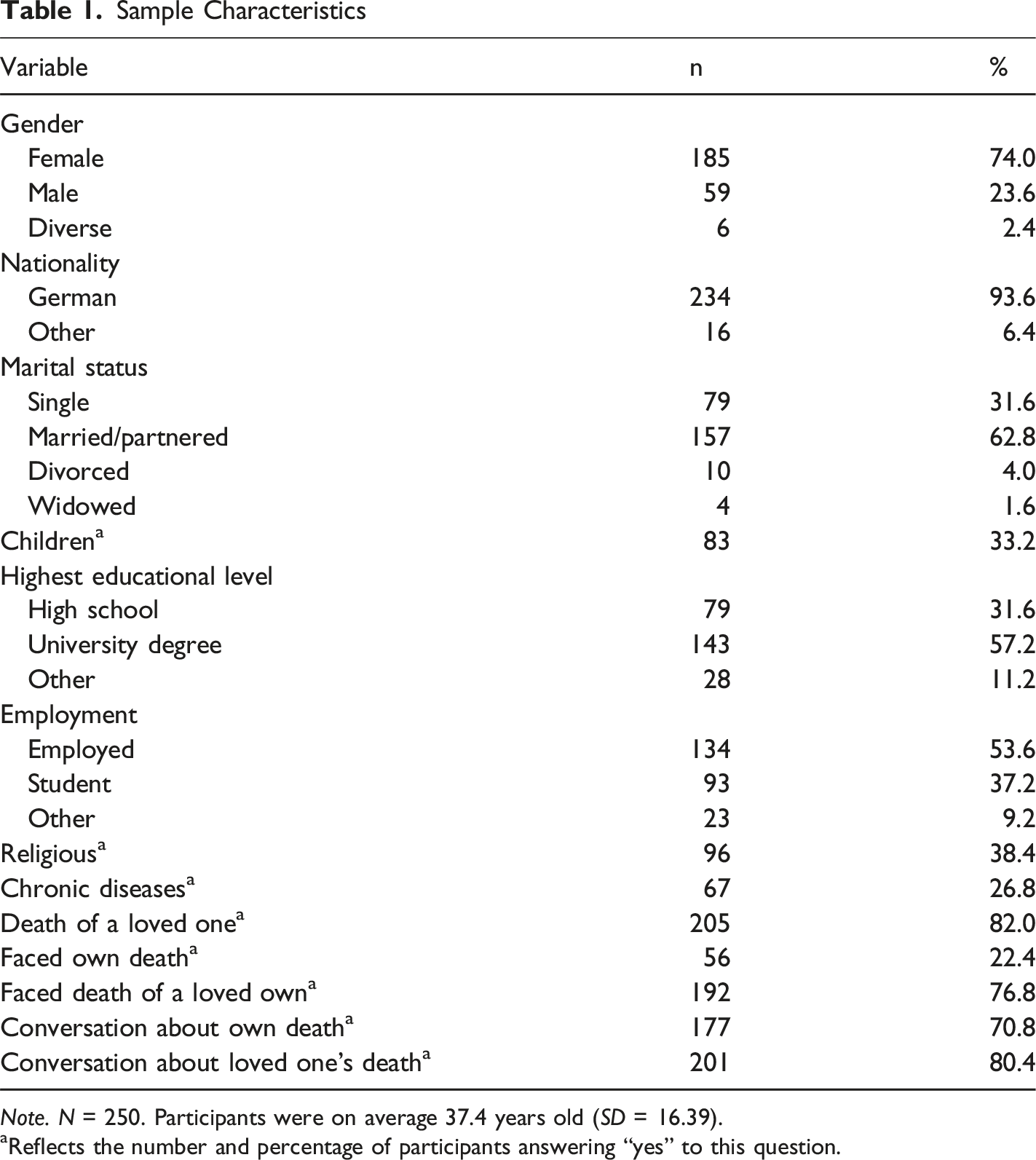
Note. N = 250. Participants were on average 37.4 years old (SD = 16.39).
aReflects the number and percentage of participants answering “yes” to this question.
Expectations and Item Analysis
Item Characteristics and Results From a Factor Analysis of the EOLC-E-c
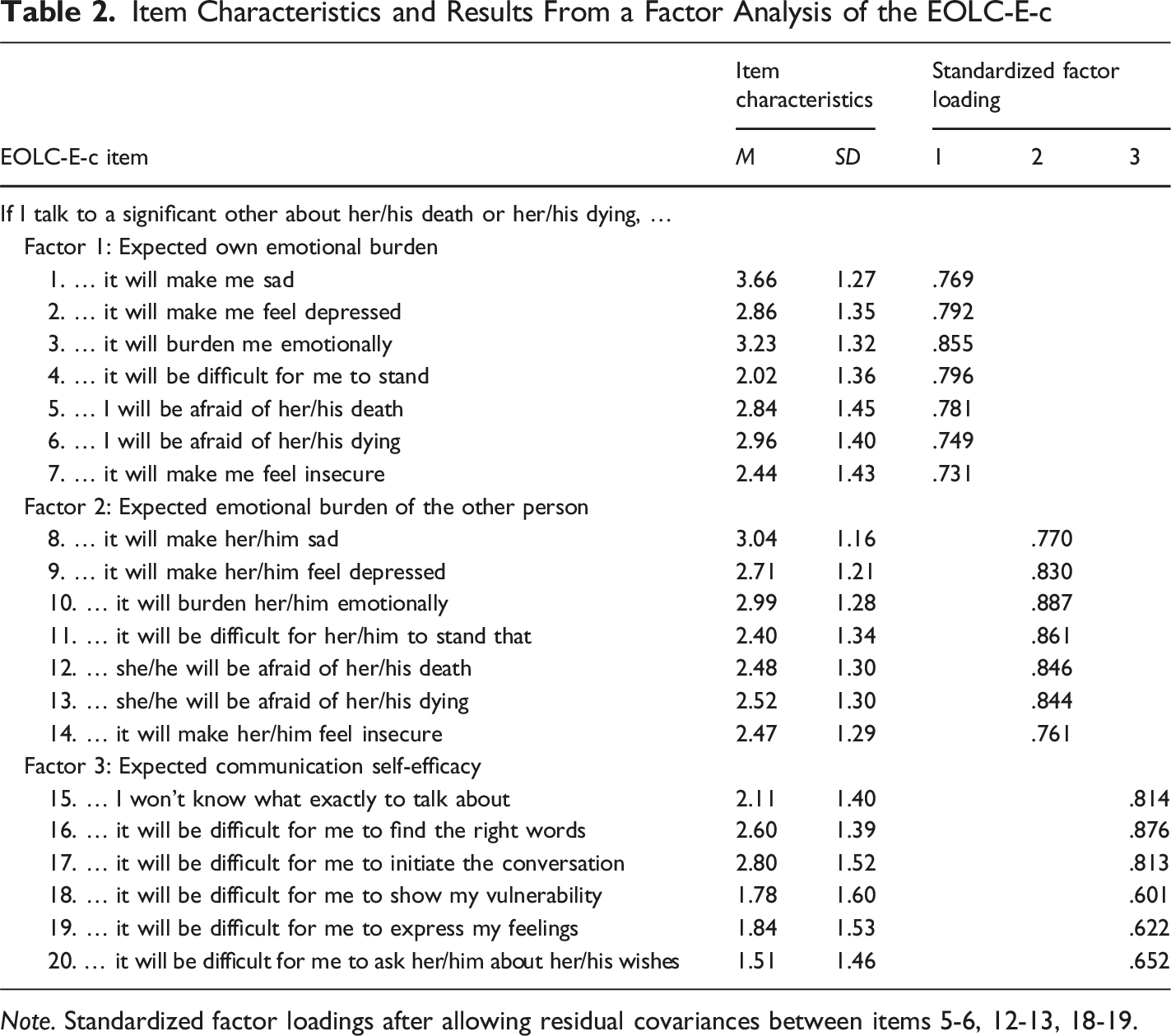
Note. Standardized factor loadings after allowing residual covariances between items 5-6, 12-13, 18-19.
Confirmatory Factor Analysis
Fit Indices of the Confirmatory Factor Analysis of the EOLC-E-c
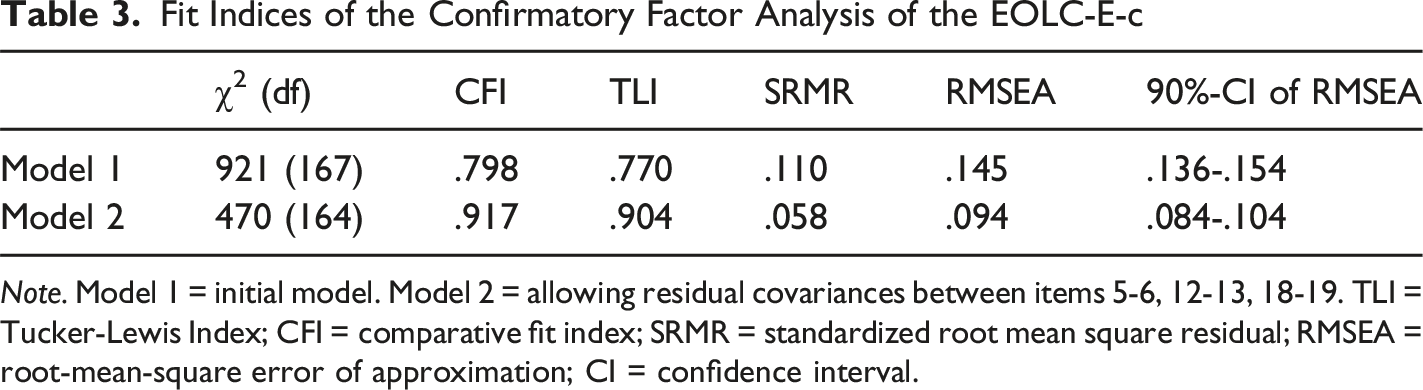
Note. Model 1 = initial model. Model 2 = allowing residual covariances between items 5-6, 12-13, 18-19. TLI = Tucker-Lewis Index; CFI = comparative fit index; SRMR = standardized root mean square residual; RMSEA = root-mean-square error of approximation; CI = confidence interval.
Internal Consistency
Excellent internal consistency was demonstrated for the EOLC-E-c scale (α = .92) and its subscales: expected own emotional burden (α = .92), expected emotional burden of the other person (α = .94), and communication self-efficacy (α = .90).
Validity
Correlations Between EOLC-E-c, its Subscales, and Related Measures
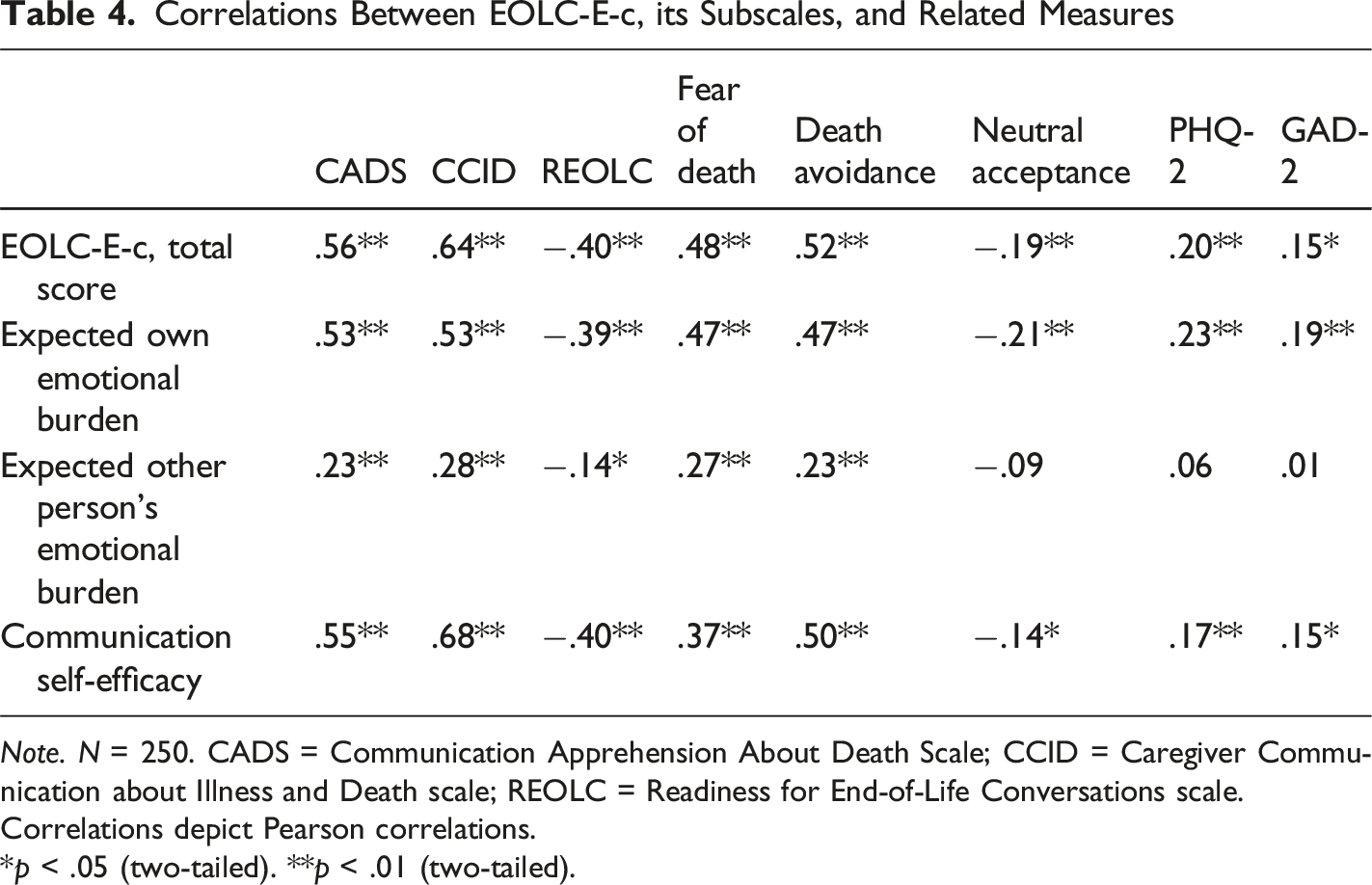
Note. N = 250. CADS = Communication Apprehension About Death Scale; CCID = Caregiver Communication about Illness and Death scale; REOLC = Readiness for End-of-Life Conversations scale.
Correlations depict Pearson correlations.
*p < .05 (two-tailed). **p < .01 (two-tailed).
Additional Analyses
Effects of Demographics, Death-Related Experiences and Death Attitudes on EOLC-E-c
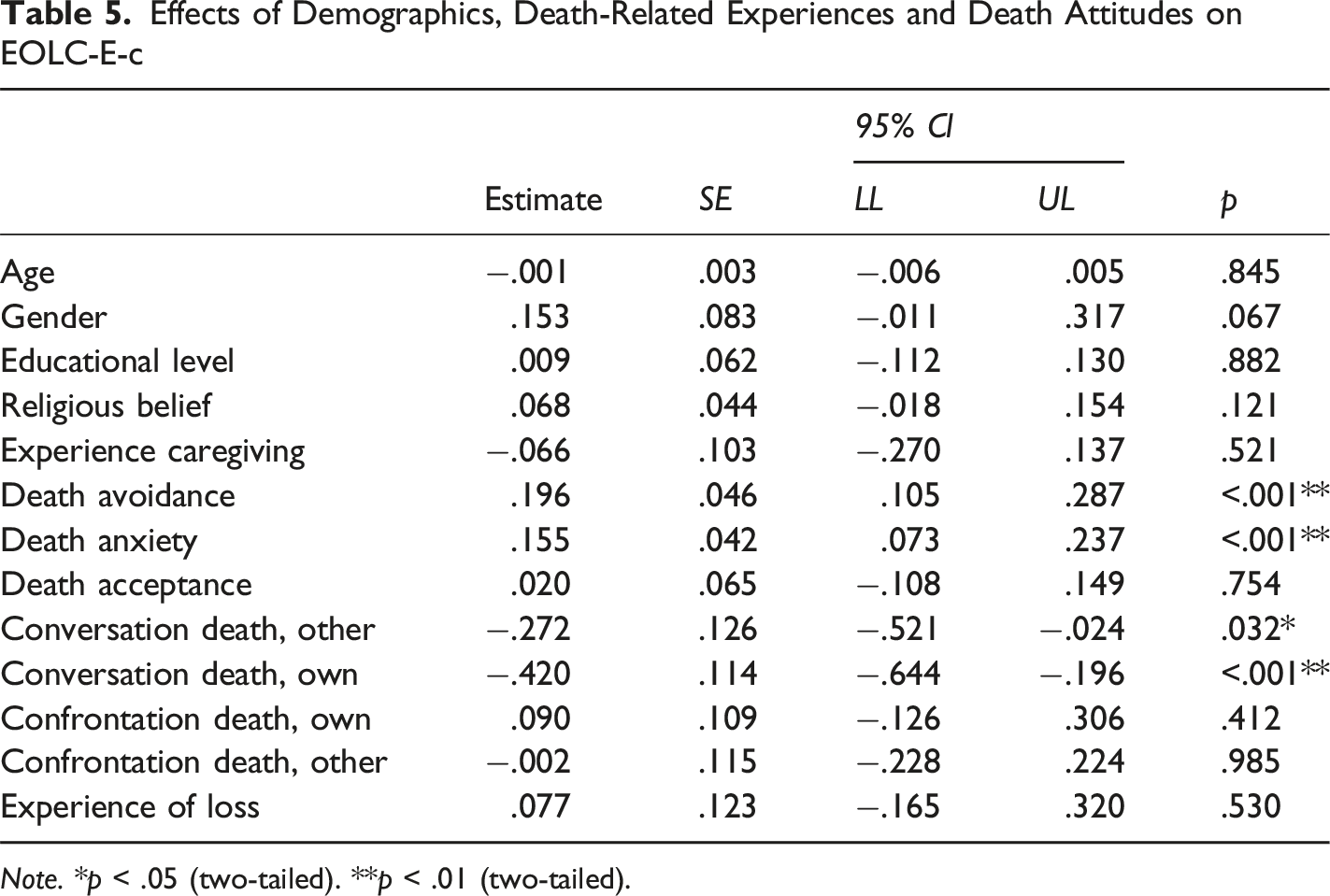
Note. *p < .05 (two-tailed). **p < .01 (two-tailed).
Reasons for the Lack of EOL Conversations
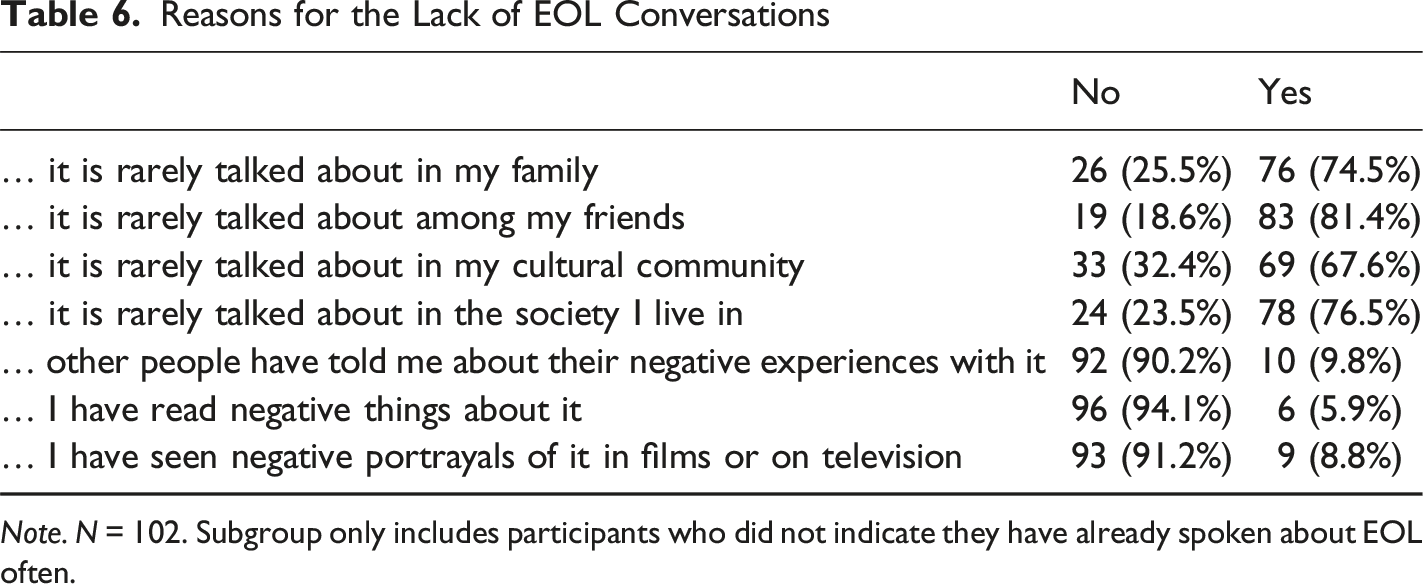
Note. N = 102. Subgroup only includes participants who did not indicate they have already spoken about EOL often.
Discussion
This study explored expectations surrounding communication about death and dying from the perspective of caregivers and validated the corresponding scale (EOLC-E-c) in a German online community sample. Most participants reported prior engagement in conversations about death. Overall, participants’ agreement lay between somewhat disagree and somewhat agree, as reflected by the average score of the EOLC-E-c scale. Agreement was highest for items referring to elicited sadness—both one’s own and that of the conversational partner—whereas disagreement was strongest for items referring to difficulties in inquiring about the conversational partner’s wishes and in displaying vulnerability.
After respecification, confirmatory factor analysis yielded support for the 20-item three-factor structure comprising: (1) expected own emotional burden, (2) expected emotional burden of the other person, and (3) communication self-efficacy. These factors underscore the shared anticipation of emotional strain for both the self and the conversation partner during EOL discussions.
Supporting its validity, the EOLC-E-c scale was positively associated with measures assessing fear of death, death avoidance, communication apprehension about death, and avoidance of conversations about death and illness. It was negatively associated with readiness for end-of-life conversations. Small correlations with depression (PHQ-2) and anxiety (GAD-2) measures support the scale’s discriminant validity, suggesting that the EOLC-E-c captures distinct constructs. Contrary to most previous findings (Bachner et al., 2021; Seifart et al., 2020; Strupp et al., 2021), the majority of participants in the current sample, reported prior engagement in EOL conversations – either about their own death or that of a significant other. This discrepancy may reflect a selection bias, as the study’s objective was transparently communicated, possibly deterring individuals who habitually avoid such conversations. A similar trend was observed in a recent Dutch study (Haaksman et al., 2024).
Interestingly, the findings suggest that mere confrontation with death (e.g., through witnessing or working around dying individuals) is not sufficient to explain interindividual differences in EOL communication expectations. Rather, prior conversations about death are associated with reduced negative expectations, suggesting that such experiences may be linked to differences in held beliefs. In contrast, confrontation without communication appears not to be associated with similar differences in expectations. These findings emphasize the communicative nature of expectation change. However, given the cross-sectional design, causal conclusions cannot be drawn. It remains unclear whether reduced negative expectations lead to more frequent EOL conversations—or whether engaging in such conversations reduces negative expectations. Longitudinal research is needed to determine the directionality of this relationship.
Participants in this study were predominantly German, highly educated and identified as either non-religious or Christian. Previous research has shown that one’s cultural background, religious beliefs, and educational level may also explain differences in the extent of EOL conversations (De Graaff et al., 2012; Piracha et al., 2024). To better understand predictors of EOL conversations and associated expectations, future studies should aim for more diverse samples in terms of culture, religion, and socioeconomic status. This is especially relevant given that participants cited sociocultural environments as barriers to engaging in EOL conversations. Understanding these barriers is essential for developing effective interventions and public education efforts. Internationally, several initiatives have emerged to promote open dialogue about death, such as festivals addressing death and grief (Endlich.menschlich, n.d.), death cafes (Miles & Corr, 2017), public health campaigns such as the “Dying to Know Day” in Australia (Proveda, n.d), and websites promoting conversations about death such as the website “Death Over Dinner” (Death Over Dinner, n.d). The latter may be particularly useful for individuals with low communication self-efficacy, as it offers conversational prompts and guidance on initiating discussions. Death Cafés, by providing informal spaces to talk about death, may help individuals confront and adjust their expectations about emotional burden and communication difficulty. Likewise, information campaigns could normalize death-related discussions and reduce avoidance by highlighting their benefits.
Several potential limitations of the current study should be acknowledged. Confirmatory factor analysis indicated an acceptable fit, however the RMSEA remained above conventional cutoffs, suggesting that future research should replicate these findings in a large sample and may consider shortening the item set to reduce redundancy. Furthermore, despite efforts to recruit a culturally diverse sample, such as recruiting during a cultural exchange evening, the sample was relatively homogenous. The German language of the questionnaire may have presented a hindrance in this regard. Future studies should replicate the study in other languages. The study validated the scale in the general population and not in an active caregiver population. Thereby limiting the direct clinical validity and generalizability of the scale for active or clinical caregiver populations. Future studies should replicate the current study with a sample of caregivers of individuals with life-limiting diseases and healthcare workers who are frequently confronted with death, in order to broaden the scope of its application.
Practical Implications
This study offers important implications for both research and practice. Investigating the underlying reasons for avoiding EOL conversations can inform future interventions and educational campaigns. Using the EOLC-E-c in conjunction with its parallel version could serve as a screening tool in clinical settings to identify individuals with high levels of negative expectations. Tailored interventions—such as cognitive restructuring—could then be implemented to reduce these expectations and facilitate EOL communication.
Conclusion
This study supports the validity and reliability of the EOLC-E-c scale in a German online community sample. The scale can be employed in both research and clinical contexts to assess expectations regarding end-of-life conversations with significant others. By identifying and addressing negative expectations, interventions can be developed to facilitate such conversations, potentially improving end-of-life experiences for both patients and caregivers.
Footnotes
Ethical Approval
Ethical Review Committee of the Department of Psychology at Philipps University of Marburg (2021-32k-Amendment), German Clinical Trials Register (DRKS00034105).
Consent to Participate
Written consent was provided.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Deutsche Forschungsgemeinschaft (DFG; German Research Foundation), project number 290878970-GRK2271, Project 10.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Upon request.
Author Biographies