
Abstract
Numerous age estimation methods in unidentified bone have been a long time developing for application in forensic anthropology. The histomorphometric technique is one of the alternative methods that relied upon the evaluation of the cortical bone microstructure over the lifespan as a result of the remodeling process in bone. Remodeling is a sophisticated event occurring from the coupled function of bone formation and resorption cells for maintaining mineral homeostasis and repairment of microdamage in bone tissue. Products derived from remodeling are primary changes in the osteon or haversian system in various regions in the cortical bone, including periosteum, endosteum, and trabecular bone. Throughout life, bone remodeling rate with osteon alteration can be predictable. In the forensic field, histological methods are getting more attention due to the unavailability of macroscopic methods. Histomorphometry approach can be accomplished in fragmentary or incomplete bone remains indicating the limited use of gross morphological methods. In addition, the microscopic methods can aid to increase the more accuracy of analyses and diminish the biased subjective assessment for determining age. Most histomorphometry method utilizes a cross-section of the midshaft of the long bones including the mandible, rib, and clavicle. This review provides the basic knowledge of bone biology and anatomy, several age-estimating methods of histology, and crucial factors for age methods. Studies regarding overall age determination methods from the past until now contribute to obtaining more benefits for developing methods of histomorphometry using human bone in forensic identification.
Introduction
Identification in forensic anthropology usually undergoes the challenge of examining the skeletal remains, especially in adult age due to the more variants than that of subadults.1,2 It is well known that the data derived from bone remains will be constructed a biological profile consisting of sex, age, ancestry, and stature. This profile can assist to narrowing in the primary identification of unidentified human cases.3,4 Focusing on age at death estimation, age is a crucial factor impacting the bone gross morphology, geometry, and microstructural compositions. Various methods depended on macroscopic,5–7 microscopic studies,8–10 biochemical methods,11,12 as well as radiology. 13 The conventional macroscopic technique has been generally used to identify when the skeletal remains are complete since this method is based on morphological changes along with the growth and degenerative processes. 14 Although the gross anatomical method is a nondestructive, quick, and simple approach to evaluation, there are still problems due to requiring the complete remains for detection to provide more reliability and reduce the error of estimated age. Since human skeletons in most cases of forensic context are usually found in fragmentary, gross morphological methods may not be available. Moreover, most techniques are qualitative evaluation that is quite substantially subjective assessment.5,14,15 The results become the progressive decrease of accuracy in older specimens making the methods high estimated errors when applying.15–17 In this such situation, histological methods may consider more beneficial. The methods have been developed using quantitative histomorphometric analyses of many bone types typically based on the remodeling process in the cortical bone. It will provide more accurate results and can be used in incomplete, eroded, or fragmentary bone remains.18–20 Data are being presented pertinent to the histological methods for age determination in human bone with regards to the biology and histology of bone, age estimation methods, and affecting factors of histomorphometry.
Bone biology and histology
Human bone is hard supporting connective tissue consisting of bone cells and bone acellular matrix. It provides a strong supporting framework of the body, protects the soft tissue and internal organs, and serves as a reservoir of mineral ions and calcium. 21 Bone is always altering along with the metabolic and mechanical processes during life. In general, the periosteum, the external surface of bone, is the outer connective tissue layer of bone, whereas the inner surface is occupied by the endosteum. The central cavity of bones, the marrow cavity, contains bone marrow where the formation of blood cells takes place. 22
Individual bone cells are composed of osteoprogenitor cells, osteoblasts, osteocytes, and osteoclasts. 23 All these cells provide the growth, remodeling, and repairment of bone. 24 Bone cells comprise the different cell types. (I) Osteoprogenitor cells are the precursors of other cells. (II) Osteoblasts, function to generate bone matrix. (III) Osteocytes, mature bone cells, differentiate from many osteoblasts enclosed by bone matrix and have a role associated with the metabolic process of bone. (IV) Osteoclasts are commonly known as resorption cells. They function as bone resorption and remodeling processes.21,22
The bone matrix has both organic and inorganic parts surrounding the bone cells. The organic matrix includes mostly dense bundles of collagen type I, glycoprotein, and proteoglycans. The inorganic part, containing about 50% of bone-dry weight, consists of high calcium hydroxyapatite and other minerals such as phosphorus, magnesium, potassium, and sodium. This part provides bone rigidity. 25
For microstructural observation of bone, histological procedures for bone tissue are applied. Generally, complete cross-sections or some area sections of bone are selected. The thin section of bone is embedded in epoxy resin and cut with a precision low-speed saw to reduce its thickness. 26 To obtain the final thin section, the section is mounted with a glass microscope slide and ground by using a Buehler Grinder-Polisher. The normal final thickness of the section is range from 50 to 100 μm. Then, it is cleaned in an ultrasonic bath, and dehydrated in 95% and 100% ethanol. Finally, the section is cleared with Histoclear and mounted with a coverslip employing a xylene-based mounting medium.27,28 To receive high-quality magnification, high power microscope is necessary for the investigation of bone microstructures. 29
Type of bone
Indeed, two main types of bone structure have been classified as mature bone (lamellar bone) and immature bone (woven bone). Based on gross observation, mature bone divides into the compact or cortical bone and cancellous or trabeculae bone. 23 Only highlighting on cortical bone. Generally, cortical bone generates bone strength. Microscopically, its characteristic is haversian system (Osteon) containing the following structures: (1) Outer circumferential lamellae are located under the periosteum and enclose the entire cortical bone; (2) Interstitial lamellae, remnants of remodeled haversian systems, are between the osteons; (3) Osteon or haversian system is several concentric lamellae enclosing the central canal. Between lamellae, there are osteocytes within lacunae. The cement line or reversal line, the layer of collagenous bundle, is the entire outer border of each osteon. Haversian canal in the central region of each osteon contains nerves and blood vessels. Each haversian canal will connect each other by the Volkmann canal 21 ; (4) Inner circumferential lamellae are the inner layer of cortical bone and adjacent to the endosteum. 24 In the period of osteon formation, the lamella nearest to the cement line will be formed firstly and other lamellae will be followed to be harversian system. Then, the thickness of osteon increases and size of haversian canal decreases.22,25 If considering bone types by shape, there are many types as long, short, flat, irregular, and sesamoid bones. Long bones are usually used in histomorphometry of age determination.30,31 Cross-section of the cortical bone histology is demonstrated in Figure 1A and 1B.
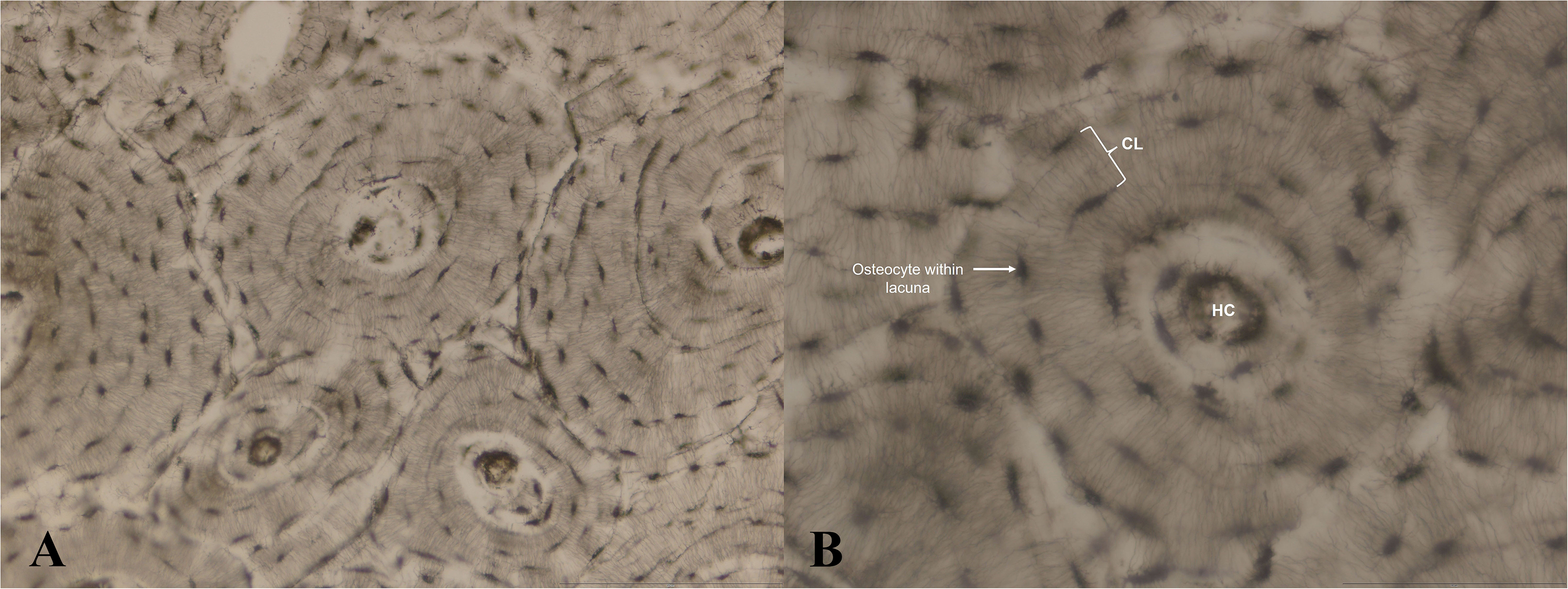
(A) Magnification at 200X, undecalcified cross section of human cortical bone illustrating various haversian systems (osteons). (B) Magnification at 400X, undecalcified cross section of human cortical bone illustrating an osteon; HC = haversian canal and CL = concentric lamellae.
Bone modeling and remodeling
Bone modeling and remodeling are associated with the formation and maintenance of the skeleton. The function of bone shaping by osteoblasts and osteoclasts during growth and development is called the modeling process. It adapts the shape and size of each bone for suitably functional bone during growth. Bone modeling will be ongoing until maturity and the modeling rate decreases later. 30 Bone remodeling (bone turnover), a complex long-life process, involves in the resorption and formation of bone without damaging bone structure. Osteoblasts and osteoclasts will work together to remove old or damaged bones and at the same time construct new bone instead. Both cell types are called the Basic Multicellular Units (BMUs).32,33 Sequence of remodeling comprises activation of bone cells, resorption of old bone, and new bone formation or replacement. The area in which osteoblasts start forming and osteoclasts stop resorbing is the reversal line (or cement line). This line is the boundary of new osteon or remodeled bone, called secondary bone.21,25 The obtained product from remodeling is an osteon (secondary osteon). This remodeling process proposes to protect bone from mechanical stress or force during life as weight changes or postural adaptation, maintain balance of vital nutrients in the body, and repair bone microdamage derived from mechanical loading.30,33–35 Apart from the cortical bone, remodeling also occurs in trabecular bone, periosteum, and endosteum at diverse times and rates.36–38 This bone remodeling throughout the lifespan with altering microstructures provides the possible evidence for histological age estimation.
Type of osteons
In the bone remodeling process, there are probably many kinds of secondary osteons as follows: (1) Primary osteons are the result of bone lamellae formation around the central canal of woven bone. They have no reversal line around them. Sometimes, the term of primary osteon refers to non-haversian canals or unremodeled bone; (2) Secondary osteons (or remodeled bone) are an important product of remodeling which can be found in many types like type I osteons, type II osteons, double-zonal osteons, and drifting osteons. Common secondary osteons used in histomorphometry methods are type I osteons; (3) Fragmented osteons are remains of primary and secondary osteons which partially resorb in remodeling.38,39
Histomorphometry based on estimating age in human bone
Long bones of the upper and lower limbs
Aging introduces significant changes in the remodeling process in bone microstructures as described above. Prior to the original establishing age determination method, researchers revealed age-associated changes in histological structures in the mid-diaphysis of the femur. 40 Bone histology had been first employed in age-at-death estimation by Kerley and colleagues in1965. Ground cross-sections of the midshaft femur, tibia, and fibula were analyzed. Their preliminary study found that the outer third of the cortex was a better relationship with aging. They investigated four parameters and found that all parameters in all bones significantly correlated with age (r = 0.79–0.97). With advancing age, osteon and fragment numbers increased while the percentage of circumferential lamellar bone decreased. Non-haversian canals number found highly in infancy and childhood and tended to decrease with age. The number of fragmented osteons in the fibula was the best correlation with age. Osteon parameters gave better values than those of the others. They also found no sex and race differences in this method. Furthermore, when applying the age equation using fragmented osteon, the estimated age was within ± 10 years. 8 After the first report in the principle of age histological method, several modification methods were developed. Ahlqvist and Damsten in1969 modified the method in the femur. Location fields were relocated between the original fields of Kerley's method. Results found that the definitions of parameters in previous Kerley's study were uncertain and confusing to examine resulting in an increase of observational errors. Some definition was too difficult to distinguish such as complete and fragmented osteons. 18
By 1970, Singh and Gunberg studied in the mandible, femur, and tibia for practical and beneficial age indicators. The results depicted that the total number of osteons (r = 0.92–0.97) and the number of lamellae per osteon increased (r = 0.89–0.95) whereas haversian canal diameter decreased with aging in all bone types (r = −0.94 to −0.97). The total number of osteons in the mandible was the best correlation relative to age with an SEE of 2.6 years. 19 Overall SEE of equations was a range in 2.6–5.0 years. Many researchers tested age estimation using Kerley's method and found considerably underestimated age from the problem of field size. Thus, Kerley and Ubelaker in 1978 recalculated the new field size. Sections of the femur, tibia, and fibular were examined by utilizing the same variables of Kerley's original method. The best accuracy was found in fibular fragmented osteons with 3.7 years of error, followed by femoral osteon fragments (SEE = 6.9), fibular intact osteons (SEE = 8.3), tibial osteon fragments (SEE = 8.4), femoral intact osteons (SEE = 9.2) and tibial intact osteons (SEE = 10.5), respectively. They suggested that it should be considered the variance in field diameter with a different microscope when using the method of Kerley and a field diameter of 1.62 mm should be applied. In addition, correction factors were recommended with the number of intact, fragmented osteons, and non-haversian canals measuring. 40 Correction factors will make an observed field size equal to the original size. Comparing the accuracy and reliability of the previous literatures,18,40 Stout and Gehlert in 1980 compared the reliability between Kerley's and Ahlqvist and Damsten methods examining in the femur, tibia, and fibula. The greatest accuracy of age determination was found using Kerley's equation of the femur. In young individuals, the variable of femoral intact osteon gave the most accuracy for age equation meanwhile, fibular osteon fragment was found the greatest in older age. 41 An earlier study by Thompson and colleagues in 1979 used the cortical bone section of the femur, tibia, ulna, and humerus for age estimation in over 50 years of individuals. The sample included 116 with the age of 30–97 years. They concluded that the percentage of osteon area was the best predictor for human age estimation. 42
Nevertheless, authors 43 reported in midshaft of the tibia in 53 specimens. Histological parameters were cortical thickness, cortical density, the number of secondary osteons, secondary osteon area and perimeter, and haversian canal perimeter quantified by the image analysis tool. The number of secondary osteons was the highest correlation with age for age estimation in beneath 55 years of individuals. They also studied the variability of black and white population and found no difference between them. This study determined age in samples less than 55 years in the tibia; however, the best variable for each age group is probably different. It may be necessary to get separately two equations for a person less and beyond the age of 55 years.
Undecalcified sections were taken from the femur in the study of Ericksen and colleagues in 1991. 9 The five fields at the edge of the periosteum were selected in all 328 samples. Results showed that all histological parameters were significantly correlated with age (r = 0.36–0.72) except for resorption space for all samples. Additionally, the percentage of unremodeled bone (r = −0.72) and non-haversian canals (r = −0.66) found a negative correlation. Osteon fragments and percentage of unremodeled bone were a high correlation. Regression equations provided mostly SEE within ±10 years. They also claimed that specific equations for each sex gave better results. The accomplished study by Yoshino and colleagues (1994) 44 developed a method using a microradiograph in the humerus. Six in all ten variables significantly correlated with increasing age, i.e., the number of osteons (r = 0.51), type II osteon (r = 0.46), low-density osteon (r = 0.41), fragmented osteon (r = 0.79), total haversian canal area (r = 0.31), and average osteon area (r = −0.33). Using stepwise regression, overall multiple R and SEE were 0.79–0.90 and 6.1–8.8 years, respectively. They also tested this method employing the same sample and found 5.1 years in mean absolute difference between actual and predicted ages.
Additionally, another study performed in Japanese population, 45 undecalcified sections of the femur were included. The femoral sections stained by Villanueva's bone staining powder and analyzed by image analysis software were applied for measuring the parameters. All variables significantly correlated with age, particularly in osteon perimeter (r = −0.84), osteon length (r = −0.83), and osteon area (r = −0.83). Besides, the number of osteons, fragmented osteons, and type II osteons demonstrated a moderate positive correlation (r = 0.65–0.74). In contrast, all variables regarding haversian canal found very low correlation, indicating that these parameters hardly did not change with aging. They analyzed both stepwise and forward methods for age prediction. In two equations, the perimeter of osteon, length of haversian canal, and osteon fragment number were commonly selected. Watanabe claimed that the SEE of this study was better than those of others since using Villanueva bone powder staining made demarcation among osteons, interstitial layer, type II, and fragmented osteons easy to investigate.
In the examination of previous research, 46 decalcified thin sections of the 29 femoral midshaft were used. The fields of each cross-section stained by Sirius red staining were analyzed using image software. With age, the number of intact and fragmented osteons increased while the percentage of lamellar bone area decreased. Authors separately determined the 4 and 20 fields in the outer third as well and found that whether 4 or 20 fields osteon number was the highest correlation with advancing age (r = 0.82 in 4 fields, r = 0.87 in 20 fields). For equations in all ages and less than 70 years, the number of fragmentary osteons was the most value of the determination coefficient (r2).
Applying age histomorphometry in Malaysian, Nor et al. in 2014 47 utilized an undecalcified section of several long bones, i.e., the humerus, radius, ulna, femur, tibia, and fibula. There were found that osteon count, osteon diameter, osteon perimeter, and osteon area showed significant correlation with age. With advancing age, the overall osteon size tended to decrease, and the number of osteons increased. The highest correlation was found in osteon diameter (r = −0.44), followed by osteon count (r = 0.40). Haversian canal variables were not significant correlation with age which was not consistent with other studies.19,48 The best equation of this study included the parameters of diameter and area of haversian canal, medullary cavity diameter, and osteon diameter with 9.7 years of error.
Chompoophuen et al. in 2019 48 developed age estimation by focusing on only area of histological variables in the femoral cortex in Thai population. Various histomorphometric variables of the decalcified section with Sirius red staining were calculated using an image processing technique. Five measurement parameters showed a significant correlation with advancing age (r = −0.345 to 0.86) excepting for fragment osteon area. The most correlation coefficient was found in haversian canal perimeter (r = 0.86), followed by the total osteon area (r = 0.72). Both of secondary osteon area and the percentage of lamellar bone area tended to decrease with age. The best predictive equation employed the perimeter of haversian canal, collagen density, and the percentage of lamellar area as age indicators was 0.91 of multiple R2 with 8.3 years of error.
According to the study of Maggio and Franklin in 2021, 49 an examination of the femoral microradiograph section was done in Australian samples. All 16 parameters were calculated in the region of interest using image J software. The finding of the relationship with age was low significant correlation of most parameters in both the anterior (r = −0.16 to −0.38) and posterior (r = 0.15 to 0.29) aspects of the femoral cortex. When considering the combined surface of the cortex, there was significant relation in six parameters (r = 0.15–0.30). Likewise, there were moderate to strong correlations between parameters and anterior, and posterior aspects including the combined surface cortex of the femur. It was notable that osteon population density increased but the size of osteon and haversian canal decreased which affirmed the relationship of the bone remodeling process and osteon dimension. Haversian canal diameter had the highest significant correlation with aging (r = 0.30) in the combined surface cortex. In the anterior area, cortical width was the most correlated with age (r = −0.38), followed by osteon fragment number (r = 0.32), haversian canal area (r = 0.29), and haversian canal diameter (r = 0.27). In the posterior aspect, osteon fragment number and OPD were the highest correlation (r = 0.29).
The ribs and clavicle
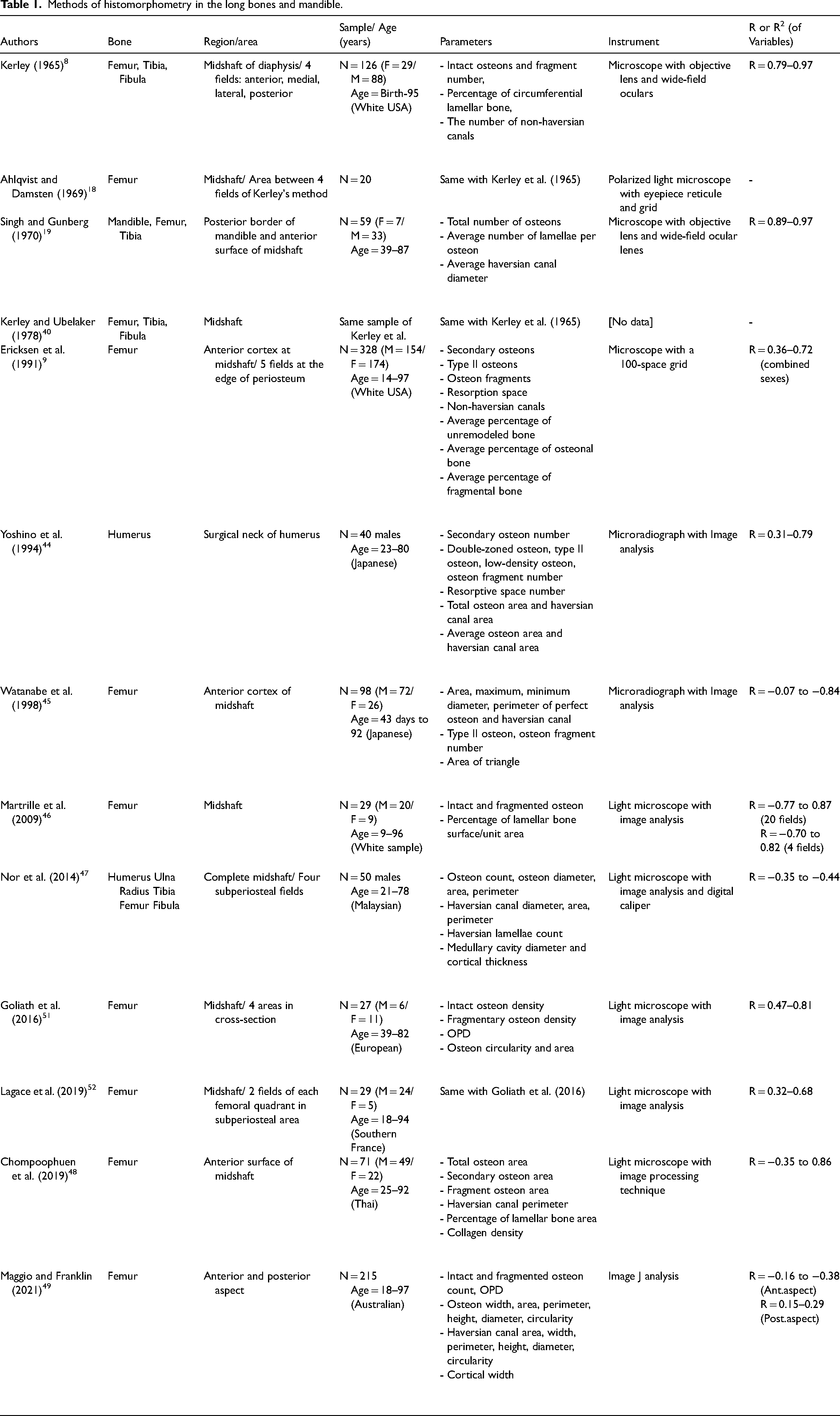
A diversity of methods developed so far had varied types of bone. Besides the long bone of the femur, tibia, fibula, humerus, radius, ulna, mandible, the rib, and clavicle were conducted for histomorphometry. Stout and Paine in 1992 10 proposed age estimation using the middle third of the 6th rib and midshaft of the clavicle. Intact and fragmented osteons were summed together in counting as total osteon density or OPD to eliminate the problem of incorrect interpretation. For testing the accuracy of this method, the differences between estimated age and actual age were −2.7 to 9 years (mean = 2.6) in the rib, −8.1 to 20.6 years (mean = 1.1) in the clavicle, and −2.5 to 14.5 years (mean = 3.4) in combined rib and clavicle equations. They suggested using the combined formula for rib and clavicle in age estimation because it gave better overall accuracy and reliability. In 2002, Cho and colleagues 50 studied in both African-American and European-American using the middle third of the 6th rib. They modified some variables from the study of Stout and Paine in 1992. All parameters correlated with age and the highest was OPD. They also found that OPD, relative cortical area (RCA) and osteon area significantly changed associated with ancestry and osteon size varied among these populations. A summary of the histomorphometric studies in various long bones and mandible is illustrated in Table 1.
Methods of histomorphometry in the long bones and mandible.
After that time, there were more studies concerning histomorphometry utilizing the rib. As a result of being low weight-bearing bone and obtaining less biomechanical stress, the rib has been considered one of the good samples for the histological method.53,54 Another investigation in rib histomorphometry by Kim et al. in 2007, 55 employed 64 specimens of the sternal end of the fourth ribs. Seven parameters were calculated using the image analysis tool. In combined sexes, parameters of OPD (r2 = 0.80), RCA (r2 = 0.10), osteon area (r2 = 0.77), and haversian canal area (r2 = 0.12) significantly correlated in a positive way with age. In separated sex, haversian canal area in males and RCA in females were not correlated. Two equations of known and unknown sexes were established using OPD and osteon area parameters. Overall multiple r2 was 0.83–0.84 and SEE was 4.8–4.9 years. Known sex equation had slightly better reliability. Interestingly, haversian canal size was unchanged with age in males but slightly decreased in females. Parameter of RCA rarely did change with age in the three groups contrary to Cho et al. 50 It may be due to the different sites of interest. They pointed out that sex was an important factor affecting the bone turnover process including menopause in women.
Absolonova et al. in 2013 56 attempted to apply in the burned (at 700 °C and 800 °C) and unburned ribs. Undecalcified sections without any staining were measured with an image analyzer. They also analyzed both internal and external sites of rib curvature and found that these two sites did not differ in microstructures. Among the three groups, haversian canal perimeter/osteon perimeter, haversian canal area/osteon area, and haversian canal diameter/osteon diameter were not different indicating that these parameters were independent of the burning effect. In unburned ribs, 19 parameters significantly correlated with age (r = −0.29 to −0.75). In burned ribs at 700 °C and 800 °C, there were significant correlations in 11 and 10 parameters, respectively. The parameters regarding the osteon dimension provided the most correlation with age in all groups. In practice, authors recommended the equation of unburned ribs in both sexes and the equation of burned ribs at 700 °C in both sex and males. It was not feasible to apply the equation of unburned bone to determine the age of burned bone.
A recent study accomplished by García-Donas et al. in 2022, 57 the histomorphometric analysis in the 6th rib in both Greek-Cypriot sample and Cretan sample was made on a microscope with image analysis. It was reported that most of the parameters significantly correlated with increasing age apart from total osteons, total area, and endosteal area. The highest correlation was found in fragmented osteon number (r = 0.78), OPD (r = 0.71), osteon perimeter (r = −0.67), and osteon circularity (r = 0.67). There was a difference between sexes, i.e., cortical area. Higher values were found in males. Considering the distinction of population, cortical area, osteon area, and osteon perimeter showed different values. Noteworthy, cortical area differed from the perspective of sex and population. The best age equation in pooled sex was 10.7 years of estimated error (R2 = 0.64) including the variables of OPD, osteon perimeter, and circularity. In the view of separate sex, the models of male and female were SEE of 10.4, and 10.8 years, respectively. Additionally, the model equation for the Greek sample, SEE of the best model was 8.1 years with R2 of 0.68. There was a considerable point regarding sex that the variable of osteon circularity had a collaboration with pooled sexes, male, and female groups. The authors suggested that it should be applied the sex-specific equation if known sex was available for providing more accuracy.
Apart from the rib, age-associated histomorphometry in the clavicle was getting more attention because the clavicle was usually found in the pattern of complete remains and had low feasibility of fragmentation and was non-weight bearing bone like the rib. Lee and Jung in 2014 58 examined the cross-section of the sternal end of the clavicle in Korean. A positive relationship between OPD and age was found (r2 = 0.58) while RCA (r2 = 0.27) and OA (r2 = 0.10) parameters expressed negative relation. For regression equation analysis, OPD and RCA were chosen for age prediction with 11.4 years of SEE.
As noted by Sobol et al. in 2015, 59 they took into account eight parameters of features of the clavicle shaft. All analyzed parameters showed a significantly positive correlation with age (r = 0.58–0.90). The highest correlated parameter was the average diameter of the haversian canals (r = 0.90), followed by the number of osteons with the haversian canal diameter of more than 70 μm (r = 0.87), percent of osteons with a diameter > 70 μm (r = 0.87), percent area of interstitial lamellae (r = 0.86), and the percent area of fragmented osteons (r = 0.85) indicating the crucial age predictors. The equation of this study showed 7.7 years of SEE when using an average diameter of haversian canals as an age indicator. They stated that the clavicular shaft was suitable for age histomorphometry because it was not as loaded mechanically as other long bones. The clavicle shaft only derived mechanical force from the subclavius muscle. 60
With regards to another clavicle method, Kranioti and colleagues in 2020 61 performed in modern Balkan utilizing the clavicle. In relation to aging, six parameters showed a positively significant correlation (r = 0.42–0.78) with the exception of cortical area and RCA that was a negative correlation. The OPD was the highest positive relationship with age (r = 0.78). As predicted, simple linear regression using the OPD indicator provided the best SEE of 8.3 years. Additionally, they also applied three formulae of the previous published studies10,58,62 to this Balkan sample. Their results showed underestimated age with a mean error over 20 years in all formulae. When comparing mean OPD among various population, there found the significant difference in the age of less than 20, 20–29, and 40–49 years but the age of 50–59 years did not differ. This finding concentrated on requiring of specific population equation for histological age estimation.
Combined the long bone and ribs
However, an interesting study developed a method in both the femur and rib, Goliath et al. in 2016 51 determined the potential impact of osteon shape (circularity) and size on the histological age method. The samples of European were collected to get undecalcified thin sections of the femur and rib. Statistically significant correlations with age were found in OPD, osteon area, and osteon circularity in both the femur and rib. The circularity of osteon gave the most correlation (r = 0.81) in either bone. Osteon area was found decrease with increasing age in contrast to OPD and osteon circularity. When comparing the same variables in the femur and rib, osteon circularity and OPD not differed but osteon area significantly differed. The size of osteons in the rib was smaller than those of the femur. Interestingly, there was a low correlation between sex and osteon area in the rib. The combined rib and femur formula provided the best predictive model in this study with a SEE of 5.6 years.
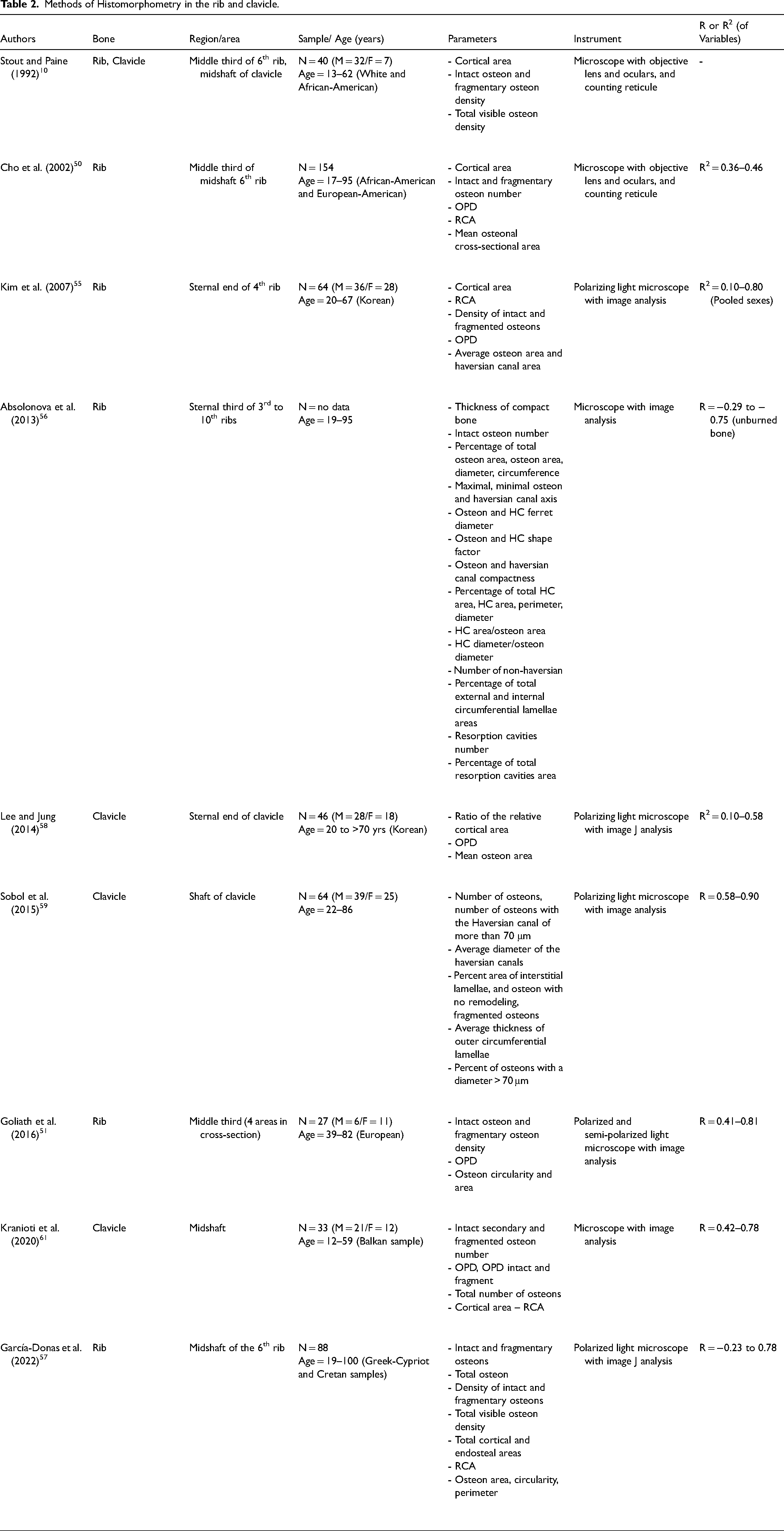
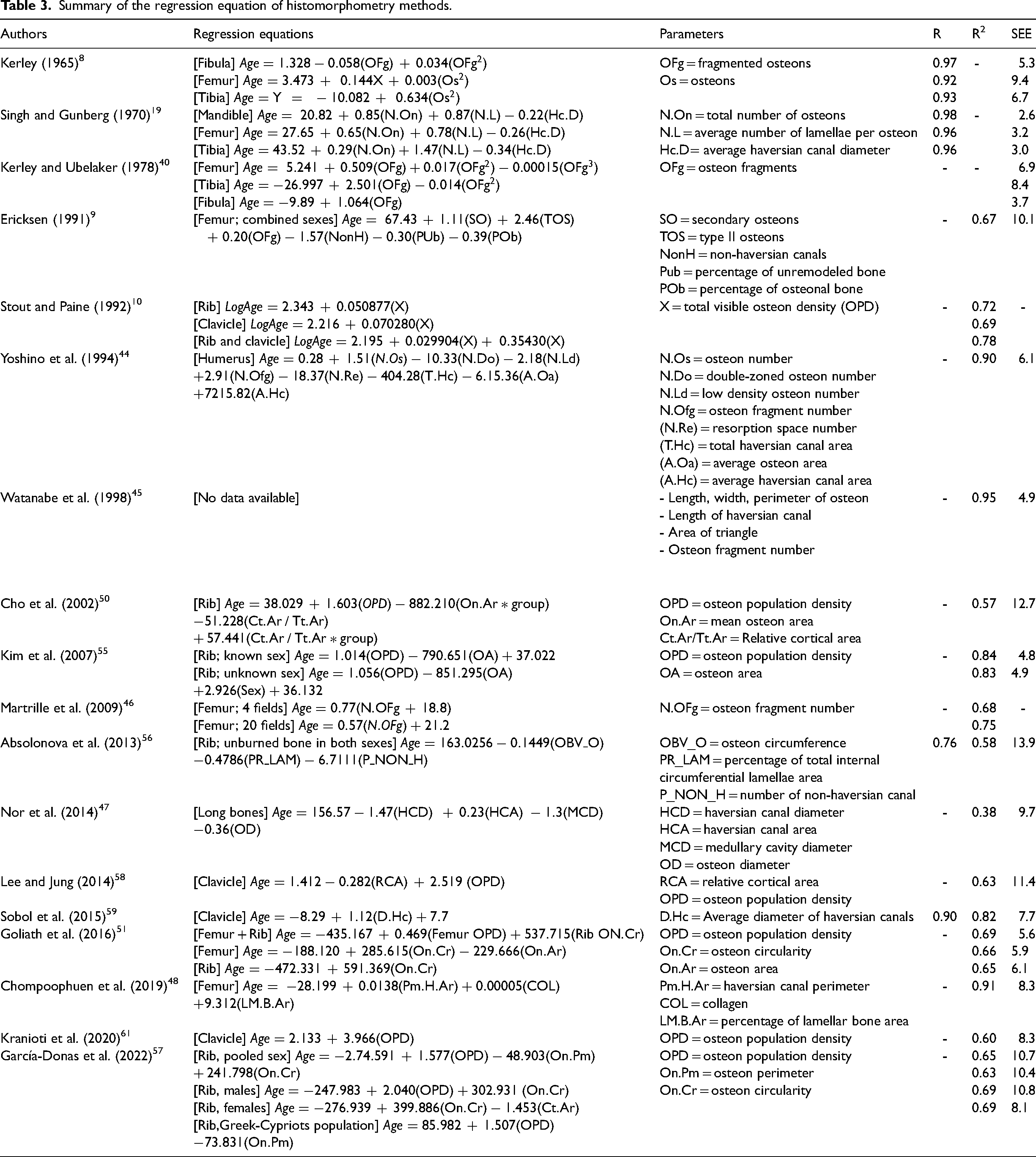
After that, Lagace et al. in 2019 52 evaluated the method of Goliath's study in Southern France. Decalcified sections with Sirius red staining of the 29 femoral midshaft were used to study. Two fields in the subperiosteal area of each femoral quadrant were observed the osteon variables using the image tool. With increasing age, an increase of OPD and osteon circular shape and a decrease in the size of osteon were found. The OPD had the highest relationship with age (r = 0.68) considerably contradicted to the original study of Goliath et al. (2016). In this study, the circularity of osteon was the lowest relative value (r = 0.32). For testing intra-inter observers, good agreement in the osteon area and OPD was depicted. They recommended that osteon circularity might not a good parameter for age determination resulting from low repeatability. When applying Goliath's formula, only 13% of all samples in this study showed accurate results, indicating the possible influence of a specific population. Moreover, the different preparation methods and age of samples contributed to obtaining different accurate results. Summary of histomorphometry studies using the rib and clavicle demonstrates as Table 2 and Table 3 provide the overall formulae using histomorphometry for age estimation in human bone.
Methods of Histomorphometry in the rib and clavicle.
Summary of the regression equation of histomorphometry methods.
In accordance with the early literatures, histological methods mostly employed the midshaft of the diaphysis of the long bones particularly in the femur resulting from age-associated changes, a durable bone from the well-preserved condition, and a good representative of compact bone structure.47,63 Even if the femur was widely used, its correlation with age did not always get the most. Sometimes the parameters of the mandible and fibula were obtained by far the highest correlations. Considering all histomorphometric variables from an estimation of age at death methods, in the long bones, mandible, clavicle, and rib, the variables relative to the number of osteons i.e., intact osteon, fragmented osteon, and OPD including osteon geometry (osteon area, osteon perimeter, and osteon diameter) achieved evidently high correlation with increasing age. Moreover, haversian canal geometry as well as interstitial lamellar also correlated. Noteworthy, most of osteon dimensions, cortical area, and the percentage of lamellar bone area decreased with age, whereas osteon number increased. Haversian canal dimensions were still controversial results. These progressive changes gave evidence of the bone remodeling process occurring in the compact bone. In consequence of the different bone remodeling rates of human, the different bone types will provide a variety of accurate methods. So, the histomorphometric study should be examined in various bones. 58
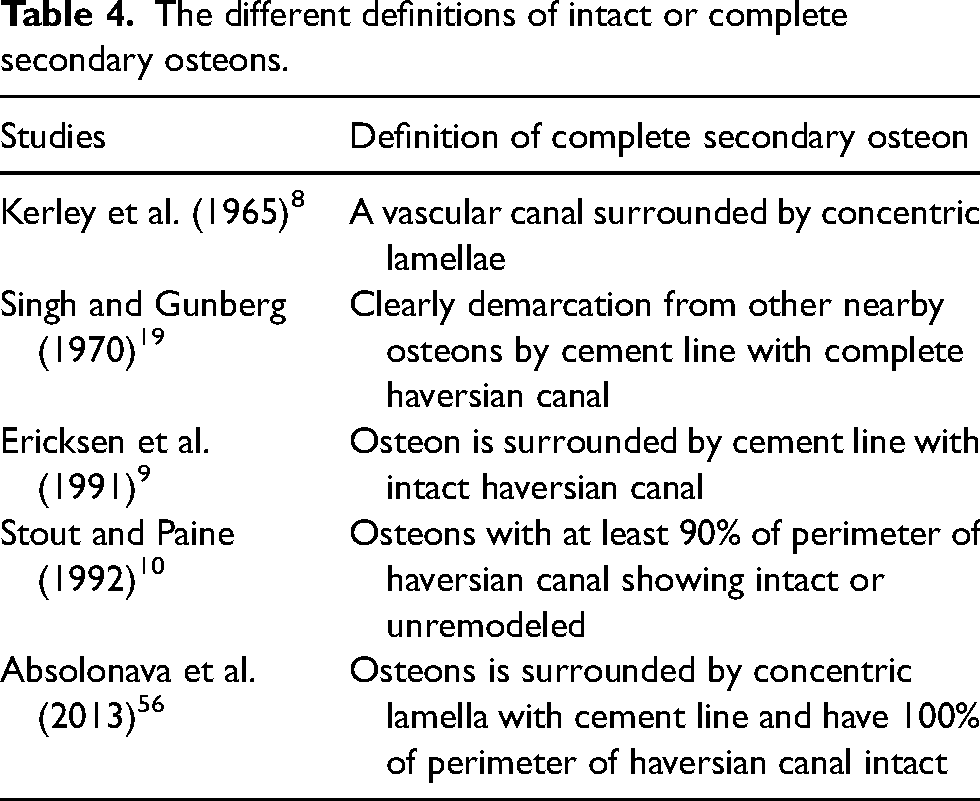
As the previous studies included in this review, the most correlation related to age was found in fragmented osteons in the mandible, followed by the number of intact osteons in the fibula.8,19 Precise definitions defined of histological parameters are one of the important points affecting the accuracy and reliability of the age estimation method specifically intact or complete secondary osteon and osteon fragments. These osteons parameters had moderate to strong correlation with advancing age in most literatures thus, the different definitions will probably get variability of accurate results. The difference in complete secondary osteon definitions is demonstrated in Table 4. Descriptive terms of some research gave confusing interpretations for observers. Thereby, for osteons, the sum of complete and fragmented osteons into osteon population density (OPD) should be used instead of separate osteon types to minimize the error problem. Almost all methods had similar osteon density and osteon metrics including within age predictive formulae indicating the vital association with age. However, in some studies, OPD parameter did not selected as one of the indicators in the age formula although its correlation coefficient was high. In intra–inter observer tests, good agreement in OPD was obviously found. 52 Suggesting that assembling OPD parameter for age prediction may increase the accuracy and reproducibility of the method. The study of Nor et al. 47 determined the various long bones and found low correlations between age and osteon count and osteon diameter. It might be due to none of the separate bone type analyses. Changes in other histomorphometric variables related to age had clear definitions making good interpretation.
The different definitions of intact or complete secondary osteons.
With regards to the haversian canal parameters in this review, controversial findings were found. In the mandible, femur, and tibia, haversian canal diameter decreased with age 19 while another study in the femur found increasing. 49 For haversian canal perimeter, it showed a positive correlation with age.48,49 In the rib, some studies found very low significant correlation in haversian canal area but, another found not indicating the variant of haversian canal area that seemed to be no correlation with age.55,56 The diameter and perimeter of haversian canals decreased with aging. 56 In the clavicle, the diameter of haversian canal found a high positive correlation (r = 0.90). 59 However, there were few studies found that the dimension of haversian canal had no correlation with age.44,45,47 The obtained different results may be due to the different kinds of bone and site. Additionally, the parameter of osteon circularity was still controversial in inaccurate results and observer error agreement as well thus, it may be gotten more further evaluation. Histomorphometric variables are shown in Figures 2 and 3.
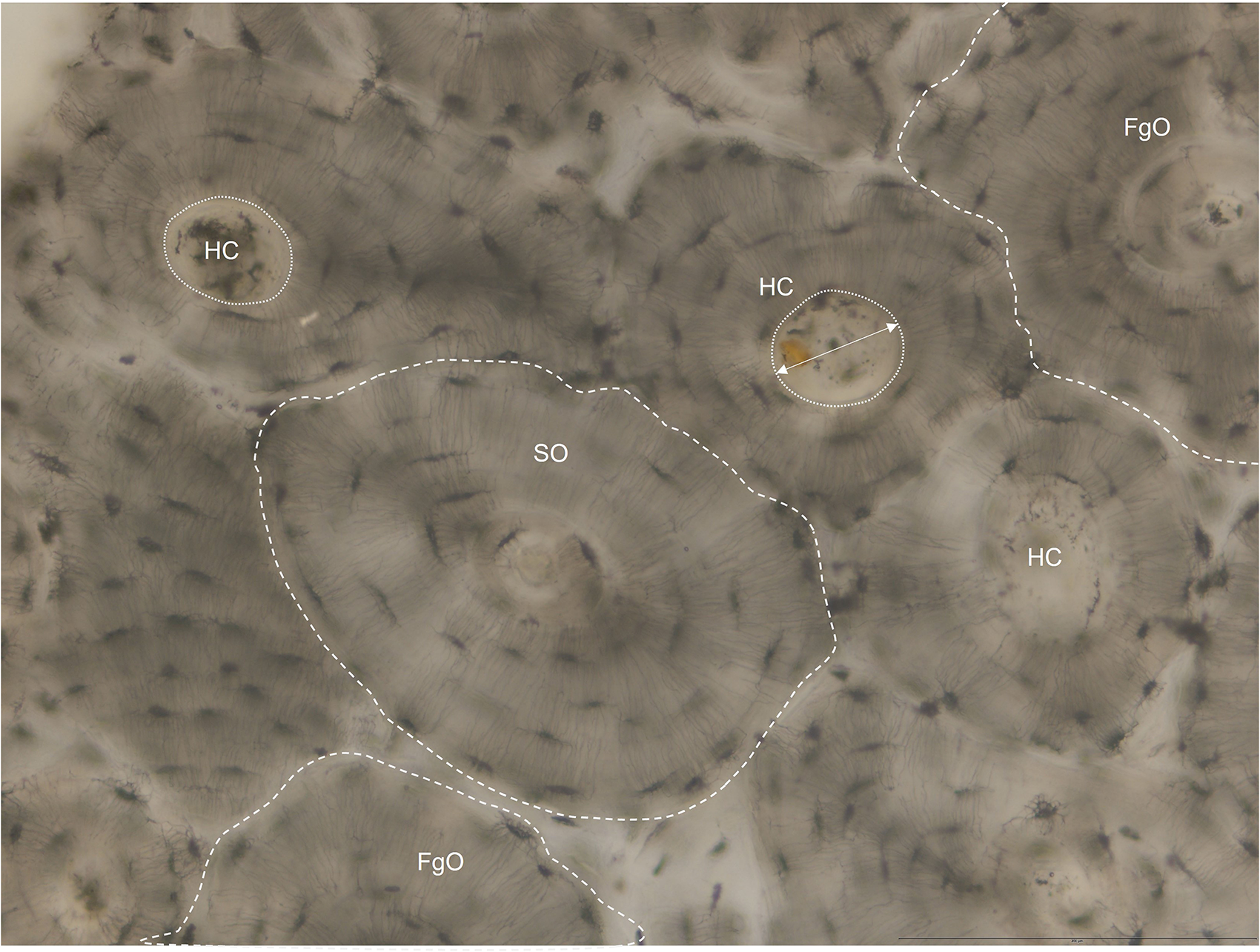
Undecalcified cross section of human cortical bone showing histomorphometric variables; SO = secondary osteon, FgO = fragmented osteon, HC = haversian canal, dashed line = boundary of osteon area, two-way arrow = diameter of haversian canal, and dotted line = perimeter of haversian canal.
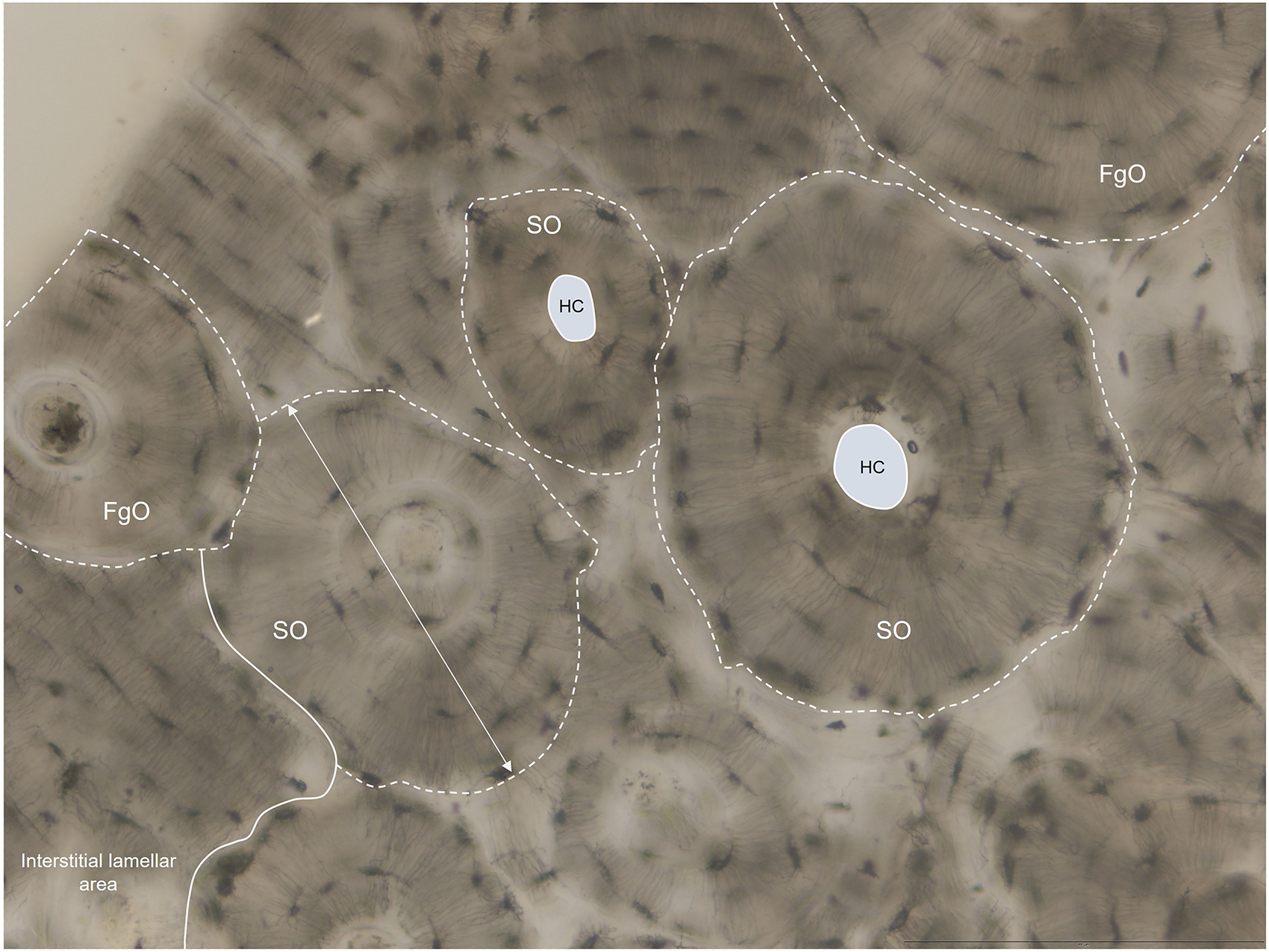
Undecalcified cross section of human cortical bone showing histomorphometric variables; SO = secondary osteon, FgO = fragmented osteon, dash line = boundary of osteon area, two-way arrow = diameter of secondary osteon, HC = haversian canal, and opaque circle area = area of haversian canal.
Among the variability of SEE for age formulae, as predicted, the histomorphometry using the mandible found the least of 2.5 years of SEE. Unfortunately, there was no additional study on this bone. Most histological methods provided the SEE values within less than 10 years,8,19,40,44,45,47,48,51,55,59,61 indicating the possible application of bone histomorphometry. The highest SEE was 13.9 years which was found in the rib. 56 The difference between sex and population in the histomorphometry approach or variables was still a contradiction. Some researchers reported that there was no difference between sex and population,8,43 meanwhile lots of studies stated that separated sex provided better results.9,56,57 Moreover, the specific population equation was still needed.50,61,64
Initial time in the past, utilizing human bones in the age histological estimation method, used simple instruments such as a light microscope with gridded-eyepiece, reticules, or ocular lens for quantitative data acquisition. Counting and calculation of histomorphometry applied with the use of the manually direct microscope. Until the present time, there was more use of semi-automated methods using image analysis software along with a microscope. This method also contributed to avoiding variation in different brands of microscope and eyepiece. Nevertheless, the advantages of the computer-assisted tool are substantially apparent because of obtaining more precise or accurate results, reducing the amount of analysis time, and more convenience.46,56 Besides the equipment used, the preparation method of the bone section is important as well. Applying staining techniques with sections is useful such as Sirius red staining. This staining provides easily differentiated between osteons and surrounding structures like lamellar bone.46,48,52
Throughout life, the aging process affects the histological variations of the bone. The difference between age groups was distinctively found. In childhood, the circumferential lamellar bone area, the number of non-haversian canals, was high. 8 There was no illustration of the perfect structure of osteons. It can be seen in adolescents. There were many primary osteons in childhood and were replaced by secondary osteons when grow up. The number of osteons was low. 45 Size of osteons such as osteon area, perimeter, diameter, and was large.45,51 In adult age, non-haversian canal numbers and the circumferential lamellar bone area decreased. 8 The number of secondary and fragmented osteons was high density8,46,47,58 Osteon sizes were smaller and more circular shape in adult age.47,51,58 For haversian canal, some studies found that size of haversian canal was associated with osteon size which had small size in adult. 49
Although the long bones like the fibula, tibia, and femur provided clear and suitable features of cortical bone, they were substantially weight-bearing bones and physical activities also influenced them. 65 Meanwhile the ribs and clavicle underwent slightly weight-bearing loads, resulting in reducing the effect on the remodeling process. 53 They were good alternatives for histomorphometry even if they did not provide the best accuracy. When studying in various populations, there was definitely found different outcomes. Variability of inter-population was common because of the different genetics, physical daily activities, and nutrients. 66 However this topic is still a discrepancy in histomorphometric methods, investigation of the population specificity has been a vital target in further study. The determination of age estimation using many kinds of bone within the same sample may minimize the influence of a specific population. In addition, the observer's experience was substantially important to be considered. As mentioned above, some definitions of histological features provided misunderstanding interpretation. Adaptation of histomorphometric variables to own population will be good for improving the error of estimation. In addition, it is noted that the histomorphometric technique is suitable for incomplete, fragmented, and eroded bone remains which can use only some parts of the bone. If well-preserved or complete bone remains were found in autopsy or forensic cases, the gross morphological methods may be better to apply.
Affecting factors on the histomorphometric method
Abundant additional factors are probably influential to the application of age predictive methods such as bone types, sex, population, pathological condition, and physical activity. In addition, nutrition, sample size, and method also affect the accuracy of histomorphometric method.57,65
First, mechanical loading from life physical activities can be affected by the bone remodeling process. The long bones are primary weight-bearing bone responding to mechanical variations. It affects the bone remodeling process and the accuracy of the age estimation method later. 65 Furthermore, exercise can increase bone mass which responds to mechanical strain. 61 Rib and clavicle are slightly weight-bearing bones and obtain less concerning biomechanical stress contributing to mineral changes in bone.53,54 When observed histological features in cross-section, part of bone exposing little strain provided smaller number of osteons. 60 Additionally, smaller size of osteons was found in the region of greater strains. 67
Second, sexual differences also affect the bone remodeling rate increasing this rate in women with initial menopause condition. Menopause will accelerate the activity of bone cells in remodeling process that affect to worsen the loss of bone. 68 Moreover, there was a difference occurring in approximately 73% of those over 50 years in females, indicating due to menopause conditions concerned with bone loss and osteoporosis.51,57 Some variables differed between males and females as the cortical area which greater values found in males. 57 Burr et al. reported that secondary osteons in older females were larger sizes than those of males. 69 Another supportive study found the difference in accumulation of osteons between sex. It was observed that in females there was gathering intact osteons until the 6th decade, while accumulated until 10th decade in males. 70 Third, regarding variations in population, several studies claimed that a specific age equation for a specific population was necessary since there were different remodeling rates in any population providing an increase of more errors.52,57,61,64 Some parameters like cortical area, osteon perimeter differ among population. 57 Pfeiffer et al. employed a study in European-American and African-American 50 to South African population. They found osteon area was smaller in the White group. However, until now there is not clear evidence for sex-specific population for histomorphometric methods.
Fourth, the types of bone and locations, the femoral midshaft was widely used in age estimation by histomorphometry since it was easily identifiable, well-preserved from burial events, and showed an evidence of bone remodeling.8,9,18,19,42 Each bone has a different remodeling rate resulting in obtaining various accuracies when using the different bone types.43,58,71 There was reporting that the posterior anatomical surface of the femoral cortex had more variation than that of the anterior surface. 72 Pfeiffer et al. 73 stated that in the ribs the average osteonal area was smaller than that of the femur. They supposed that size of bone directly altered with osteon size.
Lastly, in pathological conditions, an excessive amount of parathyroid makes increasing in osteon activation affecting the accuracy of age method. 66 Metabolic disease, trauma, and inflammation can affect the metabolism of bone and the reliability of the age prediction method later. 8 Abnormal conditions would be disrupted the histological structures of bone. For example, in Paget's diseases, an excessive number of osteons was detected. 8 In osteogenesis imperfecta, there was obviously increase in the number of osteons resulting in overestimated age. 74
Future direction
Histological quantitative assessment associated with age changes can be investigated using histomorphometry obtained from the product of the remodeling process in bone overtime of life. Changes in both complete and fragmentary secondary osteons are fundamentally important variables related to aging. Secondary osteon counts and dimensions, including the percentage of lamellar bone, and sometimes haversian canal metrics show a correlation with increasing age. Initially, almost all previous research commonly employed manual microscope analyses directly with additional equipment and then used an image analysis system for data acquisition. Nowadays, it is well known that imaging technologies have substantially crucial tools in various fields, particularly in the medical field. The neural network parted of artificial intelligence have been far-reaching use in various classification tasks. In future research, the likelihood of utilizing the deep learning function for establishing the automated age estimation software is getting more attention for improving and developing histological methods in human bone. This automatic age method using bone histomorphometry provides ease, more accuracy of analyses, saving time, good working with numerous parameters, good accuracy of prediction, a decrease of bias subjective evaluation, and good dealing with non-linear information. The automated method will provide more benefits for forensic pathologists for more accuracy, and convenience of data interpretation. However, the study of age-dependent changes of the clavicle and rib or combined with the long bones using the automated age estimation software is interesting and there are very few researches focused on them. The rib and clavicle are small bones that can observe in the whole cross-section. These bones are one of the useful alternative methods when other long bones are not available. The previous study using the combined femur and rib examined only osteon variables. Some variables of haversian canal dimensions, e.g., haversian canal diameter, perimeter, and area including the percentage of lamellar bone did not quantify. Additionally, age estimation in both males and females and specific population also is needed to further investigate.
Conclusion
In consequence of the bone remodeling process, microscopic structures in human bone change associated with advancing age. This remodeling can occur in variable sites of bone, especially in the cortical bone. As regards gradual aging, the number of complete and fragmentary osteons, osteon population density, osteon dimensions, and the percentage of lamellar bone, including haversian canal metrics illustrated correlated changes. Evaluation concerning detailed microscopic features deriving from the product of bone remodeling is crucial for developing and applying the age estimation method in the forensic context. Most of the histological formulae provided the error less than 10 years using the various types of long bones, i.e., the femur, tibia, fibula, humerus, radius, ulna, mandible, rib, and clavicle, indicating employing them as age indicators in histomorphometry.
Footnotes
Acknowledgments
The authors are appreciative of the Excellence of the Osteology Research and Training Center (ORTC) for their assistance, which was partly upheld by Chiang Mai University.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Excellence Center in Osteology Research and Training Center (ORTC), Chiang Mai University, Chiang Mai, 50200, Thailand.