
Abstract
Forensic estimation of biological age is essential as routine forensic practice, especially in cases of mass disaster, and illegal immigration to countries. Criminal, civil, and other legal cases claim determination of age. Modified Cameriere’s approach applied to estimate sex on the German population showed quite low predictive value. Fifty-two pelvic radiographs of the eastern Indian population from both genders of age between 18 and 25 years were evaluated. The area of iliac crest radiographs was measured and a linear regression model was established. The model for male patients explained 25% of the total variance (R2 = 0.25 males); whereas, only 15% (R2 = 0.15) in females. The predictive value of this model was compared with others, and the cause of low statistical validity was explained. However, this is the first of its kind study conducted on the Asiatic population and needs to be replicated on a larger sample size.
Abbreviation
ICA: iliac crest area; IW: iliac wing.
Introduction
Forensic estimation of chronological age is essential for the purpose of human identification in case of mass disaster, or illegal immigration to countries. In criminal, civil and other cases of legal purpose determination of age threshold is a pre-requisite. 1
Cameriere et al. introduced forensic age diagnostics between 2006 and 2009, by means of area measurements from the apposition of secondary dentine (dental radiographs) and ossification of carpal skeleton (wrist radiographs).2–7 Thus biological age could be determined as a linear function of different ratios, for example, an area ratio of root pulp to tooth; and mineralized bone centers to carpal bones. 7
Wittschieber et al. (2013) modified Cameriere’s approach toward a different skeletal landmark, iliac crest apophysis (ICA). 7 Authors claimed that the said region due to its late completion of maturation during human development can be a good predictor for determination of chronological age. 7
The aim of the present study was to investigate whether the modified Cameriere’s approach can be applied in sex estimation from an area of pelvic radiographs on the East Indian population.
Materials and Method
One hundred twenty-seven pelvic radiographs of the eastern Indian population from both genders of age between 18 and 25 years were evaluated. The radiographs were taken during an emergency diagnosis at Calcutta National Medical College, Kolkata between periods December 2021 and June 2022.
Pelvic radiographs were done in standard procedure, patient lying, anterior/posterior path of rays. Approximately 75 kV was used with a digital luminescence radiography system. Radiographs having projection artifacts, fractures, and superimposition of foreign material or with intestinal loops were excluded. Image evaluations were done at standard picture archiving with a communication system (PACS) workstation using software: GE Centricity RIS-I 4.2 plus.
Area Measurements
Analogically area ratios were determined consisting of the ICA and IW, in order to access degree of apophyseal iliac crest ossification. First, the iliac crest is identified. Subsequently, the ossification centers of ICA were defined by manual segmentation in order to obtain the area (in millimeters) of ICA.
Second, the area of IW was measured. The upper rim of the iliac bone was defined, beginning from the angular point of the lateral convexity of the iliac bone and ending at the medial point where the iliac wing projection crosses the sacral bone. Both points were connected to close the area, as semi-circular.
Finally, the ratio between the area of the iliac crest apophysis and the area of the iliac wing was calculated by linear regression equation.
Statistical Analyses
In order to find out the relation between age and ICA/IW ratio, linear regression models were calculated. Age was the dependent variable. Intra-class correlation coefficients were determined to evaluate inter and intra-observer reliability.
Results
Of 127 pelvic radiographs, the area of an ICA could be determined in 52 cases (30 males and 22 females) at least on one side. In 40 cases, projection artifacts, fractures and superimposition of foreign material or intestinal loops prevented area measurements. In 35 of the 127 cases, ICA was not assessable because it was not ossified yet, or it was already in the final stage of complete fusion with the iliac bone. No statistically significant differences were found between the right and left pelvic sides (P = .142). Hence, in the following paragraphs, only the right pelvic side is regarded.
The regression models, describing age as a linear function of percentage, yielded the following equations for the ICA/IW ratio:
Males: Age = 11.563+22.352× (ICA/IW) based on 30 cases; Females: Age =15.632+14.963× (ICA/IW) based on 22 cases.
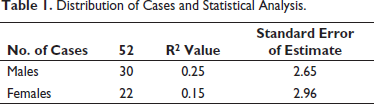
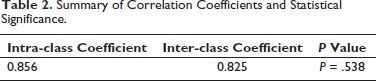
The model for male patients explained 25% of the total variance (R2 = 0.25 males); whereas, only 15% (R2 = 0.15) in females. The standard error of the estimate is 2.65 years in males and 2.96 years in females. Differences between males and females were not statistically significant (P = .538). Calculation of intra-class correlation coefficients revealed good agreements intra and inter-observer agreement (0.856 and 0.825, respectively). A summary of the results is shown in Tables 1 and 2.
Distribution of Cases and Statistical Analysis.
Summary of Correlation Coefficients and Statistical Significance.
Discussion
The present study is based on the area measurements following the method applied by Cameriere et al.2, 5 and modified for pelvic radiographs by Wittschieber et al. (2013), 7 the ratio of iliac crest apophysis and iliac wing to generate a linear regression equation. 7
For males, only 25% of the total variance can be explained by the regression model. For females, it is only for 15%, which shows that the correlation between subjects’ chronological age to the ratio of ICA/IW is very poor (R2 = 0.25 in males; R2 = 0.15 in females). The limiting aspect of this model for the eastern Indian population is practically not approachable for forensic diagnosis of age.
A similar study, by Wittschieber et al. (2013) on the German population; showed 38% (R2 = 0.38) of total variance is explained by the model for male subjects, compared to only 20% (R2 = 0.20) for females. 7 The standard error of estimate is 2.00 years in females, and 1.91 years in males. The study was conducted on pelvic radiographs (N = 102, males = 52, females = 50). 7
Another study by Bartolini et al. (2018), showed a moderate correlation with age in young Italian adults (N = 497 pelvic radiographs; age groups 10 and 25 years), and the method may be applied as a supplementary tool for ≤14 years of age to complement its forensic requirements. 8
Other studies conducted on apophyseal ossification of iliac crest to the forensic estimation of age, from radiographic examination show a wide spectrum of variation, low to moderate and up to par.9–12 However, population-based further studies are claimed to ascertain the reproducibility of the method toward better forensic diagnosis.
Showing the Area Measurements by Cameriere’s Method in Pelvic Radiograph (Area Outlined with Yellow Color).

Conclusion
As seen from the study, of pelvic radiographs done by modified Cameriere’s method for measurements of iliac crest area it was found that the predictive value in the Indian model was lower than the study done on German subjects by similar methods (Figure 1), but in either case the predictive value continued to be quite low which makes this difficult to be used as a single test in practical forensic investigation and practice. However, it can be used as an adjunctive technique to augment the results obtained by conventional methods. Therefore, we propose from this study that the method if used on larger samples in multicenter studies, can probably improve its chances of being considered as a standalone test which can be useful to forensic application. However, a certain degree of reservation has to be kept in mind while applying this test under present circumstances. This is the first study of its kind on the Asiatic population and thus is the first point of comparison with European counterparts which lends special significance to its conduct.
Footnotes
Author’s Contribution
Soumeek Chowdhuri: Origin of concept, data analyses, editing of manuscript. Biswajit Sukul: Editing of manuscript. Debraj Acharya: Data collection. Somasish Ghosal: Literature survey, manuscript writing. All authors approved the final draft of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
The study was conducted after taking ethics approval from Institutional Ethics Committee Calcutta National Medical College.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.