
Abstract
The ischaemic button model is frequently used for the induction of adhesions in laboratory rats. Male rats are often used because of the common belief that the peritesticular (intra-abdominal) fat in males facilitates adhesion formation, although this theory is not evidence based. Comparing the model’s performance in both sexes is an important aspect of refining animal experiments. The aim of this study is to compare baseline performance of the modified ischaemic button model in both male and female rats. Follow-up was 1 week and noted endpoints were intra-abdominal adhesion formation and differences in welfare assessment. A total of 192 ischaemic buttons (96 male/96 female) were created in 24 Wistar Han rats (12 male/12 female). After 1 week of follow-up, 93 buttons survived in the male group (96.9%) compared with 91 in the female group (94.8%) (p = 0.409). In the male group, 85 out of 93 (91.4%) buttons induced adhesions compared with 84 out of 91 (92.3%) in the female group (p = 0.881). All but one animal had a Zühlke score of 3. There were no clinically relevant differences in welfare scores. Male animals increased in weight significantly faster compared to females (p < 0.001), after correcting for physiological growth. The ischaemic button model resulted in equal quality and quantity of intra-abdominal adhesions in both male and female Wistar Han rats. Both male and female Wistar Han rats are suitable for the induction of experimental adhesions in the ischaemic button model.
Intra-abdominal postoperative adhesions are fibrotic connections between intra-abdominal organs and structures that are normally unconnected. 1 The adhesions are the results of a pathological healing following inflammation of the peritoneum and occur after nearly 100% of all intra-abdominal surgical procedures.2,3 Approximately 5–18% of the adhesions will become clinically relevant and cause intestinal obstruction, infertility or chronic abdominal pain.1,4,5 Because of the vast number of intra-abdominal procedures performed every year, intra-abdominal adhesions pose a billion dollar burden on the global health care system.1,3–7 As a consequence, the development and evaluation of anti-adhesive components is a large industry that depends heavily on the use of experimental animal models that provide a consistent induction of experimental adhesions. The ischaemic button model is one of the most frequently used animal models for experimental adhesions. In short, the technique uses a suture tied around a 5 mm portion of the parietal peritoneum. Subsequently, the ligated tissue becomes ischaemic, resulting in the development of an adhesion. The original model described by Buckenmaier et al. is susceptible to failure of the buttons, due to slipping of the sutures. 8 In an attempt to improve the original technique, Rajab et al. introduced a modified ischaemic button model in 2010. 9 Rajab et al. improved the model by introducing a backstitch ligature to reduce the number of slipped sutures and create durable ischaemic buttons. In their validation article they compared the modified ischaemic button model to the original model and found a lower percentage of button obliteration in the modified ischaemic button model (18.8% vs 3.8%). 9 Since the introduction of the modified technique, it has been applied multiple times in both male and female rats in several studies. The majority of studies concern male rats, possibly because they potentially have larger fat depositions in the lower body, their epidydimal or peritesticular fat. Despite the frequent use of the ischaemic button model in animal experiments, a comparison in baseline performance between male and female rats has never been performed. Comparing baseline performance between both sexes is an important aspect of refining animal experiments and provides evidence-based data regarding the number and sex of the animals included in future research. The aim of this study is to compare baseline performance of the modified ischaemic button model in both male and female Wistar Han rats.
Methods
Before commencement of this study, ethical approval was obtained from the Dutch Central Committee of Animal Experiments and from the institutional review board of the Maastricht University Medical Centre, Animal Ethical Committee and Inspection for Animal Welfare (licence no. AVD107002016720). This study was performed according to the European Convention for the Protection of Vertebrate Animals used for Experimental and other Scientific Purposes (European Treaty Series (ETS) no. 123).
Twenty-four adult Wistar Han rats (12 males/12 females) aged 8 weeks (weight range: male 200–250 g, female 150–175 g) and bred by Charles River Laboratories (Sulzfeld, Germany) were socially housed in an EU type IV Macrolon cage of 1800 cm2, with cage enrichment in the form of a cardboard cylinder and a wooden block at the centralised animal experiments facility of the Maastricht University Medical Centre (Maastricht, The Netherlands). Rooms were fitted with an artificial 12-hour light/dark cycle, room temperature was standardised at 25℃ and food and water were provided ad libitum in the form of sterilised compressed food pellets (10 mm Sniff rat/mouse maintenance food) and acidified drinking water. All animals were followed for 7 days before being euthanised under general anaesthesia via cardiac puncture.
Procedure
All operations were performed by two surgeons (EHHM and LH) certified for working with laboratory animals. All animals were randomly assigned to one of the two surgeons via a 2 × 12 block randomisation list (Sealed Envelope Ltd. 2016). Buprenorphine (0.05 mg/kg; Buprecare®, AST Pharma) and carprofen (4 mg/kg; Norocarp®, Norbrook Laboratories) were administered subcutaneously as preoperative analgesia. Anaesthesia was induced using 3–4 vol.% isoflurane (IsoFlo®, Abbott laboratories), and maintained with 2–3 vol.%. Animals were placed on a heating pad at 38℃ and their temperature was monitored with a rectal probe. The abdominal fur was removed with electric clippers. The ischaemic button model was applied according to the original publication of Rajab et al. 9 In short, the technique comprises a midline incision and the creation of four paramedian ischaemic buttons on both sides of the abdominal wall (eight buttons per animal), placed 1 cm lateral of the midline incision and spaced 1 cm apart. Each button was created by grabbing a small 5 mm portion of parietal peritoneum and ligating the base of the tissue with a non-absorbable suture (4-0 Prolene® Ethicon). After tying the suture, it was turned around the entire base of the tissue and tied again to create the ischaemic button. This procedure was repeated for all eight buttons. Thereafter, the abdomen and the skin were closed in the midline by absorbable sutures (4-0 Polyglactin 910 Vycril® Ethicon and 4-0 poliglecaprone 25 Monocryl® Ethicon respectively). The animals were placed in a heated recovery cage (temperature ≈36℃) ventilated with 100% oxygen at 1 L per minute for postoperative recovery.
The standard analgesia regime was buprenorphine 0.05 mg/kg administered preoperatively, and buprenorphine 0.03 mg/kg administered postoperatively, 12 hours after the preoperative analgesia. The morning of the first postoperative day, carprofen 4 mg/kg was given to all animals. Thereafter, analgesia was administered based on clinical signs of distress such as wet-dog shakes, stretching or abnormal body posture, the animal not increasing in weight compared with the previous day or the welfare scores not improving compared with the previous day.
Outcome measurement
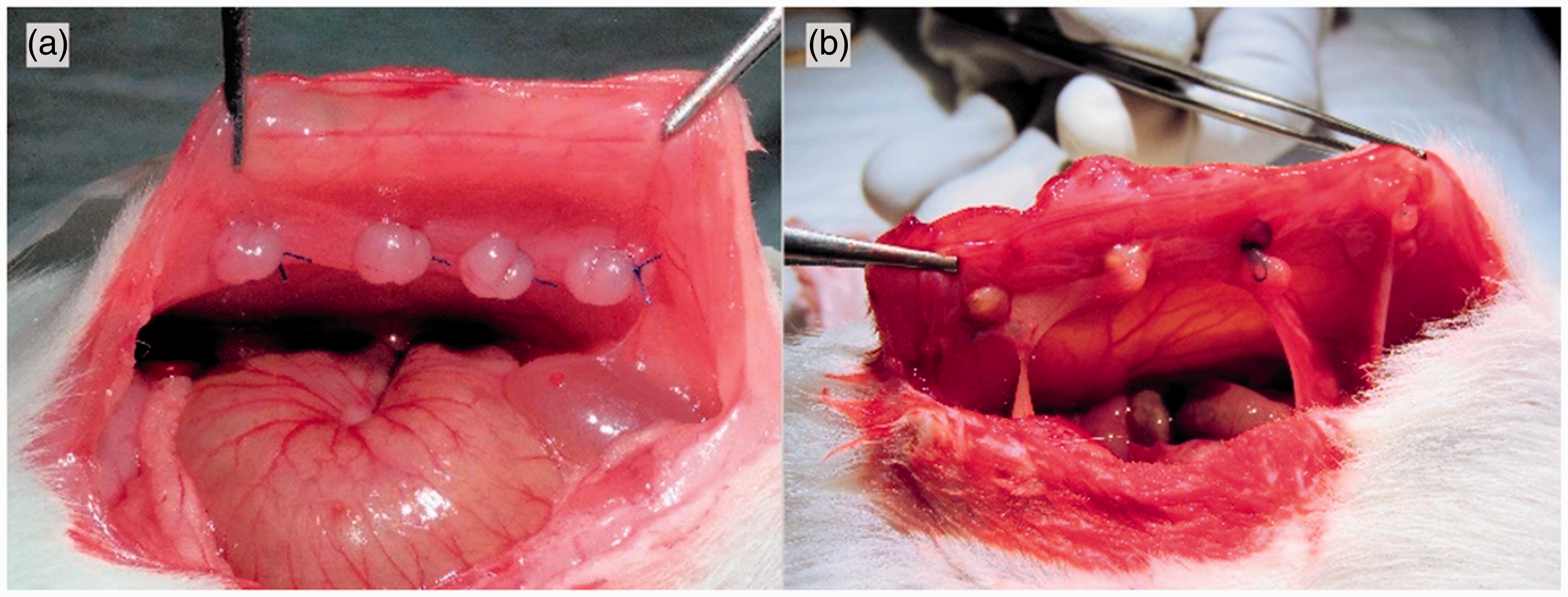
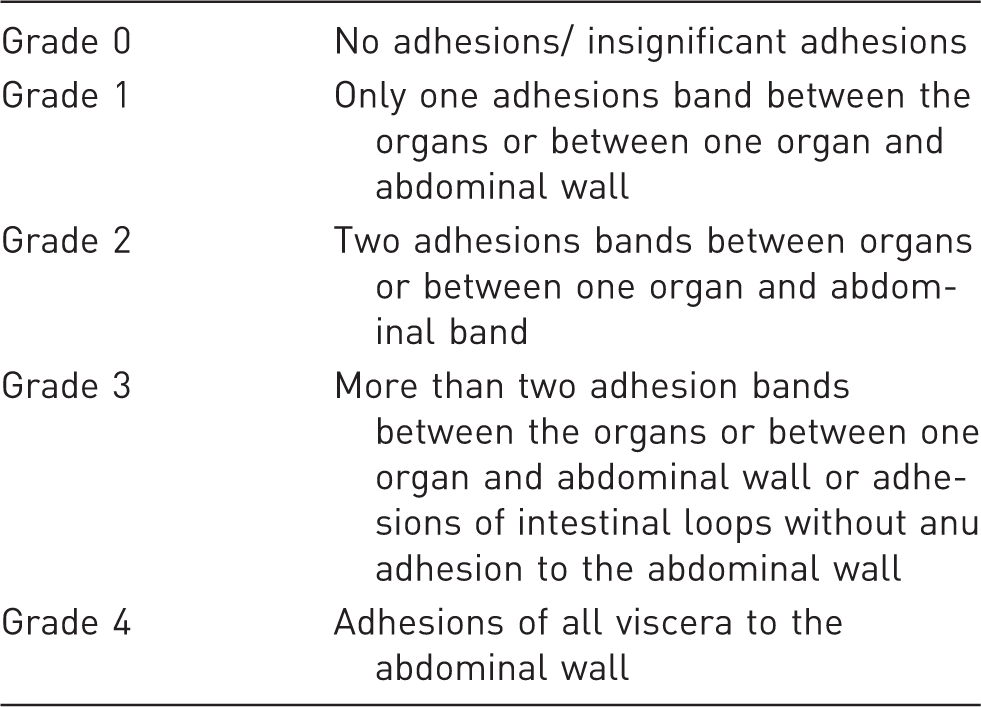
The primary outcome of the study was intra-abdominal adhesion formation. The quantitative analysis of adhesion formation was scored by calculating the amount of intra-abdominal adhesions formed to the number of remaining buttons after 1 week of follow-up (eight buttons per animal – obliterated buttons due to postoperative mobilisation or slipped sutures). Standardised scoring of the adhesion was based on standardised pictures taken by the surgeons (Figure 1) and performed by two researchers (EHHM and LH) blinded for sex. Qualitative analysis of the adhesions was performed using the macroscopic Zühlke score (Table 1).
10
Secondary endpoints were welfare scores, postoperative weight gain, need of postoperative analgesia and inter-surgeon variability. Welfare was assessed using a standardised welfare scoring sheet. All animals were scored daily during the full follow-up of the experiment. During the first two postoperative days, an additional ‘in cage’ observation was performed. Two authors (EHHM and LH) performed each assessment together to reduce interobserver bias. Each welfare assessment comprised of weighing the animal, checking the surgical wound for complications and scoring the following items: activity, behaviour, gait, posture, body condition, fur, hydration, breathing, faeces/urine and mucosa/extremity. Each item was scored 0 (no abnormality), 1 (any deviation from normal), 2 (clearly abnormal) or 3 (very abnormal). In the surgical wound category, a score of 0 reflected normal skin (no wound), 1 indicated a healing wound, 2 indicated a fresh wound and 3 indicated a wound complication.
Pre- and postoperative view of ischaemic buttons. (a) Preoperative view of four ischaemic buttons; (b) postoperative view of four ischaemic buttons with adhesions to the omentum and epidydimal/peritesticular fat. Zühlke macroscopic adhesion scoring system. Source: adapted from Zühlke et al.
10
A total welfare score was computed by adding all 11 previously mentioned items, and subscores for ‘surgical wound’, ‘behaviour’ (items: ‘behaviour’, ‘gait’ and ‘activity’) and ‘appearance’ (items: ‘posture’, ‘body condition’, ‘fur’ and ‘breathing’) were computed for a more detailed analysis of welfare. Delta welfare scores were calculated for each of the previously mentioned categories to evaluate the effect of additional analgesia.
Statistical analysis
Based on an alfa of 0.05, a beta of 0.20 and an effect size of 2.0, 12 rats were needed in each group. Statistical analysis for the outcomes ‘adhesions’ and ‘welfare/analgesia’ were performed using SPSS® version 22 (SPSS Statistics for Windows, IBM, Armonk, New York, released 2013). Analysis of weight gain and visual representation of delta weight gain was analysed/computed by GraphPad Prism®, version 6.00 for Windows (GraphPad Software, La Jolla, California; www.graphpad.com). Any group comparison was performed by independent student T-tests or Mann–Whitney U tests, depending on the distribution of the data (F-test).
Results
Two male rats had wound dehiscence in the middle of the laparotomy wound, with an intact underlying fascia. These animals were reoperated on the first postoperative day, the wound was cleaned and the edges of the wound were trimmed until punctate bleeding was observed. Thereafter, the abdomen was closed intracutaneously with 4-0 monocryl® sutures.
Adhesions
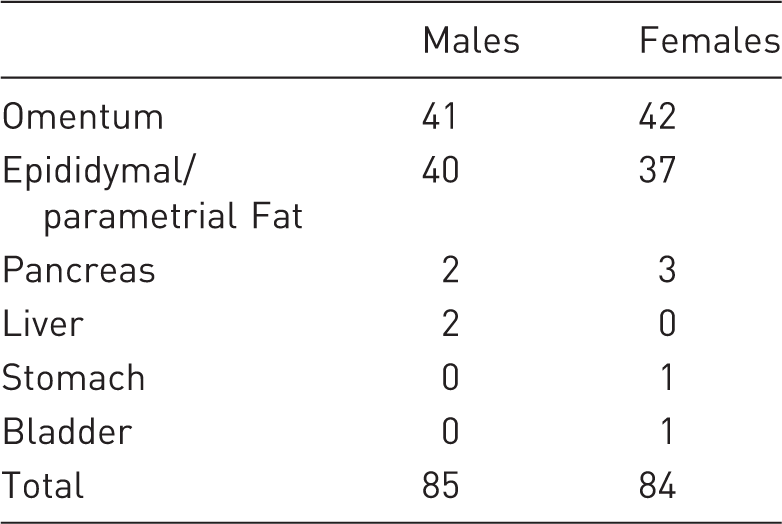
Anatomical structures that adhered to the ischemic buttons.
Welfare/analgesia
The difference in total welfare scores between male and females was not statistically significant, except for on postoperative day 4. At the fourth day, the mean overall welfare score for the male rats was 7.3 compared with 5.3 in the female group (p = 0.043). A higher score indicates more welfare impairment. The difference in welfare score at day 4 is based on a difference in the ‘behaviour’ subscore at day 4 (p = 0.012). The remaining subscores ‘wound’ and ‘appearance’ did not differ statistically significant between male and female rats (Figure 2).
Welfare scores during follow-up. Total welfare scores (a), as well as subscores for ‘appearance’ (b), ‘behaviour’ (c) and ‘wound’ (d) are presented. A score of 0 indicates good health and a higher score indicates abnormal behaviour or observations. There is a statistically significant difference in total welfare score and behaviour score at postoperative day 4 in favour of the female sex. There are no other statistically significant differences.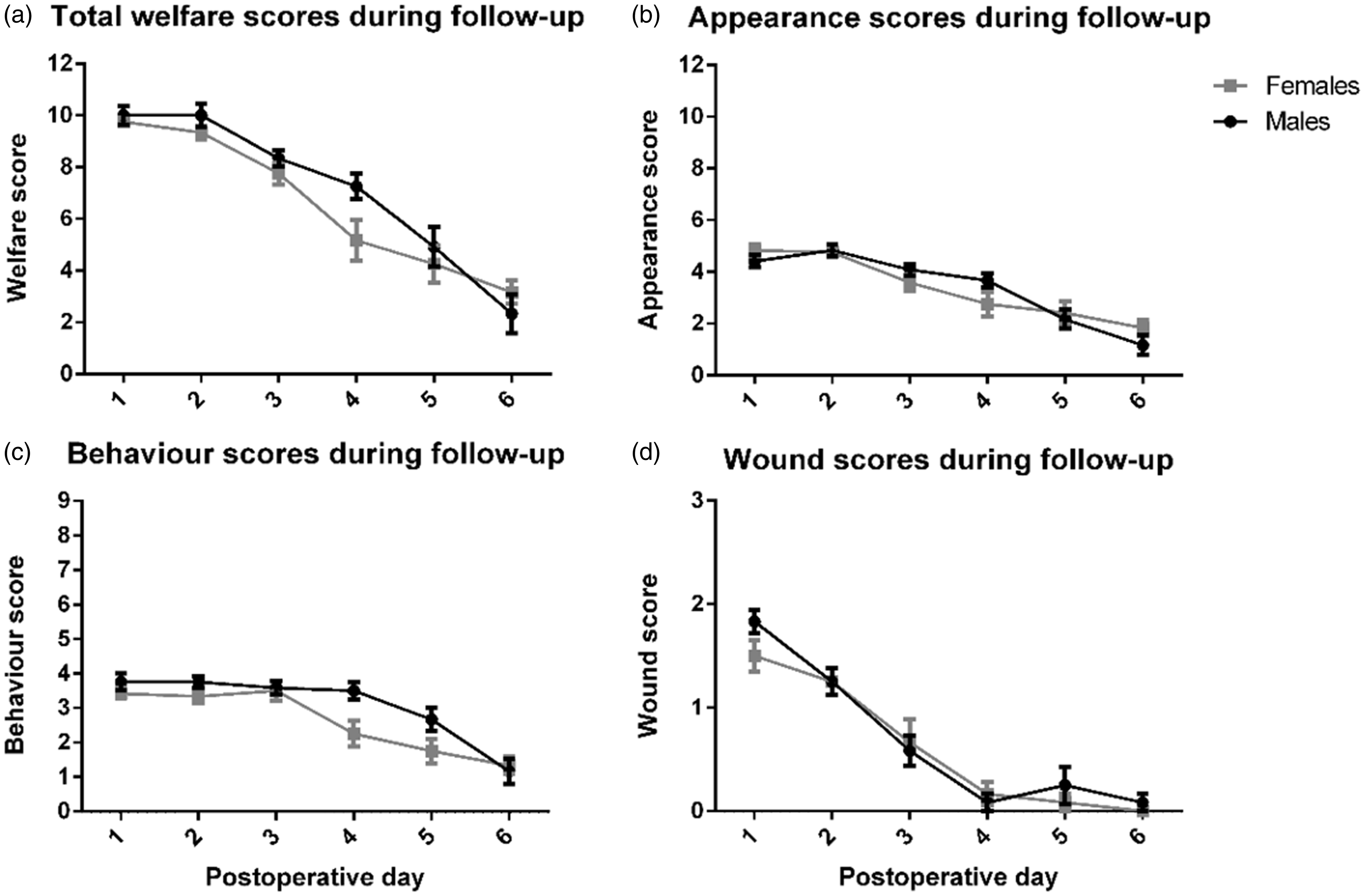
All animals received analgesia for the first 48 hours. Thereafter, analgesia was provided based on the welfare scores of an individual animal and/or clinical signs of distress. Additional analgesia was administered nine times (six rats) in the male group and eight times (six rats) in the female group (p = 0.807). As mentioned previously, there were two male rats with a reoperation for wound dehiscence, if analgesia within the first 48 hours from reoperation are excluded from the analysis, then there was no statistically significant difference between male and female administration of analgesia (p = 0.797). Differences between consecutive days were analysed by calculating delta differences of each category to evaluate the effect of additional analgesia. Only two statistically significant differences were found in the female group at postoperative day 6 between the total welfare (p = 0.02) and behavioural scores (p = 0.023) in the female group, indicating that the three female rats who received additional analgesia on postoperative day 5 performed significantly better compared with the female rats who did not receive pain medication. Indication for additional analgesia were confirmed by analysing the delta differences the day before analgesia was given, which showed statistically significant differences in at least one of the welfare categories at each day, indicating that the rats who received analgesia were not recovering as quickly as the remainder of the group.
Weight gain
Weight was measured daily throughout the follow-up. A delta weight gain was calculated by subtracting the baseline weight of each animal from the measured value to correct for sex-based differences at baseline. Male rats seemed to gain weight significantly faster compared with females (Figure 3). At the end of follow-up, 83% of the male rats had reached or exceeded the preoperative weight compared with 33% of the female rats. Differences at postoperative days 5–7 are statistically significant (Figure 3).
Delta weight gain during follow-up for males and females. The dotted line reflects baseline weight. Whiskers show the SEM. Postoperative day 0 is the value at baseline. **p < 0.01, ***p < 0.001.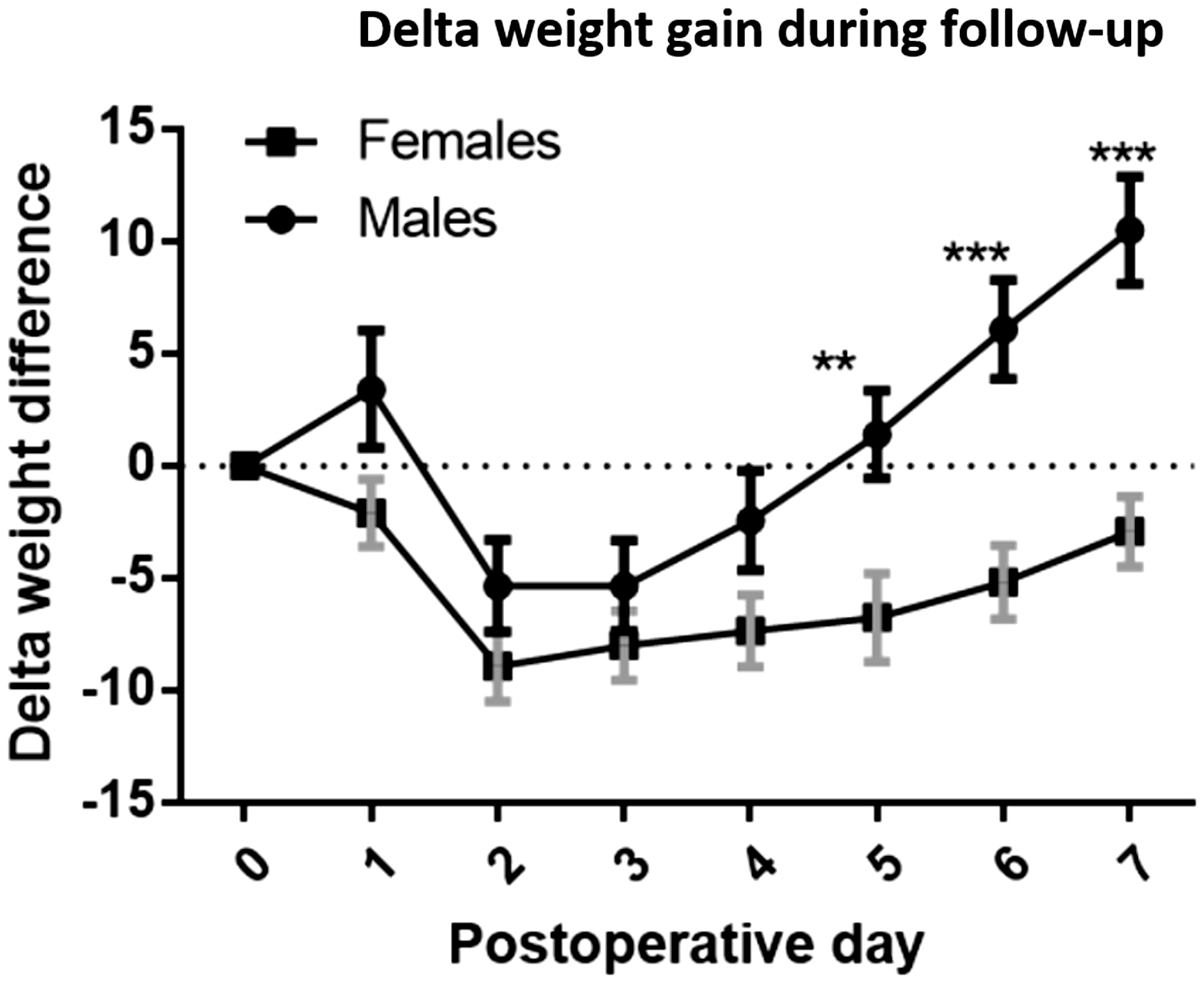
Figure 4 shows the delta weight gain corrected for normal physiological growth. The first 6 postoperative days did not differ significantly. Postoperative day 7 shows a significant difference between males and females (−10.56 g vs −16.9 g, respectively; p = 0.035).
Delta weight gain corrected for physiological growth. The dotted line reflects a ‘normal’ weight for each timepoint based on growth data supplied by Charles River Laboratories concerning German bred Wistar Han rats aged 8 weeks. Whiskers show the SEM. *p < 0.05; statistical significance on postoperative days 6 (p = 0.068) and 7 (p = 0.035).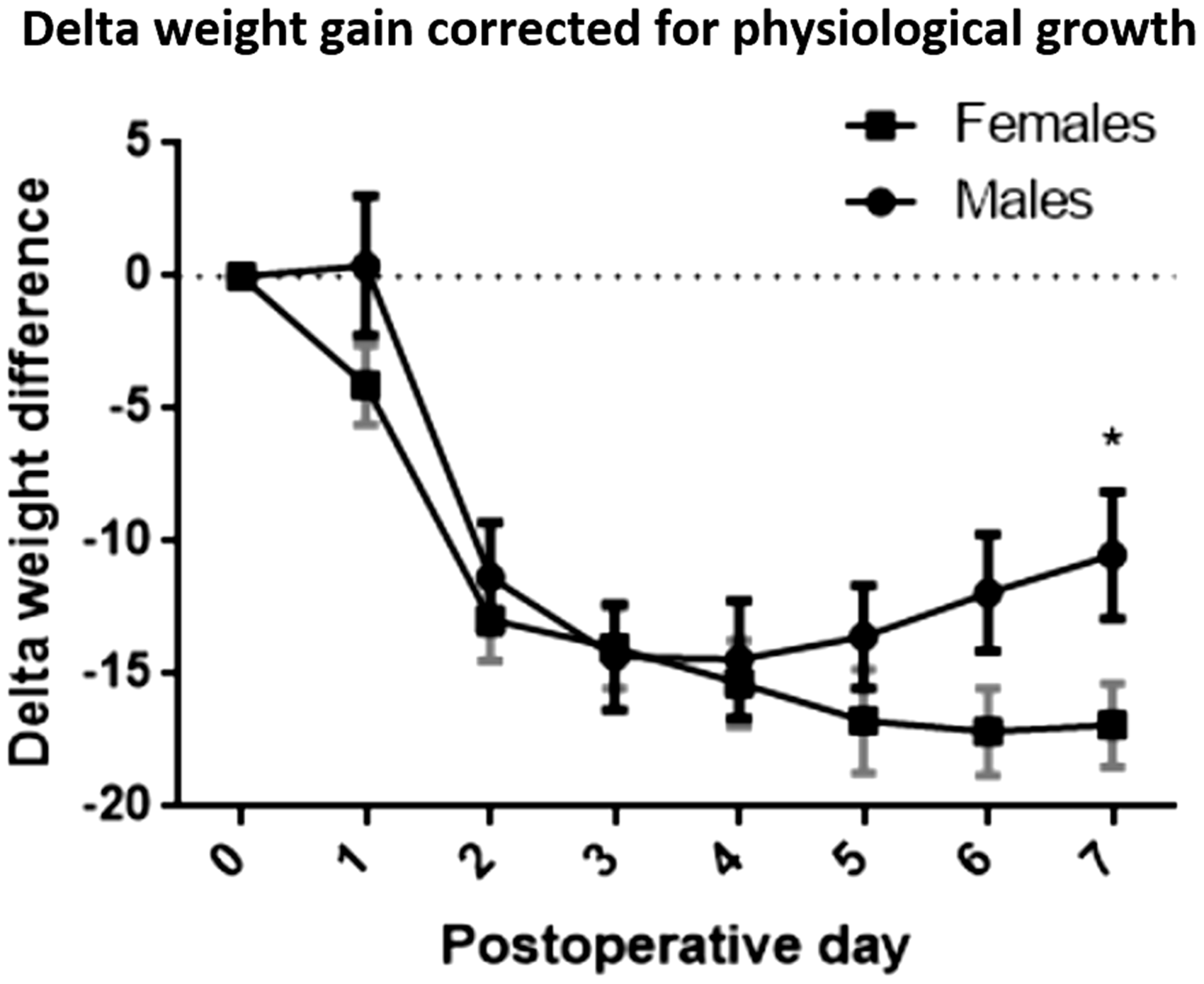
Discussion
The ischaemic button model is amongst the most frequently used models for the induction of experimental adhesions.11–15 This study shows there is no quantitative nor qualitative difference in the performance of the ischaemic button model between male and female Wistar Han rats. There was a significant difference in welfare on postoperative day 4, in favour of the female rats, and this difference in total welfare score was the result of a difference in the ‘behaviour’ subscore on day 4. The average difference was one point on a total score of nine points (behaviour subscore) and was deemed not clinically relevant. There was no statistically significant difference in the need for additional postoperative analgesia. Despite these similarities, male rats reached baseline weight significantly faster compared with female rats. When the delta weight gain was corrected for physiological growth, the statistical significance persisted at the end of the follow-up. The faster weight gain in male rats can be explained by multiple factors, ranging from faster postoperative recovery in the male group to insufficient analgesia schemes in the female group, or unrecognised need for pain medication in the female group. 16 There is increasing evidence that pain perception has sex-based differences. 17 Sorge et al. conducted a study in 2015 concerning pain perception in male and female mice, and found sexual dimorphism in pain perception based on Toll-like receptor 4 and dorsal horn gene expression.17,18 Previous studies have evaluated the dimorphism effect and demonstrated that opioids have a larger analgesic effect in male rats compared with female rats.19,20 These findings suggest sexual dimorphism in pain perception, as well as efficacy of analgesia. In our study, additional analgesia during follow-up (carprofen 4 mg/kg) was given if the welfare scores of an animal did not improve or the animal showed clear signs of distress. After receiving carprofen, both male and female rats improved clinically.
In this study, approximately one-half of the animals needed additional postoperative pain medication during follow-up despite the pre- and postoperative administration of buprenorphine and carprofen during the first 24 hours, indicating that future studies can and should include a more refined analgesia scheme. Based on the welfare scores of this study, analgesia should be continued for longer than 24 hours postoperatively, for example, 48 or 72 hours.
Button obliteration due to slipping of the suture (3.1% male group vs 5.2% female group) in this study was comparable with the study of Rajab et al. that reported a button obliteration of 3.8%, using the modified method.
9
Adhesion induction of the remaining studies is noticeably higher (91.4% male group vs 92.3% female group) than previously published work, such as the study of Rajab et al., who reported 62.3% adhesions in the modified group and 69.2% adhesions in the original ischaemic button group. However, adhesion induction in this model varies in the published literature from 62.3 to 92%.9,12,13 Variation in button obliteration and adhesion induction can be explained by multiple factors such as surgeon performance, suture material, button size, duration of the procedure and duration of follow-up. Button size refers to the amount of tissue protruding over the suture. When tying the back and front ligature of the ischaemic button, it is important to keep the angle between the suture and the abdominal wall as small as possible. This will ensure the creation of a large, durable ischaemic button (Figure 5). The type of suture used in the ischaemic button model varies from braided absorbable sutures to monofilament non-absorbable sutures.9,11–15 A suture comparison for the ischaemic button model has not been performed, although each type of suture has advantages and disadvantages. Braided sutures are easier to tie but are usually thicker. Silk or monofilament sutures are thinner and create a smaller base of the button with profound bulging of the tissue, although they are difficult to tie. Differences in histological response between absorbable and non-absorbable sutures may exist, but are currently based on speculation.21,22
Making durable ischaemic buttons. When tying the suture (after completing the backstitch), the angle between the suture and the abdominal wall (double-headed arrow) can vary. A large angle, shown by suture line ‘A’, will result in a small button. A small angle, shown by suture line ‘B’, will result in a bigger and more durable button.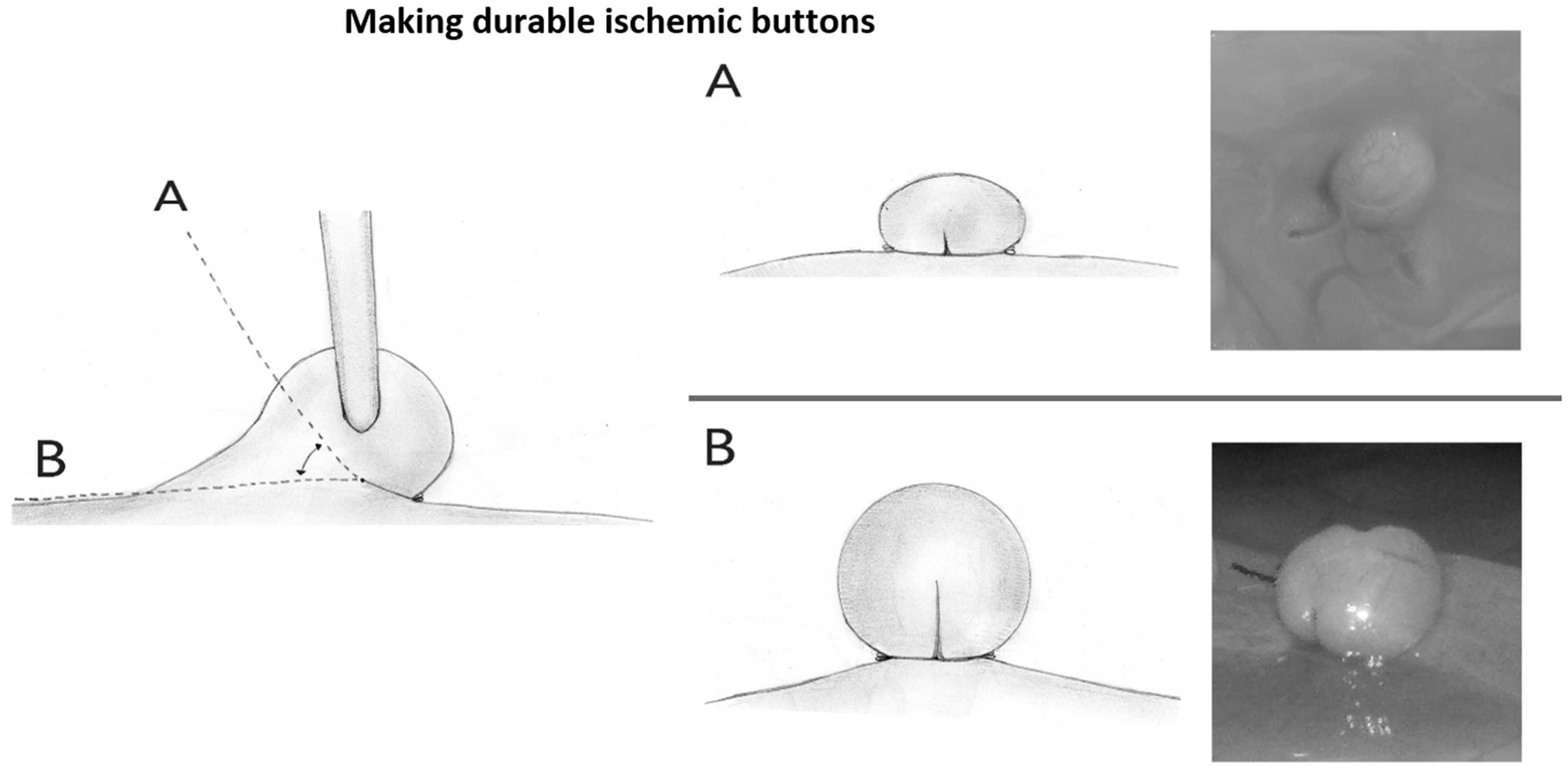
The type of tissue adhering to the buttons was comparable in male and female rats. Often male rats are used for this model because of their abundance of epidydimal fat, which is prone to adhere to the buttons. This study demonstrates that there is no difference in the type or location of adhesion induction between male and female rats. Females may have smaller intra-abdominal (parametrial) fat storage but this did not influence proneness to adhesion formation in the lower abdomen. There was no significant difference in welfare scores based on the type of organ involved in the adhesion. However, the effector the number of animals may have been too small to detect a difference in welfare scores because of organ involvement, as most animals had adhesions to intra-abdominal fat and only eight animals had adhesions to other organs such as the bladder, gut, liver or pancreas.
This study used an extensive 11-item visual welfare assessment, but this instrument has never been validated. Monitoring welfare in rodents is a difficult task because rodents are prey animals and will try to hide visual indicators for distress if possible. Moreover, behaviours or signs that are scored as signs of distress, such as sluggish movement or decreased food intake, could be a side-effect of the analgesia given. The aim of this study was to perform a clinical comparison of male and female rats in terms of adhesion induction. There were no separate analgesia regimens for male and female rats. Visual welfare assessment was performed directly at the cage, whereas video monitoring of welfare may be less stressful for the animals and therefore be more sensitive to abnormal behaviour.
Welfare in males and females was scored by the same observer to prevent inter-observer bias. Postoperative analgesia was standardised during the first postoperative 48 hours, although during the remainder of follow-up, analgesia usage differed between the groups, depending on clinical/welfare assessments. Additional analgesia was given if the total welfare score did not improve compared with the previous day, if the animal had not gained weight compared to the previous day or if the animal showed clear signs of distress (wet-dog shakes, stretching, abnormal body posture, etc.) No fixed cut-off point in welfare scores was defined for providing additional analgesia to the animals. As mentioned previously, the high number of animals needing additional pain medication in this study indicates that future postoperative analgesia protocols should include a longer postoperative analgesia scheme.
After analgesia was given, the welfare scores of the animals improved and showed no statistical differences compared with the other male/female rats that did not receive additional pain medication, with the exception of one timepoint (postoperative day 6 in the female group) that was considered not clinically relevant because the effect was not consistent with observations made on any of the other postoperative days, and therefore was most likely related to the small groups included in this analysis. Given the previously mentioned dimorphism in pain perception and analgesic efficacy of opioids, comparing welfare and pain perception between male and female rats is difficult, and attributing any observed difference in pain perception or analgesia treatment to a single cause is not possible in the current experiment.
Conclusion
Despite the discussed limitations, we can draw a conclusion from this study, namely that the qualitative and quantitative performance of the ischaemic button model is equal in male and female Wistar Han rats. In this study, there are no clinically relevant differences in postoperative welfare scores between male and female rats. Male rats seem to gain weight faster during follow-up and reach baseline weight sooner compared with female rats, even if corrected for physiological growth.
Tips and tricks for making ischaemic buttons
The type of organ/tissue adhering to the ischaemic button depends heavily on the location of the button. Hence, scoring organ type or even ‘organ involvement’ seems unjust in this model. When making the button, the angle between the suture and the abdominal wall must be as small as possible to create large durable buttons (Figure 5). Hold the suture knot for approximately 5 seconds during tying of the suture to allow the tied tissue to settle before tying the last knot to guarantee a tight ligature. Results of the ischaemic button model vary in the published literature, possibly because of surgeon performance, button size, type of suture material and differences in follow-up. Surgeon performance and button size can be perfected by experience, for instance in post-mortem animals.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.