
Abstract
Bile duct cannulation (BDC) studies are usually carried out in the rat to support the absorption, distribution, metabolism and excretion profiling of novel agrochemicals and pharmaceuticals. The different aspects of these studies (e.g. surgical preparation, dosing and collection of bile) can be intricate and/or technically complex. The animals are often kept singly housed for the duration of the studies following surgical implantation of the cannulas. The generation of insufficient data to meet the study objectives, for example due to failure in cannula patency, can result in the need to repeat these studies. A working group of contract research organizations that routinely carry out BDC studies was brought together by the National Centre for the Replacement, Refinement and Reduction of Animals in Research (NC3Rs) to share their experiences, and to establish the key factors necessary to ensure routinely high success rates. Through these discussions the group has identified opportunities for best practice across various aspects of the studies. The aim of these recommendations is to support all staff involved in conducting BDC studies to maximize the amount of useful data generated using the fewest animals possible, while ensuring the highest possible standards of animal welfare.
The absorption, distribution, metabolism and excretion (ADME) of agrochemicals and pharmaceuticals is primarily assessed using in vivo studies. These studies provide information on test substances and metabolite kinetics, including the rates and routes of elimination. ADME studies may be conducted to meet regulatory requirements (see example 1 ), to support the evaluation of pharmaceuticals with a specific half-life or rate of clearance, or to better understand the mechanisms underlying unusual pharmacokinetic, toxicokinetic or pharmacological profiles. These data are also used to inform design and interpretation of subsequent regulatory toxicology studies. Wherever possible, the same species should be used in toxicology and ADME studies, to support extrapolation during non-clinical to clinical studies. This is most commonly the rat. ADME studies are often conducted to OECD Test Guideline 417, 2 particularly for agrochemical regulatory studies.
ADME profiles can be assessed in the rat following oral and intravenous (IV) substance administration. For substances where >20% is present in faeces following oral dosing, the extent of absorption can be determined through measurement of biliary excretion for substances that cannot be dosed intravenously, for example if they cannot be appropriately formulated. Bile can be collected from animals over several days following/during substance administration via surgical cannulation of the bile duct. Henceforth these studies are referred to as bile duct cannulation (BDC) studies.
Preparation of the animals for BDC studies is technically complex, requiring relatively invasive and surgical techniques and skilled surgeons. The dosing and bile collection aspect of the studies can also be intricate, involving the single housing of animals within metabolism cages (Metabowls®) and cannulas that are at risk of twisting and/or blocking. Failure of the patency of a cannula during a study can result in insufficient data being generated to meet the study objectives, which may therefore necessitate the repetition of the study.
Prior to embarking on a BDC study, it is critical to assess whether the data that will be obtained are necessary to answer the scientific question at hand, and whether there are other means of obtaining the required information. When it is clear that these studies add value, useable data should be generated in line with the study objectives using the fewest animals possible. The UK’s National Centre for the Replacement, Refinement and Reduction of Animals in Research (NC3Rs) recently convened a working group of experts (study directors/metabolism leaders, veterinarians and surgeons) across three major contract research organizations that routinely carry out BDC studies. The group shared their experiences with BDC studies and the continuing refinements to processes and procedures, including measures their organizations have taken to ensure routinely high success rates. These organizations have a combined experience of conducting dual BDC studies of over 35 years across approximately 2500 surgeries. Through these discussions the group has identified opportunities for best practice. Consideration and incorporation of the recommendations described here should, in the experience of the working group, result in the generation of useable data from >80% of animals that are surgically prepared; data shared between the group show that out of 984 animals surgically prepared for bile duct studies, bile could be collected from 92% (n = 905). The aim of these recommendations is to support all staff involved in conducting these studies, to maximize the amount of useful data generated while ensuring the highest possible standards of animal welfare.
Considerations prior to starting BDC studies
Before animals are prepared for a BDC study, some key factors should be considered to establish whether the BDC study is most appropriate and necessary to answer the scientific questions, and if so, how the studies should be designed with regard to sex and strain of animals used and doses tested. A flow diagram summarizing the steps described can be seen in Figure 1.
Decision tree to aid in the selection of either an intravenous (IV) or bile duct cannulation (BDC) study.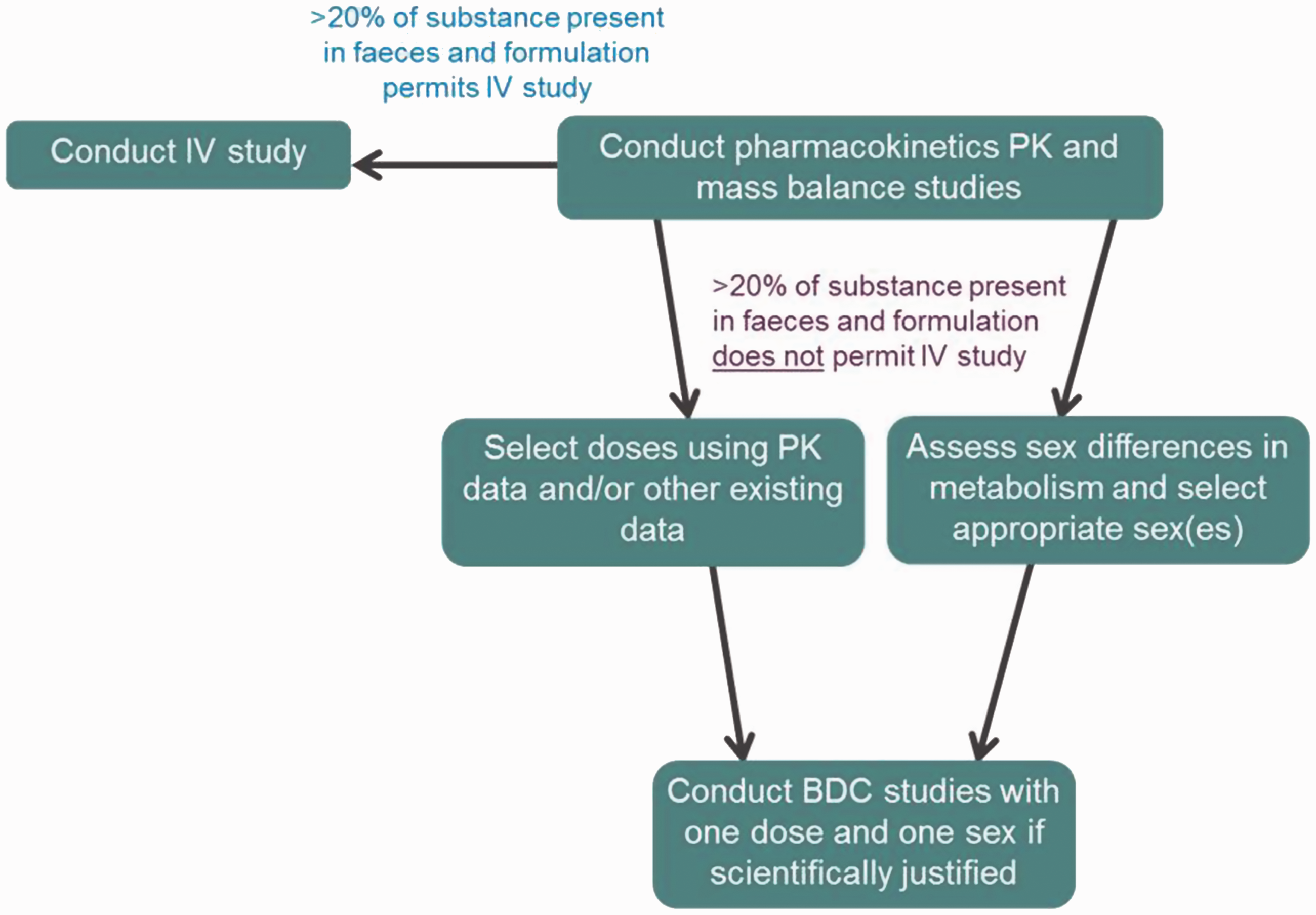
Selection of an oral BDC study or an IV administration study
Mass balance studies should first be completed, and this information used to determine the exact extent of absorption following oral dosing. If this cannot be established (e.g. where >20% of the administered dose is present in faeces), further investigations might be necessary. The subsequent studies could be comprised of either the oral administration of the substance and its measurement in bile through a BDC study, or both oral and IV administration of the substance and measurement of net substance present in urine, expired air, and carcass for each route. The recovery in faeces following IV administration would also provide an indication of biliary elimination.
Where formulation and solubility of the substance permit, the preference is to conduct an IV administration study rather than a BDC study, as IV studies are less invasive and thus have less impact on the experimental animals. Pharmaceutical formulations are more often amenable to IV formulation than agrochemicals. For pharmaceuticals, an oral/IV crossover design may be used, as the absorption profile of the IV dose will confirm the absorption profile of the oral dose within the same animals and without the need for surgical preparation.
It is unlikely that both IV and BDC studies will be necessary to complete the absorption profile and therefore only one of these should need to be conducted. BDC studies with IV rather than oral substance administration may be necessary where quantification of intestinal secretion is needed; however this only applies if there is evidence of direct secretion of the absorbed dose across intestinal membranes.
Inclusion of one or both sexes in BDC studies
Sex differences in metabolism are possible, for example as a result of gender-specific cytochrome P450 (CYP) liabilities, but these should be thoroughly investigated prior to the inclusion of both sexes in BDC studies. This is generally achieved through in vitro assays as part of cross-species comparison studies conducted during non-clinical development, prior to first in human dosing for pharmaceuticals. Sex differences can be identified using information from pilot in vivo studies using a very small number of animals (e.g. n = 1 per gender), or other pharmacokinetic/toxicity studies that have already been carried out. In a BDC study inclusion of one sex is justified where no genuine sex differences can be detected. This would preferably be male, as male animals tend to be larger and more background data are available than for females.
Selection of doses and number of dose groups
OECD Test Guideline 417 states that ‘a single dose of the test substance should be administered’, i.e. one concentration of test substance. Data from other studies, such as pilot or pharmacokinetic studies, should be utilized for dose selection purposes. The testing of both a high and low dose for instance is only justified if a notable difference has been identified between excretion patterns of low and high dose groups for intact animals. If the profiles are similar between the two doses, the lower dose should be selected for testing in the BDC study.
Ensuring high success rates once BDC studies are triggered
Number of days generally required for each stage of preparation and conduct of bile duct cannulation (BDC) studies following animal arrival and acclimatization.

Note that these are suggested timings which in the experience of the authors are sufficient to ensure the welfare of the animals and should be considered in the context of individual facilities’ standard animal welfare procedures, as well as taking into account variability between animals. Differences in necessary timings, particularly for acclimatization periods, may be dependent on the strain and sex.3,4 Animals should remain group-housed for as long as possible.
General considerations
Monitoring of success rates
With optimal animal preparation and study set-up, success rates should routinely exceed 80%. If this level of success is not achieved or if there are fluctuations in the degree of success, troubleshooting should be undertaken to address the underlying causes. Troubleshooting should be conducted in a logical manner, varying only one technical aspect at a time. It is crucial that good records are kept detailing how the procedures have been carried out. There should be recording and close monitoring of at least the following: (a) how many animals survive surgery; (b) how many fully recover from surgery; (c) rates of bile flow during recovery and post-administration; and (d) how many provide useful information at the end of the study. This will aid in identifying the key areas to focus on for improvement should there be suboptimal success rates.
Impact of additional cannulations
The highest success rates are achieved when the ‘dual cannulation’ method is employed. For this method both the bile duct and gastrointestinal (GI) tract (duodenum) are cannulated, to allow for the simultaneous collection of bile and reinfusion of bile salts. This has been recommended previously (see example 5 ). Single cannulation of the bile duct without reinfusion of bile is not recommended, since the bile can become depleted, requiring the provision of additional supplements; 6 see ‘Surgical considerations’. Additional cannulations (e.g. jugular vein catheterization for test substance infusion or blood sampling) tend to negatively impact success rates, but are technically possible. Full justification for the inclusion of additional cannulas should be provided during pre-study ethical review discussions, to optimize study design and scientific and welfare considerations.
Weight of animals selected for study
Animals should be at least 200–250 g, preferably 225–275 g, at the time of surgery. This will ensure that the bile ducts are of a sufficient size for cannulation. The provision of high nutrient diets does not increase the size of the bile duct. Although BDC study animals should ideally be the same age as for other toxicity studies that are carried out for the same substance, OECD Test Guideline 417 does permit the use of animals of a different age, providing there is scientific justification, i.e. if it is necessary to ensure the success of the study. This is particularly important for smaller strains of rat such as the Han Wistar; for example the guideline age of 6–12 weeks should be acceptable for Sprague Dawley rats, with surgery performed between 9 and 10 weeks and dosing at 10–11 weeks of age; whereas for smaller strains, justification could be given for surgery between 11 and 12 weeks and dosing at 12–13+ weeks, as these can still be considered young healthy adults. It is important that protocols are kept flexible regarding the age of animals to ensure that those of the most appropriate weight can be selected for the studies.
External influences
It should be ensured that animals are fit enough following surgery to follow their normal feeding regime, thus avoiding the need for additional supplements. Hydrogel/DietGel (nutrient fortified water gel) tubs and water-softened pellets can be beneficial during the first few days after surgery, but it should not be necessary to offer oral rehydration solutions during the bile collection phase of the study, particularly since the infusion of replacement bile salts into the duodenum provides supplementary fluids, and by this stage animals should be sufficiently recovered from surgery to maintain normal hydration. If other supplements are given these should be standardized between animals in terms of the amount given and the timing of administration since they could otherwise affect the outcome of the study.
Surgical considerations
Surgery should be performed in a serviced surgical facility suitable for aseptic procedures, by personnel trained and experienced in the appropriate techniques. A high standard of asepsis must be maintained throughout the whole surgical procedure (including handling of equipment). Asepsis is crucial for surgical success and for full recovery of the animal before the start of the study. Guiding principles for preparing for and undertaking of aseptic surgery can be found at www.lasa.co.uk/pdf/lasa_guiding_principles_aseptic_surgery_2010.2.pdf and http://www.procedureswithcare.org.uk/aseptic-technique-in-rodent-surgery/. The surgical procedure must be performed consistently to deliver a repeatable outcome while reducing complications. This is achieved by the overall building of experience through encountering different situations related to the technique, followed by iterative improvement and refinement of the technique.
There are different types of surgical technique which can be employed, each varying in the method by which bile is returned to the intestine. Single cannulations of the bile duct without reinfusion of bile is not recommended, as the bile can become depleted requiring the provision of additional supplements. A comparison of two surgical techniques which use dual cannulations was conducted by Wang and Reuning. 5 The authors found that the preferred surgical method for the return of bile into the intestine was to cannulate the GI tract, rather than the distal bile duct. This method showed better survival rates, body weight gain profiles and mean plasma lipase than when returning bile to the bile duct, which may be associated with potential interference with the pancreatic ducts during catheterization of the distal bile duct. 7
Specific issues can arise as a result of suboptimal positioning of the bile duct cannula. If suboptimal success rates are experienced, the positioning of the cannula should be one of the first factors examined. Incorrect positioning of the cannula either during surgery or due to its movement following surgery can lead to leakage from the cannula or complete dislodgment of the catheter, and possibly other effects such as bloating of the stomach, as it may affect the transit of the food along the gut. Occasionally bile will stop flowing through the cannula for no identifiable reason and successful flow of bile observed at the time of surgery may cease on completion of surgery, when the animal is no longer lying on its dorsal surface. A number of failures related to positional problems such as twisting or kinking of the bile catheter are due to animal movement post-surgery, and are not always related to incorrect placement of the catheter. For further guidance on cannula positioning, see van Wijk et al. 7 Some animals may possess larger bile ducts than others, even if they are of a similar weight. This will be apparent during the surgery and if so there is the option to use different diameter catheters to address this, i.e. a smaller diameter catheter when the bile duct appears to be on the smaller end of the spectrum. There is the option of using either silicone or polyurethane catheters for this technique; the preferred material will vary between different facilities and surgeons. If there are issues with success rates the type of catheter material used is an aspect that can be considered.
Examples of anaesthesia that can be used for these surgeries include isoflurane in oxygen, with the use of carprofen and buprenorphine as analgesics pre- and post-surgery. Use of anaesthetics and analgesics should be in line with both recommendations from veterinarians and standard practice within individual facilities.
Post-operative considerations
Ideally a dedicated and consistent study team will oversee the post-operative care of the animals. This ensures that staff members have the appropriate level of experience with the model and understand the gentle approach required following surgery, and successful troubleshooting of issues that arise with the cannulas or swivel system. It must be noted that different exteriorization methods can be used (e.g. via the neck or tail; Figure 2) and staff should have the specific experience for the relevant method. Issues that may occasionally arise where neck exteriorization is used include chewing of the harness, harness straps found in the mouth, removal of legs from the harness or escape of the animal out of the harness, and ill-fitting of the harness leading to catheter movement and cessation of bile flow or irritation/sores of the skin. The degree of tightness of the harness is critical to prevent issues such as these, and the correct technique will be established with experience. Issues with the tail cuff technique can include tether and catheter chewing due to the high level of movement afforded by this technique, and the kinking and knotting of the tether if it is too long. Handling of animals following surgery should be minimized so as not to disturb the cannulations, and flushing of bile duct cannulas should be avoided. Blockage of the duodenal catheter following surgery is possible if food occludes the end of the catheter. When this occurs the duodenal catheter should be flushed with 0.1 mL saline to remove the blockage.
Following surgery animals should be placed into solid-bottomed cages and nesting material should be provided. Animals should be monitored closely throughout the recovery period; food and water consumption should be assessed visually and the flow of bile monitored, as well as daily body weights, visual urine/faecal output and clinical observations, paying particular attention to the surgical sites.
The decision whether to take forward a surgically prepared animal for use in a study is dependent on the general condition of the animal following surgery, satisfactory food and water intake, urine and faecal production, whether the animal has retained sufficient body weight (no higher than a 15% loss in pre-surgery weight), and whether there is successful bile flow through the cannula. Clinical signs that should be assessed routinely following surgery include (but are not limited to) hunched posture, piloerection, and reduced urine and faeces output. If an animal is not showing signs of recovery four days after surgery then it is unlikely that it will recover sufficiently for use in the study.
Bile flow can either be recirculated via the duodenal catheter until the study begins, or be collected. Flow should be checked daily following surgery and, where collected, a record kept of the volume –approximately 10–20 mL/day bile flow (0.5–1 mL/h) from a 250 g rat should be observed. If there has been an unusual amount collected pre-dosing, this information may be utilized later in the study to explain outliers in the data. The colour of the bile should be monitored, as a dark colouration can indicate bile stasis. Occasionally bilirubinuria is seen if biliary drainage is reduced. A shift in excretion of the test substance from biliary to urinary excretion may accompany the bilirubinuria in some cases of biliary stasis – this can be identified by a bright yellow colour to the urine. The tether by which the animal is attached to the cage should be long enough to allow free movement of the animal but not too long that it may become kinked or knotted if the animal is quite active.
If an animal cannot enter the data collection phase of the study or if it is removed from the study during the data collection period then it is important that a necropsy is performed to understand the cause of the problem, including examination of the cannula positioning.
Considerations during dosing/bile collection
Animals should be placed in their Metabowls overnight the night before the study and successful bile flow through the cannula checked at this point. Bile collection should always take place below the level of the animal, as this is reliant on gravity. It is important to observe the syringe containing the bile salts regularly and change this if crystallization of bile salts is apparent.
If pilot study data or data from other phases of the metabolism study are available these should be used to determine the length of time necessary for bile collection. As animals are singly housed during the dosing and collection stage of the study it is preferable that studies only continue for as long as scientifically necessary.
There is scope to consider modifying standard Metabowls to improve the animals’ access to food and their overall welfare. Some exteriorization methods, particularly those utilizing harnesses, are not compatible with the glass arms of some Metabowls and thus restrict access to food and water. In this case, modifications to the equipment to ensure sufficient access should be sought prior to starting studies. Other modifications applicable to all types of metabolism study include the application of red transparent film to the sides of the Metabowl (Figure 2). The use of transparent red caging has been shown previously to have a beneficial effect on markers of well-being in rats.8,9
(A) Typical Metabowl set-up for animals with tail exteriorization. (B) Example of amended Metabowl enabling easier access to food and water. (C) Animal with nape of neck exteriorization and harness attachment of swivel system.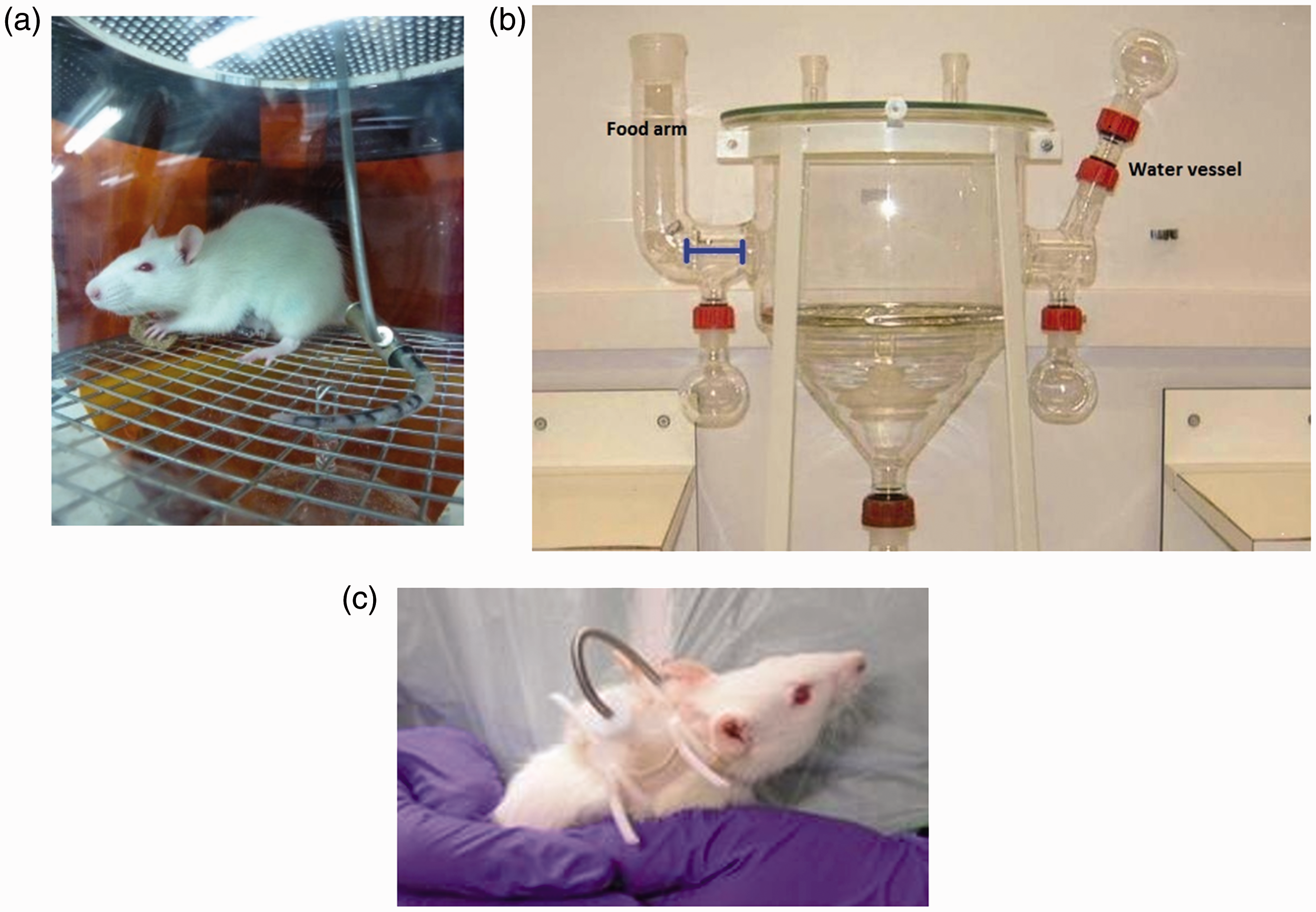
The need for using Metabowls and single housing are not ideal in terms of animal welfare, and therefore a future research priority should be centred around the development of methods which allow for long-term collection of urine and faeces that allow the study objectives to be met but which negate the need for single housing and the use of metal grids at the bottom of cages.
Concluding remarks
It is imperative that BDC studies are only carried out when there is no alternative, and/or a less invasive means of answering the scientific questions posed. Where triggered, efforts can be made to decrease the numbers of animals that must be used through consideration of the study design. On the other hand, sufficient animals should be surgically prepared so as not to risk having to repeat a study that does not provide sufficient data to meet the scientific objectives. Through consideration of the recommendations described here, success rates in excess of 80–90% are feasible. The ultimate aim is, of course, to consistently achieve 100% success rates. In some instances however, removal of an animal from a study will be unavoidable, for example if the cannula becomes irreversibly twisted after an animal has been placed in a Metabowl. Nonetheless, undertaking the measures proposed here will minimize these events as far as possible. The authors welcome feedback from practitioners in the field who are conducting these studies and have identified other techniques and key factors that impact on the success rates of these studies. Feedback should be shared with the corresponding author of this paper by email, with a view to the authors potentially updating the recommendations presented here in a future publication.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.