
Abstract
This study was designed to determine whether perineural injections of local anaesthetics decreases intraoperative nociception and improves postoperative analgesia in New Zealand White rabbits undergoing experimental stifle arthrotomy. All animals were anaesthetized using isoflurane and received morphine intramuscularly. The sciatic and femoral nerves of the leg to be operated on were located using a nerve stimulator (1 Hz, 0.5 mA). Rabbits were assigned to a treatment group (LB; n = 12) or a placebo group (P; n = 12) in a randomized blinded fashion. Group LB received lidocaine 2% (1 mg/kg) combined with bupivacaine 0.5% (0.25 mg/kg) injections around the sciatic and femoral nerves (0.1 mL/kg total volume per site) and subcutaneous infiltration of the incision site with lidocaine 1% (1.25 mg/kg). Group P received the same volume of 0.9% NaCl. Rabbits in group P required higher doses of intraoperative fentanyl and propofol to reduce heart rate and suppress increase in systolic blood pressure, and maintain an adequate anaesthetic plane. Interventional analgesia (buprenorphine and carprofen) was required significantly earlier in rabbits in group P (2 and 6 h after the first nerve blockade, respectively) based on assessment of their pain-related behaviour and range of motion. Using a visual analogue scale (0 mm= no pain to 100 mm= maximal possible pain), rabbits in group LB were judged to show significantly less pain compared with rabbits in group P (14 ± 10 mm and 37 ± 25 mm, respectively) 2 h after nerve blockade. In conclusion, this technique of perineural analgesia combined with incision site infiltration reduced intraoperative fentanyl requirements and improved postoperative analgesia in rabbits.
Postoperative pain management is a challenge in laboratory animal anaesthesia.1,2 Over the past decades the use of analgesics has increased, but the overall level of postoperative pain relief for laboratory animals is still low. 3 Opioids and non-steroidal anti-inflammatory agents (NSAIAs) are both effective analgesics for rabbits. However, in some research settings their use is limited as they can cause undesirable side-effects and may interfere with the results.4,5
Effective analgesia of the stifle joint can be obtained when the sciatic and femoral nerves are contemporaneously desensitized with local anaesthetics 6 and can be used perioperatively as part of balanced anaesthesia. The application of local anaesthetics in the vicinity of sensory nerves is considered to be one of the most efficient analgesic techniques because transmission of nociceptive information to higher neural levels is reversibly interrupted. 7 Nerves that contain motor fibres (i.e. femoral and sciatic nerves) can be localized using a peripheral nerve locator. 8 An electrical impulse is sent through the tip of a purpose-made insulated needle causing a motor response when placed close to a motor nerve. This technique improves the success rate of the local blockade 9 and reduces the effective dose of these potentially toxic drugs since the local anaesthetic drugs can be deposited very close to the target nerve.10,11
Electrolocation of the sciatic nerve has been reported in rabbits. 12 The feasibility of blocking the sciatic and the femoral nerves with local anaesthetics has recently been described in a case series. 13 However, the analgesic efficacy of a dual nerve block of the femoral and sciatic nerves with a combination of two local anaesthetics (lidocaine and bupivacaine) combined with a subcutaneous lidocaine infiltration at the incision site has not been evaluated in this species. We hypothesized that this technique would decrease intraoperative nociceptive responses and would provide adequate postoperative analgesia in rabbits undergoing stifle joint arthrotomy.
Materials and methods
Animals
Twenty-four male New Zealand White rabbits (Crl:KBL(NZW) strain, Charles River Laboratories, l’Arbresle, France), aged four months, were used in the study after approval from the local ethical committee for animal experimentation. The animals were part of a larger study in which a chondroprotective agent was used in a stifle joint arthrotomy model. The rabbits were brought to the research facilities in Switzerland four weeks before the experiment where they were handled daily to get accustomed to the new environment and to personnel. The animals were housed in individual steel cages with polyvinyl chloride (PVC)-coated grill floors and a wooden retreat placed in a room with an open system at a temperature of 18℃ and 60% humidity. A 12/12 h light/dark cycle (07:00–19:00 h) with artificial lighting was applied. Rabbits were fed a pelleted diet (LRP; Kunz Kunath Fors AG, Weinfelden, Switzerland), carrots and hay ad libitum and had free access to tap water. Pellets and carrots were withheld for 12 h before the experiments but hay and water were provided until half an hour prior to anaesthesia. Rabbits were given a physical examination and healthy rabbits were graded with a ‘physical status I’ according to the American Society of Anesthesiologists.
Study design
The study was designed as a blinded, placebo-controlled, prospective, experimental trial. Rabbits were randomly allocated to one of two treatment groups by drawing lots (LB: treatment group; P: placebo group). One anaesthetist (KK) performed induction of anaesthesia, endotracheal intubation and all local anaesthetic injections, as well as postoperative pain assessment and treatment. Another anaesthetist (HK) performed anaesthesia monitoring and assessment and treatment of intraoperative nociceptive responses. Both anaesthetists were blinded to the treatment protocol. A third investigator (MPL) prepared the drugs for both groups (LB and P).
Anaesthesia
Anaesthesia was induced with isoflurane (Isoflurane Baxter; Baxter AG, Volketswil, Switzerland) in oxygen (O2) delivered via a face mask connected to a paediatric circle system of a small animal anaesthesia machine (Draeger BN 75; Draeger Medical AG, Bern, Switzerland). A single operator restrained the rabbit gently and O2 delivery was started at a flow rate of 2 L/min. When the rabbit accepted the restraint and breathed comfortably through the face mask, isoflurane delivery was commenced using a precision vaporizer (Datex Ohmeda Isotec 3, Dr Mueller GmbH, Prittriching, Germany). The vaporizer was first set to deliver at 5% and gradually its setting was reduced to 3%. When the animal lost its righting reflex and reached an appropriate anaesthetic plane (muscle relaxation, eyeball rotation, reduced palpebral reflex and absence of swallowing reflex), 0.2 mL of tetracaine (Gingicain D; Sanofi Aventis, Frankfurt, Germany) was sprayed onto the larynx. An orotracheal tube (internal diameter 3.5 mm) was placed into the trachea with the aid of a stethoscope attached to the endotracheal tube via an adaptor. Immediately after intubation, morphine 1 mg/kg (Morphini hydrochloridum; Streuli Pharma, Uznach, Switzerland) was administered intramuscularly. A 24 G over-the-needle catheter was placed into a marginal ear vein for fluid and drug administration. Lactated Ringer’s solution (10 mL/kg/h) was delivered during anaesthesia. A 22 G arterial catheter was placed into a middle ear artery for invasive blood pressure measurements. The endotracheal tube was connected to a breathing system and anaesthesia was maintained with isoflurane in O2 at 0.5 L/min with the vaporizer set at 2.5% throughout the anaesthesia. Rabbits breathed spontaneously during the whole anaesthetic episode. Normothermia was maintained with a forced-air patient warming system (Bair Hugger Model 505; Arizant, La Ciotat, France).
Sciatic and femoral nerve block technique
Both skin areas for needle insertion, of the leg to be operated on, were clipped, surgically scrubbed and draped with the rabbit placed in dorsal recumbency. A 24 G, 25 mm insulated, atraumatic short bevel needle (Stimuplex STIM-A; B Braun, Melsungen, Germany) and a peripheral nerve locator (TOF Guard; Biometer Int, Odense, Denmark) were used to locate the nerves. The drug delivery port of the insulated needle and the tubing were primed with 0.4 mL of the test solution (LB or P). The peripheral nerve locator was set to deliver short duration pulse stimuli (40 µs) with a frequency of 1 Hz and an initial current of 2 mA.
Anatomy
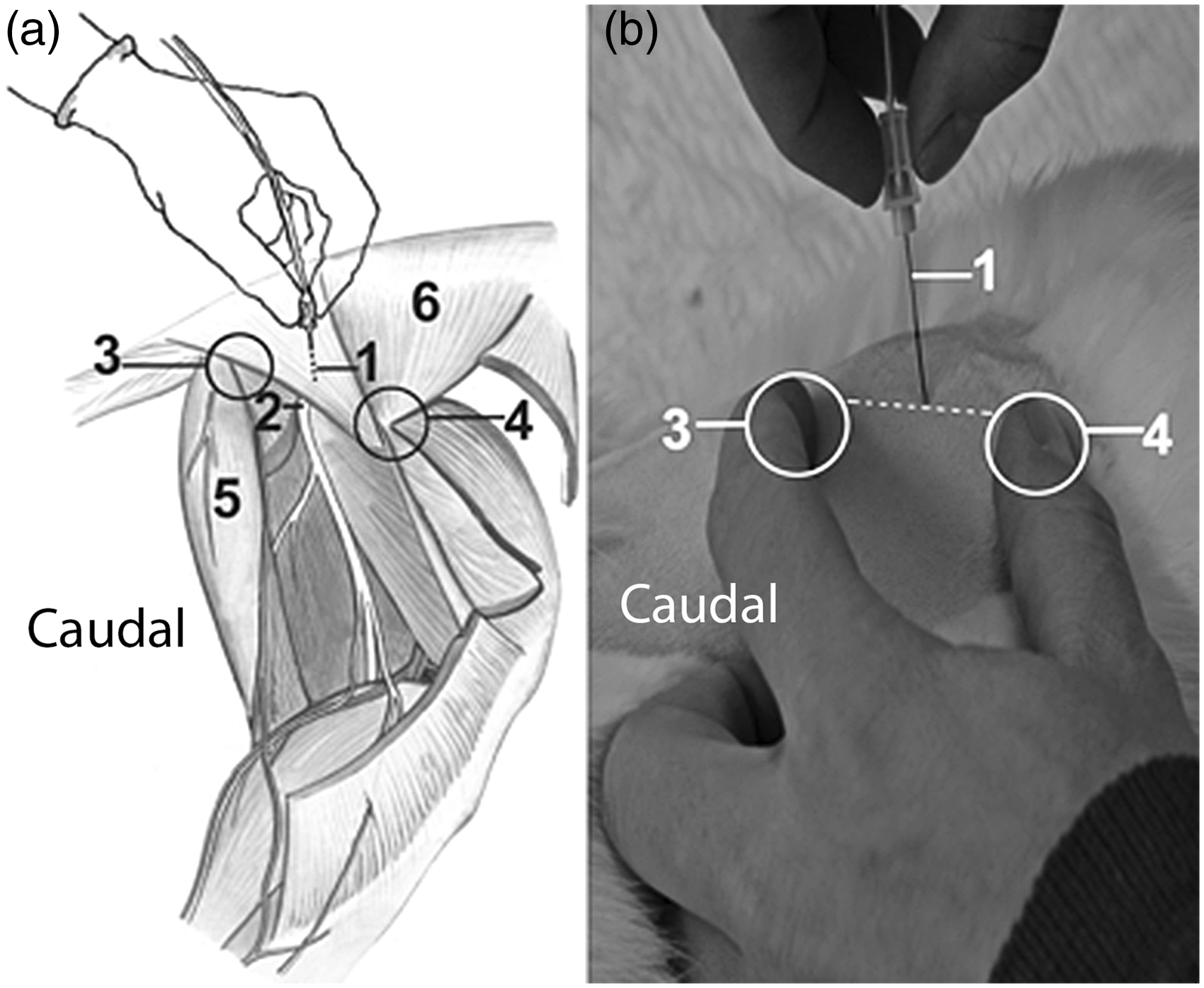
The anatomical structures used to locate the femoral nerve were the inguinal ligament and the femoral artery. The rabbit was placed in dorsal recumbency and the femoral artery was located by palpation distal to the inguinal ligament (Figure 1). The insulated needle was inserted just cranial to the artery through a 2 mm skin incision performed with a hypodermic needle to an approximate depth of 0.5 cm following the abdominal wall line, at a 30–45° angle to the skin. A constant negative pressure was applied to the syringe during femoral nerve localization to avoid inadvertent intra-arterial injection of the test solution. Small adjustments of the needle position were made until movements of the patella and quadriceps muscle group were observed with each delivered electrical impulse. At this time, the stimulation intensity was adjusted and 0.9% NaCl or the local anaesthetic solution was injected as described below. Thereafter, the rabbit was placed in lateral recumbency and the sciatic nerve was localized in the groove between the ischial tuberosity of the pelvis and the greater trochanter of the femur (Figure 2). The insulated needle was introduced (0.7–1 cm deep) perpendicularly to the skin in the middle of an imaginary line connecting these two prominences until movements of the lower hindlimb extensors were observed with each delivered electrical impulse. Negative pressure was applied to the syringe and a lack of blood return rendered intravascular injection unlikely. For both nerves, the stimulation intensity was adjusted downward and, if necessary, the needle was gently redirected until motor responses were observed at currents of 0.5 mA and, at this point, the test solution was injected. If any resistance was encountered while injecting or if motor responses were observed with currents below 0.5 mA, the needle was slightly withdrawn and redirected to avoid intraneural injection. Per injection site, rabbits in group LB received 0.1 mL/kg of a 1:1 combination of lidocaine 2% (Lidocain, 1 mg/kg; Streuli Pharma, Uznach, Switzerland) and bupivacaine 0.5% (Carbostesin, 0.25 mg/kg; AstraZeneca, Zug, Switzerland) and rabbits in group P received 0.1 mL/kg of 0.9% NaCl. After administration of the test solution, the injection port of the insulated needle was flushed with 0.4 mL of 0.9% NaCl (internal volume of the injection tube) and the needle was subsequently removed. To achieve optimal stifle area anaesthesia, the skin of the dorsocranial aspect of the knee of the rabbits in group LB was infiltrated subcutaneously with 0.125 mL/kg of lidocaine 1% (1.25 mg/kg). Group P received an equivalent volume injection of 0.9% NaCl. After the nerve blocks were performed, the rabbits were placed in lateral recumbency and were prepared for surgery.
Schematic drawing (a) and actual photograph (b) of the medial aspect of the right thigh of an anesthetized rabbit showing the insulated-needle placement and anatomical structures used to localize the femoral nerve with a peripheral nerve locator (PNL; not shown). 1: insulated needle; 2: from cranial to caudal: femoral nerve, artery and vein; 3: inguinal ligament; 4: Musculus (M.) vastus medialis femoris; 5: M. rectus femoris; 6: M. gracilis; 7: Patella; 8: ground electrode of the PNL. Schematic drawing (a) and actual photograph (b) of the lateral aspect of the right thigh of an anesthetized rabbit showing the insulated-needle placement and anatomical structures used to localize the sciatic nerve with a peripheral nerve locator (not shown). 1: insulated needle 2: sciatic nerve; 3: ischial tuberosity; 4: greater femoral trochanter; 5: Musculus (M.) glutaeus medius; 6: M. glutaeus superficialis; dashed line: imaginary line between greater femoral trochanter and ischial tuberosity; the sciatic nerve is located in the middle perpendicular to the skin approximately 0.7–1 cm deep.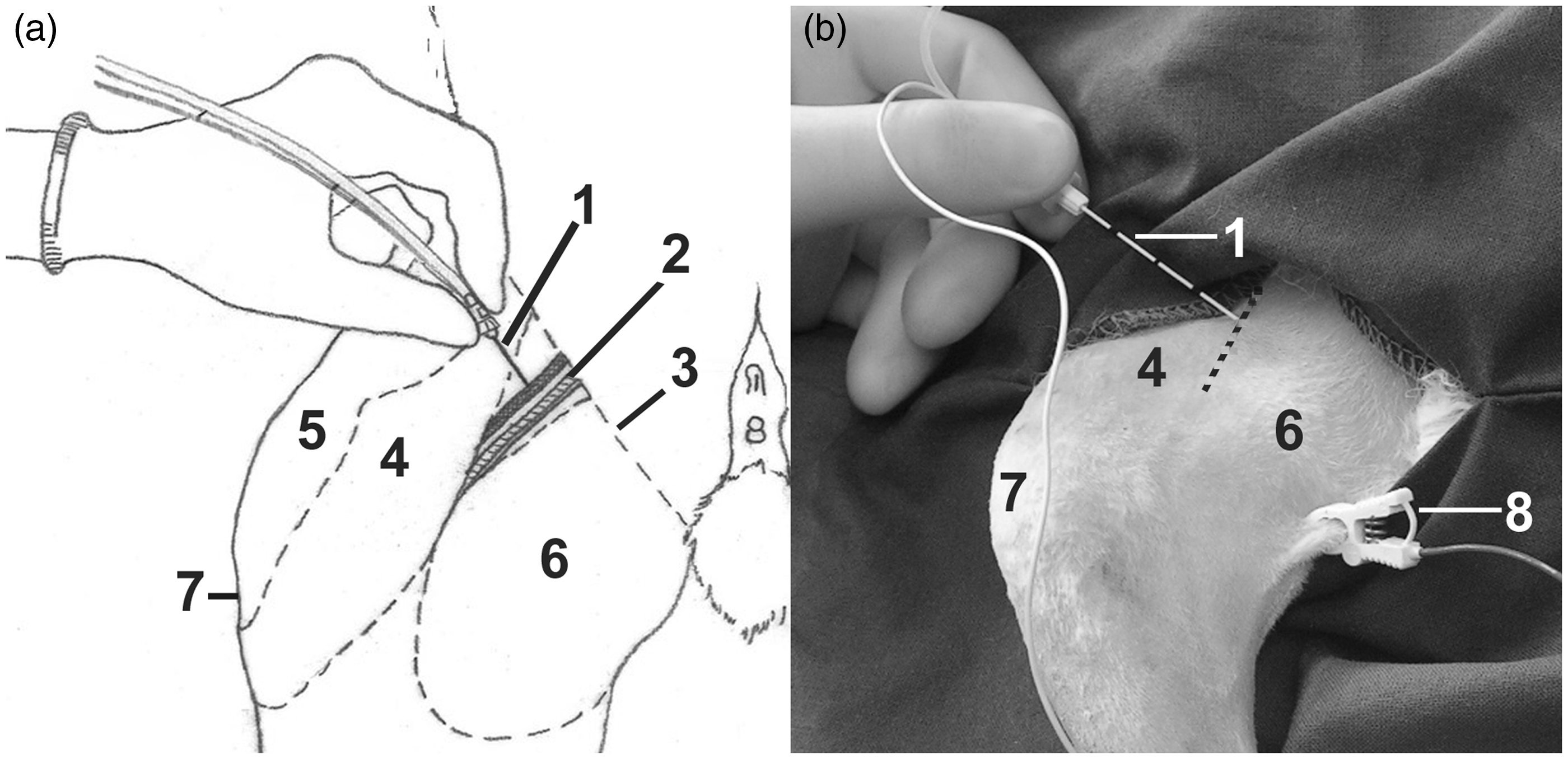
Anaesthesia monitoring and intraoperative nociceptive response assessment and treatment
An anaesthesia monitor (HP CMS 24 Omnicare M1204A, Hewlett Packard, Switzerland) was used to continuously display the following parameters: heart rate (HR) from a lead II electrocardiogram; end-tidal carbon dioxide (EtCO2) and respiratory rate (RR) from a mainstream paediatric capnographic probe using infrared technology; temperature with an electronic probe placed in the oesophagus (Toesop); haemoglobin O2 saturation (SpO2) from a pulse oximetry probe placed on the interdigital skin of a forelimb; direct systolic blood pressure (SAP) from the arterial catheter placed into the middle ear artery that was connected to a calibrated electronic transducer via a fluid-filled non-distensible line (Transducer Set HM6008.1SZB; Codan Medical AG, Baar, Switzerland); and zeroed to ambient pressure at the level of the sternum of the rabbit. All these parameters were manually recorded every 5 min. Baseline HR and SAP were calculated as the mean value of the three consecutive 5 min interval measurements obtained before the skin incision. Surgery consisted of a single incision in the lateral stifle with open arthrotomy and a 4 mm long perpendicular defect 2 mm deep in the femoral condyle was created by the same surgeon.
During surgery either propofol or fentanyl was administered according to the following algorithm:
Presence of palpebral reflex, central eye position, leg withdrawal and/or movement of the whole body were interpreted as insufficient depth of anaesthesia, and propofol (1–2 mg/kg, Propofol 1% MCT Fresenius; Fresenius Kabi, Stans, Switzerland) was delivered intravenously until movement stopped and the dose was noted. A low-grade intraoperative nociceptive response (LGNR) was defined as HR and SAP values increasing 20% above baseline or withdrawal of the operated leg without other signs of awakening from anaesthesia. The nociceptive response was treated with 1 µg/kg fentanyl (Fentanyl; Janssen–Cilag, Baar, Switzerland) intravenously. A high-grade intraoperative nociceptive response (HGNR) was considered to occur when HR and SAP values increased 40% above baseline or if the rabbit withdrew the operated leg several times without signs of awakening from anaesthesia. This response was treated with 2 µg/kg fentanyl intravenously.
At the end of the surgical procedures, isoflurane delivery was discontinued and 100% O2 was delivered until the rabbit swallowed. Thereafter, the endotracheal tube was removed and the rabbit was placed in a recovery cage with infrared light heating. Fluid administration was ceased and both arterial and venous catheters were removed from the ear.
Postoperative pain assessment and treatment
Pain assessment by scoring of behaviour and operated leg manipulation.
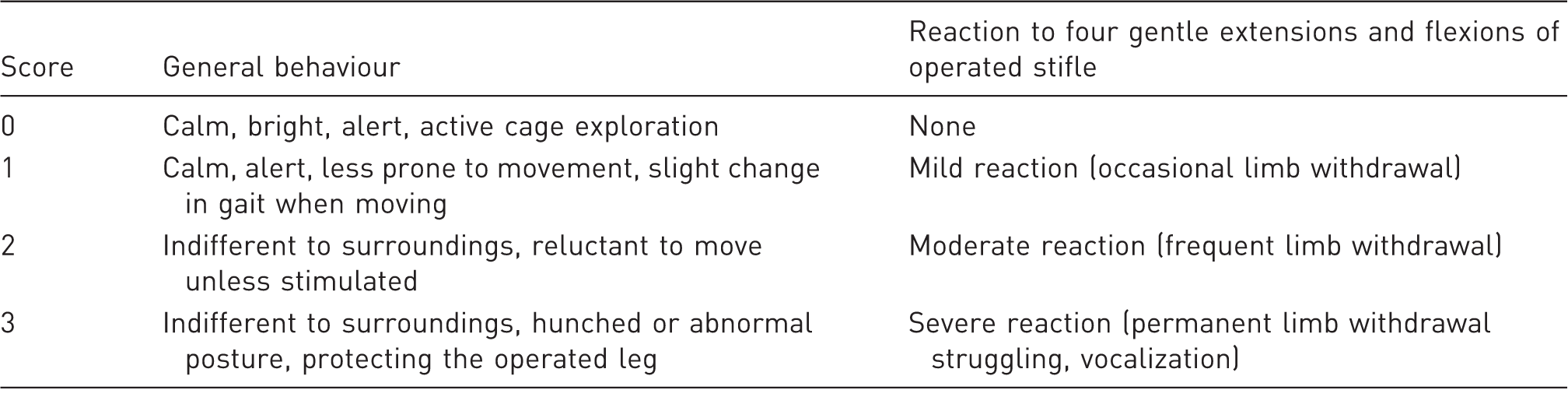
Four-point descriptive scales were used to assess pain in rabbits after stifle joint arthotomy, using behavioural parameters and reactions to operated leg manipulation with the rabbit held in an upright position by the operator (see figure 3 for representation of restraining position). Total score (0–6) derived by adding scores.
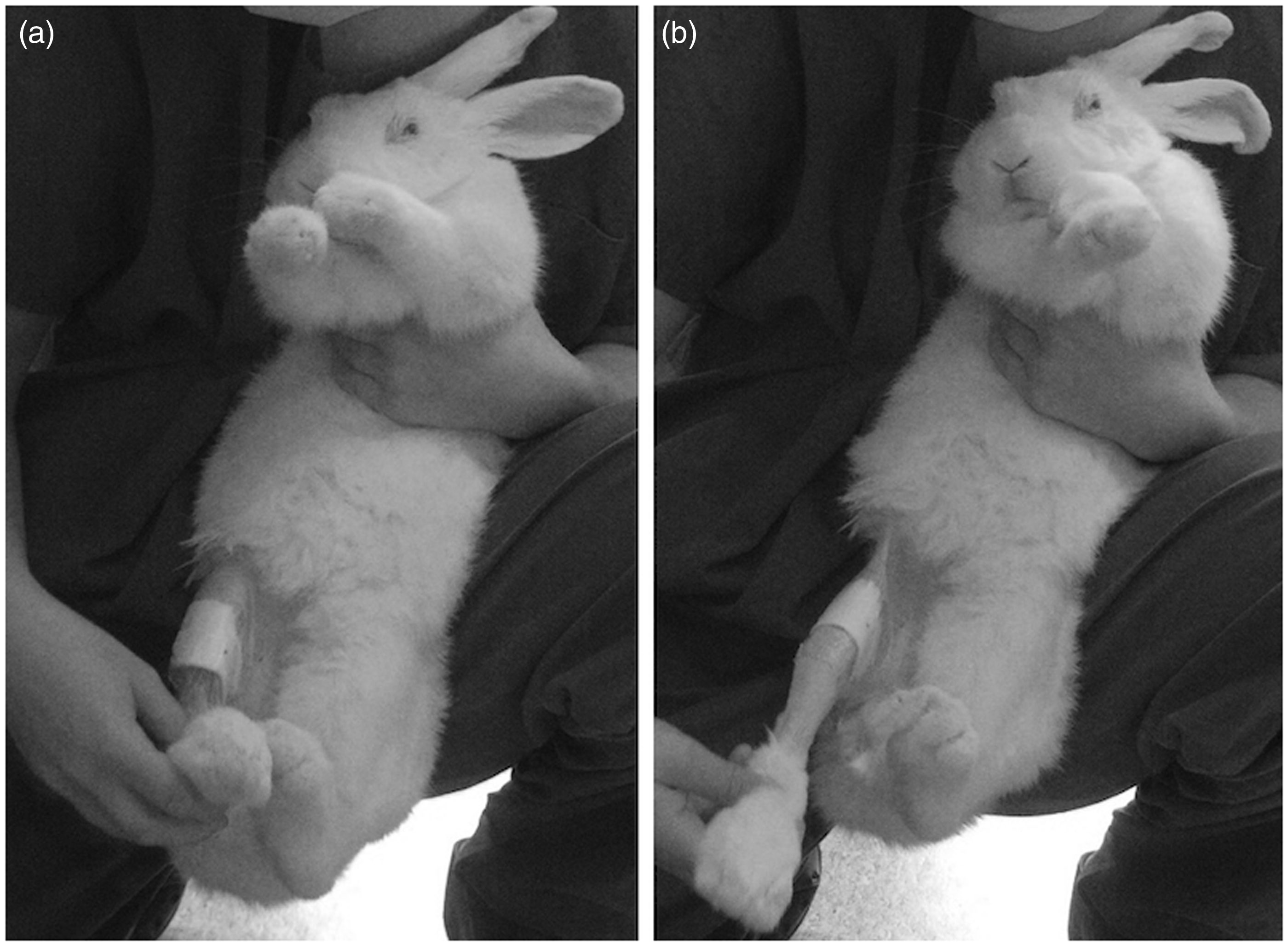
Method of restraint used to evaluate the reaction to gentle flexions (a) and extensions (b) of operated stifle with the rabbit held in an upright position by the operator (see Table 2 for description of scoring system used).
Statistical analysis
For all data analyses, the NCSS 2000 software package (NCSS; Kaysville, Utah, USA) was used and an overall P < 0.05 was considered to be significant. Data were analysed for normality. Data were compared using two-sample Student’s t-tests for parametric and Mann–Whitney U-tests for non-parametric data. Five-minute interval recordings of EtCO2, RR, HR and SAP collected at baseline and intraoperatively were averaged and compared between groups. Parametric data are presented as mean ± SD, non-parametric data as median [range] or interquartile ranges or by using percentages.
Results
Weight, duration of anaesthesia and surgery and baseline and intraoperative cardiopulmonary data of 24 rabbits undergoing stifle joint arthrotomy.
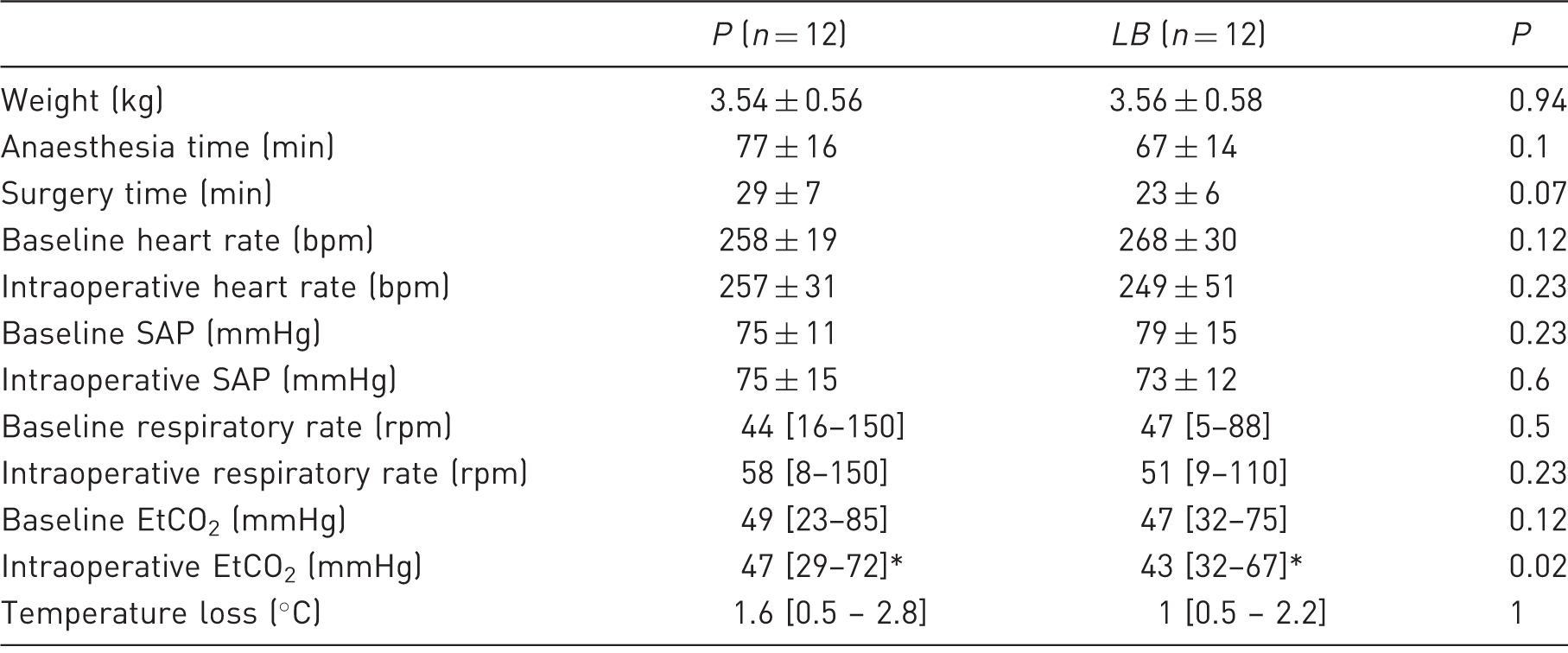
Parametric data are presented as mean ± SD, non-parametric data as median [range]. P: placebo group, LB: treatment group, SAP: systolic arterial blood pressure, EtCO2: end-tidal carbon dioxide partial pressure; *: significant difference.
The sciatic and femoral nerves could be located without complications. None of the rabbits in group LB or group P showed further motor responses after injection.
To achieve an adequate intraoperative anaesthetic plane, nine out of 12 (75%) rabbits in group P and four out of 12 (33%) rabbits in group LB received propofol intraoperatively (P = 0.019). Rabbits in group P received significantly (P = 0.04) higher total doses of propofol (1 [0–4] mg/kg) than those in group LB (0 [0–1] mg/kg).
A significantly higher proportion of rabbits allocated to group P required intraoperative fentanyl (8/12; 67%) compared with those allocated to group LB (2/12; 17%) (P = 0.006). In addition, rabbits allocated to group P required significantly (P = 0.007) higher total doses of intraoperative fentanyl (1.5 [0–3] µg/kg) compared with rabbits in group LB (0 [0–2] µg/kg) to maintain HR and SAP within 20% of the baseline values.
All anaesthetic episodes were uneventful and the rabbits recovered well from anaesthesia.
Two hours after performing the perineural blocks, rabbits allocated to group P showed significantly (P = 0.01) higher VAS scores (37 ± 25 mm) compared with rabbits in group LB (14 ± 10 mm). The numeric rating scales leading to interventional analgesia are presented in Figure 4. The time to postoperative interventional analgesia was significantly shorter (P = 0.007) for rabbits in group P with a median of 2 [range 2–6] h post-block than for rabbits in group LB with a median of 6 [2–6] h post-block. Rescue analgesics were given to 11 of 12 rabbits (92%) in group P and to three of 12 rabbits (25%) in group LB during the 6 h postoperative observation period.
Median and interquartile ranges (box plots; whiskers indicate 75th percentiles) of the scores obtained from the use of a rating scale to evaluate pain (score 0 = no pain/minimal score possible; 6 = severe pain/maximal score possible) in rabbits undergoing knee surgery which received preoperatively saline (a; n = 12, grey boxes) or a combination of lidocaine and bupivacaine (b; n = 12, white boxes) in the proximity of the femoral and sciatic nerves of the operated leg. Scores were performed at 2, 4 and 6 h after test solution injection. Rabbits receiving rescue analgesia were excluded from further analysis (i.e. 8 and 11 rabbits receiving saline and 2 and 3 rabbits receiving local anaesthetics at 4 and 6 h, respectively).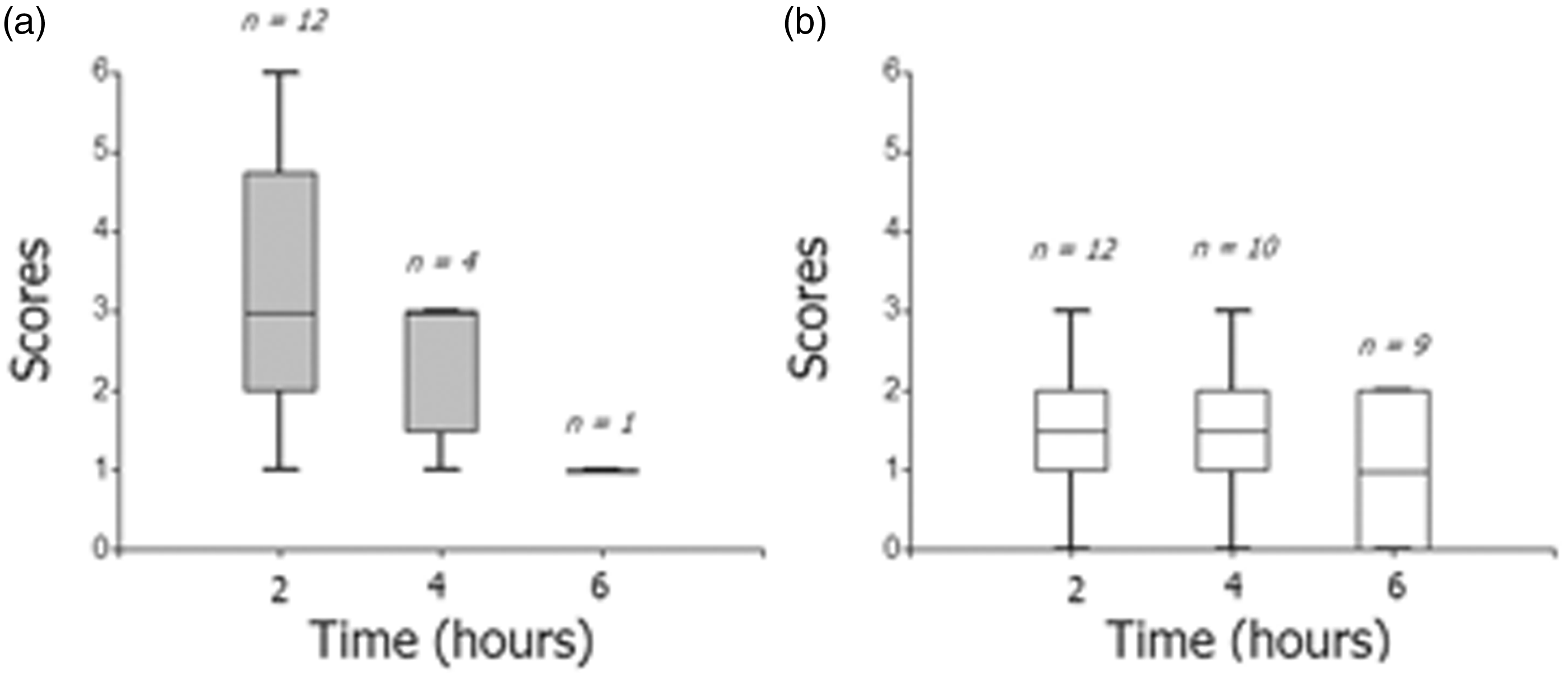
Discussion
In the present study nerve desensitization with a combination of lidocaine and bupivacaine by means of electrolocation combined with subcutaneous infiltration of the incision site proved to be a straightforward and rapid technique for knee arthrotomy using the rabbit model. Local anaesthesia reduced the intraoperative requirements for opioids and propofol and delayed the first dose of postoperative analgesics. In the treated group 17% of the rabbits needed additional analgesia during surgery and 33% were judged to need propofol, indicating some degree of nerve block failure. In the present study, 83% of the animals receiving nerve blocks were considered to have adequate intraoperative analgesia. In contrast to this only 33% of the animals in the control group did not require additional analgesia intraoperatively. Postoperative analgesia was also judged to be superior in the treated group.
Local anaesthetics (in conjunction with general anaesthesia) have been widely used to improve analgesia in both paediatric human patients and in veterinary medicine.15–18 Local anaesthetics act by decreasing the rate and degree of depolarization of the nerve membrane such that the threshold potential for transmission is not reached and the electrical impulse is not propagated along the nerve due to blockade of voltage-gated sodium channels. 19 A local anaesthetic such as lidocaine with a short onset and an intermediate duration of action is often combined with an anaesthetic with a late onset and prolonged duration of action such as bupivacaine. 18 A combination of these two agents in one syringe has been questioned as alteration of pH may alter the dissociation constant for each drug and therefore absorption of the drugs may be compromised.20,21 However, Cuvillon et al. 22 showed that mixtures of long-acting local anaesthetics such as bupivacaine with lidocaine induced faster onset blocks of decreased duration in humans receiving equal volumes of bupivacaine 0.5% and lidocaine 2% for sciatic and femoral nerve blockades for lower limb surgery. The volumes of local anaesthetic solution used in this study were similar to previous investigations in which 0.1 mL/kg per site of bupivacaine 0.5% was enough to block the sciatic and femoral nerves in dogs undergoing tibia plateau levelling osteotomy surgery. 23
Pelvic limb nerve blocks have been shown to provide less haemodynamic changes and urinary retention in people 15 and in dogs 23 when compared with neuraxial blocks (intrathecal or epidural anaesthesia). The incidence of incomplete regional analgesia was higher after pelvic nerve blocks compared with neuraxial anaesthesia for knee surgery in humans, 6 whereas in dogs the analgesia was similar when comparing these two techniques.23,24 The success rate of nerve blockade could not be directly assessed in this study in the anaesthetized rabbits. Efficacy of local anaesthesia was therefore evaluated indirectly based on rescue analgesia requirements. In the current study 17% and 25% of the rabbits in the treated group needed intraoperative fentanyl and postoperative rescue analgesia, respectively. A possible explanation is an incomplete nerve block. Infiltration of lidocaine in the subcutaneous tissue of the dorsocranial aspect of the knee was performed to obtain a more reliable sensory nerve blockade of the skin in this region with possible alternative innervation with supplementary nerve fibres from the obturator nerve. Additionally, low-dose morphine was administered intramuscularly after anaesthesia induction to provide a background level of pre-emptive analgesia.
In humans, the use of a peripheral nerve stimulator to localize nerve trunks significantly increased the success rate when performing this technique compared with the use of only the anatomical landmarks or eliciting paresthesia. 6 The current (0.5 mA) at which the local anaesthesia was injected in the current study was similar to currents used in a previous study (0.47 mA) that showed a mean nerve-needle distance of 2.2 mm, enabling the use of a small injectate volume, and helping to reduce the incidence of side-effects. 12 Possible local side-effects involve inadvertent puncture of the femoral or caudal gluteal vessels with haematoma formation and subsequent nerve compression as well as intraneural injection resulting in nerve damage. 25 Systemic toxicity can cause cardiovascular side-effects such as bradycardia, vasodilation or vasoconstriction and even cardiac arrest if they are injected in large quantities and or are absorbed rapidly. 26 In our study the animals received a total dose of 3.25 mg/kg lidocaine and 0.5 mg/kg bupivacaine. The bupivacaine dose administered was nine-fold lower than the cardiotoxic dose published in rabbits (4.5 mg/kg). 27
The intraoperative variables used in the present study to assess LGNRs and HGNRs (HR and SAP) are commonly used variables to assess sympathetic responses to surgical stimulation in subjects anaesthetized with volatile agents. 28 In the current study, no efforts were made to reduce the delivered concentrations of isoflurane during surgery. The end-tidal volatile anaesthetic concentration was not monitored but all the rabbits were anaesthetized with the same precision vaporizer and O2 flows. Instead of measuring the efficacy of the local blocks by comparing the differences between HR and SAP between groups, we chose to treat the nociceptive responses with fentanyl and to measure and compare the opioid consumption. As a consequence, similar HR and SAP values were found for both groups.
All other measured variables were also found to be similar between groups except for the intraoperative EtCO2. The increase in EtCO2 was probably caused by the significantly higher doses of propofol and fentanyl administered to rabbits allocated to group P when compared with group LB. Both propofol and fentanyl have been associated with respiratory depression in rabbits, 29 leading to reduced alveolar ventilation.
In this study the beneficial effect of local and regional application of local anaesthetics extended to the postoperative period phase with rabbits in group LB requiring postoperative analgesics (buprenorphine and carprofen) significantly later. These results are consistent with a previous study performed in dogs undergoing distal forelimb surgery, which received an injection of a mixture of lidocaine/bupivacaine or saline around the brachial plexus using a nerve stimulator. Most dogs receiving local anaesthetics did not require early postoperative methadone administration. 18
In the current study rabbits in group LB had lower VAS values 2 h post-block indicating better pain relief. However, the use of VAS has been questioned, as it is a subjective method of evaluating pain. Objective evaluation of pain in rabbits is difficult and may lead to biased interpretation as this species often hides pain so as not to become a target for predators.14,30,31 However, significant differences between groups were seen in this study with the methods used. As there are no current pain scales validated for postoperative orthopaedic pain in rabbits, some general behaviours associated with pain after femoral orthopaedic surgery in rabbits 14 were used in this study. In addition, the range of motion of the operated knee was evaluated assuming that if motor and/or sensory fibres of the sciatic and/or femoral nerves were still blocked, the rabbits would allow greater extension or flexion of the joint, otherwise the pain intensity would correlate with the intensity of leg withdrawal. Similar approaches involving the manipulation of the operated extremity have been used by other investigators in several species.32–34 Local and regional techniques have been shown to reduce the postoperative consumption of systemic analgesics in humans. 35 Opioid analgesics, such as buprenorphine, have been associated with the risk of anorexia and gastrointestinal ileus in some rabbit strains. 5
Limitations
In the present study, a technique involving anaesthesia induction and maintenance with isoflurane was selected which aimed to minimize the confounding effects of commonly used injectable anaesthetics in rabbits such as ketamine and sedatives such as medetomidine on intraoperative nociception assessment and postoperative pain evaluation. The use of inhalant anaesthetics as induction agents in rabbits is controversial as these might cause the animals to struggle and hold their breath during the induction phase. 36 Nevertheless, in this study rabbits accepted the anaesthesia induction technique well and endotracheal intubation could be performed without complications after desensitizing the larynx.
In conclusion, the use of femoral and sciatic nerve blockades combined with subcutaneous infiltration of the incision site may be a useful analgesic technique in adult New Zealand White rabbits undergoing stifle joint arthrotomy. It provides a superior anaesthetic regimen compared with placebo-treated animals during and after anaesthesia and less analgesia is required.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.