
Abstract
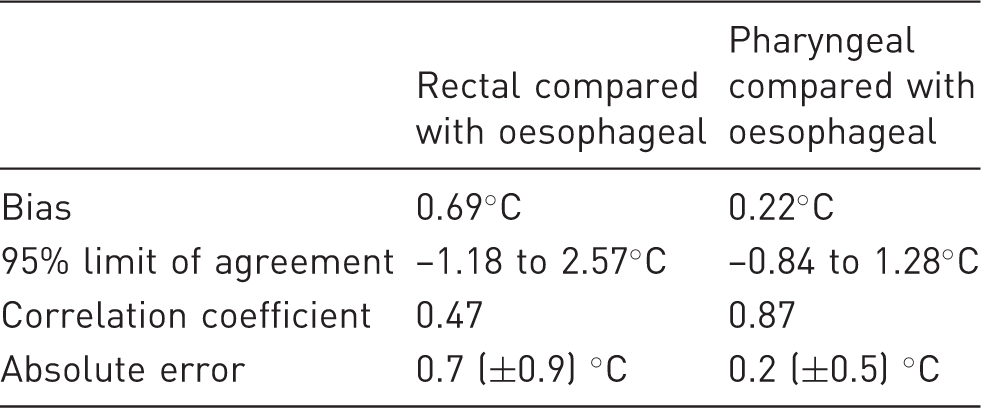
The aim was to compare rectal, pharyngeal and oesophageal temperature measurements in anaesthetized pigs. Data were compared using the Bland–Altman method, and correlation coefficients and error measures were calculated. Sixty-six sets of data were collected from 16 pigs weighing 16.2 ± 4.2 kg. The bias (and 95% limit of agreement) for rectal and pharyngeal compared with oesophageal temperature were 0.69 (–1.18 to 2.57) ℃ and 0.22 (−0.84 to 1.28) ℃, respectively. The correlation coefficients for rectal and pharyngeal compared with oesophageal temperature were 0.47 and 0.87, respectively. The absolute error for rectal and pharyngeal compared with oesophageal temperature was 0.7 ± 0.9℃ and 0.2 ± 0.5℃, respectively. Pharyngeal temperature measurement may be more suitable than rectal temperature measurement for estimation of oesophageal temperature during general anaesthesia of pigs.
Hypothermia is a common complication of anaesthesia and occurs due to altered thermoregulatory control and evaporative and conductive heat loss.1,2 In dogs, the incidence of hypothermia during anaesthesia is 83.6% and the variables that are associated with a decrease in temperature are duration of pre-anaesthetic time, duration of anaesthetic time, body condition, invasive surgery and body position. 2 Hypothermia increases the time to extubation in dogs2,3 but the consequences of hypothermia are not otherwise well reported in animals. In humans, however, the consequences of hypothermia during anaesthesia are well documented and include an increased incidence of surgical wound infections, increased number of post-operative hospital days, increased intra-operative blood loss and requirement for transfusion, prolonged duration of action of anaesthetic drugs, prolonged post-anaesthetic recovery periods, and an increased incidence of morbid cardiac events. 1
There are no data on the incidence of hypothermia in pigs during general anaesthesia, or the consequences of hypothermia, but by extrapolation from other species this anaesthetic complication is likely to occur and may contribute to post-anaesthetic morbidities. In order to manage these complications, reliable measurement, and appropriate management, of core body temperature during anaesthesia are essential. Core temperature cannot actually be measured directly as it is the temperature of the blood bathing the hypothalamus. 4 Methods of core temperature measurement that have been investigated in humans include measurements of blood (pulmonary artery), nasopharyngeal, rectal, axillary, tracheal, tympanic membrane and urinary bladder temperature.4–7 In animals oesophageal temperature is considered to be a reliable representation of core temperature3,8 but rectal temperature is often measured instead. 9
Measurement of core temperature during anaesthesia in pigs is important as this species is commonly used as an animal model in biomedical research. Furthermore, in pigs especially, core temperature measurement facilitates the detection of malignant hyperthermia and quantification of hyper- and hypothermia. 10 This study investigated the accuracy of body temperature measurements in the pharynx and rectum and compared them to oesophageal temperature to determine if these sites were suitable for assessment of core temperature. We hypothesized that the pharyngeal site would be more accurate than the rectum, but that increasing the fresh gas flow delivered through an anaesthetic breathing system may decrease the accuracy of the pharyngeal measurements.
Animals
This study was approved by the Animal Ethics Committee of Murdoch University according to the guidelines of the National Health and Medical Research Council of Australia code of practice for the care and use of animals for scientific purposes. 11 The study population was a convenience sample of 16 large white pigs (Sus scrofa) utilized in surgery and anaesthesia teaching for veterinary students.
Materials and methods
The animals were weighed and anaesthetized with a combination of zolazepam and tiletamine as Zoletil 100 (4 mg/kg; Virbac Australia Pty Ltd, Milperra, NSW, Australia) and xylazine (2 mg/kg, Ilium Xylazil 100 mg/mL; Troy Laboratories Australia Pty Ltd, Glendenning, NSW, Australia) by intramuscular injection in the neck. An auricular vein was cannulated and propofol (1–2 mg/kg, 1%; Norbrook Laboratories Ltd, Tullamarine, Victoria, Australia) was administered intravenously if required to achieve an adequate depth of anaesthesia for orotracheal intubation. Anaesthesia was maintained with isoflurane (Attane Isoflurane 1 mL/mL; Bayer Australia Ltd, Pymble, NSW, Australia) delivered in oxygen via a Bain (Vetquip, Castle Hill, NSW, Australia) breathing system (for pigs <10 kg) or a Circle (Fisher and Paykel Healthcare, East Tamaki, Auckland, New Zealand) breathing system (for pigs >10 kg). The pigs breathed spontaneously unless the end-tidal carbon dioxide (ETCO2) exceeded 55 mmHg in which case manual intermittent positive pressure ventilation (IPPV) was commenced. The fresh gas flow was set and maintained at 200 mL/kg/min for the Bain breathing system and at 2 L/min for the circle breathing system. The fresh gas flow was altered with the circle breathing system to collect data on a range of fresh gas flows.
A veterinary student under supervision of an experienced veterinary anaesthetist assessed the depth of anaesthesia subjectively throughout the procedure, and the delivery of isoflurane was adjusted accordingly (vaporizer setting: 0.5–2.5%). Oxyhaemoglobin saturation, pulse rate, heart rate, respiratory rate, ETCO2, non-invasive arterial blood pressure and an electrocardiogram were monitored continuously and recorded every 5 min. All variables were measured with a Surgivet V9203 multivariable monitor (Polymount GCX® Corp, Petaluma, CA, USA). The pigs were euthanized with intravenous pentobarbitone at the end of surgery.
Three thermometers were utilized in this study. The Surgivet temperature probe was used to measure oesophageal temperature and two new handheld digital thermometers were used to measure the rectal temperature and the pharyngeal temperature (Surgipack Clear Tip Digital Thermometer; Tyco Healthcare Pty Ltd, Lane Cove, NSW, Australia). At the beginning of each study day all three thermometers were simultaneously immersed in water baths between 35.6 and 43.9℃. The maximum difference between the thermometers was 0.4℃. The oesophageal temperature probe remained in situ for the duration of the anaesthesia while the handheld probes were positioned for each measurement and the temperature was recorded when the device beeped after one minute and according to the manufacturer’s instructions. The oesophageal temperature probe was positioned so the tip was approximately at the level of the heart base. The rectal thermometer was positioned so it was at least 5 cm within the rectum and the pharyngeal thermometer was positioned in the mouth so the tip was adjacent to the soft palate. The fresh gas flow was also recorded at each time point. The pigs were actively warmed with electronic heat pads or circulating warm air blankets to maintain normothermia.
Data were analysed using the Bland–Altman method to calculate the bias and 95% limit of agreement. Correlation coefficients and error measures were also calculated and the impact of the fresh gas flow on the difference between the temperature measurements was determined. Data are expressed as mean (±SD).
Results
Bland–Altman analysis, correlation coefficient and absolute error of rectal and pharyngeal temperatures compared with oesophageal temperature measured simultaneously.
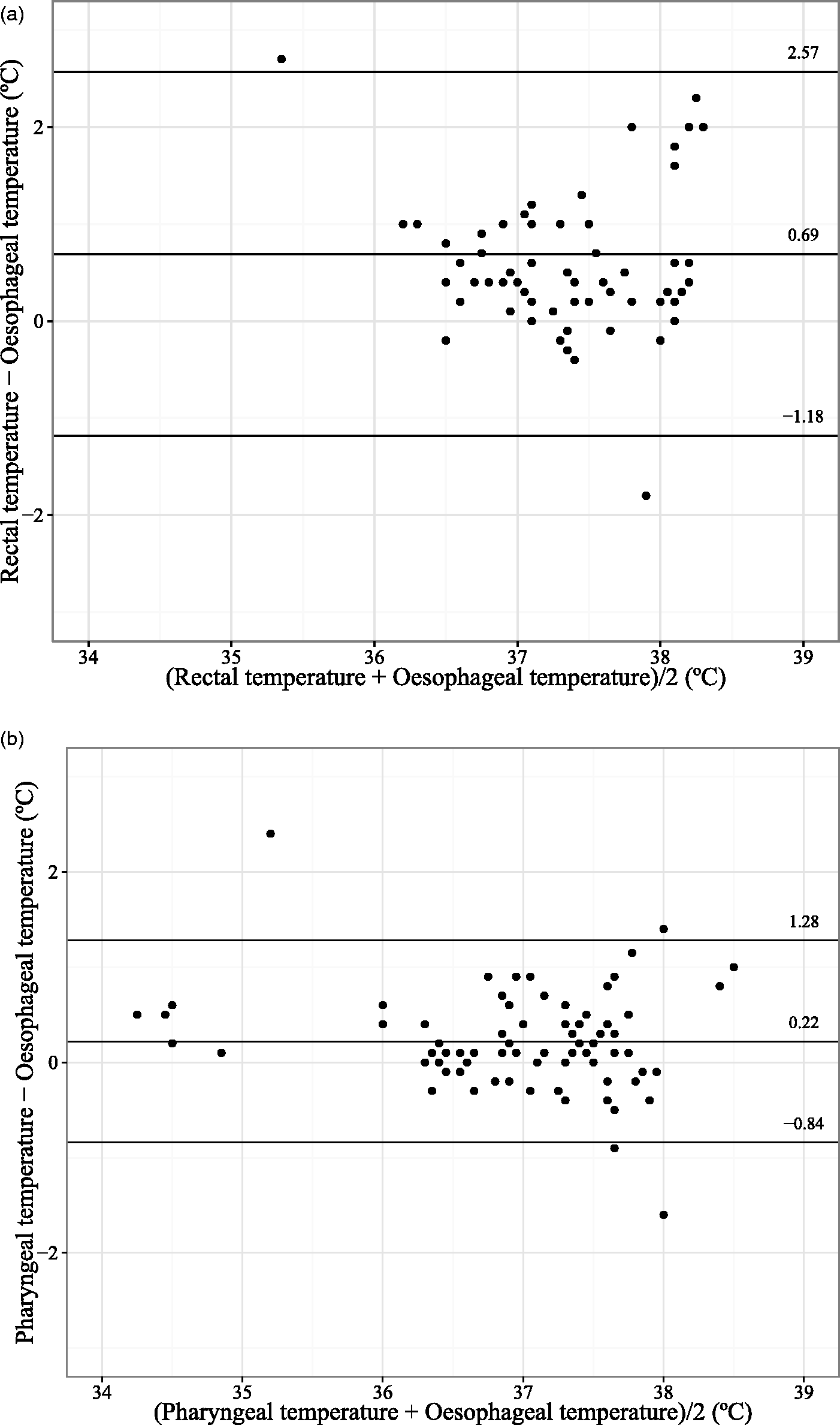
(a) Bias and 95% limit of agreement for rectal compared with oesophageal temperature. (b) Bias and 95% limit of agreement for pharyngeal compared with oesophageal temperature.
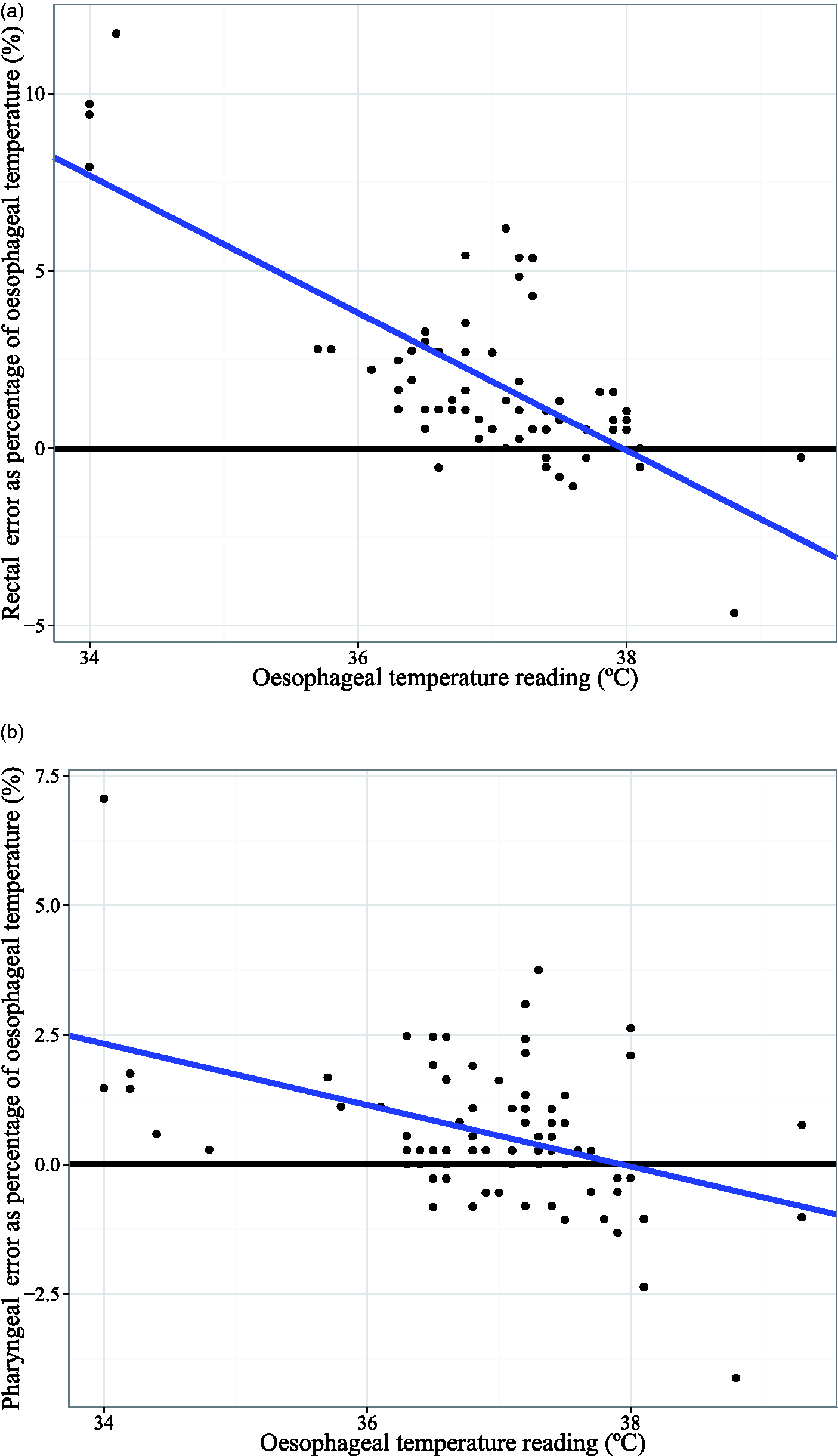
(a) Correlation between oesophageal and rectal temperatures and the absolute error (difference between rectal and oesophageal temperature/oesophageal temperature and expressed as a percentage). (b) Correlation between oesophageal and pharyngeal temperatures and the absolute error (difference between pharyngeal and oesophageal temperature/oesophageal temperature and expressed as a percentage).
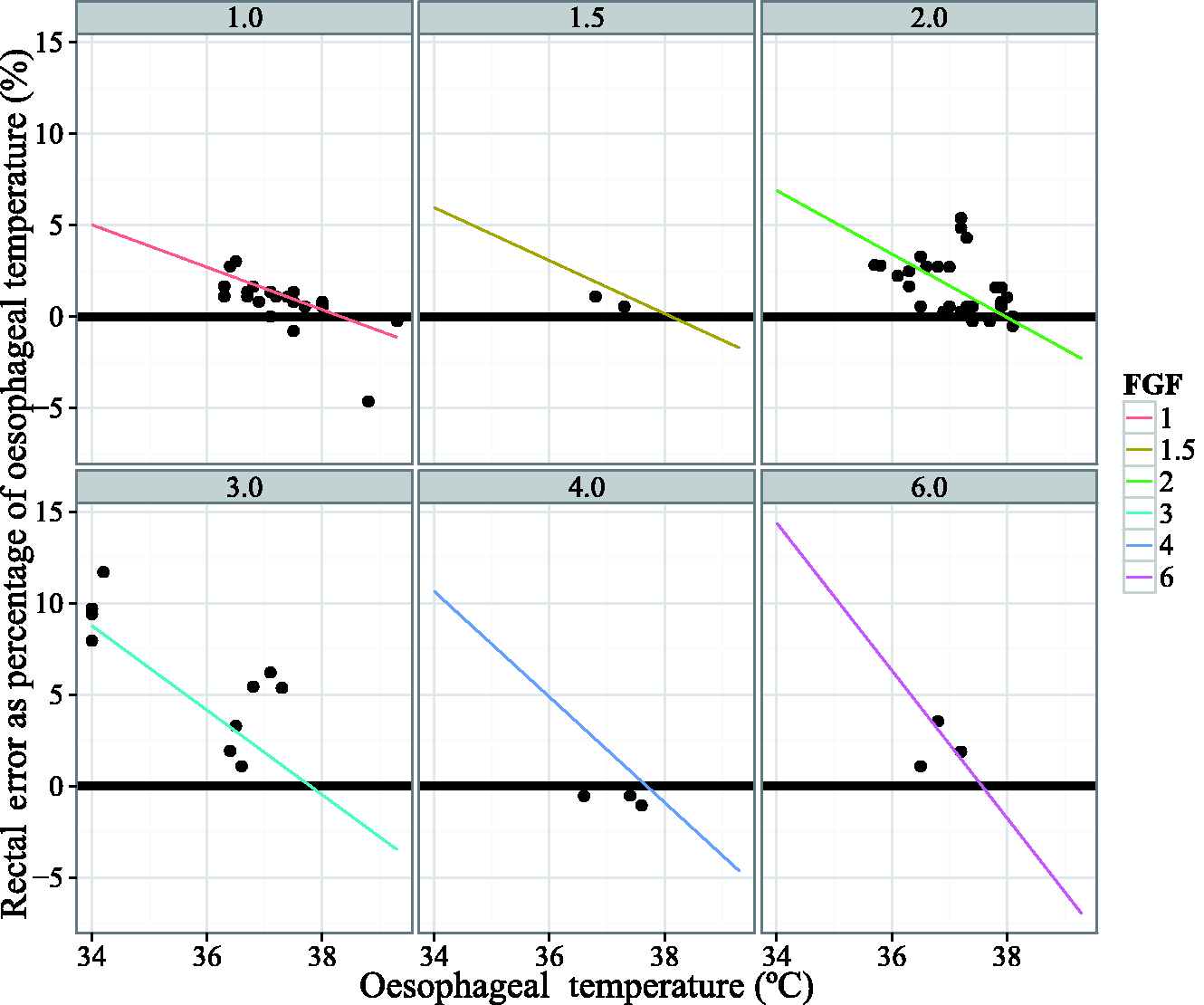
Correlation between oesophageal and rectal temperatures and the absolute error according to the fresh gas flow.
Discussion
The temperature measured by placing the tip of a handheld digital thermometer adjacent to the soft palate gave a more accurate representation of oesophageal temperature than the rectal temperature during anaesthesia of large white pigs weighing 16.2 (±4.2) kg. In dogs, rectal temperature measurement provides an accurate estimate of core temperature, 12 however accuracy may be affected by the presence of faeces and air in the rectum and by local blood flow in the rectal mucosa. 4 Pharyngeal temperature measurements have been reported in anaesthetized dogs 13 and in human patients for estimation of core body temperature. 6
This study compared rectal and pharyngeal temperature measurements with oesophageal temperature measurement because in anaesthetized pigs undergoing surgery these sites are accessible and instrumentation is relatively non-invasive. While other sites have been investigated in human patients, the aim was to determine whether sites that met the aforementioned criteria for convenience were appropriate for an estimation of core body temperature. The factors that affect the accuracy of measurements are those that create a temperature gradient between measurement sites. These factors include the ambient temperature, the rate of change in temperature and the local blood supply. 4 In humans, pharyngeal measurements are reported to be as accurate as oesophageal temperature measurements 14 for approximation of brain temperature, but the authors state that monitoring multiple sites is the best approach when accurate knowledge of brain temperature is critical. During re-warming of hypothermic human patients rectal temperature is very slow to change so the rectum may not be the best site for approximation of core temperature. 15
The carrier gas for inhalant anaesthetic drugs is cold and dry and may impact upon the local temperature at the pharyngeal site as the endotracheal tube is adjacent to the soft palate. Our hypothesis was that increasing the fresh gas flow decreases the accuracy of the pharyngeal temperature measurements. Fresh gas flow has no influence on pharyngeal measurement accuracy between 1 and 6 L/min but the rectal temperature measurements became more inaccurate with a higher absolute error as the fresh gas flow increased. This result was unexpected and is difficult to explain. One explanation is that the small data set may be overemphasizing this result. Another issue may be that the fresh gas flow has an influence on both the pharyngeal and oesophageal measurements to the same extent, thereby altering these results simultaneously. The rectal temperature measurements are unlikely to be affected by the fresh gas flow and therefore the difference between the oesophageal and rectal readings may be accentuated. Hitherto investigations into the impact of fresh gas flow and temperature measurement at different sites is warranted. These investigations should include assessment of local blood flow at the temperature measurement site and determination of the temperature gradient between the endotracheal tube through which the fresh gas flow passes and the surrounding soft tissues.
As a difference of >0.5℃ is considered unacceptable for different methods of temperature measurement, 12 bias was lower and the correlation coefficient was higher, pharyngeal temperature measurement may be more suitable than rectal temperature measurement for estimation of oesophageal temperature during general anaesthesia in pigs.
Footnotes
Acknowledgements
The authors would like to thank Kim Thomas for the care and husbandry of the pigs prior to anaesthesia and surgery, and Ann Graham for nursing assistance during the practical classes.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.