
Abstract
The aim of this study was to find the fastest, easiest and safest method of achieving orotracheal intubation for general anaesthesia in laboratory pigs. Twenty-one Yorkshire × Landrace crossbreed male castrated pigs (32.9 ± 4.8 kg) were investigated. Dorsal and ventral recumbency are the alternatives most frequently described for animal positioning during intubation procedures. Based on standardized induction of general anaesthesia using pentobarbital and remifentanil, the dorsoventral and ventrodorsal positions were compared with regard to the time needed, changes in oxygenation and circulatory response. Positioning was found to be crucial for fast orotracheal intubation. The time required for safe intubation is significantly shorter with the ventrodorsal position (17.3 s) in comparison with the dorsoventral position (58.4 s; P < 0.001). Hypoxia did not occur in either group. A significant drop in systolic blood pressure was observed in both groups. Diastolic and mean arterial pressures were not influenced by intubation. A significant increase in heart rate was observed in pigs intubated in ventral recumbency, but not after intubation in the dorsal position. Preoxygenation before intubation is vitally important for preventing hypoxia. With regard to clinical practice, the haemodynamic changes observed in this investigation do not appear to be relevant, as the mean arterial pressure was not altered and heart rates only increased moderately. It may be concluded that the ventrodorsal position can be recommended for orotracheal intubation in pigs as the first choice for providing a smooth and fast airway.
John Hunter, in the 18th century, was the first to describe pigs (Sus scrofa) as being suitable models for use in experimental biomedicine. 1 In recent years, domestic pigs have become very popular for this purpose and have replaced the traditional canine models for investigations on topics including transplantation, shock, cardiology and gastrointestinal physiology. 2–6
In accordance with animal welfare requirements and good laboratory practice, adequate anaesthesia is required for surgical procedures and various examinations in swine. In this context, safe and standardized orotracheal intubation is very important. However, achieving endotracheal intubation in pigs is still regarded as being technically difficult. 5,7–9 Failed endotracheal intubation after induction of anaesthesia, resulting in hypoxia and death, is regrettably common, even when experienced scientists are performing the procedure. 10–13 As intubation is challenging in pigs, many scientists avoid the procedure. 14 Various authors have strongly recommended using spontaneously breathing animals and avoiding any airway precautions, in order to prevent major problems developing due to intubation manoeuvres. 9,15,16 Other groups favour mechanical ventilation but prefer a primary tracheotomy, as they consider that pigs easily develop laryngospasms and other complications during intubation. 16–18 Since spontaneous respiration is associated with many risks and tracheotomy is an invasive procedure, various techniques have been proposed for managing the problems caused by orotracheal intubation. 6,19–23
These techniques differ particularly with regard to the positioning of the animal during intubation. The present study investigated the two positions most frequently used – the ventrodorsal and dorsoventral positions. The aim was to determine the influence of positioning on the time needed for the intubation manoeuvre, on changes in oxygenation and finally on haemodynamic responses. In addition, the anatomical structures were visualized during the intubation procedure. The results have been summarized in this paper in order to provide evidence-based procedural advice.
Materials and methods
Animals
The study was approved by the Institutional Animal Use Committee (Department of Veterinary and Food Surveillance, Regional Administration for Münster; G62/2003). Twenty-one healthy Yorkshire × Landrace crossbreed male castrated pigs (UPB Deutschland Ltd, Drensteinfurt, Germany), which were free of endoparasites and ectoparasites, were included. Before the investigation, the pigs were randomly assigned to one of two study groups involving intubation in either the dorsoventral position (n = 10) or ventrodorsal position (n = 11). The randomization list was generated by a special software program (RandList version 1.0, DatInf Ltd, Tübingen, Germany).
The mean body weight of all the pigs was 32.9 ± 4.8 kg. There were no differences in body weight between the two groups (dorsoventral position group 33.6 kg, interquartile range 27.0 kg, 35.2 kg; ventrodorsal position group 33.6 kg, interquartile range 31.1 kg, 35.2 kg). Equivalent baseline conditions were thus ensured in both groups with regard to anatomical characteristics, i.e. the width of the pharynx, larynx and trachea.
Housing
To allow them to adapt to their new environment and to prevent stress, the animals were housed in the University of Münster's animal facility for at least 14 days before the investigation. Room temperature was maintained within the range of 20–22°C. The relative humidity was approximately 40–70%. The pigs were housed together with their pen mates. The room was adjusted to make the animals comfortable, and they were able to lie down with outstretched limbs or move around.
Feeding
The pigs were fed a commercially available standard ration of pellets and water in open troughs and watering places. Food, but not water, was withheld for 18 h before the induction of anaesthesia.
Premedication and sedation
Sedation was achieved by intramuscular administration of 3.75 mg/kg tiletamine, 3.75 mg/kg zolazepam (Zoletil, Virbac France SAS, Carros, France; contains tiletamine and zolazepam) and 1.5 mg/kg xylazine (Xylazin 2%, Alvetra, Neumünster, Germany). 5,24–26 After the onset of sedation, the pigs were placed on the operating table in the ventrodorsal or lateral position. A 20-G intravenous (i.v.) line and a 22-G arterial cannula (Insyte, Becton Dickinson, Heidelberg, Germany) were inserted into an auricular vein and artery, respectively. Infusion of Ringer's solution (Delta Select, Dreieich, Germany) was started at a rate of 3 mL/kg/h. Vital signs were monitored using pulse oximetry (PM 8050, Dräger, Lübeck, Germany), invasive arterial pressure measurement and electrocardiography (SMK 154-9, Hellige, Freiburg, Germany).
Anaesthesia
All the animals were preoxygenated for at least 5 min via a tight-fitting facemask with 100% oxygen delivered at a flow rate of 15 L/min from an anaesthetic machine (AV-1, Dräger). Anaesthesia was induced by i.v. administration of 22.5 mg/kg pentobarbital (Narcoren, Merial, Hallbergmoos, Germany) and continuous infusion of 0.25 μg/kg/min remifentanil (Ultiva, GlaxoSmithKline, Munich, Germany) in accordance with general practice. 27–32 No neuromuscular blocking agents were used. At the onset of apnoea, the animals were moved into either dorsal or ventral recumbency in accordance with their randomization. Depending on the position, the head (dorsal position) or the legs (ventral position) were allowed to overhang the operating table slightly. All of the intubation manoeuvres were carried out by the same investigator (MMT) in accordance with the technique described previously. 8,19,21,33 In summary, an assistant opened the pig's mouth widely using two loops made of gauze and applied to the animal's upper and lower jaws. The neck was moderately dorsiflexed during this procedure. The tongue was extracted using a gauze compress for improved grip. The laryngoscope was then carefully introduced until the soft palate became visible, with the palatal velum and ventral surface of the epiglottis. The epiglottis was drawn into the oropharynx by capturing it gently with the tip of the laryngoscope blade. Aligning the epiglottis in this way exposes the entrance to the larynx. An orotracheal Magill-type tube (Super Safety Clear, Rüsch PLC, Kernen, Germany) with an inner diameter of 6.5 mm was inserted into the laryngeal entrance. The convex side of the tube was placed facing upwards, as this makes introduction into the entrance of the larynx easier due to the anatomical structures. While the tube was being advanced, it was rotated 180° to allow a smooth procedure. After the tube had been inserted, the cuff was blocked immediately and the animal was connected to the anaesthetic machine for ventilation. Correct positioning was verified by confirmation of carbon dioxide indicated by the anaesthetic gas monitoring system (PM 8050, Dräger) and by auscultation of the thorax. Initially, the tidal volume was set at 10 mL/kg and the respiratory rate was 12–18 breaths/min; the peak inspiratory pressure did not exceed 20 cmH2O. During anaesthesia, ventilation was adjusted according to the results of blood gas analyses and end-tidal capnometry.
Measurements
Immediately before and after successful intubation, the peripheral pulse oximetric oxygen saturation, heart rate and mean arterial pressure were recorded. The time needed for the complete intubation procedure was recorded using an electronic stopwatch. The time measurement was started at the beginning of the laryngoscope insertion and detection of carbon dioxide was defined as the endpoint of the intubation procedure.
Statistics
Statistical data were collected and computed using commercially available statistical and graphic software (SigmaStat 2.0, SigmaPlot 2000, Jandel Scientific Corp, Erkrath, Germany). For normal distributions, t-tests were carried out for intragroup and intergroup comparisons. For data that did not have a normal distribution or had equal variance, the Mann-Whitney rank sum test was used for intragroup and intergroup comparisons. A Pearson product moment correlation was carried out to verify the correlation between heart rate and the length of the intubation manoeuvre.
Visualization of anatomy during intubation
For detailed anatomical and procedural visualization, pictures were taken with a digital camera (Exilim Zoom EX-Z40, Casio, Norderstedt, Germany). The images were edited using freeware photo-processing software (iPhoto Plus 4.0, Ulead Corp, Corel Ltd, Unterschleissheim, Germany; SnagIt 8.2.3, TechSmith Corp, Okemos, MI, USA).
Computed tomography (CT) scans were obtained from comparable pigs that were originally scheduled for CT investigations in another porcine model. 34 A 64-slice device was used for CT (LightSpeed VCT, GE Medical Systems, Milwaukee, IL, USA). The examination protocol consisted of an arterial contrast-enhanced scan and a supplementary venous phase with automatic i.v. injection of 100 mL non-ionic iodinated contrast medium (370 mg/mL iodine). The scan parameters were standardized (tube current 120 kV and 140 mAs; collimated slice thickness 64 × 0.64 mm; total detector width 40 mm; rotation speed 0.5 s; table feed per rotation 40 mm), resulting in a scan speed of approximately 8 s for a 30 cm scan length on the z-axis. Image analysis was carried out using Advantage Windows 4.2 (GE Medical Systems, USA) and AccuLite (AccuImage Diagnostics Corp, South San Francisco, CA, USA).
Results
Data from all 21 animals were obtained for analysis in this study. The first attempt of orotracheal intubation was successful in all the animals. Using the technique described above, no tube displacements or other intubation-related complications were observed.
Intubation manoeuvres in the ventrodorsal position took significantly less time than those in dorsal recumbency. The mean duration in the ventral recumbency group was 17.3 s vs. 58.4 s in the dorsal recumbency group; the power of the test performed was 0.986 (Table 1). No hypoxia was observed in either group (Table 2). Heart rates in pigs intubated in the ventrodorsal position increased significantly after intubation, but did not significantly exceed the values monitored for animals intubated in the dorsoventral position (Table 2). Analysis of the correlation between the total time needed for intubation and the heart rate after intubation was carried out for both groups, but did not show any significant relationship between these two variables (correlation coefficient 0.066, P value 0.86 in the dorsoventral position group; 0.26 and 0.45 in the ventrodorsal position group, respectively). After intubation, systolic blood pressure decreased in both groups, but diastolic blood pressure decreased only in the dorsoventral group. In both groups, the mean arterial pressure was not influenced by intubation.
Duration of orotracheal intubation manoeuvres in 21 laboratory pigs
Data are medians and interquartile ranges
*P < 0.001 for dorsoventral vs. ventrodorsal position
Haemodynamic and oxygenation variables during orotracheal intubation in 21 pigs
Data are medians and interquartile ranges. SpO2: peripheral oxygen saturation; HR: heart rate; SAP: systolic arterial pressure; DAP: diastolic arterial pressure; MAP: mean arterial pressure
*Significant at P < 0.05 vs. the value before intubation
Since ventral recumbency provides a clear view of the larynx, compared with a Cormack and Lehane grade 1 situation in humans, images for illustration (Figures 1 and 2) were easily obtained. 35 In contrast, it was not possible to take any pictures showing the exposed larynx during conventional laryngoscopy in dorsal recumbency. This emphasizes the fact that visualization of the larynx is significantly reduced and that the oropharyngeal space is narrowed with the dorsoventral position.
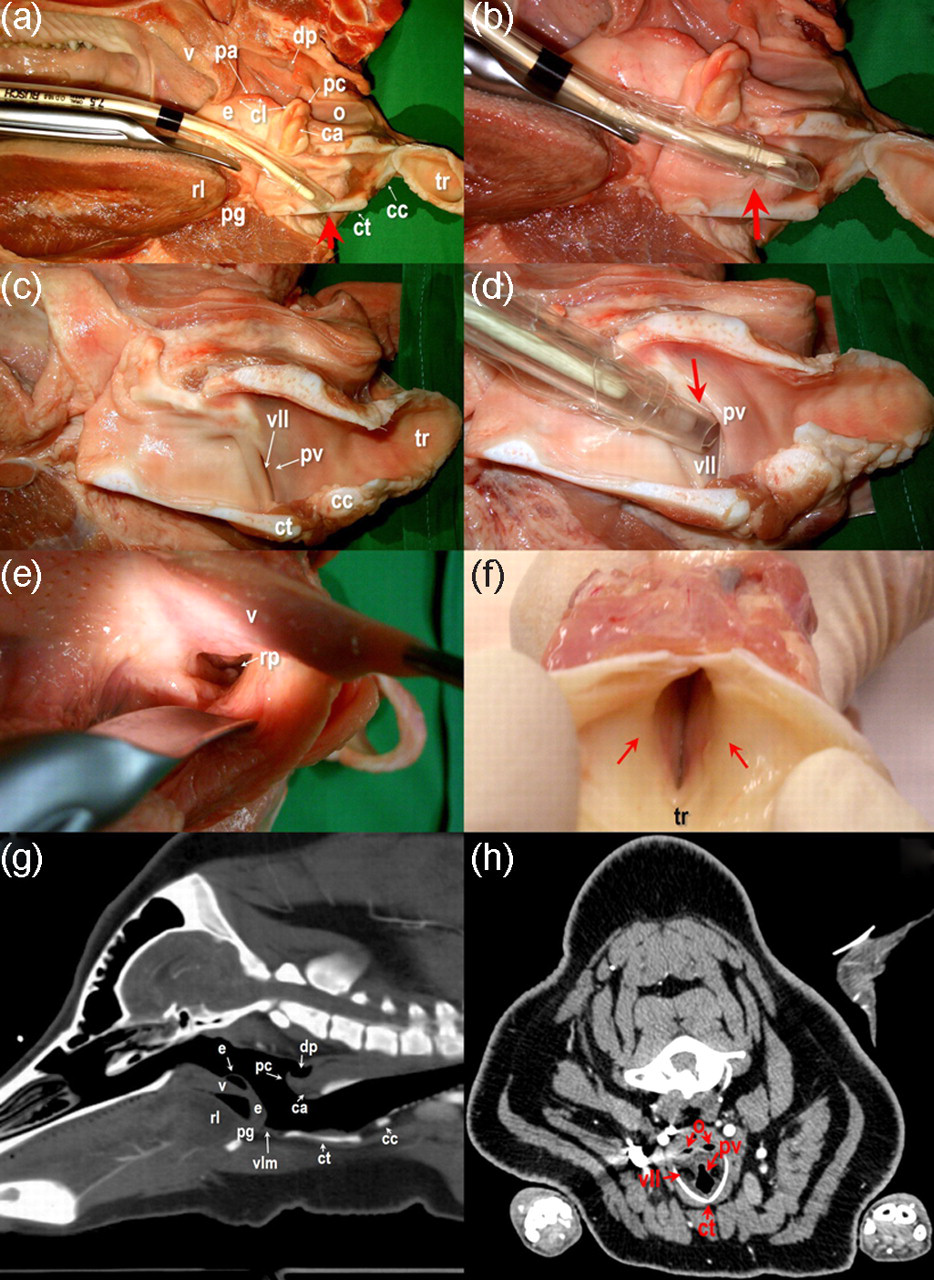
Essential anatomical characteristics during intubation in pigs: anatomical transections and computed tomograms (CTs). (a) The tube becoming stuck at the thyroid or cricoid cartilage (arrow). (b) 180° rotation of the tube during advancement to the trachea solves the problem (arrow). (c) Close-up view of the lateral ventricle of the larynx. (d) The arrow indicates the tube becoming trapped in the lateral laryngeal ventricle. (e) The wrong direction for ‘tracheal’ intubation: view into the recessus piriformis. (f) View from the trachea towards the larynx. The arrows indicate the subglottic constriction of the trachea, a potential problem in advancing the tube. (g and h) The anatomy shown in the corresponding CT scans ca: cartilago arytenoidea; cc: cartilago cricoidea; cl: ‘corona laryngis’; ct: cartilago thyreoidea; dp: diverticulum pharyngeum; e: epiglottis; o: oesophagus; pa: plica aryepiglottica; pc: processus corniculatus; pg: plica glossoepiglottica mediana; pv: plica vocalis; rl: radix linguae; rp: recessus piriformis; tr: trachea; v: velum palatinum; vll: ventriculus laryngis lateralis; vlm: ventriculus laryngis medianus
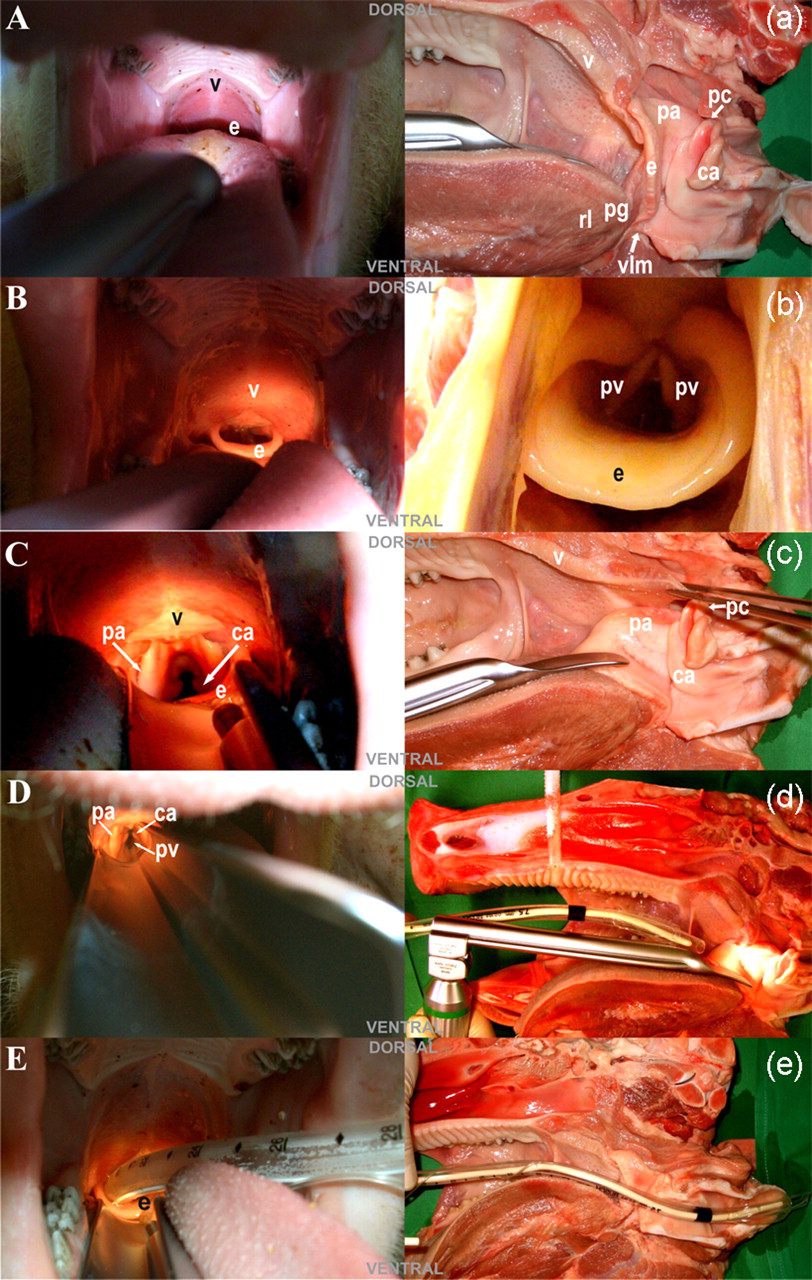
Orotracheal intubation in pigs. Demonstration of the procedure, with the corresponding anatomical sagittal sections. (A/a) The view along the tongue; the soft palate and back of the epiglottis, which obstructs a clear view of the entrance to the larynx. (B/b) The epiglottis, dislocated in the oropharynx; the ‘corona laryngis’ is visible. (C/c) The epiglottis has been captured by the laryngoscope blade. This manoeuvre improves the view of the deeper laryngeal structures. (D/d) The vocal folds are dimly visible in the deep larynx after slight forward movement of the laryngoscope. (E/e) The situation after correct intubation: the tube is in place. See Figure 1 for abbreviations
Discussion
The main result of this study is the finding that orotracheal intubation of pigs can be performed much faster and therefore more easily in the ventrodorsal position than in the dorsoventral position. This is due to better visualization of the pharyngeal and laryngeal structures during laryngoscopy, as well as the greater extension that can be provided by the technical assistant. In addition, optimal handling of the equipment is ensured by the ergonomic working position of the researcher that is achieved when intubation is carried out with the animal in the ventral recumbency position.
The animal's oropharyngeal anatomy has been described as being the main reason why orotracheal intubation is more complicated in pigs than in any other domestic animal. 11,19,21,36 The major anatomical characteristics responsible for potential problems during orotracheal intubation are the long, beak-like snout and the small, narrow and long oropharyngeal cavity filled with a wide and thick tongue. The epiglottis is usually hidden by a large and floppy soft palate, in such a way that the elongated epiglottis reaches the epipharynx, closely fitting the velum of the soft palate. A pharyngeal diverticulum and a narrow larynx with one large ventral and two lateral ventricles are other very specialized characteristics. The larynx is long, narrow and easily relocatable, lying at an angle to the trachea. The distance between the laryngeal entrance and the glottis is elongated in comparison with many other laboratory animals. Angular, caudoventrally positioned, slit-like vocal cords and a sigmoidal laryngeal passage are further characteristics of porcine laryngeal anatomy. The tendency of the pig to develop laryngospasm easily also has to be taken into account (Figure 1). 7,8,10–12,15,21,22,37–42 These anatomical characteristics are clearly substantial obstacles to porcine orotracheal intubation. However, if the procedure is carried out with the animal in ventral recumbency, most of these hindrances are alleviated. The positioning of the animal is therefore crucial for completing the procedure in the majority of animals with these anatomical peculiarities.
In general, the findings of the present study confirm the results published by other groups, who have pointed out that intubation in the ventrodorsal position is associated with better results and a lower complication rate. 8,33 Many reports have strongly recommended using the ventrodorsal position for orotracheal intubation of swine, although without presenting any evidence-based data for the recommendation. 4,7 In contrast to these authors, as well as to his own earlier publications, Swindle 6 has stated in his latest monograph that the position used is not relevant to successful intubation in swine. He only suggests dorsal recumbency in pigs with a total body weight of less than 50 kg. 6 Earlier studies by authors favouring the dorsoventral position should also be mentioned. 36,37,43 The preference for dorsal recumbency is probably due to the fact that clinicians are accustomed to performing intubation in this position in humans. 44 However, it should be noted that none of the authors concerned have provided support for this recommendation with any objective data.
Evaluation of haemodynamic parameters in the present study revealed interesting results. Heart rate in the ventrodorsal group was significantly higher after intubation in comparison with the dorsoventral group. As the same anaesthesia regimen was used in both groups, and hypoxia was strictly prevented by preoxygenating the animals via a facemask, the differences appear to be due to the different positioning of the animals. Higher heart rates would usually be attributed to higher levels of stress and/or hypercapnia. 45 However, hypercapnia was not observed as a cause of the increased heart rate in the pigs. In addition, the total time needed for intubation was longer in the dorsoventral group. It may therefore be hypothesized that vagal nerve stimulation was distinctly less intense in the ventrodorsal group due to the significantly faster intubation manoeuvre. As a result of the fast intubation manoeuvre, no relevant vagal nerve stimulation took place. It is possible that an absence of vagally mediated heart rate depression caused the increased heart rate in the ventrodorsal group. Vagal nerve stimulation is very often accompanied by bradycardia, which probably counteracts an increase in heart rate and in turn masks potential changes in haemodynamics during intubation in dorsal recumbency. There was no correlation between the total time needed for intubation and the heart rate. However, turning the pig from the dorsoventral to the lateral or ventrodorsal position during instrumentation caused a significant drop in heart rate. This may have been due to a shift in the blood volume, particularly as a result of reduced cardiac preload after compression of the caval vein by the intestines. This hypothesis is supported by the results reported by Nakao et al. 46 who investigated the effects of different animal positions on cardiac output in dogs and pigs. Turning the animals from lateral recumbency to a dorsoventral position induced a 32% drop in cardiac output. 46 As the animals were not subjected to any intervention apart from the positional change, no vagal nerve stimulation took place. It may be assumed that this was why Nakao and colleagues 46 did not observe any difference in heart rate.
In addition, a decrease in systolic blood pressure during intubation was observed in both groups in the present study. They both had a significantly higher systolic arterial pressure before orotracheal intubation than afterwards, without any intergroup difference. As this occurred in both groups, it may be concluded that it is not a specific effect of the positioning of the animals, but rather a general response derived from a reduction in sympathoadrenal reactions by two mechanisms – the onset of an adequate depth of anaesthesia and lower levels of stress due to the cessation of mechanical stimuli. It is well known that this phenomenon occurs during general anaesthesia. 44,47
In the present study, comparing ventral and dorsal recumbency, none of the animals suffered hypoxia during the entire intubation procedure. This is due to adequate preoxygenation before intubation, as well as experience and skill on the part of the investigators. Good preparation is the reason why no complications occurred even during the more challenging intubation procedures in dorsal recumbency.
Both swine and other mammals are susceptible to respiratory depression during general anaesthesia, and safe airway management is therefore crucial. 8,11,48–50 It was demonstrated as long ago as 1964 that intubation can be a fast and safe method of protecting the airways. Schmitz and co-workers reported a study in pigs undergoing general anaesthesia. Intubation was achieved in 30–120 s without any fatal complications. 37 Marshall 12 also showed that the mortality rate decreases if pigs are intubated before surgical intervention. Whenever appropriate premedication and depth of anaesthesia are achieved, together with proper preoxygenation before intubation, we have not observed any laryngospasm during the entire procedure. In our 10 years' experience with pigs of different breeds, ages, weight and sex, as well as with differences in the technical equipment used, we have not encountered the findings reported by Rodriguez Montes and co-workers, 16 who described laryngospasms as a common problem. In earlier experimental protocols, we demonstrated that even pigs with cardiopulmonary compromise tolerate the procedure quite well when preoxygenation and a ventral recumbent position are used. The orotracheal intubation procedure using the method described is illustrated in Figure 2.
In summary, our own results and experience do not support the view that orotracheal intubation endangers pigs to a greater extent than spontaneous respiration or tracheotomy. After some training, all investigators should be able to carry out quick and successful orotracheal intubation with the animal in the ventrodorsal position in accordance with the method described. From our point of view, complete preparation of the animal and ensuring an adequate depth of anaesthesia, extensive practical experience and assistance from a trained assistant (if available) will help avoid almost all of the complications associated with orotracheal intubation. Finally, it should be emphasized that gentle and fast orotracheal intubation is the gold standard for airway management in pigs.
Footnotes
ACKNOWLEDGEMENTS
Financial support for this study was provided by the German Federal State of North Rhine–Westphalia (grant HBFG-112-470) and, in part, from the Else Kröner-Fresenius Foundation, Germany (grant P52/05//A32/05//F01). We are indebted to the perfusionists T Erker and G Kock of the Department of Thoracic and Cardiovascular Surgery at Münster University Hospital for their excellent technical assistance.