
Abstract
Optimal mechanical ventilation of the pregnant ewe during anaesthesia is of vital importance for maintaining fetal viability. This study aimed to compare peak inspiratory pressure (PIP), oxygenation and cardiovascular parameters with pressure-control (PCV) or volume-control (VCV) mechanical ventilation of anaesthetized pregnant sheep. Twenty ewes at 110 days gestation underwent general anaesthesia in dorsal recumbency for fetal surgery in a research setting. All the sheep were mechanically ventilated; one group with PCV (n = 10) and another with VCV (n = 10) to maintain normocapnia. PIP, direct arterial blood pressure, heart rate, arterial pH and arterial oxygen tension were recorded. PIP was lower in the PCV group (P < 0.001). Arterial oxygen tension was higher in the PCV group (P = 0.013). Mean and diastolic pressures were lower in the PCV group (P = 0.029 and P = 0.047, respectively). Both VCV and PCV provide adequate oxygenation of pregnant sheep anaesthetized in dorsal recumbency, though PCV may provide superior oxygenation at a lower PIP.
Pregnant sheep are commonly utilized as a model for studying human pregnancy and fetal physiology,1–3 and in keeping with the Australian code of practice for the care and use of animals for scientific purposes appropriate anaesthesia and perioperative analgesia must be provided to both the ewe and the fetus (National Health and Medical Research Council 2013). 4 There are a number of specific considerations relevant to general anaesthesia in sheep, which include the risk of regurgitation and subsequent aspiration of rumen contents; rumenal bloat; hypoventilation; hypoxaemia; and hypotension. Pregnancy also brings with it specific considerations: a higher than normal risk of regurgitation and subsequent aspiration of rumen contents; reduced cardiac reserve; reduced anaesthetic requirements; and the requirement to maintain fetal viability which depends upon adequate oxygen delivery to the placenta. Sheep undergoing surgical procedures are often in dorsal recumbency and when these animals are pregnant the potential for hypoxaemia to develop is higher than if they were in other positions, due to a reduction in lung functional residual capacity (FRC) and an increased risk of atelectasis.5–7 Given these considerations optimal mechanical ventilation of the pregnant ewe during anaesthesia may be difficult, but it is of vital importance to maintain maternal and fetal oxygenation, and therefore fetal viability.
Most modern anaesthetic workstations allow the selection of either volume-control ventilation (VCV) or pressure-control ventilation (PCV) when conventional positive pressure ventilation is applied. While both modes are time-cycled, termination of the inspiratory phase is determined when either a set tidal volume is delivered (VCV) or a set peak inspiratory pressure (PIP) is achieved (PCV). During VCV, therefore, PIP may vary from breath to breath while during PCV the tidal volume is likely to vary. These variations are functions of lung and thoracic wall compliance.
Positive pressure ventilation increases intrathoracic pressure and may reduce cardiac output due to impaired venous return. 8 Positive pressure ventilation may also cause acute lung injury if barotrauma or volutrauma occur. Barotrauma is caused by high airway pressures which lead to alveolar rupture and leakage of air into the pleural cavity. 9 Volutrauma occurs due to over distension of alveoli and subsequent damage to alveolar endothelium and epithelium. 10
Various human studies have investigated the potential benefits of choosing one type of mechanical ventilation over another. Results of these studies have been conflicting in terms of which mode produces the most satisfactory arterial oxygenation and PIPs. The majority of these studies were performed in an intensive care setting, with co-existence of complicating factors such as pre-existing lung disease or pneumoperitoneum. As far as we are aware there have been no studies investigating which ventilation modality is safer and more effective in pregnant sheep. Therefore the aim of this study was to compare PIP, arterial oxygen tension (PaO2) and arterial blood pressure with VCV and PCV in pregnant sheep during general anaesthesia. We hypothesized that PCV would lead to improved PaO2 at a lower PIP compared with VCV, and furthermore that this lower PIP would have a minimal impact upon arterial blood pressure.
Materials and methods
This study was approved by the Animal Ethics Committees of the University of Western Australia and Murdoch University.
Animals
Twenty merino singleton ewes at 110 days of gestation (term ∼150 days) underwent anaesthesia and surgery as part of another study. The sheep were held in the Large Animal Facility at the University of Western Australia in raised group pens for at least one week prior to surgery. Rooms were controlled for temperature (20.5–21.5℃) and relative humidity (40–60%). Ewes were weighed on the morning of surgery.
Anaesthesia
Food was withheld for 18 h before anaesthesia and free access to water was allowed until the premedication drugs were administered. Following physical examination the ewes were premedicated with a combination of acepromazine (0.03 mg/kg, ACP 2 injection, 2 mg/mL; Ceva Delvet Pty Ltd, Asquith, NSW, Australia) and buprenorphine (0.01 mg/kg, Temgesic, 0.3 mg/mL; Reckitt Benckiser, West Ryde, NSW, Australia) by intramuscular injection 30–40 min prior to the induction of anaesthesia. Anaesthesia was induced with a combination of midazolam (0.25 mg/kg, midazolam injection, 5 mg/mL; Pfizer Australia Pty Ltd, West Ryde, NSW, Australia) and ketamine (5 mg/kg, Ketamil, 100 mg/mL; Troy Laboratories, Smithfield, NSW, Australia) by intravenous injection and, with sheep in sternal recumbency, the trachea was intubated (Portex cuffed tracheal tube, 8.5 mm internal diameter; Portex Ltd, Hythe, UK). The sheep were positioned in dorsal recumbency and anaesthesia was maintained with isoflurane (1–2%, Attane Isoflurane 1 mg/mL; Bayer Australia Ltd, Pymble, NSW, Australia) in 100% oxygen delivered through a circle breathing system. The isoflurane vaporizer was adjusted, as judged by an experienced veterinary anaesthetist, to maintain an adequate depth of anaesthesia. A line block of ropivacaine (100 mg, Naropin 1%; AstraZeneca, North Ryde, NSW, Australia) was performed along the laparotomy incision site prior to surgery. Intermittent positive pressure ventilation was commenced immediately following anaesthetic induction, in order to maintain normocapnia (end tidal carbon dioxide [ETCO2] 35–45 mmHg) using a Datex Ohmeda ADU anaesthetic machine (GE Healthcare, Uppsala, Sweden). Physiological monitoring included electrocardiogram, pulse oximetry (with probe positioned on ear pinna), side-stream capnography (sampling rate 150 mL/min ± 20 mL), temperature and invasive blood pressure using a multiparameter monitor (Surgivet V9203; Smiths Medical, Rockland, MA, USA). Intravenous fluid therapy was administered throughout anaesthesia with 0.9% sodium chloride at 10 mL/kg/h. The rate of fluid administration was adjusted if required to manage intraoperative hypotension. At the end of surgery a transdermal fentanyl patch (Durogesic 75 µg/h; Jansen, Macquarie Park, NSW, Australia) was placed on clean skin of the medial thigh, adjacent to the udder.
Mechanical ventilation
The order in which the sheep underwent anaesthesia was already randomized for the fetal study, so allocation to VCV (n = 10) or PCV (n = 10) was in an alternating pattern. Respiratory rate was set to10 breaths per minute, inspiratory to expiratory ratio to 1:2 and positive end expiratory pressure to 0 cmH20; these parameters remained the same throughout anaesthesia. In the VCV group the initial tidal volume was set at 10 mL/kg and in the PCV group the initial PIP was set at 15 cmH2O. These settings were selected on empirical grounds from previous work with pregnant sheep in this environment. Tidal volume or PIP was adjusted as required to achieve a target ETCO2 between 35 and 45 mmHg. If ETCO2 was >45 mmHg the tidal volume was increased in increments of 25 mL for VCV, or the PIP in increments of 1 cmH20 for PCV, every 10 min until normocapnia was achieved. If ETCO2 was <35 mmHg the tidal volume was decreased in increments of 25 mL in VCV, or 1 cmH20 in PCV, every 10 min. PIP was recorded according to the measurement provided by the anaesthetic machine; the workstation incorporates a pressure transducer in the inspiratory limb of the circle system distal to the inspiratory valve. Set tidal volume was recorded continuously for all the sheep in the VCV group, however measured tidal volume was not recorded for either group as the workstation had no facility displaying or recording this variable.
Data collection
An 18 gauge over-the-needle catheter was placed into the radial artery to measure direct arterial blood pressure and to obtain arterial blood samples for blood–gas analysis. The catheter was attached to a fluid-filled transducer situated at the level of the heart base. Prior to arterial blood pressure measurements the transducer was flushed with heparinized saline, and zeroed to atmospheric pressure. Three consecutive measurements of systolic, mean and diastolic arterial blood pressure (SAP, MAP and DAP respectively) were made at each data collection time period. The mean of the three measurements was later calculated for each variable and used for the statistical analysis. The transducer was positioned approximately level with the right atrium of the heart. The arterial catheter was also used to collect samples for blood–gas analysis (Siemens RAPIDLab 248 system, Erlangen, Germany). Arterial blood pressure measurements and heart rate (HR) were recorded alongside PIP and ETCO2 at four separate time points, each approximately 20 min apart: T1 approximately 10 min following induction, once the arterial cannula was placed and the animal was moved to the theatre; T2 just prior to start of surgery; T3 during closure of the uterus; and T4 during skin closure. Blood–gas analysis was performed for the measurement of pH and PaO2 at T2 and T4 only.
Data analysis
For each sheep; the mean and 95% confidence intervals of the data for weight, isoflurane vaporizer setting and number of changes made to ventilator settings were calculated. A student’s t-test was then applied to test for any differences in these variables between the two groups (VCV and PCV).
The mean and 95% confidence intervals for each variable measured at each for the four time intervals (T1, T2, T3 and T4) were also calculated. A two-way repeated measures analysis of variance (ANOVA) was then applied to the data for ETCO2, PIP, arterial blood pressure, HR, pH and PaO2 considering ventilation mode (VCV versus PCV) and time as factors. This allowed the testing for differences between ventilation mode and between time intervals, as well as to consider whether any difference between ventilation modes also depended on a time interaction. If a significant difference in mean values (defined as P value of <0.05) was determined for either factor, pairwise multiple comparison procedures were applied using the Holm–Sidak method.
Results
Anaesthetic data for pregnant sheep ventilated using either volume-control ventilation (VCV) or pressure-control ventilation (PCV).

Data are expressed as mean (95% confidence interval [CI]) or median (interquartile range [IQR])*.
Mean (95% confidence interval) tidal volume setting for sheep in the VCV group was 9.4 mL/kg (8.0–10.8) at T1, 9.3 mL/kg (7.9–10.8) at T2 and 9.2 mL/kg (7.5–10.9) at both T3 and T4.
Cardiopulmonary variables for pregnant sheep ventilated using either volume-control ventilation (VCV) or pressure-control ventilation (PCV), at four different time intervals.
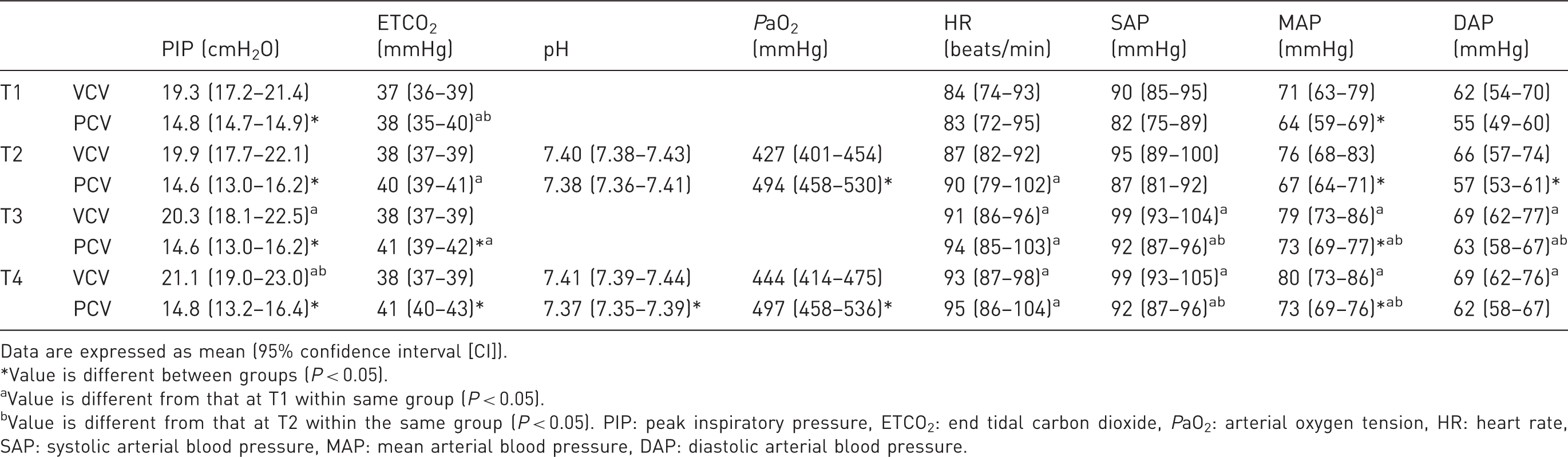
Data are expressed as mean (95% confidence interval [CI]).
Value is different between groups (P < 0.05).
Value is different from that at T1 within same group (P < 0.05).
Value is different from that at T2 within the same group (P < 0.05). PIP: peak inspiratory pressure, ETCO2: end tidal carbon dioxide, PaO2: arterial oxygen tension, HR: heart rate, SAP: systolic arterial blood pressure, MAP: mean arterial blood pressure, DAP: diastolic arterial blood pressure.
ETCO2 was maintained between the target range of 35–45 mmHg in all sheep in both groups throughout anaesthesia. ETCO2 was similar between the VCV and PCV groups at T1 (P = 0.829) and T2 (P = 0.096), however it was lower in the VCV group than the PCV group at T3 (P = 0.010) and T4 (P = 0.001). Within the VCV group there was no difference in ETCO2 between the different time intervals. Within the PCV group, ETCO2 increased over time.
The effect of ventilation mode on PIP depended on the time interval considered. PIP was higher in the VCV group when compared with the PCV group at all time points; T1 (P = 0.003), T2 (P < 0.001), T3 (P < 0.001) and T4 (P < 0.001). Within the VCV group PIP increased over time. Within the PCV group PIP did not differ significantly between the different time intervals.
There was no difference between SAP in the VCV group at any time point when compared with the PCV group. MAP was higher in the VCV group at T1 (P = 0.04), T2 (P = 0.023) and T4 (P = 0.046). DAP was higher in the VCV group at T2 (P = 0.037) when compared with the PCV group, but similar at all other time intervals. In both groups, arterial blood pressure tended to increase over time.
HR did not differ between the two groups at any time interval. In both groups, HR increased over time.
pH was similar in the VCV group when compared with the PCV group at T2, but higher in the PCV group at T4 (P = 0.007). pH did not differ between time intervals in either group.
PaO2 was lower in the VCV group when compared with the PCV group at T2 (P = 0.008) and T4 (P = 0.028). PaO2 did not differ between time intervals in either group.
Discussion
This study aimed to compare PIP, arterial oxygenation and cardiovascular parameters during PCV and VCV of anaesthetized pregnant sheep in dorsal recumbency. While the variables measured were within clinically acceptable ranges in both groups; PCV was associated with lower PIP, lower mean and diastolic blood pressure, and higher arterial oxygenation.
Both VCV and PCV modes of ventilation offer some advantages and disadvantages. In the VCV mode it is relatively easy to adjust ventilator settings based on tidal volume which can be estimated from the animal’s body weight. Once tidal volume is set, the ventilator will deliver that volume regardless of the PIP generated, unless a maximum allowed PIP has also been set. The PIP is a function of lung and chest wall compliance and resistance. As chest wall compliance is lower in pregnant animals the PIP may be relatively high for a given tidal volume. 11 The increased PIP that developed with time in the VCV group in our study indicates that compliance may have decreased with an increasing duration of anaesthesia. As previously mentioned, high inspiratory pressures may reduce venous return and therefore cardiac output. Maintenance of cardiac output is especially important in the anaesthesia of pregnant animals due to an increased likelihood of cardiovascular compromise resulting from physiological changes to the maternal cardiovascular system, and in order to maintain uteroplacental blood flow and fetal oxygenation.12,13 A further disadvantage of VCV is increased risk of volutrauma due to over distension of alveoli with more compliance or less resistance. 14 PCV can be less ‘user friendly’ as the delivered tidal volume varies from breath to breath, again as a function of respiratory compliance and resistance. However, in our study PCV did not pose any more difficulties than VCV to the user, given that we were able to maintain a normal ETCO2 with no significant difference in the number of changes to ventilator settings during anaesthesia between the two modes. A recognized benefit of the PCV mode is a more homogenous distribution of volume throughout different areas of the lung, thus improving gas exchange and potentially improving oxygenation. 14
Many studies investigating ventilation strategies in human patients have shown that inspiratory pressures generated during VCV are higher than those with PCV, however results have been conflicting. Peak airway pressures were found to be lower in patients receiving PCV compared with VCV in a study of adults undergoing one-lung ventilation and another study during adult laparoscopic surgery.15,16 Another study of adults undergoing laparoscopy found no difference in plateau and mean airway pressures between PCV or VCV groups; and in children during laparoscopic surgery PIP was similar between PCV and VCV groups, although mean airway pressure was higher with PCV.17,18 The shape of the inspiratory flow waveform generated by a ventilator may influence mean and peak airway pressures. In 1996, Davis et al. investigated the use of VCV with a traditional square flow waveform, VCV with a decelerating flow waveform, and PCV with a decelerating flow waveform in patients with acute lung injury: in all modes a set tidal volume was delivered and positive end-expiratory pressure adjusted to maintain PaO2 > 70 mmHg. They found that PCV and VCV with a decelerating waveform lead to a lower PIP yet also to a higher mean airway pressure when compared with VCV with a square waveform. 19 A decelerating flow pattern (as is generated in PCV mode) is met with less flow resistance than the constant flow pattern of VCV, meaning that less airway pressure is generated and PIP is lower; however the decelerating pattern does tend to lead to higher mean airway pressures. 20 Unfortunately in our study we had no facility for measuring the mean airway pressure, so it is possible that despite generating a higher PIP, VCV may have produced equal or lower mean airway pressures.
Different inspiratory flow waveforms may account for the differences in arterial pressure found between the VCV and PCV groups in our study. One would expect that arterial pressure might have been lower in the VCV group given the higher inspiratory pressures generated. However our findings were to the contrary. Lower mean airway pressure in the VCV group due to a different flow waveform may explain this difference in arterial pressure. Increased mean airway pressure might be expected to have more negative impact on venous return than increased PIP. 8 It should be noted that the power of our study to determine a difference in HR or arterial blood pressure was low (<0.5); and increasing our sample size might have produced different results.
Studies investigating the effects of different ventilation strategies on oxygenation of human patients have also had varying results. Arterial oxygenation was improved with PCV when compared with VCV in a study of adult patients undergoing one-lung ventilation, another of adults undergoing laparoscopy, and in patients with acute lung injury.15,18,19 By contrast, there was no difference in oxygenation between patients receiving VCV and PCV in a different study of adults undergoing laparoscopy. 16 The superior oxygenation observed with PCV is thought to be due to improved alveolar gas distribution. An important cause of hypoxaemia in anaesthetized animals is the development of areas of lung with a low ventilation/perfusion ratio.21,22 This type of hypoxaemia is particularly relevant in animals with reduced FRC, as occurs in pregnancy.5,11,22 A more homogenous distribution of inspired gases throughout the alveoli improves the ventilation/perfusion ratio and reduces atelectasis, lessening the risk of hypoxaemia.14,17,22 In our study, despite a higher PaO2 during PCV, both methods led to more than adequate oxygenation with an inspired oxygen fraction of 100%. It is important to note that although there was a statistically significant difference in the PaO2 between the two groups, hypoxaemia did not occur in any sheep at any of the time points. It is possible that the difference between the two modes may have been more clinically relevant had a lower fraction of inspired oxygen been used. Had we the ability to measure arterial carbon dioxide tension (PaCO2) and haemoglobin concentration we would also have been able to calculate indices of oxygenation, such as the P(A–a)O2 gradient, which may have provided further information regarding efficiency of oxygenation and gas exchange.
Failure to measure PaCO2 was a major limitation to our study. A technical fault precluded this measurement. Instead we had to rely upon ETCO2 as a surrogate for PaCO2. ETCO2 reflects the PaCO2 in a variety of species, provided ventilation and perfusion are matched normally.23,24 PaCO2 is expected to be approximately 3–5 mmHg higher than ETCO2 in healthy small animal patients, although there may be a 5–12 mmHg difference in anaesthetized horses in dorsal recumbency. 25 If there is a high ventilation/perfusion ratio, for example due to increased alveolar dead space secondary to poor pulmonary perfusion, the difference between ETCO2 and PaCO2 increases. 23 Alveolar–arterial gas tension gradients in pregnant sheep have not been investigated. Without comparing ETCO2 and PaCO2 in our study we cannot preclude a widened alveolar–arterial gradient, and thus cannot directly compare the adequacy of ventilation between the two groups of sheep. As previously mentioned, the different flow patterns of the two ventilation modes in this study may have influenced ventilation/perfusion matching within the lung. If the ventilation/perfusion ratios were different the efficiency of CO2 elimination from the arterial blood into the lung may also have been affected. This phenomenon may create variable gradients between the ETCO2 and PaCO2 between the study groups.
Another limitation to our study was the inability to measure respiratory volumes. It is possible that the tidal volume delivered varied widely between the two groups. We attempted to measure tidal volume using a Wright’s respirometer placed between the proximal end of the endotracheal tube and breathing system. Unfortunately a large amount of condensation within the breathing system lead to concern over inaccuracies in measurement subsequent to inertia, and corrosive damage to the gearing mechanism of the instrument. 26
In conclusion, this study indicates that at the chosen settings both VCV and PCV modes of mechanical ventilation provide adequate oxygenation of pregnant sheep anaesthetized in dorsal recumbency. PCV in these animals was associated with superior arterial oxygenation at a lower PIP without having a clinically significant impact upon arterial blood pressure.
Footnotes
Acknowledgements
The authors would like to thank the Dr Matthew Kemp and his research team at the School of Women and Infants Health, University of Western Australia.
Declaration of conflicting interests
None declared. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sector.